

Research article | DOI: https://doi.org/31579/2834-5126/012
Evaluation of Q Angle Endurance and Flexibility of Athletes with Knee Pain
1 Eastern Mediterranean University, Department of Physical Therapy and Rehabilitation, Famagusta, North Cyprus via Mersin 10 Turkey
2 Eastern Mediterranean University, Department of Physical therapy and Rehabilitation, Famagusta, North Cyprus via mersin 10 turkey
3 Eastern Mediterranean university, Department of physical therapy and rehabilitation, Famagusta, North Cyprus via Mersin 10 Turkey
*Corresponding Author: Burçin Uğur Tosun, EASTERN Mediterranean University, Department of Physical Therapy and Rehabilitation, Famagusta, North Cyprus Via Mersin 10 Turkey.
Citation: Burçin Uğur Tosun, Tayfun Arslan, Emine Handan Tüzün. (2023), Evaluation of Q Angle Endurance and Flexibility of Athletes with Knee Pain. Clinical Trials and Clinical Research. 2(1); DOI:10.31579/2834-5126/012
Copyright: © 2023 Burçin Uğur Tosun, this is an open access article distributed under the creative commons’ attribution license, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 13 January 2023 | Accepted: 23 January 2023 | Published: 13 February 2023
Keywords: athlete; pain; q angle; endurance; functionality
Abstract
Objective: This study aims to compare the pain intensity and physical fitness parameters of athletes with and without anterior knee pain.
Material and Methods: This is a comparative cross-sectional study including elite athletes between the ages of 13-19 years. Twenty-one athletes with a VAS score of more than 3 were assigned to the knee pain group, while 19 athletes without knee pain were assigned to the control group. Visual analogue scale, lower extremity functionality scale, lower extremity and trunk flexibility and endurance, dynamic Q angle of both groups were measured and compared.
Results: The mean age was 16.95 ±1.4 in the knee pain group and 16.32 ±1.5 in the pain-free control group. There difference in age, gender, weight, height, or body mass index values between the groups (p>0.05). The number of repeated squats, duration of single leg stance, hip abductor strength and lower extremity functional scale values were statistically lower in the knee pain group (p<0.05). The analyses revealed a negative correlation between anterior knee pain and trunk extensor endurance and lower extremity functions of athletes. Hip endurance was positively correlated with flexibility tests and negatively correlated with the Q angle.
Conclusion: Core endurance is linked to hip endurance and flexibility. An increase was observed in the hip endurance values as the Q angle decreased. Pain intensity and Q angle decreased as lower extremity functionality values increased. To prevent sports injuries in athletics, risk factors for anterior knee pain should be reduced.
Introduction
Athletics is a basic sports branch consisting of running, throwing, jumping, multiple branches, cross country running, mountain and slope running. Elite athletes often encounter sports injuries due to the nature of sports, with knees and hip being the most common areas of injury [1]. While ankle and knee are the frequent sites of injury in running, knee, thigh and lower back injuries are more common in throwing and jumping branches [2]. Anterior knee pain is a typical problem that significantly limits the participation of athletes in sports [3]. In athletes, knee pain is usually caused by overuse injuries. The cause of these injuries is repetitive and excessive stress on the musculoskeletal structure [4]. Knee pain is categorized by its location as anterior, medial, lateral, and posterior. Hoffa syndrome, idiopathic anterior knee pain, infrapatellar bursitis, Osgood-Schlatter disease, osteochondritis dissecans, patellar stress fractures, patellar tendinitis, prepatellar bursitis, quadriceps tendinitis and Sinding-Larsen-Johansson syndrome may occur in the anterior region. Patellofemoral pain syndrome (PFPS) is defined as anterior knee pain associated with these problems [5]. The prevalence of PFPS in athletes is 15%-45%. It is stated in the literature that PFPS is caused by overloading of the joint in those who perform activities such as running, jumping, squatting, and climbing [6]. PFPS has recently been re-defined as pain around or behind the patella aggravated by movements that load the joint during these activities [7]. Factors reported to be associated with PFPS in the literature include quadriceps strength and angle, hip biomechanics, strength, and endurance [8]. Studies have also shown decreased strength of the painful lower extremity of athletes with knee pain. Finoff et al. reported decreased hip strength in individuals with PFPS secondary to pain, stating that this decrease was due to the lower chain mechanism aligned from top to bottom. Based on the lower chain mechanism, it is recently believed that the strength and endurance of the hip muscles have a significant effect on the knee joint, and hip muscle weakness may play a role in the risk