

Research article | DOI: https://doi.org/10.31579/2834-5126/01
Etiological Factors and Short-Term Outcome of Relaparotomy Involving Gastrointestinal Surgery at Mbarara Regional Referral Hospital
- Ali mohamed ali 1*
1Mr. Deus twesigye mbchb (must), mmed (must).
2Mr. David mutiibwa mbchb (must), mmed (must).
*Corresponding Author: Ali mohamed ali
Citation: Ali mohamed ali. (2022). A research dissertation submitted to the faculty of medicine in partial fulfilment of the requirements for the award of master’s degree of medicine in surgery of mbarara university of science and technology (must). Clinical trials and clinical research. 1(1); doi: 10.31579/2834-5126/01
Copyright: © 2022 Ali mohamed ali, this is an open access article distributed under the creative common’s attribution license, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 07 September 2022 | Accepted: 09 September 2022 | Published: 19 September 2022
Keywords: re-laparotomy; anastomotic leak; intra-abdominal sepsis
Abstract
Background: An increasing number of patients undergo repeat abdominal surgery during their lifetime often, due to complications following initial laparotomy, and if not corrected, complications can lead to high morbidity and mortality. Our objective was to determine the clinical characteristics, etiological factors and outcome of relaparotomy.
Methods: A prospective study of 54 patients who underwent relaparatomy at Mbarara Regional Referral Hospital in Mbarara, Uganda between the months of October 2018 to May 2019 was conducted. Data including demographics, initial diagnosis, initial surgery, indication of relaparotomy, time interval between primary surgery and re-operation and outcome was collected and analyzed.
Results: The incidence of relaparotomy was 19.3%. There were 31 males and 23 females, the M:F ratio of 1.3:1 The most commonly affected age group was between 15-45 years (46.3%) with mean age 27.4(SD 21.4). The most common indication was anastomotic leak 18(33.3%) and burst abdomen 15(27.8%). The mean duration between the primary surgery and relaparotomy was 9.4 days. The majority of relaparotomies (66.7%) had prior lower gastrointestinal surgery. About one-third (n-16 29.6%) required intensive care postoperatively. The overall mortality rate was 37.0 % mostly commonly due to septicemia (60.0%). The mean duration of hospital stay was 30days and wound infection (55.6%) was most common postoperative complications overalls.
Conclusion: Relaparatomy is common among patients undergoing gastrointestinal surgery and is usually secondary to anastomotic leak and is coupled with intra-abdominal sepsis, which leads to high morbidity and mortality
Background
Early recognition and treatment of postoperative complications which can necessitate surgical reoperation is important to achieve a successful outcome(Himpens et al., 2006).
Re-operative abdominal surgery (relaparotomy) means an unplanned re-intervention carried out during the immediate postoperative period after laparotomy and causally related to first operation within 60 days (Hyman, 2009). If its performed within 21 days after the first operation it is known as “early relaparotomy”(Unalp et al., 2006). .
An increasing number of patients undergo abdominal surgery multiple times during their lifetime, As life expectancy increases and advances in surgical and medical care continue to allow more surgical options for critically ill patients, this is expected to increase even further (Kwok et al., 2011). Today, as many as 40 to 66 % of elective laparotomies in general surgery are reoperations (ten Broek et al., 2013, Erdem et al., 2013).
The risk for bowel injuries also increases with each consecutive laparotomy and can be as high as 50 % (ten Broek et al., 2014).It is important to understand which patients may be at high risk for repeat surgery and allow for optimal resource utilization to reduce morbidity and mortality of re-exploration.
The incidence of relaparotomy in literature ranges from 0.5 -15% in various reported studies(Unalp et al., 2006, Koirala et al., 2015).The highest incidence was seen in gastrointestinal surgeries, while lowest in vascular surgeries(Unalp et al., 2006).
Some of the important indications of relaparotomy are anastomotic leak, septic peritonitis, intestinal obstruction, burst abdomen, intestinal perforation and haemorrhage (Koirala et al., 2015). Mortality after relaparotomy ranges from 24 to 71 %(Mulier et al., 2003).
Measures which can be carried out to reduce the incidence of re-laparotomy are proper pre-operative work up and stabilization, supportive antibiotics and proper antiseptics techniques, improved fluid and electrolyte management, proper surgical techniques, secured haemostasis, complete exploration and appropriate drainage(Patel et al., 2016)
Methodology Study Design
This was a prospective cohort study among patients who underwent abdominal re-exploration starting from October 2018 to May 2019 and followed up from the period of relaparotomy, within 30 days of hospital stay, or to discharge from the ward or another relaparotomy or death at Mbarara Regional Referral Hospital, Southwestern Uganda
Sample size calculation
Sample size was calculated using (Kish 1965).Prevalence used was 2.8
participants enrollment and eligibility criteria
All patients who underwent gastrointestinal surgery for various indications and required re exploration following laparotomy,both gender and all ages(emergency, elective)were recruited and those who had relaparotomy in other centers and referred and all obstetrics and gynaecological patients who were in need of re-exploration were excluded.
