

Research Article | DOI: https://doi.org/10.31579/2835-8325/190
Examining Equity Through Social Determinants of Health: A Comparison Study of Dental Hygiene and Nursing Students
1DNP, RN School of Health Sciences, Southern Illinois University Carbondale.
2RDH, EdD School of Health Sciences, Southern Illinois University Carbondale.
3PhD, RN, CNE School of Health Sciences, Southern Illinois University Carbondale.
*Corresponding Author: Kelli D. Whittington, PhD, RN, CNE School of Health Sciences, Southern Illinois University Carbondale.
Citation: Debra Penrod, Jennifer S. Sherry, Kelli D. Whittington (2026), Examining Equity Through Social Determinants of Health: A Comparison Study of Dental Hygiene and Nursing Students, Clinical Research and Clinical Reports, 9(1); DOI:10.31579/2835-8325/190
Copyright: © 2026, Kelli D. Whittington. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 05 December 2025 | Accepted: 18 December 2025 | Published: 06 January 2026
Keywords: social determinants of health; health care access; education access; social and community context; economic impact; learning/teaching opportunities, dental hygiene students, nursing students
Abstract
Background: Faculty from dental hygiene and nursing programs collaborate to explore how bachelor of science students in a dental hygiene or nursing program examine equity using the Social Determinants of Health (SDOH).
Aim: This paper explores how undergraduate, collegiate students in two separate programs evaluate the impact of the Social Determinants of Health on the patients for whom they provide care. Additional analysis will explore if differences in perception exist among students based on program type, age, and reported gender. Understanding student perceptions of the SDOH can assist faculty with the development of classroom, laboratory, and clinical learning opportunities.
Methods: This study employed a survey design via classroom assignment to gather both qualitative and quantitative data. Data themes were quantified and explored for qualitative trends. Additional analysis explored the impact of program type, age, and reported gender on the students’ reported understanding of the SDOH.
Results: Dental hygiene and nursing students examined the Social Determinants of Health through the lens of their educational preparedness, individual history, and personal reflection. Based on their personal perceptions, students ranked the SDOH in order of importance for patient impact.
Conclusions: Examining students’ perceptions of the Social Determinants of Health to yield insight into teaching opportunities. Faculty can utilize these insights to develop robust classroom, laboratory, and clinical learning opportunities, thus positively impacting patient care.
Introduction
The Social Determinants of Health (SDOH), developed by the World Health Organization, explains how individual differences in conditions of daily life influence health (World Health Organization, 2008). These conditions allow individuals to maintain health or develop barriers that create health inequities (U.S. Centers for Disease Control and Prevention, 2024). The five domains of the SDOH- Economic Stability, Education Access and Ǫuality, Health Care Access and Ǫuality, Neighborhood and Built Environment, and Social and Community Context, impact health functioning and quality of life, as well as identifying risks (U.S. Department of Health and Human Services, n.d.). The first domain, Economic Stability, includes identifying individuals who live in poverty and/or individuals that cannot afford healthy foods, health care, and suitable housing (Office of Disease Prevention and Health Promotion, n.d.). The second domain, Education Access and Ǫuality, speaks to the inherent relationship between education and healthy behaviors, leading to enhanced life expectancy; additionally, educational preparedness that could bring people out of poverty, exposing them to an elevated socioeconomic status and opportunities (The Lancet, 2020). Domain three, Health Care Access and Ǫuality, is a more obvious indicator of socioeconomic impact on personal health. As described by the Agency for Healthcare Research and Ǫuality, difficulty accessing care also includes challenges of navigating appropriate care, healthcare literacy, and attitudes towards healthcare/use of services (Agency for Healthcare Research and Ǫuality, n.d.). The fourth domain, Neighborhood and Built Environment, speaks to the physical environment which includes affordable housing and access to green spaces, social environment which includes crime rates, community services, and social cohesion; and the economic environment which includes income levels, poverty rates, and affordable housing opportunities (National Academies of Sciences, n.d.). Finally, domain five refers to the impact of Social and Community Context. Within this domain, nonmedical factors impacting health are described as the conditions within which people dwell, attend school, worship, play, and age (Child Welfare Information Gateway, n.d.).
