

Research Article | DOI: https://doi.org/10.31579/ 2834-8788/001
Estimation And Prediction of Ten-Year Survival Rate and The Risk of Cardiovascular Complications in The Population of Men and Women in Russian Region
1 National Medical Research Center for Therapy and Preventive Medicine, Moscow, Russia.
2 Vladimir State University named after A.G. and N.G. Stoletovs, Vladimir, Russia.
*Corresponding Author: Mamedov M.N, National Medical Research Center for Therapy and Preventive Medicine, Moscow, Russia.
Citation: Mamedov M.N, Sushkova L.T, Kutsenko V.A. (2022). Estimation And Prediction of Ten-Year Survival Rate and The Risk of Cardiovascular Complications in The Population of Men and Women in Russian Region. Journal of Heart and Vasculature.1(1); 10.31579/ 2834-8788/001
Copyright: © 2022 Mamedov M.N, This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 09 September 2022 | Accepted: 14 September 2022 | Published: 22 September 2022
Keywords: prevalence; comorbidity of chronic noncommunicable diseases; cardiovascular risk; charlson index
Abstract
The aim: To evaluate the predicted ten-year survival rate and the risk of cardiovascular complications (CVD) in an unorganized population of men and women in the Vladimir region of Russia.
Material and methods. The cross-sectional population study included 1200 men and women aged 30-69 years from 5 cities of the Vladimir region. The response was over 80 Percentage. Overall, 1,004 people were included into the study. Of these, 346 men (34.5 Percentage) and 658 women (65.5 Percentage). Respondents were interviewed using a questionnaire that assessed socio-demographic indicators, behavioral risk factors, the presence of somatic diseases, medical records, and psychosomatic status. Routine instrumental and laboratory studies were performed. The European SCORE scale was used to assess cardiovascular risk. Charlson's comorbidity index was used to assess 10-year survival rate of study participants.
Results. In the surveyed population, arterial hypertension (AH) was detected in 38 Percentage of men and 43 Percentage of women. Coronary heart disease among men was registered three times more often compared with women: 15 Percentage and 5 Percentage (p less than0.0001). Diabetes mellitus, chronic obstructive pulmonary disease and malignant tumors were detected in no more than 5 Percentage of cases. 67 Percentage of women had low to moderate cardiovascular risk (CVR). 19 Percentage of men showed high and 10 Percentage very high CVR, which turned out to be higher than in women (6 Percentage and 0 Percentage). The prevalence of the combination of two diseases was 32.6 Percentage in general – in 36.7 Percentage of men, and in 10 Percentage less of women. Overall, the combination of diseases was found in every fourth study participant (27 Percentage) (p=0.002). The combination of three diseases was seen in 12 Percentage of men, and 5.9 Percentage of women (p less than0.001). Short ten-year survival (21 Percentage) according to the Charlson index was determined in less than 10 Percentage of men and women. Most respondents had 90 Percentage and 77 Percentage ten-year survival.
Conclusion. In an unorganized population of adults, high and very high CVR was found in every 4th man and only in every 16th women. A short ten-year survival rate according to the Charlson index was found in every 10th respondent, while at the same time, every second participant had an average ten-year survival rate.
List of abbreviations
AH - arterial hypertension
BP - blood pressure
CHD – coronary heart disease
CCI - Charlson Comorbidity Index
BMI - body mass index
INR - international normalized ratio
NMRC TPM - National Medical Research Center for Therapy and Preventive Medicine
OR - odds ratio
CVD - cardiovascular diseases
CVR - cardiovascular risk
CNCD - chronic non-communicable diseases
COPD - chronic obstructive pulmonary disease
HR - heart rate
ECG – electrocardiogram
WHO - World Health Organization
Introduction
According to the forecast of the World Health Organization (WHO), in the next decade, chronic non-communicable diseases (CNCDs) will be the main cause of disability and amostality among adults worldwide. Moreover, despite some changes mortality rate among working population, it is obvious that in the next decade, cardiovascular diseases (CVD) associated with atherosclerosis, neoplasms and chronic obstructive pulmonary disease (COPD) will retain their leadership [1].