Study procedures
All patients who had laparotomy presenting with complications requiring re-exploration as emergency or those admitted for elective surgery starting from October 2018 to May 2019 and consent or assent were recruited in the study. Patients were assessed by the principal investigator through history and physical examinations, including vital signs and laboratory investigations (CBC and serum electrolytes) was done, and if imaging is indicated as per the complication postoperatively were done where necessary (abdominal x-ray and U/S)Administration of questionnaire was done before the second laparotomy after informed consent by principal investigator and a trained research assistant. Patients were assigned a study number at enrolment and this served as their unique identifiers throughout the study period the questionnaire was used to enter information for each patient capturing the different parameters based on the conceptual framework All the decision on diagnosis and management, re-exploration or conservative was made by a General and pediatric surgeons (pediatric patients for re-exploration) as defined by the specific international standards
Statistical analysis
We summarised baseline characteristics as means (standard deviations) and frequencies. Our primary outcomes of interest were wound infection,anastomotic leak,relaparatomy,intra-abdominal abscess and death. 2nd or 3rd relaparatomy,intra-abdominal abscess,long hospital stay and death. Other co variables age and gender. Analysis was done using STATA version 15.Data Presentation: descriptive statistics was done using univariate analysis to describe distribution of variables such as central tendency mean.Univariate analysis was used to determine frequencies and proportions for categorical variables. Relationships between two variables were assessed using bivariate analysis including cross tabulations and chi square testing.Data was summarised in one-way tables, pie chart and graphs (bar graph).
Ethics
The study participants gave written informed consent or assent. Study protocols and procedures were reviewed and approved by faculty of medicine research committee (Ref.DMS 6), Mbarara University of Science and Technology research commitee (Ref. MUREC 1/7) and Mbarara Regional Referral Hospital before study commencement.
Ethics
The study participants gave written informed consent or assent. Study protocols and procedures were reviewed and approved by faculty of medicine research committee (Ref.DMS 6), Mbarara University of Science and Technology research commitee (Ref. MUREC 1/7) and Mbarara Regional Referral Hospital before study commencement.
Results
A total of 54 patients were recruited in the study, The mean age was 27.4(SD 21.34) and range 3days-68years.Among the 54 patients 31(57.4%) were male and 23(42.6%) were female. The M:F ratio was 1.3:1. The frequency of relaparotomy was highest in 14-45 years age group (46.3%) followed infants less than or equal to 1 year (24.1%).) About one quarter (n=12(22.2%) were from Mbarara,and the other major region being Isingiro (n=12(22.2%),followed by Rakai, Masaka and Fortporto. Table 1 below shows additional demographic characteristics.
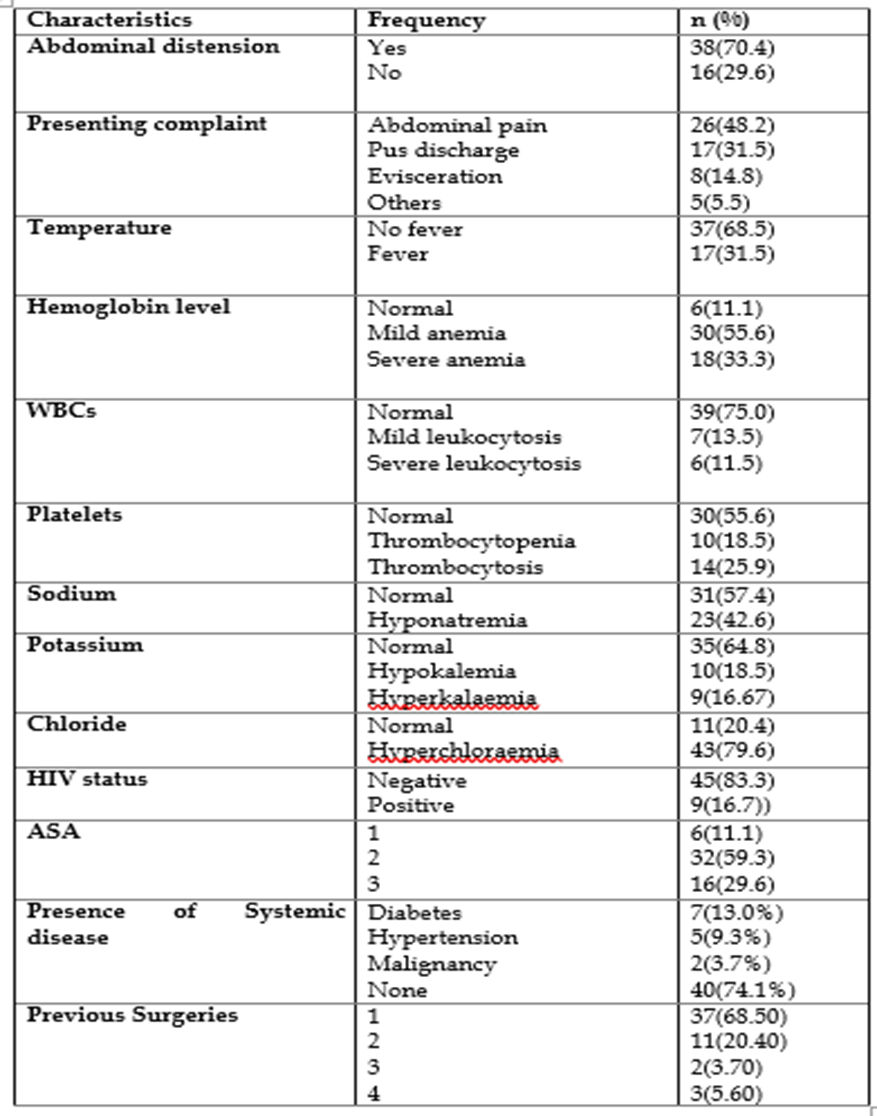
Table 2: Clinical Characteristics
Clinical Characteristics of The Study Populations.