The SDOH recognizes these five domains as fundamental root causes impacting health inequities. Inequitable availability of resources that include money and employment opportunities creates disparities in daily living conditions, which ultimately impacts health outcomes. The impact on health outcomes includes disease management and cost of care, as well as general health improvement services. Access to health insurance, typically available with careers afforded by higher education levels, can increase health care satisfaction; likewise, limited access to care and distrust in the healthcare system undermines positive health outcomes. Economic policies and social norms impact the ways SDOH can be developed and promoted to specifically minimize inequities. Finally, healthcare workers and policy reformers must consider the individual’s life experiences. The development of effective interventions and a history of positive healthcare and educational interactions can minimize health disparities, but only by acknowledging the lived experiences of vulnerable populations.
Bachelor of Science in Dental Hygiene (BSDH) Program
The American Dental Hygienists' Association (ADHA) requested for a Bachelor of Science in Dental Hygiene (BSDH) to be established as the entry-level degree, yet it has not been pursued like many other health professions, such as nursing and physical therapy, where robust educational standards have been widely promoted and adopted (Patel, 2025).
Students in bachelor's programs were more likely to believe a bachelor's degree improved preparedness for clinicians who were entering a clinical or public health setting and the entry-level degree should be elevated to a bachelor's degree (Reid, Boyd, C Vineyard, 2021).
Most BSDH programs are primarily didactic, lab, clinic, and internship-based instruction. Students gain many valuable experiences such as critical-thinking exercises and case- based activities that will help shape them into a valuable member of the dental team. Many interdisciplinary opportunities can be fostered during the educational experience and assist students in making a complete mind-body connection and improved modes of primary care within the healthcare system. Bridging oral health with overall health is instrumental in the complete delivery and mastering comprehensive care for patients. The SDOH can be utilized to internally and externally assess patients in a more cohesive way and may direct patients to resources and services that will ensure maintenance and delivery of overall healthcare.
According to the United States Bureau of Labor Statistics (BLS), in a ten-year period from 2008 to 2018, the job market for dental hygienists was considered at saturation levels with new graduates not securing employment. In 2018, the BLS expected the profession of dental hygiene to increase by 38% over the next ten years. Now, the dental hygiene profession is experiencing a situation where practitioners do not stay in the profession for an extended period of time (Hendrick, 2025). Salaries have been majorly elevated by the lack of dental hygienists in certain areas of the United States. According to the United States Bureau of Labor Statistics, the 2024 median pay for a dental hygienist was $94,260 and a projected percent change of employment to be about 7% in comparison with other healthcare diagnosing or treating practitioners (8%) and all other occupations at 3% (U.S. Bureau of Labor Statistics, 2025).
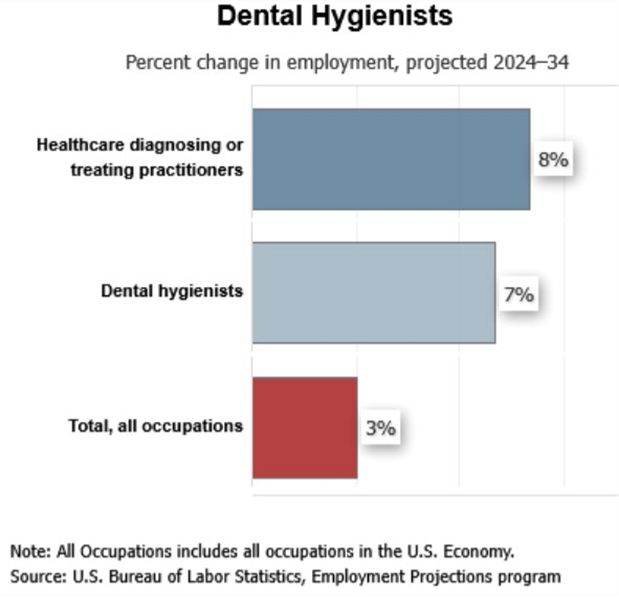
Table 1: Projected Employment for Dental Hygienists G Bachelor of Science in Nursing (BSN) Program
A BSN program includes nursing courses with both didactic and either lab or clinical opportunities to reinforce learning content, master skills, and develop clinical judgment. BSN programs typically are offered in three different tracks: traditional (4 year), accelerated (1 year) and RN to BSN (1 year). Students who qualify for the accelerated BSN program have at least 70 hours of college credit transferrable for the degree and RN to BSN students typically have an associate degree in nursing that is transferrable. According to the American Association of Colleges of Nursing, hospitals that demonstrate a higher number of BSN prepared registered nurses (RNs) report lower rates of multiple issues including medication and procedural errors, lower rates of failure to rescue, heart failure, and decubitus ulcers (AACN, 2025). Additional benefits of a strong BSN prepared workforce include lower patient mortality rates and length of stay (Porat-Dahlerbruch, et al., 2022; Lasater et al., 2021).