of PFPS. In addition, it has been reported in the literature that the loss of gluteus maximus muscle endurance may be associated with the internal rotation of the knee due to its role in the external rotation of the hip [9]. The gluteus maximus, medius, and external rotators are important shock absorbers during running. These muscles should be both strong and flexible in an elite athlete. Quadriceps (Q) overuse, hip muscle weakness, and muscle imbalance are factors that increase knee pain. Decreased hip and knee muscle flexibility, gait abnormalities, exercise mistakes, and changes in the Q angle of athletes pose a potential risk in the knee region [10]. A 2003 study by Ireland et al. showed a lower range of motion of hip abduction and less isometric strength of hip external rotation in individuals with PFPS (11). Another 2015 study showed increased lower extremity chain alignment and improved patella chain movements with the strengthening of the gluteus medius muscle. At the same time, excessive retropatellar joint pressure decreases and knee pain reduces [12]. Despite these studies, there is no clear explanation in the literature about the effect of gluteus medius muscle weakness on PFAS [13]. It has been stated that the muscle strength and endurance of not only the knee and hip regions but also the trunk may be affected due to pain and loss of function in the patellofemoral region. In parallel with this view, Earl and Hoch demonstrated in their study that an increase in core endurance led to a decrease in patellofemoral pain [14]. Later pain-related loss of function also negatively affects flexibility [3,4,9]. Eventually, knee pain can be directly related to the strength, endurance and flexibility of the hip and trunk muscles. It has been reported that future studies should focus on the relationship between knee pain and hip muscle strength [9]. This study compared athletes with and without PFPS for various reasons in terms of pain intensity, endurance, flexibility, and lower extremity functions. The results of this study may highlight risk factors for anterior knee pain in elite athletes and help create correct exercise. Moreover, these results can provide athletes with a valuable roadmap for returning to sports after injury.
Introduction
Athletics is a basic sports branch consisting of running, throwing, jumping, multiple branches, cross country running, mountain and slope running. Elite athletes often encounter sports injuries due to the nature of sports, with knees and hip being the most common areas of injury [1]. While ankle and knee are the frequent sites of injury in running, knee, thigh and lower back injuries are more common in throwing and jumping branches [2]. Anterior knee pain is a typical problem that significantly limits the participation of athletes in sports [3]. In athletes, knee pain is usually caused by overuse injuries. The cause of these injuries is repetitive and excessive stress on the musculoskeletal structure [4]. Knee pain is categorized by its location as anterior, medial, lateral, and posterior. Hoffa syndrome, idiopathic anterior knee pain, infrapatellar bursitis, Osgood-Schlatter disease, osteochondritis dissecans, patellar stress fractures, patellar tendinitis, prepatellar bursitis, quadriceps tendinitis and Sinding-Larsen-Johansson syndrome may occur in the anterior region. Patellofemoral pain syndrome (PFPS) is defined as anterior knee pain associated with these problems [5]. The prevalence of PFPS in athletes is 15%-45%. It is stated in the literature that PFPS is caused by overloading of the joint in those who perform activities such as running, jumping, squatting, and climbing [6]. PFPS has recently been re-defined as pain around or behind the patella aggravated by movements that load the joint during these activities [7]. Factors reported to be associated with PFPS in the literature include quadriceps strength and angle, hip biomechanics, strength, and endurance [8]. Studies have also shown decreased strength of the painful lower extremity of athletes with knee pain. Finoff et al. reported decreased hip strength in individuals with PFPS secondary to pain, stating that this decrease was due to the lower chain mechanism aligned from top to bottom. Based on the lower chain mechanism, it is recently believed that the strength and endurance of the hip muscles have a significant effect on the knee joint, and hip muscle weakness may play a role in the risk of PFPS. In addition, it has been reported in the literature that the loss of gluteus maximus muscle endurance may be associated with the internal rotation of the knee due to its role in the external rotation of the hip [9]. The gluteus maximus, medius, and external rotators are important shock absorbers during running. These muscles should be both strong and flexible in an elite athlete. Quadriceps (Q) overuse, hip muscle weakness, and muscle imbalance are factors that increase knee pain. Decreased hip and knee muscle flexibility, gait abnormalities, exercise