Abdominal distension and abdominal pain were the most common presenting symptoms. The majority of patients presented with multiple symptoms. Seventeen patients (31.5%) had systemic diseases such as diabetes (n=7(41.2%%) in hypertension (n=5, (29.1%) and malignancy (n=2 (11.8%) Table 2 below describes other clinical presentations the of study cohort.
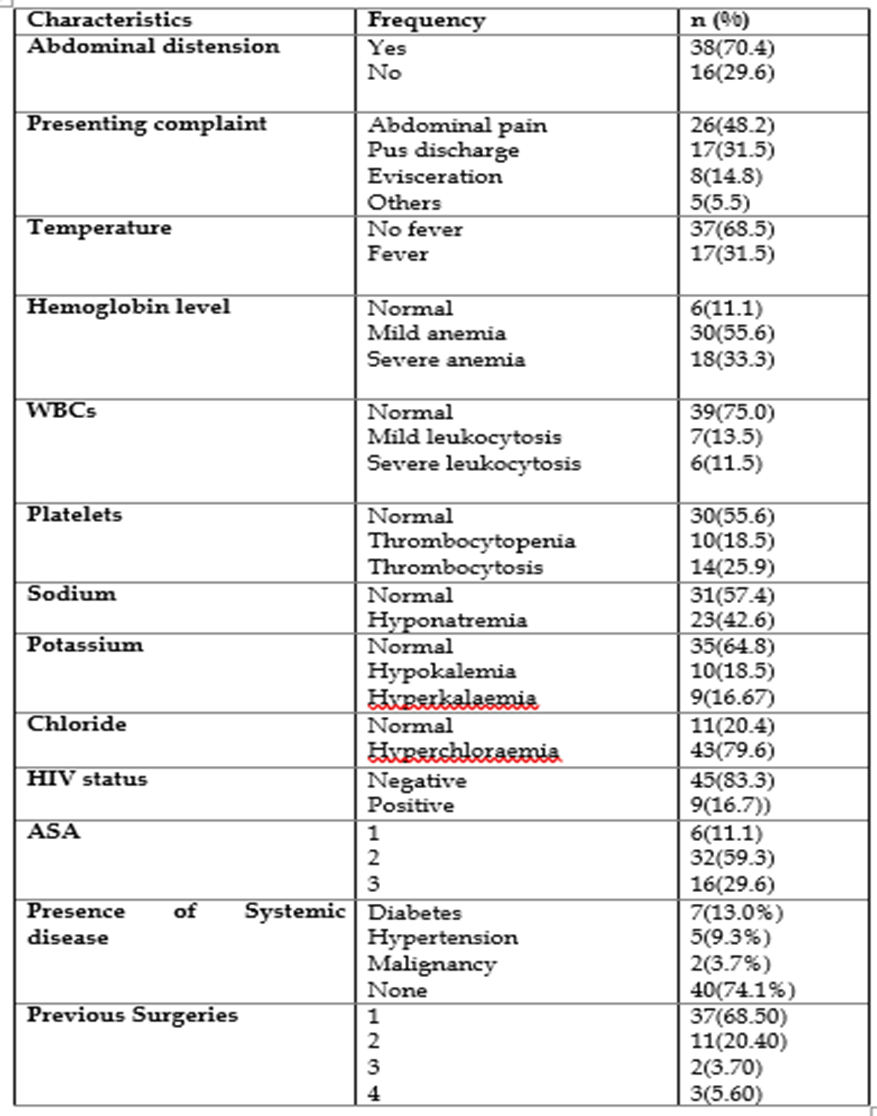
Table 2: Clinical Characteristics
Etiological factors of relaparatomy
| Frequency | Percent (%) |
Presumptive diagnosis | Peritonitis PUD Perforation Intestinal Obstruction Others | 31(57.4) 13(24.1) 8(14.8) 2(3.7) |
Urgency of surgery | Emergency Elective | 53(98.1) 1(1.9) |
Number of relaparotomy | 1st 2nd 3rd 4th | 27(50.0) 16(29.6) 6(11.1) 5(9.3) |
Indication of relaparotomy | Anastomotic leakage Intestinal obstruction Other peritonitis Burst abdomen | 18(33.3) 8(14.8) 13(24.1) 15(27.8) |
Initial Procedure | Resection and anastomosis Graham’s Patch Colostomy/Ileostomy Others
| 23(42.6) 7(13.0) 7(13.0) 17(31.5)
|
Location of index operation | Upper GIT Lower GIT Abdominal wall Hepatobiliary | 13(24.1) 36(66.7) 3(5.6) 2(3.7) |
Duration of the surgery(hrs)
| 1-2 3-4 ≥4
| 21(39.0). 27(50.0) 6(11.0)
|
Time interval
Cadre of surgeon | 1-48hrs 2-7 days >7 days 40-60 days
SHO 1st SHO 2nd SHO 3rd Qualified surgeon
| 2(3.7) 30(55.6) 15(27.8) 7(13.0)
4(7.4) 25(46.3) 7(13.0) 18(33.3) |
Table 3: primary indication diagnosis, urgency and indication of relaparotomy
Acute peritonitis of various causes was the most common initial indication for the surgery, was peritonitis was present in (57.4%), followed by PUD perforation (24.1%) and intestinal obstruction (14.8%). Ninety-eight percent of the cases were emergency and only one case was classified as elective (1.9%). The lower GIT (66.7%) was the most common site requiring relaparotomy followed by the upper GIT (24.1%). There were only 2 hepatobiliary cases which was due to biliary atresia (3.7%). The initial operation was usually due to either bowel resection with primary anastomosis (n=23, 42.6%) or closure of gastric perforation(n=7,13.0%) Anastomotic leakage (n=15, 27.8%) was the most common cause of relaparotomy followed by burst abdomen (n=7, 13.0%) The mean duration between first laparotomy and relaparotomy was 9.3±7.45days (See table 3 above for further details).