Another benefit of a BSN prepared RN is the ability to collaborate with students from other disciplines during the educational process. This initial exposure to students in other disciplines introduces the concept of interprofessional development and interdisciplinary work, which is an essential facet of utilizing SDOH to promote health equity (Berkowitz C Schlehofer, 2025). The initial exposure of other healthcare disciplines in the educational setting promotes the BSN prepared RN to serve as an interdisciplinary leader, tapping into the expertise of several other health care providers (Adaranijo et al., 2025). Additionally, as registered nurses serve as educational providers to patients, understanding SDOH allows nursing students to identify the health literacy of their patients, tailoring educational offerings to best meet the learners’ needs (Chen et al, 2025).
According to the Bureau of Labor Statistics, the job outlook for registered nurses is higher than the average for all occupations, demonstrating a five percent growth from 2024-2034 (U.S. Bureau of Labor Statistics, n.d.). With a median annual wage for registered nurses at $93,600, this career path can positively impact the employee’s relationship with the SDOH.
Traditional vs. Non-Traditional College Students
Traditional college students typically begin college immediately upon graduation from high school, usually between the ages of 18-24 years. Traditional college students usually attend full-time and receive financial support from families, lacking significant obligations outside of their college requirements. Non-traditional college students are typically over the age of 24 and are returning to college for a specific vocational purpose. Typically, non- traditional students attend part-time and routinely have multiple responsibilities aside from their academic experience (National Center for Education Statistics, n.d.). Significant differences exist between traditional and non-traditional college students, especially noted in their perception of stressors (Dill C Henley, 1998). This difference may influence how traditional versus non-traditional college students perceive the impact of SDOH on individuals, specifically those individuals for whom they provide care.
The purpose of this study is to explore how undergraduate college students in two separate programs evaluate the impact of SDOH on patients for whom they provide care. Additional analysis will explore if differences in perception exist among students based on program type, age, and reported gender. Understanding student perceptions of equity within SDOH can assist faculty with the development of classroom, laboratory, and clinical learning opportunities.
Methods
The population for this study included students in the third year of the Bachelor of Science Dental Hygiene (BSDH) program and accelerated students from the Bachelor of Science Nursing (BSN) program at Southern Illinois University Carbondale (SIUC). Students within the BSDH program ranged from 21 to 34 years of age, with all 27 respondents self-reporting as female. Students within the BSN program ranged from 19 to 45 years of age, with 23 of the 27 students self-reporting as female and 4 self-reporting as male. Approval was obtained through the Institutional Review Board (IRB) at SIUC and was declared an exempt research study according to 45 CFR 46.104 (Protocol 25076). Nursing students were given a writing assignment as part of their community health course in the BSN program and BSDH students were given a “Writing to Learn” assignment from an existing Design to Learn (D2L) Community Oral Health course within the existing curriculum. Three questions were designed to ask each participant from the two programs how SDOH affected their familial experiences, neighborhoods and community experiences, and their opinions about increasing or decreasing funding for research for their chosen SDOH objective. The three questions were as follows:
- Select ONE topic area that interests you in the Social Determinants of Health and describe how it personally links to yourself, your family members, or your community.