On the other hand, the WHO shows that the life expectancy of the population is increasing. Along with this, the number of patients with comorbidity of somatic diseases is increasing that also affect their life quality. The term "comorbidity" was proposed in 1970 by the American epidemiologist and researcher Alvan R. Feinstein. By comorbidity, he meant the presence of a concomitant clinical picture. According to the modern definition, comorbidity is the coexistence of two or more syndromes (trans-syndromal comorbidity) or diseases (trans-nosological comorbidity) in one patient that are interconnected pathogenetically or coincided together [2].
Currently, the study of comorbidity is relevant due to the pandemic nature of CVD and its increasing prognostic value. According to Russian scientists, the combination of three or more somatic diseases, adjusted for sex and age, increases the risk of primary endpoints development by 2-5 times compared with individuals with the presence of one disease. A linear relationship between age and comorbidity frequency of somatic diseases was determined. If at the age of 20 its frequency is less than 10 Percentage, then at the age of 80 it increases up to 80 Percentage [2].
Data from individual registries on the assessment of comorbidity of somatic diseases have been published in the literature [3,5]. The systematization of the principles of themanagement of patients with comorbidities is presented. However, to assess the significance of the comorbidity of somatic diseases at the population level, epidemiological studies are required, that would consider socio-demographic indicators such asgender and age. From this point of view, clinical studies have a number of limitations, since the results of the study can only be applied to certain cohorts.
The aim of this study is to assess the prevalence of major NCDs and their comorbidity in a random sample of men and women aged 30-69 years in the cities of the Vladimir region.
Materials and Methods
A cross-sectional population study was conducted from May 2018 to September 2020 in 5 cities of the Vladimir region (Vladimir, Kovrov, Murom, Yuryev-Polsky and Vyazniki). From 6 medical institutions, 8 therapeutic sites were selected, then, according to the lists of the assigned population aged 30-69 years, every tenth respondent from each site was invited to the study. On average, out of 1500 people of the attached population, every tenth (1500:10 = 150; in total, 150 respondents per polling station). Thus, the study included 1200 people, men and women aged 30-69 years. The response to the study wasover 80 Percentage. Overall, 1,004 people completed the survey - 346 men (34.5 Percentage) and 658 women (65.5 Percentage). Table 1 presents gender characteristics of study participants in 5 cities of the Vladimir region.
Cities | Total, n | Men, n | Women, n |
Vladimir | 282 | 102 | 180 |
Vyazniki | 62 | 13 | 49 |
Kovrov | 195 | 60 | 135 |
Murom | 315 | 128 | 187 |
Yuriev-Polsky | 150 | 43 | 107 |
All cities | 1004 | 346 | 658 |
Table 1: Population size by city and gender
At the first stage, the respondents were interviewed using a questionnaire that assessed social status, family history, smoking status, alcohol consumption, other risk factors and comorbidities, records of medications taken, and psychosomatic status, including the presence of chronic stress.
All respondents underwent blood pressure (BP), heart rate (HR) at rest, anthropometric parameters (height, body weight, body mass index (BMI), waist circumference) measurement, as well as biochemical blood test (including total cholesterol and fasting blood glucose levels).
The risk of fatal cardiovascular complications (CVR) in the next 10 years was assessed using the European SCORE scale (in the absence of verified CVD). The following parameters were used to assess the risk: age, gender, smoking status, systolic blood pressure and total cholesterol level. Depending on the total score, the risk was assessed as follows: low risk <1>
The determination of 10-year survival was carried out using the Charlson Comorbidity Index (CCI), which was calculated by summing up scores for age and somatic diseases. Depending on the severity of the disease, the CCI can vary from 1 (for example, myocardial infarction, diabetes mellitus (DM) without complications) to 4 points (for example, metastatic malignant tumors). In addition, 1 point was added for every 10 years of life after 40 [7]. The prognosis is defined as a percentage of survival: 99 Percentage, 96 Percentage, 90 Percentage, 77 Percentage, 53 Percentage and 21 Percentage.