| Etiology | n(%) |
Presence of peritonitis | Inflammation Perforation Ischemic/Necrosis Anastomotic Leakage | 22(40.7) 9(16.7) 5(9.3) 18(33.3) |
Table 4: Presence of Peritonitis
The most common causes of postoperative peritonitis were inflammation (n=2 (40.7%) followed by anastomotic leak (n=18, 33.3%), There were several cases missed perforation (n=9, 16.7%) during initial surgery causing fecal peritonitis and perforations due to peptic ulcer disease (n=5 pre-pyloric and n=2 duodenal)
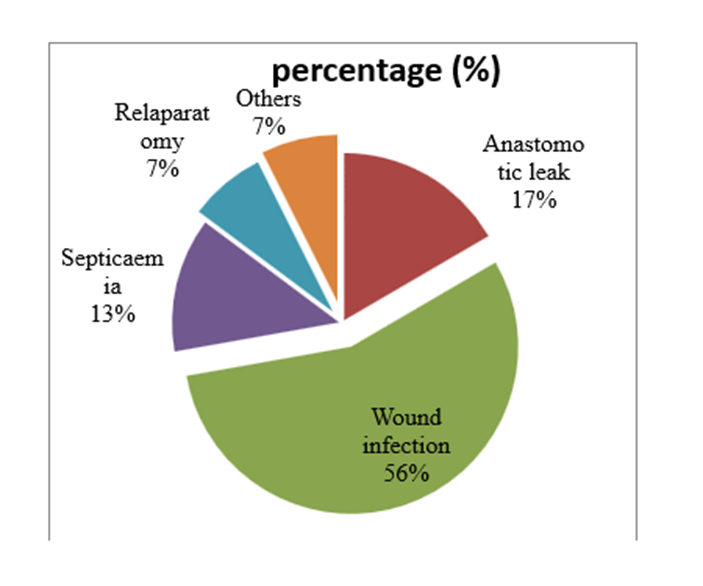
Figure 1: Showing Postoperative Complications
Figure 3: above shows reoperations are associated with high rate of complications such as wound infection(n=30,55.6%), anastomotic leak(n=9,16.6%),septicaemia(n=7,13.0%),relaparotomy(n=4, 7.4%)and others (n=4,7.4%) including wasting, decubitus ulcers and wound dehiscence
The short-term treatment outcome following relaparotomy in gastrointestinal disease at MRRH
Outcome |
| n(%) |
Length of hospital stay
Duration
Relaparotomy No. of Relaps
ICU admission
Death(Mortality)
Gender distribution in relation to Mortality
Cause of death
Mortality in relation to No.of Relaps
Outcome of relaparotomy
| 1 week 2 weeks Upto 30 days >30 days
1st 2nd >3
Yes No
No Yes
Female Male
Septicaemia/septicshock Cardiopulmonaryarrest Malignancy Others
1s t 2nd 3rd & more
Discharge Death | 9(17.0) 13(24.5) 27(50.9) 4(7.6)
12(23.1) 21(40.4) 19(36.5)
16(296) 38(70.4)
34(63.0) 20(37.0)
7(35.0) 13(65.0)
12(60.0) 2(10.0) 2(10.0) 4(20.0)
2(10) 7(35) 11(55%)
34(63.0) 20(37.0) |
Table 5: Showing short term outcome of relaparatomy
Table 5 above shows short-term outcome, -Many patients had a length of stay hospital up to 30 days (n= 27(50.9%) and four patients (7.6%) had stayed for more than 30 days. Forty percent (,n=21) of patients requiring second relap while over another one-third (n=19) multiples relaps 3 and more,which increased mortality significantly from 10
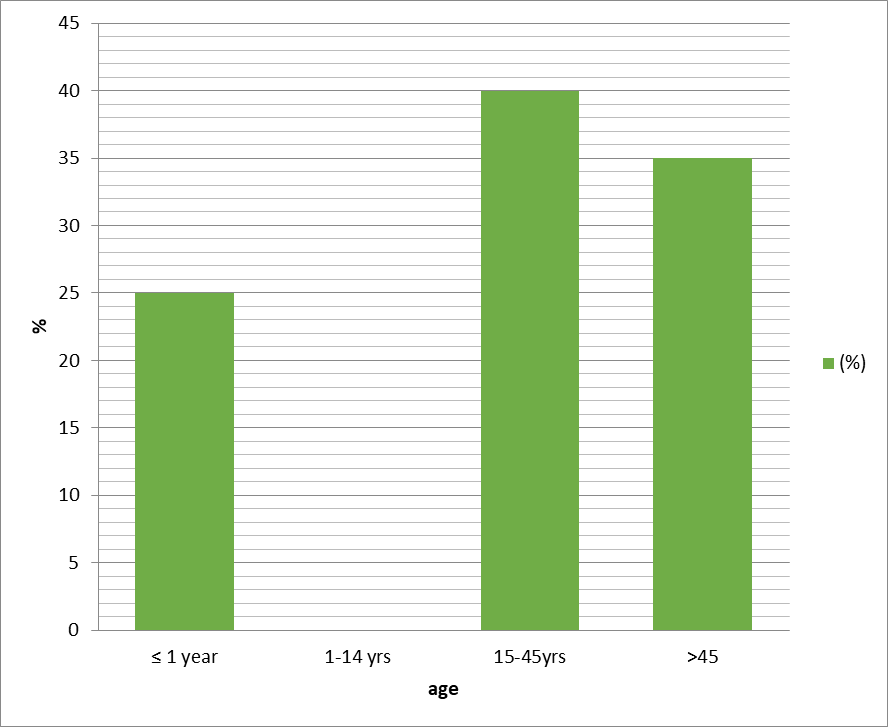
Figure 2: Age distribution in Relation to Mortality.