mistakes, and changes in the Q angle of athletes pose a potential risk in the knee region [10]. A 2003 study by Ireland et al. showed a lower range of motion of hip abduction and less isometric strength of hip external rotation in individuals with PFPS (11). Another 2015 study showed increased lower extremity chain alignment and improved patella chain movements with the strengthening of the gluteus medius muscle. At the same time, excessive retropatellar joint pressure decreases and knee pain reduces [12]. Despite these studies, there is no clear explanation in the literature about the effect of gluteus medius muscle weakness on PFAS [13]. It has been stated that the muscle strength and endurance of not only the knee and hip regions but also the trunk may be affected due to pain and loss of function in the patellofemoral region. In parallel with this view, Earl and Hoch demonstrated in their study that an increase in core endurance led to a decrease in patellofemoral pain [14]. Later pain-related loss of function also negatively affects flexibility [3,4,9]. Eventually, knee pain can be directly related to the strength, endurance and flexibility of the hip and trunk muscles. It has been reported that future studies should focus on the relationship between knee pain and hip muscle strength [9]. This study compared athletes with and without PFPS for various reasons in terms of pain intensity, endurance, flexibility, and lower extremity functions. The results of this study may highlight risk factors for anterior knee pain in elite athletes and help create correct exercise. Moreover, these results can provide athletes with a valuable roadmap for returning to sports after injury.
Material And Methods
The study including athletes between the ages of 13-19 registered in XXX was a cross-sectional study and was approved by the Scientific Research and Publication Ethics Committee with the XXX file number of XXX Ethics Committee. The study was conducted in accordance with the principles of the Declaration of Helsinki. The inclusion criteria for the study were to be a licensed athlete for at least 1 year, to have no history of orthopedic injury in the past 6 months, and to have a VAS score above 3. A history of surgery in the knee region, a long-term (at least 1 month) camp program, and a lack of motivation were determined as the criteria for exclusion from the study. Athletes who were examined by a sports physician and diagnosed with PFPS were included in the knee pain group, and those without pain were included in the control group. They were assessed by a physiotherapist in XXX units and their measurements were taken. Eight athletes with anterior knee pain with a VAS score of less than 4 were excluded from the study. As a result, 21 athletes were assigned to the knee pain group (KPG), while 19 athletes were assigned to the control group (CG). Athletes were informed about the purpose of the study and signed an informed consent form. Parental consent forms were signed by the families of the athletes under the age of 18 years. Sociodemographic information of the athletes was obtained and the Visual Analogue Scale (VAS), Lower Extremity Functionality Scale (LEFS), lower extremity and trunk flexibility and endurance tests were applied to the athletes, and dynamic Q angle was measured.
Assessments:
Sociodemographic Characteristics
Athletes' gender, age, height, body weight, body mass index (BMI), athletics branch, sports age and number of weekly training sessions were determined. Pain status and duration were questioned.
Dynamic Q angle
When the relevant extremity touches the floor while descending the stairs, the photograph of the athlete was taken from the lateral aspect and the Q angle was measured with a software called DrGoniometer. The measurement was made bilaterally and noted [15].
Lower Extremity and Core Endurance:
3.1. Repeated squat test
The athlete started squatting while in a standing position and continued the repetitive movement without interruption. The number of repetitions performed within 30 seconds (sec) was recorded during the test period [16].
3.2. Single leg stance test: The athlete was asked to stand on one leg, with the other leg flexed, hands placed on the waist, and to maintain this position. The time to stay in this position without a break was noted in sec [16].
3.3. Hip abductor endurance test
The athlete laid on the stretcher in a side-lying position, with the lower leg flexed. The upper leg was abducted. A sandbag corresponding to the calculated weight was tied to the ankle of the abducted leg by calculating 7% of the athlete's body weight. The time of maintaining the position was recorded in sec [17].
3.4. Trunk Flexor Endurance Test
The athlete was asked to stand in a supine position, with the trunk flexed at 60 degrees and the knees at 90 degrees, and to maintain this position. The test was terminated when the desired flexion position was disrupted and the time of maintaining the position was noted in sec [18].