Control of material collection and training of researchers.
The materials were carried out with the participation of primary care internists of the Vladimir region. The training on the protocol and fillingof the questionnaire was performed, then the questionnaires were checked by independent experts in a selective mode. The results were processed centrally: at the Vladimir State University (Vladimir) and at the National Medical Research Center for Therapy and Preventive Medicine (Moscow).
Statistical analysis.
Data entry was carried out in the Excel system of the MS Office package. Statistical analysis was carried out in the statistical analysis system SAS (Statistical Analysis System) and data analysis environment R 3.5.1. Qualitative indicators are described by relative frequency in percent. Quantitative indicators are described by the mean and standard error (M±m). Differences between two independent samples for continuous parameters were estimated using the Welch t-test. Comparison of prevalence was carried out by the test of equality of shares. Differences were considered significant at p less than 0.05.
Results
According to the data obtained, 1004 respondents participated in the study, of which 34.5 Percentage were men and 65.5 Percentage were women. The largest number of respondents was selected from two large cities: Vladimir (28 Percentage) and Murom (31.4 Percentage). In the rest of the cities, a total of 40.6 Percentage of the respondents were included into the study. Men and women were comparable by age (52.9±2.1 years and 53.7±1.2 years, respectively). In general, the age range of respondents (both men and women) did not differ statistically between cities.
In the sample of people of working age, 28 Percentage of respondents had higher education. The groups differed significantly by the prevalence of higher education. The largest number of people with higher education is registered in the city of Vladimir (41 Percentage of men and 44 Percentage of women), which is 1.5-2 times higher than compared with other cities of the Vladimir region.
At the time of the survey, 68 Percentage of men and 56 Percentage of women were married, divorced and widowed women were twice as many as men.
Hereditary predisposition to CNCD was analyzed for CVD, DM, bronchial asthma and various oncological diseases. Hereditary predisposition to CVD (myocardial infarction and cerebral stroke) was registered in 19 Percentage of men and 26 Percentage of women (difference is significant, p=0.01), type 2 diabetes was registered in 17 Percentage of men and 14 Percentage of women. 10 Percentage of men and 7 Percentage of women reported having bronchial asthma in their parents. Oncological diseases of various localization in the family history were detected in total in 5 Percentage of men and 6 Percentage of women. With the exception for CVD, there was no gender difference in genetic predisposition to other NCDs.
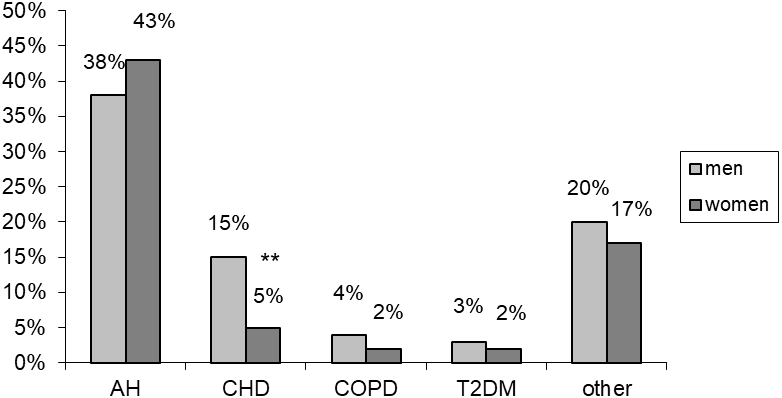
In the population, the analysis of the major NCDs prevalence reveales the highest rates for AH: 38 Percentage among men and 43 Percentage among women. Coronary heart disease (CHD) among men was registered three times more often than women: 15 Percentage and 5 Percentage, respectively (p less than0.0001). Type 2 diabetes in this sample was registered in 2.5 Percentage of cases on average (3 Percentage among men and 2 Percentage among women). COPD among men was detected 2 times more often than in women (no statistical significance: 4 Percentage and 2 Percentage). Cancer had comparable prevalence among men and women (average 3 Percentage). The presence of other somatic diseases was reported by 20 Percentage of men and 17 Percentage of women. Figure 1 shows the prevalence of NCDs in the analyzed population of men and women of working age.