The figure above shows highest mortality in age group (15-45) biological factors associated with Mortality
| Variable | n(%) | Chi |
Age ≤1yrs 1-14yrs 15-45yrs >45yrs |
5(25.0) 0(0.0) 8(40.0) 7(35.0) |
0.223
|
Gender Male Female |
13(65.0) 7(35.0) | 0.387
|
ASA 1&2 3 & > | 15(75.0) 5(25.0) | 0.568
|
P.peritonitis No Yes
|
6(30.0) 14(70.0) |
0.151
|
Other peritonitis No Yes |
14(70.0) 6(30.0) | 0.690
|
Duration from last surgery <72hrs> >72hrs
|
3(15.0) 17(85.0)
|
0.733
|
Resection and anastomosis No Yes |
12(60.0) 8(40.0) |
0.768
|
Anastomotic leakage No Yes
|
11(55.5) 9(45.0)
|
0.030
|
Number of Relaps ≤2 >2 |
9(45.0) 11(55.0)
|
0.029 |
Table 6: Association of mortality to some selected patients factors (Chi square analysis)
Factors listed above (table 6) such as age, gender, ASA, primary peritonitis, duration from last surgery, resection and anastomosis, anastomotic leak and number of relaps were checked if any Factors listed above (table 6) such as age,gender, ASA, primary peritonitis, duration from last surgery, resection and anastomosis, anastomotic leak and number of relaps were checked if any is associated to mortality using Chi square which found no association except anastomotic leak and number of relaparatomy. Anastomotic leak a P value of 0.030 and the number of relaparotomies had P value of 0.029 which was statistically significant. The variable age had a P value of 0.223, which was statistically insignificant but clinically significant, with high mortality rate in extreme of ages less or equal to one year and above 45 years. Other variables were statistically insignificant.
Factors listed above (table 6) such as age, gender, ASA, primary peritonitis, duration from last surgery, resection and anastomosis, anastomotic leak and number of relaps were checked if any Factors listed above (table 6) such as age,gender, ASA, primary peritonitis, duration from last surgery, resection and anastomosis, anastomotic leak and number of relaps were checked if any is associated to mortality using Chi square which found no association except anastomotic leak and number of relaparatomy. Anastomotic leak a P value of 0.030 and the number of relaparotomies had P value of 0.029 which was statistically significant. The variable age had a P value of 0.223, which was statistically insignificant but clinically significant, with high mortality rate in extreme of ages less or equal to one year and above 45 years. Other variables were statistically insignificant.
Factors listed above (table 6) such as age, gender, ASA, primary peritonitis, duration from last surgery, resection and anastomosis, anastomotic leak and number of relaps were checked if any Factors listed above (table 6) such as age,gender, ASA, primary peritonitis, duration from last surgery, resection and anastomosis, anastomotic leak and number of relaps were checked if any is associated to mortality using Chi square which found no association except anastomotic leak and number of relaparatomy. Anastomotic leak a P value of 0.030 and the number of relaparotomies had P value of 0.029 which was statistically significant. The variable age had a P value of 0.223, which was statistically insignificant but clinically significant, with high mortality rate in extreme of ages less or equal to one year and above 45 years. Other variables were statistically insignificant.
Factors listed above (table 6) such as age, gender, ASA, primary peritonitis, duration from last surgery, resection and anastomosis, anastomotic leak and number of relaps were checked if any Factors listed above (table 6) such as age,gender, ASA, primary peritonitis, duration from last surgery, resection and anastomosis, anastomotic leak and number of relaps were checked if any is associated to mortality using Chi square which found no association except anastomotic leak and number of relaparatomy. Anastomotic leak a P value of 0.030 and the number of relaparotomies had P value of 0.029 which was statistically significant. The variable age had a P value of 0.223, which was statistically insignificant but clinically significant, with high mortality rate in extreme of ages less or equal to one year and above 45 years. Other variables were statistically insignificant.
Factors listed above (table 6) such as age, gender, ASA, primary peritonitis, duration from last surgery, resection and anastomosis, anastomotic leak and number of relaps were checked if any Factors listed above (table 6) such as age,gender, ASA, primary peritonitis, duration from last surgery, resection and anastomosis, anastomotic leak and number of relaps were checked if any is associated to mortality using Chi square which found no association except anastomotic leak and number of relaparatomy. Anastomotic leak a P value of 0.030 and the number of relaparotomies had P value of 0.029 which was statistically significant. The variable age had a P value of 0.223, which was statistically insignificant but clinically significant, with high mortality rate in extreme of ages less or equal to one year and above 45 years. Other variables were statistically insignificant.
Discussion of Results:
.1: Incidence of Relaparotomy.
In our study, the frequency of relaparotomy was 19.3% and the incidence rate reported in different studies ranges from 1.1% to 4.4%(Ching et al., 2003, Martínez-Casas et al., 2010)which is different with our findings . A study done in India by(Koirala et al., 2015) reports an incidence rate ranging from 0.5% to 15%.which is similar to our findings and the same by (Negussie et al., 2018)in Ethiopia 17.1%.Incidence of relaparotomy differs according to hospital setup as well as patient characteristics and initial surgery. It also depends on post-operative care given to patient following first surgery and incidence of post-operative sepsis(Patel et al., 2016). In Nigeria a study done by(Ayandipo et al., 2016) reported a prevalence of 8.4%..Most of the studies that reported a low incidence rate were done for a long period (1 to 10 years)- getting a large denominator of laparotomies (primary surgery).On the other hand, our study duration was 8 months.