3.5. Trunk Extensor Endurance Test
For Mcgill's extensor endurance test, the athlete laid prone, with the pelvis, hips, and knees supported on the stretcher and the upper body off the edge of the table in a straight or slightly extended position. The athlete was asked to maintain this horizontal position and his/her feet were stabilized by physiotherapist. The time until the athlete could no longer maintain the position was recorded in sec [18].
3.6. Trunk Lateral Flexion Endurance Test
In the side-lying position, the athlete was asked to lift his body on the forearms and toes. The time until the athlete could no longer maintain the position was calculated in sec and noted [18].
3.7. Lower Extremity Functionality Scale (LEFS)
LEFS consists of 20 items and each item is scored on a 5-point scale from 0 (extreme difficulty) to 4 (no difficulty). The total score is 80 points. As the score increases, functionality increases [19].
1. Flexibility
4.1. Sit-and-Reach Test
The table used in the test measures 35 centimeters (cm) in length, 45 cm in width, and 32 cm in height. The upper surface measures 55 cm in length and 45 cm in width. It protrudes 15 cm from the side on which the athlete will rest his/her feet. The upper surface of the table is divided into intervals from 0 cm to 50 cm. The athlete put the soles on the box and bent the torso forward as much as possible by extending the arms forward without bending the knees. She/he stretched and reached along the top of the ruler as far as possible and tried to stay still. The longest distance that the athlete could reach on the ruler was considered the test result [20].
4.2. Trunk Lateral Flexion Flexibility Test
The athlete was asked to stand with the arms extended near the trunk, the feet slightly opened and parallel to each other. The point where the third finger of the hand touched the femur was marked and the athlete was asked to perform trunk lateral flexion as much as she/he could without rotation. The new point where the third finger of the hand touched was marked and the distance between the two points was measured [21].
4.3. Trunk Extension Flexibility Test
The athlete was asked to extend the trunk as much as possible while facing the wall with the trunk in contact with the wall. The distance between the wall and the sternal notch was measured in the first and last test positions and recorded [21].
4.4. Hip Adductor Flexibility Test
The athlete was asked to bring the knees closer to the floor while sitting with the soles of the feet touching each other. The knee-to-floor distance was measured with a tape measure [22].
4.5. Quadriceps and Iliopsoas Flexibility Test
The subject was asked to flex the knee to 90 degrees while lying face down. In this position, she/he was asked to raise the leg from the floor and the knee-to-floor distance was measured with a tape measure [23].
Pain Intensity
According to VAS, pain intensity rated as 1-2-3 indicates mild pain, 3-6 indicates mild-moderate pain, and 7-8-9-10 indicates moderate-severe pain. The athlete was asked to mark the point that best represents his/her level of pain in the past 24 hours on a 10-cm horizontal ruler [24].
Statistical Analysis
SPSS version 22 software package was used for data analysis. Descriptive data were given as mean, standard deviation, minimum, maximum, number, and percentage (%). Categorical data were compared between the groups using the chi-square test. Numerical data were compared using the Mann-Whitney U test. Spearman's rho test was used for correlation analyses. Values of p<0>
Results
A total of 40 elite athletes participated in the study, 20 from the athletics branch, 10 from the jumping branch, 9 from the running branch, and 1 from the multi-branch. The mean age of the participants, of whom 28 were male and 12 were female, was 16.65 ± 1.5 years. The mean sports age was 6.33 ± 2.2 years. The mean number of weekly training sessions was 5.95 + 0.3 days. The mean height of the athletes was 173.43 ± 9.2 cm, the mean body weight was 66.60 ± 12.1 kg, and the mean BMI was 21.87 ± 2.3 kg/m2. The comparison of the demographic characteristics of the groups showed no significant difference (p>0.05). While 21 (52.5%) of the athletes had anterior knee pain, 19 (47.5%) had no pain. The mean duration of pain was approximately 44+3.2 days in the knee pain group. The physical fitness parameters of the athletes are summarized in Table 1.