An assessment of the risk of cardiovascular events was carried out according to the European SCORE scale. The results of the assessment of CVR in the analyzed population are presented in Table 2. Thus, 36 Percentage of women had low CV risk, moderate CV risk was determined in 31 Percentage. High CV risk was found in 6 Percentage of women, while a very high risk was not detected at all. Among men, the picture was somewhat different. Low cardiovascular risk was found in 16 Percentage, and moderate risk in every fourth. At the time of the survey, high cardiovascular risk was found in every fifth man, a very high risk in 10 Percentage of cases. Differences in all subgroups of CVR between groups of men and women are statistically significant.
**p less than 0.01 significant difference between men and women
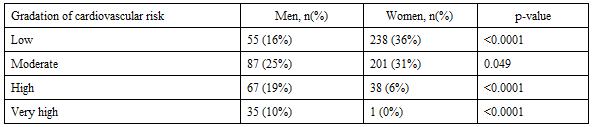
Note: Statistical difference between men and women
The analysis of the comorbidity of somatic diseases showed that in an unorganized population, the prevalence of a combination of two diseases was 32.6 Percentage - 36.7 Percentage among men, and in 10 Percentage less among women. Overall, the combination of diseases was found in every fourth study participant (27 Percentage) (p=0.002). The combination of three diseases among men was 12 Percentage, and among women - in 5.9 Percentage of cases (p less than0.001). According to the survey results, the combination of four diseases was quite rare, but gender differed by gender (1.2 Percentage in women, 0.6 Percentage in men).
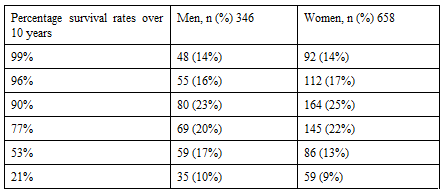
One of the main objectives of the study was to determine the ten-year survival based on the CCI. The prognosis of survival over 10 years according to the CCI is presented in Table 3. In general, these indicators were comparable between men and women. In the analyzed population, every fifth respondent (23 Percentage of men and 25 Percentage of women) had a prognosis of 90 Percentage survival in the next 10 years, every fifth (20 Percentage of men and 22 Percentage of women) had a prognosis of 77 Percentage survival. At the same time, a survival rate of 53 Percentage over 10 years was found in 17 Percentage of men and 13 Percentage of women. Similar rates were obtained for 99 Percentage (14 Percentage among men and women) and 96 Percentage (16 Percentage among men and 17 Percentage among women) survival over 10 years. A short survival rate (21 Percentage) was found in less than 10 Percentage of men and women.
Discussion
A population-based study among adults from 5 cities of the Vladimir region, randomly selected, was conducted to assess the predicted ten-year survival rate and risk of CVD. The Central Federal District in Russia is the leader in the prevalence of chronic NCDs and its complications. Thus, the adult mortality rate from CVD in 2016 in this region was 655.4 per 100 thousand people, which is 6.3 Percentage higher compared with average rate in Russia (616.4 cases per 100 thousand people). In general, mortality rates for oncology are three times lower, but a similar trend is observed: 218.6 cases per 100 thousand people in the central district, which is 6.5 Percentage more compared with average numbers in the Russian Federation (204.3 per 100 thousand people) [8]. Despite the fact that over the past 16 years the overall all-cause mortality rate in this district has decreased by 20.7 Percentage, the Central District ranks second among 8 federal districts in terms of adult mortality from NCDs. This positive dynamics of mortality ireduction in the district is the result of the implementation of national health projects and the provision of high-tech assistive technologies It is known that a family history of NCDs, along with behavioral risk factors, has an important prognostic value. In the present study, 51 Percentage of men and 53 Percentage of women have a hereditary burden for the main NCDs, while CVD associated with atherosclerosis and type 2 diabetes had the highest frequency in the family history.