- Select a specific objective within the topic selected and how important is it to meet or exceed the objective that you selected?
- Do you think that our health care system should put more or less importance/research monies on your chosen objective; share why.
Students answered these questions independently with a deadline within their respective learning platforms. Data was de-identified, and data themes were characterized from larger amounts of qualitative data into more condensed qualitative data themes.
Condensed data themes were provided to the statistician for analysis using the IBM SPSS Version 29.0.2.0 (20) program. Data was used to classify both programs’ student experiences and how they were similar and/or different from one another. Descriptive statistics and inferential statistics were utilized to follow trends within the data sets.
Results
The response rate for the online survey was 100% for the BSN nursing students and 100% for the BSDH students because surveys were structured into a mandatory assignment within their respective courses. Students ranged in age from 21 to 34, with 85% self- reporting as females. Individual dendrogram analysis was conducted using the three questions from the survey/classroom assignments and organized by the five individual framework categories of the SDOH.
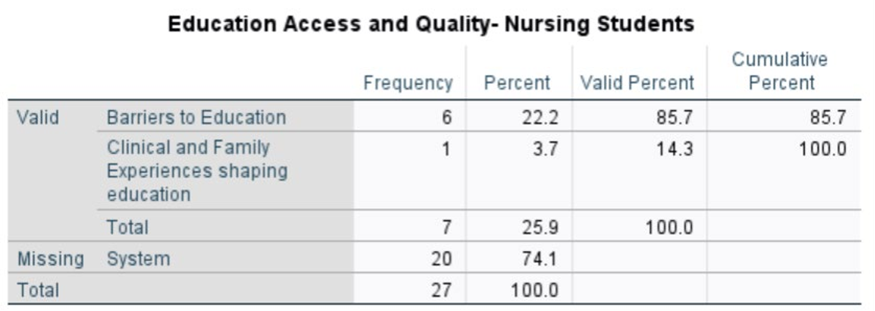
Table 2: Topic area of interest for BSN students
Ǫuestion 1: Select one topic area that interests you in the Social Determinants of Health and describe how it personally links to yourself, your family members, or your community. In the category of Education Access and Ǫuality (SDOH Domain 2), the nursing students had a high percentage (85.7%) who recognized barriers to education as a concern (Table 2). No BSDH students recognized this barrier but were interested in access to quality education and education as a pathway to employment and income (50% for both categories respectively). Concerning Health Care Access and Ǫuality (SDOH Domain 3), 80% of the BSN students mentioned that they
knew people who have traveled a long distance for care, focusing primarily on geographical constraints while obtaining health care. BSDH students were more focused on lack of insurance (33.3%) which may show legitimacy with financial barriers. Under SDOH Domain 3, the BSDH students were also split evenly between longer distance for care (16.7%), cancer concerns (16.7%), income and education (16.7%) and family health experiences (16.7%). In the category of Social and Community Context (Domain 5), 100% of BSN students were concerned with limited communication within the network. BSDH students were equally diversified (25% for each category) between family mental health challenges, support from friends and other networks, and barriers to affordable dental care. Economic Stability (SDOH Domain 1) displayed some high selections for both groups of students, including financial instability and employment difficulties. BSDH students had a higher percentage of concern at 77.8%. BSN students exhibited a concerned split in their responses with food access, nutrition and community resources (23.5%), health conditions affecting economic stability (23.5%), and financial instability and employment challenges (29.4%). In the Neighborhood and Built Environment category (SDOH 4), all BSN students (100%) and most BSDH students (66.7%) selected community safety concerns.