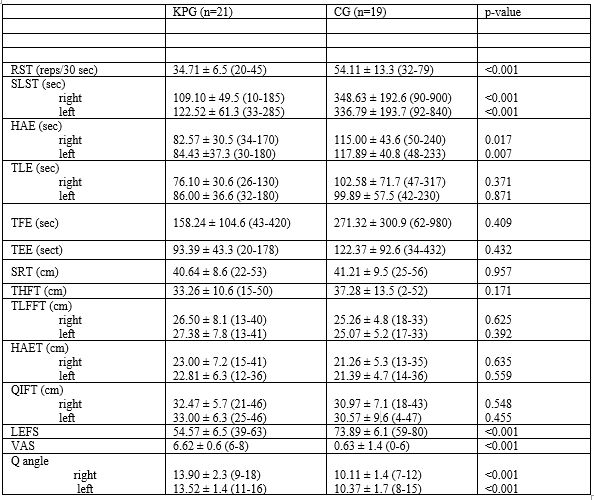
The number of repeated squats, duration of single-leg stance, and hip abductor endurance values were statistically lower in the knee pain group (p<0>0.05). The comparison of the groups in terms of flexibility values revealed no significant difference (p>0.05). The lower extremity functionality scale (LEFS) scores were lower in the knee pain group compared to the control group (p<0>
Discussion
In this study on elite athletes, the pain intensity, endurance, flexibility, and functionality of athletes diagnosed with PFPS were compared with the parameters of athletes without pain. According to the results, the endurance values of the hip muscles were directly associated with the flexibility of the hip and knee muscles. Moreover, the decrease in the dynamic Q angle showed a positive correlation with the endurance values of the hip region. The core region covers the area between the base of the rib cage and the top of the hip bone when viewed from the opposite side. It is the general nomenclature of the waist, abdominal and hip muscles that combines the body and skeleton. The strength of this region provides an advantage to the athletes [25]. Studies in the literature have reported weakness and shortness of the hip and knee regions as risk factors for core endurance loss [26]. In parallel with the literature, the results of our study showed that the athletes with high hip flexibility and endurance scores also had high core endurance scores. In 2018, Ozan et al. investigated the effects of static and dynamic core exercises added to football training programs [27]. They reported that core exercises added to the training program increased the trunk flexion and extension endurance values of the football players, with no significant increase in the lateral trunk endurance values. They emphasized that core exercises should be included in football training programs. Unlike this conclusion, we found an association between trunk endurance scores of three aspects (flexion-extension-lateral) and lower extremity flexibility and endurance scores. The inclusion of athletes from different sports branches may be the reason for these two different results. Anterior knee pain due to various reasons can cause loss of strength and avoidance of movement [28]. A study comparing PFPS and healthy people found that the lateral trunk endurance of the pain group was 24% less than that of the control group [29]. This result was interpreted by the researchers as altered lower extremity biomechanics by anterior knee pain. Considering the kinematic chain, this is in line with our hypothesis. We observed more knee and hip strength loss in athletes with high VAS values. Another study conducted in 2018 performed EMG on participants during the lateral trunk endurance test. The results objectively demonstrated the link between the lateral trunk muscles and the gluteus medius muscle [5]. Utting et al. examined the coactivation of the gluteus medius and adductor longus muscles and compared the anterior knee pain group with the control group. The results of the study revealed lower coactivation in the pain group than in the control group [30]. Both studies have emphasized the negative effect of knee pain on hip muscles. Our comparison of the hip and core endurance values of the study groups showed no significant difference. Since the loss in the already strong muscles of the athletes was not meaningful enough to disrupt the lower chain mechanism, PFPS only affected the knee and surrounding tissues locally. The significant difference between the repeated squat and single-leg stance scores of the groups also clarified this result. Given the literature, the Q angle is indicated as an important risk factor for PFPS. A possible increase in this angle adversely affects pelvic and hip mechanics. The Q angle of athletes with high athletic performance is measured to be less compared to other athletes [31]. Q angle is frequently used not only in sports activities but also in our daily life. In contrast to the static Q angle, the dynamic Q angle is more associated with functionality and balance [32]. According to our results, the dynamic Q angle was correlated with pain, lateral trunk endurance, and flexibility. Besides these, it also affects the static and dynamic balance. Brezzo et al. stated that the Q angle should be 10 degrees or less for the quadriceps to exert a strong pull [33]. The dynamic Q angles of athletes in the control group are in parallel with this interpretation. The dynamic Q angles of the athletes without pain were statistically lower than those of the pain group. Quadriceps with a good pulling force both reduces the Q angle and helps extend the H muscle. When the Q angle increases due to PFPS, the patella is medially displaced. This change may be masked