Among NCDs, AH had the highest prevalence (according to the criteria of the European Society of Cardiology 2018) [9], which was detected in 38 Percentage of men and 43 Percentage of women of working age in the surveyed population. In general, in the large epidemiological study of the ESSE RF, carried out in 12 regions of the country (different in their climatic and geographical characteristics), this trend is confirmed. Within the framework of this national project, 20,652 (37.9 Percentage of men and 62.1 Percentage of women) residents of the Russian Federation aged 25–65 were examined. According to European guidelines from 2013 and 2018, AH was diagnosed in 10,347 (50.2 Percentage) patients - 3,987 (51.1 Percentage) men and 6,360 (49.7 Percentage) women. Recently, the use of antihypertensive therapy has significantly increased (up to 61 Percentage), however, in order to achieve target levels, even greater rise is needed that would also include the use of combination therapy [10].
One of the important parameters of the analysis was the assessment of the CVR in the next 10 years. This aggregate indicator is estimated based on the main risk factors for CVD. In the study population, 41 Percentage of men and 67 Percentage of women had low to moderate CVR. Among men, high CVR was three times more common than among women (19 Percentage vs. 6 Percentage). The total high and very high CVR among men was 29 Percentage, which is 6 times higher than in women. The ESSE RF study also demonstrated that the bulk of the population has low to moderate CVR. However, men are 6 times more likely to have high risk (≥5 Percentage) than women (40.5 Percentage vs 7.4 Percentage), that shows significant gender difference. A ranked analysis of the regions showed that in Vologda, Voronezh and Tomsk more than a quarter of the population has a high or very high CVR. A low incidence of CV risk (10-15 Percentage) was found in Vladikavkaz and Samara. Of course, such factors as high blood pressure, total cholesterol and smoking also contribute to CVR, however they are not included into the SCORE risk calculator. These are, first of all, social indicators and the state of the environment [11].
Traditionally, CHD among CVD ranks second in prevalence in the population. In the present study, similar patterns were obtained. However, there are significant gender differences. Thus, the incidence of CHD among men is three times higher than among women (15 Percentage versus 5 Percentage). In another population-based study conducted in Tyumen in an open population involving 2000 people, aged 25–64 years, the prevalence of CHD in men was 12.4 Percentage, in women - 10.0 Percentage [12]. Obviously, the gender difference in this study may be due to the lack of verification of painless and other forms of CHD among women. In the population of cities in the Vladimir region, attention is also drawn to the low prevalence of type 2 diabetes and COPD, the frequency of which individually is no more than 5 Percentage of cases.
Assessment of the comorbidity of internal diseases and its gender characteristics is an urgent problem. In the local literature, most works are devoted to the study of the comorbidity of somatic diseases in individual cohorts. In previous clinical cohort studies, we have shown that >70 Percentage of patients with CHD have three or more comorbidities. According to the REQUAZA registry, among 1,000 outpatients with CVD, concomitant cardiovascular pathology was detected in 82 Percentage of cases, of which 50.4 Percentage were AH, CHD, and CHF [5]. Later, researchers in the course of a 6-year prospective follow-up concluded that individuals with the development of CVD at the age of less than50 years are the target group for the prevention of cardiovascular multimorbidity and its progression [13]. In another domestic study (n=993), it was demonstrated that comorbidity surve as an independent predictor for the development of acute heart failure in myocardial infarction, and its combination is associated with the worst hospital prognosis (1.5-3 times more compared to one disease), regardless of the primary treatment strategy [4].