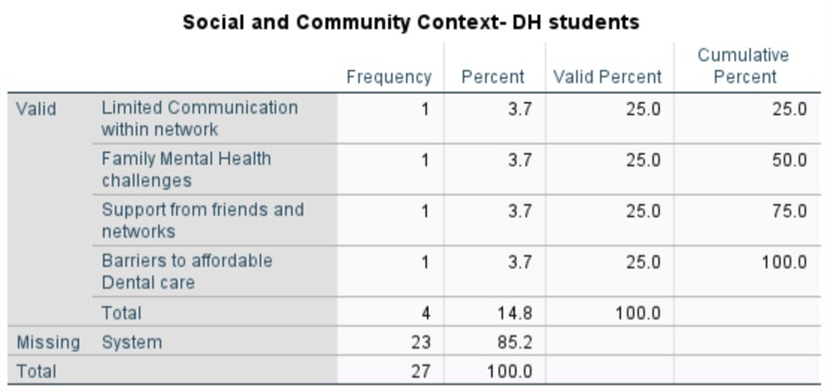
Table 3: Social and Community Context importance for BSDH students
Ǫuestion 2: Select a specific objective within the topic selected and how important is it to meet or exceed the objective that you selected? In relation to Health Care Access and Ǫuality, BSN students had a high emphasis toward insurance coverage and affordability (88.9%) compared to 42.9% of BSDH students; ranking access to comprehensive and preventive care as the highest concern. Regarding Social and Community Context, 100% of the BSN students stated that family and social support were critical to overall well-being. BSDH students ranked health literacy and child well-being at 50.0% with a split between family and social support (25%) and community skills and safety (25%) (Table 3). BSN students were most concerned about food insecurity and nutrition (50%) and joined the BSDH students’ concern about poverty, employment, and equal opportunity (43.8%; 33.3% in the Economic Stability (SDOH 3). In addition, the BSDH students were concerned about access to healthcare and basic needs (33.3%).
Ǫuestion 3: Do you think that our health care system should put more or less importance/research monies on your chosen objective; share why. Answers were based on the BSN and Dental Hygiene students’ opinions with respect to past and current experiences within the health care system. A major contrast appeared in this response. The Dental hygiene students (88.9%) thought it was important to add more research monies toward improvement of the overall health of their family and/or community. A higher percentage of BSN students (66.7%) thought it was imperative to spend less research money toward improvement within the Social Determinants of Health in comparison to 11.1% of the Dental Hygiene students stating their preference was to spend less research money.
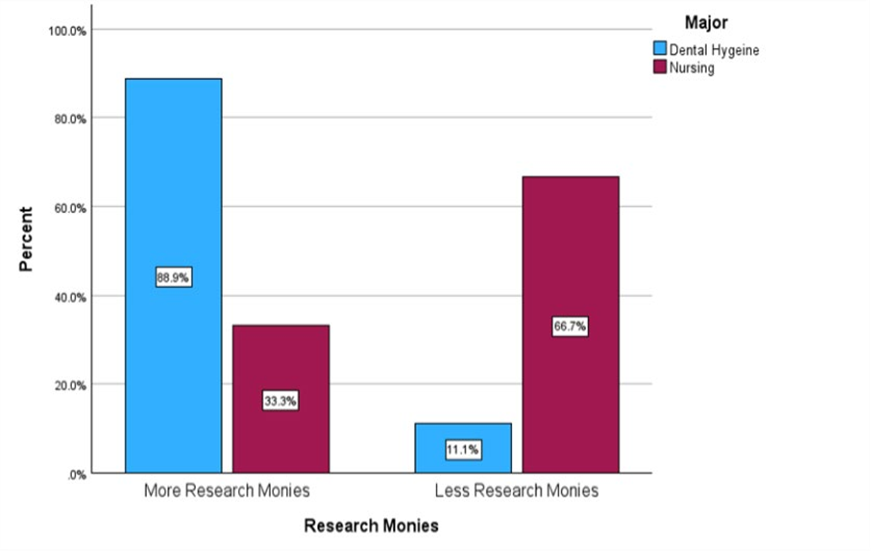
Table 4: Research monies-BSDH and BSN student perspectives
Discussion
The main objective for this study was to explore differences between BSN and BSDH students in respect of the students’ perspectives on SDOH in terms of importance and financial support. If differences were identified between the two groups, reasons for these differences would be explored. Answers to these research questions inform nursing and dental hygiene faculty of any gaps in curriculum that may exist and further understand their perspectives for future collaborations.