in the acute period, but if the problem becomes chronic, disruptions are observed in the lower chain mechanism [34]. The mean pain duration in the knee pain group was one and a half months. Although no loss of endurance was observed in the knee pain group in this short period of time, the Q angle was adversely affected by pain. During lower extremity movements, the core region moves involuntarily [35]. The core region transmits its force to the lower extremities by force transmission. Based on this information, the correlation between extensor and lateral trunk endurance and hip endurance demonstrated by our results is as expected. However, the absence of a similar correlation with flexor trunk endurance indicates that the same transmission does not occur in all movements. It has been stated in the literature that the link between strength, endurance, and flexibility should not be ignored for force transmission [36,37]. While a 2020 study reported no relationship between endurance and muscle strength and flexibility, the literature is divided into two in this respect. There are also studies showing no correlation between strength and endurance and flexibility [38,39]. According to our results, lower extremity flexibility and Q angle are correlated. We evaluated anterior knee pain intensity with VAS and found that pain was correlated with lower extremity functionality. PFPS-related pain causes reciprocal inhibition by reducing the number of motor units in the muscles, restricting the use of the knee, and reducing functionality [40]. While the correlation between pain and functionality in our results was predictable, it was unexpected that the Q angle was only correlated with hip abductor endurance among our parameters. Based on this result, we recommend paying attention to hip muscle strengthening in athletic training. In line with the correlation of pain intensity with hip endurance and Q angle, we are of the opinion that kinematic chain problems can be masked by compensatory mechanisms in athletes with strong muscles. Continuing training regardless of the knee pain felt can pave the way for serious sports injuries. Furtermore, it can negatively affect the hip and core regions. For this reason, knee pain should be considered by physiotherapists and the athlete should be referred to a sports physician after assessment. Thus, most serious problems can be prevented before injury occurs. Risk factors for anterior knee pain should be eliminated and athletes and trainers should be informed about this. Our study has some limitations. The small number of athletes included in the study and the study planning for a single sports branch are among the limitations.
Conclusions
In conclusion, PFPS is associated with hip endurance, functionality, and Q angle. The more pain an athlete with a diagnosis of PFPS feels, the less hip endurance values and lower extremity functionality he/she has. In order to increase performance and prevent injuries in athletes, risk factors for anterior knee pain should be reduced. Strength, endurance, and flexibility values should be measured with objective methods at regular intervals, and the Q angle should be followed up.
References
- Teixeira RN, Lunardi A, da Silva RA, Lopes AD, Carvalho CR. (2016). Prevalence of musculoskeletal pain in marathon runners who compete at the elite level. International Journal of Sports Physical Therapy. 11(1):126.
View at Publisher | View at Google Scholar - Lundberg Zachrisson A, Desai P, Karlsson J, Johanesson E, Grau S. (2018). Overuse injuries in Swedish elite athletics–a study protocol for a prospective multifactorial cohort study. BMC Musculoskeletal Disorders. 19(1):1-2.
View at Publisher | View at Google Scholar - LaBella CR, Huxford MR, Smith TL, Cartland J. (2009). Preseason neuromuscular exercise program reduces sports-related knee pain in female adolescent athletes. Clinical pediatrics. 48(3):327-330.
View at Publisher | View at Google Scholar - Patel DR, Villalobos A.(2017). Evaluation and management of knee pain in young athletes: overuse injuries of the knee. Translational Pediatrics. 6(3):190.
View at Publisher | View at Google Scholar - Earl-Boehm JE, Bolgla LA, Emory C, Hamstra-Wright KL, Tarima S, Ferber R. (2018). Treatment success of hip and core or knee strengthening for patellofemoral pain: development of clinical prediction rules. Journal of Athletic Training. 53(6):545-52.
View at Publisher | View at Google Scholar - Glaviano NR, Bazett-Jones DM, Boling MC. (2022). Pain severity during functional activities in individuals with patellofemoral pain: A systematic review with meta-analysis. J Sci Med Sport. 25(5):399-406.
View at Publisher | View at Google Scholar - Petersen W, Rembitzki I, Liebau C. Patellofemoral pain in athletes. Open Access Journal of Sports Medicine. 2017; 8:143.