5.2. Demographics
5.2.1 Sex Distribution.
In our study we recruited 54 patients. The study showed that male participants were almost more affected than female with a sex ratio of 1.3:1.The male predominance was also observed by (Koirala et al., 2012)in India M:F 4:3.(Hasan and Abdul-Aemmah, 2018)(4.9:1) in Iraq. However (Otshudiema et al., 2017)in Congo observed female predominance(F:M 1.2:1) and(BAHI, 2010) in Morocco found male predominance but the study site was military training hospital in Rabat.
5.2.2: Age Distribution
This study showed that the most affected age group was between 15-45 (46.3%) and extreme of age ≤1years (24.1) and >45(24.1%) .High incidence rate of relaparotomy in a similar age group was also observed in a study done in India(Patel et al., 2016)The mean age was 27.39 years which was similar to a study by (Koirala et al., 2015) who had mean age of 31.99±21.49 years.(BAHI, 2010)observed an average age of 54yers in Morocco This is due not only to the fact that surgical digestive pathology is relatively less frequent in young subjects in Morocco but also by the difference in the pathologies causing the occurrence of peritonitis(Baig et al., 2002)
5.3. Clinical characteristics
The most common presenting symptoms in our study were abdominal distension (70.4%) abdominal pain.(Hutchins et al., 2004) and (Patel et al., 2016) from India had similar findings. Presence of systemic disease in our study population was 31.5% including diabetic, hypertension and intra-abdominal malignancy similar to a study done in Europe(Gedik et al., 2009) with same findings with our study.
5.3.1. Indication of initial laparotomy and relaparotomy
In our study, the most initial cause of the primary laparotomy was peritonitis (57.4%) followed by peptic ulcer perforation and this was in agreement with other similar studies (Ayandipo et al., 2016),from Nigeria and (Koirala et al., 2015) from India ,However, some studies reported intestinal obstruction as main cause of the primary surgery(Patel et al., 2016)in India .(Otshudiema et al., 2017)in Congo also the same was observed.
Majority (98.1%) of the relaparotomy cases were emergency and only one case( 1.9%) was elective in this study, similar with a study done in Turkey 87.0%(Unalp et al., 2006)but a study by(Pérez-Guerra et al., 2017)differs with our study- 60% were elective.
In this study the number of relaparotomies was 1 to 4 times, 50% had one relaparotomy while 29.6% had two relaps. However (Otshudiema et al., 2017)findings were different from our study –relap were 3 to 5 times and more. A study on postoperative peritonitis in elderly observed that reoperations were 3 times and more (Hssaida et al., 2000)n Morocco
5.3.2: Indication of relaparatomy, site of index operation and surgery.
The causes of reoperations requiring relaprotomies are similar everywhere and our study concurred with numerous other studies. Most common cause of relaparotomy in our study was anastomotic leakage (33.3%), followed by burst abdomen (27.8%) and intra-abdominal sepsis(24.1%) and the same were observed in studies done by (Unalp et al., 2006) in Turkey and .(Sharma et al., 2016) In India. However our study differed slightly with (Mutiibwa et al., 2012)in Uganda where the causes of reoperations were intra-abdominal abscess 2.3% new intestinal perforation 4.6% and anastomotic leak 2.3%.. A Study by (Koirala et al., 2012)indicated the major indications of re-laparotomy were burst abdomen/evisceration ( 22.5%), followed by intra-abdominal collection and abscess ( 17.5%), fecal contamination (15%), and biliary peritonitis ( 12.5%).In another study in Congo, enteral fistula accounted for 64.2% of the relaps (Otshudiema et al., 2017).
Regarding the site of index operation, Lower GI procedures accounted for 66.7% followed by upper GI 24.1%, abdominal wall 5.6% and hepatobiliary 3.7%. Similar findings were observed by (Koirala et al., 2015) Lower GI 57.5% upper GI 30%, (Unalp et al., 2008)in Turkey and (Van Ruler et al., 2007).
The most common initial operation performed in our study was resection and anastomisis 42.1% followed by perforation repair and stoma 13.0%. A study by (Sharma et al., 2016)in Nepal recorded similar findings -resection and anastomosis 44.5% and closure of perforation 20..5%. (Koirala et al., 2015) in India. This similarity was due to the initial indication being peritonitis of different etiologies and the commonest site of initial surgery was Lower GI.
Most of the initial surgery and realaparotomy in our study were done by senior house officers (2nd years) and were under the supervision of a surgeon on call. Senior house officer 46.3% and qualified surgeons performed 33.3% of the relaparotomies. A similar study by (Mzaza et al 2012) in Zambia also showed that 42.0% of laparotomies were done by senior house officers. This similarity was attributed to the fact that both studies done in teaching institution. Based on the procedures performed, it was not possible to attribute the leaks to level of competence of surgeons. This doesn’t in anyway suggest that senior house officers are as good as their senior colleagues. What came out was the fact that emergence theatres are manned by senior house officers since it’s a teaching institution.
The mean duration between the primary surgery and relaparatomy in our study was 9.3±7.45 days, only 2 cases were performed within 48 hrs. The same was reported by (Koirala et al., 2015)mean duration of 9.24±7.56days from Nepal. (Sharma et al., 2016) in India observed slightly less days 6.4 days.