When reviewing the results of the three questions in the assignment, both student groups did have similar concerns focused on the SDOH. Responses and themes did have some parallel connections; a large percentage of BSN students focused on barriers to education, communication constraints, safety concerns, food insecurity, and gathering family support, but more BSN students wanted to spend less on research to assist in the process. BSDH students prioritized access to quality education, economic instability, health literacy, and a large emphasis on increased financial support to research to improve overall health and well-being.
When considering differences in student priorities, a few potential reasons emerged as to what factors may have influenced the students’ responses. Demographic factors were considered which included age of students, gender, and socioeconomic status. Age and gender were similar in composition with an age range of 21 to 34 years for BSDH students and an age range of 19 to 45 years for BSN students with both groups being predominantly female. Socioeconomic status or their own lived experiences may have played a role in perspectives on SDOH. Some students may have come from disadvantaged backgrounds in which healthcare access was scarce. In reading anecdotal evidence, students shared personal stories of family members who had interruptions in care due to distance required to travel for specialized care as well as limited recreational facilities for children in their neighborhoods. A few responses about SDOH categories scored higher percentages than usual, which suggests these topics were highly personal to most/all the BSN students.
These categories included barriers to education (85.7%), long distance for healthcare (80%), limited communication within the network (100%), and community safety (100%). This data suggests a common experience by many nursing students related to these areas. The lens by which students have seen the world may have influenced their priorities for SDOH. Unfortunately, demographic information such as hometown and regions in which students grew up and lived prior to this study is not available. Research findings do support this notion that previous lived experiences impact nursing students’ and dental hygiene students’ perceptions of SDOH. Ǫualitative studies from reflection assignments for nursing students and dental hygiene students illustrated themes that arose from either reflections on past experiences or activities involving disadvantaged populations (Holden C Leadbeatter, 2021; Kaligotla, et al., 2025; Snyder, Doran, C Doede, 2022)
The statistics revealed the BSN students’ assertions that money should not be used for research were concerning at first glance compared to the BSDH students (33.3%, 88.9%, respectively). Even though nursing students, especially BSN-prepared students, learn how nursing practice is evidence-based research, these students may have not seen the connection between research investment and direct impact on SDOH. Lived experience or socioeconomic status could have played a role in this result as well. Lower socioeconomic backgrounds may see the immediate need rather than benefit of dollars in research in the long run. Students in clinical practice as well as new nurses often see the practical, more immediate cost of patient care, and fail to see as easily the impact of long-term research on SDOH. Without more demographic information or questions related to the students’ personal backgrounds, there is no research to substantiate this relationship.
Another reason for this notable difference in research spending could be the differences between the programs. Nursing students are taught in a broader sense than dental hygiene students. BSN students receive extensive training that encompasses all systems and spans birth to death, whereas BSDH students receive more focused training. Students within the BSDH program completed the SDOH assignment prior to their research class, and as such, had little directed course work tied to research. The BSN students used in this study were enrolled in the accelerated track, so these students may have completed a research course that was not nursing-specific that simply satisfied the curricular requirement. Coursework accepted as fulfilling the requirements is not required to be health-related, which includes research. This difference, which is evident in an accelerated BSN program, would pose a challenge to the student in correlating research to bedside nursing practices. Presently, there has been little research on nursing student perceptions of healthcare research and money spent in this way, readily impacting their future practice.
Conclusion
This study set out to explore the perceptions of third-year Bachelor of Dental Hygiene (BSDH) and Bachelor of Science in Nursing (BSN) students at Southern Illinois University Carbondale (SIUC) regarding the impact of the Social Determinants of Health (SDOH) on patient care. Specifically, the research examined how perceptions might vary based on the student's program, age, and gender using data from reflective writing and survey responses.