View at Publisher | View at Google Scholar - Herbst KA, Barber Foss KD, Fader L, Hewett TE, Witvrouw E, Stanfield D, et al. (2015). Hip strength is greater in athletes who subsequently develop patellofemoral pain. The American Journal of Sports Medicine. 43(11):2747-2752.
View at Publisher | View at Google Scholar - Finnoff JT, Hall MM, Kyle K, Krause DA, Lai J, Smith J. (2011). Hip strength and knee pain in high school runners: a prospective study. PM&R. 2011; 3(9):792-801.
View at Publisher | View at Google Scholar - Abdallah AA, Mohamed NA, Hegazy MA. (2019). A comparative study of core musculature endurance and strength between soccer players with and without lower extremity sprain and strain injury. International Journal of Sports Physical Therapy. 14(4):525.
View at Publisher | View at Google Scholar - Ireland ML, Willson JD, Ballantyne BT, Davis IM. (2003). Hip strength in females with and without patellofemoral pain. Journal of Orthopaedic & Sports Physical Therapy. 33(11):671-676.
View at Publisher | View at Google Scholar - Mahmoud WS, Kamel EM. (2015). The effect of additional balance training program to gluteus medius strengthening exercises on patellofemoral pain syndrome. International Journal of Therapies and Rehabilitation Research. 4(2):7.
View at Publisher | View at Google Scholar - Motealleh A, Gheysari E, Shokri E, Sobhani S. The immediate effect of lumbopelvic manipulation on EMG of vasti and gluteus medius in athletes with patellofemoral pain syndrome: a randomized controlled trial. Manual Therapy. 2016; 22:16-21.
View at Publisher | View at Google Scholar - Earl JE, Hoch AZ. (2011). A proximal strengthening program improves pain, function, and biomechanics in women with patellofemoral pain syndrome. The American Journal of Sports Medicine. 39(1):154-163.
View at Publisher | View at Google Scholar - Vercelli S, Sartorio F, Bravini E, Ferriero G. (2017). DrGoniometer: a reliable smartphone app for joint angle measurement. British Journal of Sports Medicine. 51(23):1703-1704.
View at Publisher | View at Google Scholar - Liebenson C. (2000). Documentation of Physical Capacity: Its Purpose in Rehabilitation. Dynamic Chiropractic. 18(8).
View at Publisher | View at Google Scholar - Van Cant J, Dumont G, Pitance L, Demoulin C, Feipel V. (2016). Test-retest reliability of two clinical tests for the assessment of hip abductor endurance in healthy females. International Journal of Sports Physical Therapy. 11(1):24.
View at Publisher | View at Google Scholar - McGill SM, Childs A, Liebenson C. (1999). Endurance times for low back stabilization exercises: clinical targets for testing and training from a normal database. Arch Phys Med Rehabil. 80(8):941-944
View at Publisher | View at Google Scholar - Binkley JM, Stratford PW, Lott SA, Riddle DL. (1999). North American Orthopaedic Rehabilitation Research Network. The Lower Extremity Functional Scale (LEFS): scale development, measurement properties, and clinical application. Physical Therapy. 79(4):371-383.
View at Publisher | View at Google Scholar - Kirmizigil B, Ozcaldiran B, Colakoglu M. (2014). Effects of three different stretching techniques on vertical jumping performance. The Journal of Strength & Conditioning Research. 28(5):1263-1271.
View at Publisher | View at Google Scholar - Otman AS, Demirel H, Sade A. (1998). Tedavi hareketlerinde temel değerlendirme prensipleri. 2. baskı. Sinem ofset Ltd. Şti. Ankara. 66-68.
View at Publisher | View at Google Scholar - Seiberl W, Power GA, Herzog W, Hahn D. (2015). The stretch‐shortening cycle (SSC) revisited: residual force enhancement contributes to increased performance during fast SSC s of human m. adductor pollicis. Physiological Reports. 3(5):12401.
View at Publisher | View at Google Scholar - Franklin B, Whaley M, Howley E. (2000). American College of Sports Medicine. Guidelines for exercise testing and prescription. ACSM’s guidelines for exercise testing. Philadelphia: Lea & Febiger.
View at Publisher | View at Google Scholar - Wong DL, Baker CM. (1988). Pain in children: comparison of assessment scales. Pediatr Nurs. 14(1):9-17.