Short term outcome of relaparotomy
Relaparotomies are associated with a high rate of complications and our results were no different. Wound infection 55.6% and sepsis 13.0% were among the common complications and this was also observed in other studies(Otshudiema et al., 2017)in Congo.(Koirala et al., 2015)n Nepal and(Mefire et al., 2009)in Mexico.
Our study showed that most patients had a hospital stay of less than 30 days (50.9%). Only 7.6% had a hospital stay of more than 30 days. A study done in Morocco documented hospital stay of 27 to 35 days (BAHI, 2010) .However (Baig et al., 2002) and (Otshudiema et al., 2017) from Congo had a hospital stay of more than 60 days the reason being planned relaparotomy and persistent peritonitis as reported in their studies.
29.6% of our cases were admitted to ICU for monitoring postoperatively and mean duration in ICU of 6 to 8 days similar to (BAHI, 2010) 7 to 8 days.
The mortality rate in our study was 37.0%.Old and new studies reported mortality rate from 15.5% to 53%(Tera and Aberg, 1975, Myshkin et al., 1989, Unalp et al., 2006)..Our findings are comparable to a study done by (Martínez-Casas et al., 2010) in Valencia-Spain who reported mortality rate of 35% and India(Patel et al., 2016)of 34.72%..The mortality in our study for single relaparotomy was 10%(2/54) and after second relaparotomy 35%(7/54) and this was comparable to a study by(Koirala et al., 2012) which reported 20% after first relaparotomy and the mortality after second relaparotomy was 40% . Likewise our study showed a mortality of 55
Recommendations
All urgent cases that can wait should receive adequate resuscitation and stabilized before operation. Those undergoing reoperations must be adequately prepared with full investigations. Although we were limited by select antibiotics in our setting, we should strive to cover all possible pathogens and then target treatment following cultures results for good antibiotic stewardship.
Also, with limited investigative facilities, the decision to return to the operating room should be made as soon as possible or when highly suspected based on clinical findings, Delays in care can increase mortality and emergency supplies and theatre space should always be available if possible.
During surgery, a careful and thorough exploration must be done to avoid missing any pathology in the abdomen. And surgeons need carefully decide intra-operatively whether to do an anastomosis versus diverting surgery when a patient is unstable
Postoperative patients need regular monitoring in order to identify and manage any complications early and unfortunately lack of space in the intensive care unit to monitor critically patients after relaparotomy, is a limitation of our setting. There is need for adequate ICU space to properly manage very unstable postoperative patients
References
- AYANDIPO, O. AFUWAPE, O. IRABOR, D. ABDURRAZZAAQ, A. & NWAFULUME, N. (2016). Outcome of laparotomy for peritonitis in 302 consecutive patients in Ibadan, Nigeria. Annals of Ibadan postgraduate medicine. 14:30-34.
View at Publisher | View at Google Scholar - BAHI, M. (2010). (Les reprises chirurgicales en pathologie digestive: Facteurs etiologiques et pronostiques.(à propos de 25 cas).
View at Publisher | View at Google Scholar - BAIG, M. K. ZHAO, R. H. BATISTA, O. URIBURU, J. SINGH, J. WEISS, E. NOGUERAS, J. & WEXNER, S. (2002) .Percutaneous postoperative intra-abdominal abscess drainage after elective colorectal surgery. Techniques in coloproctology. 6:159-164.
View at Publisher | View at Google Scholar - CHING, S., MURALIKRISHNAN, V. & WHITELEY, G. (2003). Relaparotomy: a five-year review of indications and outcome. International journal of clinical practice. 57:333-337.
View at Publisher | View at Google Scholar - ERDEM, E. GOKDEMIR, Y. UNAL, F. ERSU, R. KARADAG, B. & KARAKOC, F. (2013). Flexible bronchoscopy as a valuable tool in the evaluation of infants with stridor. European Archives of Oto-Rhino-Laryngology.270:21-25.
View at Publisher | View at Google Scholar - GEDIK, E. SÖYLEMEZ, K. GIRGIN, S. UYSAL, E. & TAÇYÝLDÝZ, Ý. (2009). Relaparotomies: Why is Mortality Higher? European Journal of Trauma and Emergency Surgery. 35:547-552.
View at Publisher | View at Google Scholar - HASAN, K. C. & ABDUL-AEMMAH, A. K. 2018. A 5-year study of re-laparotomies, planned and unplanned, in Al-Hillah Teaching General Hospital. Medical Journal of Babylon. 15:25.
View at Publisher | View at Google Scholar - HIMPENS, J. DAPRI, G. & CADIÈRE, G. B. (2006). A prospective randomized study between laparoscopic gastric banding and laparoscopic isolated sleeve gastrectomy: results after 1 and 3 years. Obesity surgery. 16:1450-1456.
View at Publisher | View at Google Scholar - HSSAIDA, R. DAALI, M. SEDDIKI, R. ZOUBIR, M. ZOUBIR, M. ELGUELAA, K. & BOUGHALEM, M. 2000. Les péritonites postopératoires chez le sujet âgé. Médecine du Maghreb. 81:19-22.
View at Publisher | View at Google Scholar - HUTCHINS, R. R. GUNNING, M. P. LUCAS, D. N. ALLEN-MERSH, T. G. & SONI, N. C. (2004). Relaparotomy for suspected intraperitoneal sepsis after abdominal surgery. World journal of surgery. 28:137-141.