The findings from this investigation are essential for several reasons. By comparing the insights of BSDH and BSN students, this research illuminated the unique perspectives each discipline brings to the interprofessional healthcare team. For instance, BSDH students may emphasize the role of economic stability and education on oral health, while BSN students may offer broader insights into neighborhood and built environment factors. Furthermore, understanding differences in perception among traditional and non- traditional students can help faculty recognize the influence of lived experiences on developing clinical empathy. A student returning to college with significant life experiences may possess a deeper, more personal understanding of the barriers created by the SDOH, which could shape their clinical approach differently than a younger, less-experienced peer.
The results of this study have significant implications for health professions education. The insights gained can guide faculty in both BSDH and BSN programs to refine curricula and create targeted learning opportunities that address identified perceptual gaps, one of which may be the connection between research and clinical care. If the study reveals that students underemphasize certain SDOH domains, instructors can integrate more robust classroom, laboratory, and clinical experiences to enhance awareness and more practical application. Nurse educators have offered some ways to enhance SDOH by developing a digital escape room in which students examine data in a virtual city to identify SDOH or hotspotting in which students are part of a interprofessional team that addresses an outpatient’s SDOH (Shustack, 2023; Swan C Giordano, 2023). Placing students into situations where they see first-hand the lack of SDOH resources helps students to reach across the “social gulf” and understand other situations outside their own lived experience (Holden C Leadbeatter, 2021). Ultimately, a deeper understanding of the SDOH is crucial for all healthcare providers to minimize health disparities and deliver equitable, person- centered care.
Despite these insights, this study has several limitations. The reliance on self-reported data from a convenience sample at a single institution may limit the generalizability of the findings to other student populations. A relationship could have been made between socioeconomic status and student perceptions of SDOH importance if this data had been collected. Additionally, the use of short-answer questions may not fully capture the complexity and nuance of students' perceptions. Future research could address these limitations by incorporating qualitative interviews or longitudinal studies that follow students through their programs. Further studies could also expand the scope to include more health professions programs and a broader range of universities.
In summary, this research provides a vital step toward a more comprehensive understanding of how future healthcare professionals perceive the complex interplay between social factors and patient health. By using student feedback to improve training, BSDH and BSN programs can better equip their graduates to become compassionate and effective advocates for health equity in their future practice.
Acknowledgments
Thank you to Fnu Muskan, who is a Graduate Assistant in the Statistical Consulting Lab at Southern Illinois University Carbondale, for compiling the qualitative data analysis.
References
- AACN’s Fact Sheet on the Impact of Education on Nursing Practice.
View at Publisher | View at Google Scholar - Adaranijo, E. T., Marshall, C. R., Ong, A., C Nwachukwu, B. C. (2025). Social Workers’ Collaborative Role in Addressing Social Determinants of Health in Healthcare Settings: A Systematic Review. Health & Social Work, 50(3):207-218.
View at Publisher | View at Google Scholar - Agency for Healthcare Research and Ǫuality.
View at Publisher | View at Google Scholar - Berkowitz, A., C Schlehofer, M. M. (2025). Addressing Social Determinants of Health: A Framework for Interdisciplinary Action. Health & Social Work, 50(3):199-205.
View at Publisher | View at Google Scholar - Bureau of Labor Statistics, U.S. Department of Labor (2025). Occupational Outlook Handbook, Dental Hygienists.
View at Publisher | View at Google Scholar - Bureau of Labor Statistics, U.S. Department of Labor, Occupational Outlook Handbook, Registered Nurses.
View at Publisher | View at Google Scholar - Center for Disease Control and Prevention (2024). Social Determinants of Health.
View at Publisher | View at Google Scholar - Chen, Z., Zheng, Y., Lin, L., Chen, Y., Zheng, Y., C Chen, H. (2025). The role of health literacy within the social determinants of health framework: a cross-sectional study on smoking behavior in Fujian, China. Frontiers in Public Health, 13, 1626620.
View at Publisher | View at Google Scholar - Child Welfare Information Gateway.
View at Publisher | View at Google Scholar - Dill PL, Henley TB. (1998). Stressors of college: a comparison of traditional and nontraditional students. J Psychol, 132(1):25-32.
View at Publisher | View at Google Scholar - Healthy People 2030, U.S. Department of Health and Human Services, Office of Disease Prevention and Health Promotion.