View at Publisher | View at Google Scholar - Cugliari G, Boccia G. (2017). Core muscle activation in suspension training exercises. Journal of human kinetics. 56(1):61-71.
View at Publisher | View at Google Scholar - De Ridder R, Witvrouw E, Dolphens M, Roosen P, Van Ginckel A. (2017). Hip strength as an intrinsic risk factor for lateral ankle sprains in youth soccer players: a 3-season prospective study. The American Journal of Sports Medicine. 45(2):410-416.
View at Publisher | View at Google Scholar - Sever O, Zorba E. (2018). Comparison of effect of static and dynamic core exercises on speed and agility performance in soccer players. Isokinetics and Exercise Science. 26(1):29-36.
View at Publisher | View at Google Scholar - Şen M, Çetin S, Ece C, Aydogan A, Çetin HN. (2019). Comparison of Quadriceps Q-Angle values of soccer players and wrestlers. Journal of Education and Training Studies. 7(7):95-101.
View at Publisher | View at Google Scholar - Willson JD, Binder-Macleod S, Davis IS. (2008). Lower extremity jumping mechanics of female athletes with and without patellofemoral pain before and after exertion. The American Journal of Sports Medicine. 2008; 36(8):1587-1596.
View at Publisher | View at Google Scholar - Utting MR, Davies G, Newman JH.(2005). Is anterior knee pain a predisposing factor to patellofemoral osteoarthritis? The Knee. 12(5):362-365.
View at Publisher | View at Google Scholar - Yılmaz A, Kabadayı M, Mayda M, Cavusoglu G, Tasmektepligi M. (2017). Analysis of Q angle values of female athletes from different branches. Sci Mov Heal. 17(2):141-146.
View at Publisher | View at Google Scholar - Skouras AZ, Kanellopoulos AK, Stasi S, Triantafyllou A, Koulouvaris P, Papagiannis G, et al. (2022). Clinical Significance of the Static and Dynamic Q-angle. Cureus. 14(5): 24911.
View at Publisher | View at Google Scholar - Di Brezzo R, Frot L, Hall K. (1996). The Relationship With Selected Dynamic Performance Variable In Women. 66-70.
View at Publisher | View at Google Scholar - Lee J, Lee H, Lee W. (2014). Effect of weight-bearing therapeutic exercise on the q-angle and muscle activity onset times of elite athletes with patellofemoral pain syndrome: a randomized controlled trial. Journal of Physical Therapy Science. 26(7):989-92.
View at Publisher | View at Google Scholar - Arora C, Singh P, Varghese V. (2021). Biomechanics of core musculature on upper extremity performance in basketball players. Journal of Bodywork and Movement Therapies. 2021 ;27:127-33.
View at Publisher | View at Google Scholar - Başkurt F, Ercan S, Başkurt Z. Yaşlı Kadınlarda Alt Ekstremite Kas Kuvvetinin Denge ve Alt Ektremite Fonksiyonları ile İlişkisi. Spor Hekimligi Dergisi/Turkish Journal of Sports Medicine. 2018; 53(1).
View at Publisher | View at Google Scholar - Cursino MP, Marques AE, Quatrochi HC, Navega FR, Pedroni CR. (2016). Correlation between strength and flexibility of knee flexors and extensors muscles in youth soccer players. Manual Therapy, Posturology & Rehabilitation Journal. 1-5.
View at Publisher | View at Google Scholar - Akınoğlu B, Kocahan T, Ünüvar E, Eroğlu I, Hasanoglu A. (2020). Sporcularda Gövde Kas Kuvveti İle Otur-Uzan Esnekliği Arasındaki İlişkinin İncelenmesi. Turkiye Klinikleri Journal Of Sports Sciences.12(1).
View at Publisher | View at Google Scholar - Shariat A, Lam ET, Shaw BS, Shaw I, Kargarfard M, Sangelaji B. (2017). Impact of back squat training intensity on strength and flexibility of hamstring muscle group. Journal of Back and Musculoskeletal Rehabilitation. 30(3):641-647.
View at Publisher | View at Google Scholar - Siqueira AP, Beraldo LM, Krueger E, Ulbricht L. (2018). Reduction in knee pain symptoms in athletes using an acupuncture protocol. Acta Ortopedica Brasileira. 26:418-422.
View at Publisher | View at Google Scholar