View at Publisher | View at Google Scholar - HYMAN, N. (2009). Managing anastomotic leaks from intestinal anastomoses. The Surgeon. 7:31-35.
View at Publisher | View at Google Scholar - KOIRALA, R. MEHTA, N. VARMA, V. KAPOOR, S. KUMARAN, V. & NUNDY, S. (2015). Urgent Redo-Laparotomies: Patterns and Outcome—A Single Centre Experience. Indian Journal of Surgery. 77:195-199.
View at Publisher | View at Google Scholar - KOIRALA, R. SHAKYA, V. KHANIA, S. ADHIKARY, S. & AGRAWAL, C. 2012. Redo-laparotomies: reasons, morbidity and outcome. Nepal Med Coll J, 14, 107-110.
View at Publisher | View at Google Scholar - KWOK, A. C. SEMEL, M. E. LIPSITZ, S. R. BADER, A. M., BARNATO, A. E. GAWANDE, A. A. & JHA, A. K. 2011. The intensity and variation of surgical care at the end of life: a retrospective cohort study. The Lancet. 378:1408-1413.
View at Publisher | View at Google Scholar - MARTÍNEZ-CASAS, I. SANCHO, J. J. NVE, E., PONS, M.-J. MEMBRILLA, E. & GRANDE, L. (2010). Preoperative risk factors for mortality after relaparotomy: analysis of 254 patients. Langenbeck's archives of surgery. 395:527-534.
View at Publisher | View at Google Scholar - MEFIRE, A. C. TCHOUNZOU, R. MISSE, P. M. PISOH, C. PAGBE, J. ESSOMBA, A. TAKONGMO, S. & MALONGA, E. (2009). Réinterventions de chirurgie abdominale en milieu défavorisé: indications et suites opératoires (238 cas). Journal de Chirurgie. 146:387-391.
View at Publisher | View at Google Scholar - MULIER, S. PENNINCKX, F. VERWAEST, C. FILEZ, L. AERTS, R. FIEUWS, S. & LAUWERS, P. (2003). Factors affecting mortality in generalized postoperative peritonitis: multivariate analysis in 96 patients. World journal of surgery. 27:379-384.
View at Publisher | View at Google Scholar - MUTIIBWA, D. LOPEZ, A. TUMUSIIME, G. RIDING, D. & DIAZ, A. (2012). Aetiology and Treatment Outcome of Non-traumatic Small Bowel Perforations at Mbarara Hospital in South-Western Uganda. East and Central African Journal of Surgery. 17:25-31.
View at Publisher | View at Google Scholar - MYSHKIN, K. BLUVSHTEĬN, G. & DODIN, S. (1989). Relaparotomy after operations on the rectum and colon. Vestnik khirurgii imeni II Grekova.143:5-9.
View at Publisher | View at Google Scholar - NEGUSSIE, T. GOSAYE, A. & DEJENE, B. (2018). Outcomes of early relaparotomy in pediatric patients at Tikur Anbessa teaching hospital, Addis Ababa, Ethiopia: a five-year retrospective review. BMC surgery. 18:99.
View at Publisher | View at Google Scholar - OTSHUDIEMA, O. LOBE, L. & AHUKA, O. (2017). International Journal of Current Advanced Research. Evolution. 80:4-5.
View at Publisher | View at Google Scholar - PATEL, H., PATEL, P. & SHAH, D. (2016). Relaparotomy in general surgery department of tertiary care hospital of Western India. International Surgery Journal. 4:344-347.
View at Publisher | View at Google Scholar - PÉREZ-GUERRA, J. A.VÁZQUEZ-HERNÁNDEZ, M.RAMÍREZ-MORENO, R. & LÓPEZ-GARCÍA, F. R. 2017. Abdominal re-operations: Prevalence in elective and emergency surgery. Cirugía y Cirujanos (English Edition). 85:109-113.
View at Publisher | View at Google Scholar - SHARMA, A. SAHU, S. K. NAUTIYAL, M. & JAIN, N. (2016). To Study the Aetiological Factors and Outcomes of Urgent Re-Laparotomy in Himalayan Hospital. Chirurgia. 111:58-63.
View at Publisher | View at Google Scholar - TEN BROEK, R. STRIK, C. & VAN GOOR, H. (2014). Preoperative nomogram to predict risk of bowel injury during adhesiolysis. British Journal of Surgery. 101: 720-727.
View at Publisher | View at Google Scholar - TEN BROEK, R. P. STRIK, C. ISSA, Y. BLEICHRODT, R. P. & VAN GOOR, H. (2013). Adhesiolysis-related morbidity in abdominal surgery. Annals of surgery. 258:98-106.
View at Publisher | View at Google Scholar - TERA, H. & ABERG, C. (1975). Relaparotomy. A ten-year series. Acta Chirurgica Scandinavica.141:637-644.
View at Publisher | View at Google Scholar - UNALP, H. R. KAMER, E. KAR, H. BAL, A. PESKERSOY, M. & ONAL, M. A. (2006). Urgent abdominal re-explorations. World Journal of Emergency Surgery. 1:10.
View at Publisher | View at Google Scholar - UNALP, H. R. KAMER, E. & ONAL, M. A. (2008). Analysis of early relaparotomy after lower gastrointestinal system surgery. Surgery today: 38:323-328.
View at Publisher | View at Google Scholar - VAN RULER, O. LAMME, B. GOUMA, D. J. REITSMA, J. B. & BOERMEESTER, M. A. 2007. Variables associated with positive findings at relaparotomy in patients with secondary peritonitis. Critical care medicine. 35:468-476.
View at Publisher | View at Google Scholar