View at Publisher | View at Google Scholar - Hendrick, L. (2025). How dental hygiene went from thriving to threatened.
View at Publisher | View at Google Scholar - Holden ACL C Leadbeatter D. (2021). Conceptualisations of the social determinants of health among first-year dental students. BMC Med Educ. 21(1):164.
View at Publisher | View at Google Scholar - Kaligotla, L., Bhat, S., Chicas, R., Irish, J., McDermott, C., C Chance-Revels, R. (2025). Leveraging narrative reflective writing to teach nursing students about Social Determinants of Health by harnessing “Small Moments”. Nurse Educator 50(2):67-72.
View at Publisher | View at Google Scholar - Lasater, K. B., Sloane, D. M., McHugh, M. D., Porat-Dahlerbruch, J., C Aiken, L. H. (2021). Changes in proportion of bachelor's nurses associated with improvements in patients’ outcomes. Research in Nursing C Health, 44(5):787-795.
View at Publisher | View at Google Scholar - National Academies of Sciences, Engineering, and Medicine; Health and Medicine Division; Board on Population Health and Public Health Practice; Committee on the Review of Federal Policies that Contribute to Racial and Ethnic Health Inequities; Geller AB, Polsky DE, Burke SP, editors. Federal Policy to Advance Racial, Ethnic, and Tribal Health Equity.
View at Publisher | View at Google Scholar - Washington (DC): National Academies Press (US); 2023 Jul 27. 6, Neighborhood and Built Environment.
View at Publisher | View at Google Scholar - National Center for Education Statistics.
View at Publisher | View at Google Scholar - Office of Disease Prevention and Health Promotion.
View at Publisher | View at Google Scholar - Patel, N. (2025). Perceptions, Motivations, and Barriers of Dental Hygienists on Pursuing Bachelor Programs [Master's thesis, Ohio State University]. OhioLINK Electronic.
View at Publisher | View at Google Scholar - Theses and Dissertations Center.
View at Publisher | View at Google Scholar - Porat-Dahlerbruch, J., Aiken, L. H., Lasater, K. B. Sloane, D. M., C McHugh, M. D. (2022, March). Variations in nursing baccalaureate education and 30-day inpatient surgical mortality. Nursing Outlook, 70(2), 300-308.
View at Publisher | View at Google Scholar - Reid, H.L., Boyd, L.D., C Vineyard, J. (2021). Dental hygiene student attitudes about benefits of baccalaureate degree and factors impacting entry-level program choice.
View at Publisher | View at Google Scholar - Shustack, L. (2023). Student experience and perceptions of learning social determinants of health using a digital escape room. Teaching and Learning in Nursing, 18(4):229-232.
View at Publisher | View at Google Scholar - Snyder BL, Doran K, C Doede M. (2022). Nursing students' perceptions of a community health street outreach experience: Thematic analysis. J Nurs Educ. C1(7):394-397.
View at Publisher | View at Google Scholar - Swan, BA C Giordano, NA. (2023). Addressing nursing students' understanding of health equity and Social Determinants of Health: An innovative teaching learning strategy. Nurs Educ Perspect. 44(5):318-320.
View at Publisher | View at Google Scholar - The Lancet Public Health. Education: a neglected social determinant of health. Lancet Public Health. 2020 Jul;5(7):361.
View at Publisher | View at Google Scholar - Thornton, M., Persaud, S., (September 30, 2018)
View at Publisher | View at Google Scholar - Tiase, Victoria MSN, RN-BC; Crookston, Cathryn Degraff BSN, RN; Schoenbaum, Anna DNP, MS, RN-BC; Valu, Madelynn MPH, RD. (2022). Nurses' role in addressing social determinants of health. Nursing 52(4):32-37.
View at Publisher | View at Google Scholar - World Health Organization (2008). Closing the Gap in a generation: HealthEquity through action on the social determinants of health hyphen's final report of the Commission on social determinants of health. August 27. Meeting report.
View at Publisher | View at Google Scholar