In the present study of unorganized population, a combination of two diseases is the most common, it is detected in every third respondent, while a combination of three diseases occurs 3 times less. The comorbidity of somatic diseases has gender differences, in particular, among men it is detected significantly more often than in women.
Estimation of survival rate in case of comorbidity of somatic diseases is an important issue problem of modern medicine. In general, 5 scales for the prediction of comorbid conditions are described in the literature. The Charlson comorbidity index is widely used for the assessement 10-year survival prognosis. In the Scandinavian MADDEC study in individuals with acute coronary syndrome (n=1576), the HCI was compared with the hospital GRACE scale in three time ranges up to two years. It has been demonstrated that the predictive value of CCI increases in the long-term [14]. In a study involving newly diagnosed patients with AH, it was shown that the use of CCI effectively affects the prognostic model of survival rate [15]. In a Korean study of 228,000 people aged 65 years and older with type 2 diabetes without CV events, the CCI was used. The presence of comorbidities and low glucose levels were associated with high cardiovascular mortality [16].
In this study, every second respondent from the surveyed population had a 10-year survival rate from 77 Percentage to 90 Percentage, a low 10-year survival rate was found in every 10th respondent. Consequently, a high ten-year survival rate occurs in one in three adults. Obviously, up to 70 Percentage of adult men and women with comorbid internal diseases, with low and average ten-year survival rate need complex preventive interventions.
Research limitation
The article does not provide the values of risk factors, on the basis of which the risk assessment of cardiovascular complications was carried out, since these materials will be analyzed in subsequent publications.
Research limitation
The article does not provide the values of risk factors, on the basis of which the risk assessment of cardiovascular complications was carried out, since these materials will be analyzed in subsequent publications.
Conclusion
In the unorganized population of adults in the cities of the Vladimir region, high and very high CVR is detected in every 4th man, which is 4 times higher compared with women. A combination of two diseases is detected in every third respondent. A short ten-year survival rate according to the ICH was found in every tenth respondent. Every second man and woman had an average ten-year survival rate.
Thus, the comorbidity of somatic diseases with a short and average ten-year survival rate requires complex preventive interventions.
Conflict of Interest
There is no conflict of interest.
References
- NCD Countdown 2030: worldwide trends in non-communicable disease mortality and progress towards Sustainable Development Goal target 3.4. Lancet. 2018;392(10152):1072-1088.
View at Publisher | View at Google Scholar - Drapkina O.M., Kontsevaya A.V., Mamedov M.N. et al. 2022 Prevention of chronic non-communicable diseases in the Russian Federation. National guidelines. Cardiovascular Therapy and Prevention. 2022;21(4):3235.
View at Publisher | View at Google Scholar - Tolpygina SN, Zagrebelnyi AV, Martsevich SYu. Influence of cerebral stroke on life prognosis of patients with stable coronary heart disease according to the data of CHD prognosis registry. The Clinician. 33-41.
View at Publisher | View at Google Scholar - Zykov MV, Kashtalap VV, Bykova IS, on behalf of all participants in the RECORD-3 registry. Comorbidity in acute heart failure complicating myocardial infarction. Russian Journal of Cardiology. 2020;25(7):3427.
View at Publisher | View at Google Scholar - Boytsov SA, Yakushin SS, Martsevich SYu, et al. Outpatient register of cardiovascular diseases in the Ryazan Region (RECVASA): principal tasks, experience of development and first results. Rational Pharmacotherapy in Cardiology. 2013;9(1):4-14.
View at Publisher | View at Google Scholar - Conroy RM, Pyörälä K, Fitzgerald AP, et al. Estimation of ten-year risk of fatal cardiovascular disease in Europe: the SCORE project. Eur Heart J. 2003;24(11):987-1003.
View at Publisher | View at Google Scholar - Charlson ME, Pompei P, Ales KL, McKenzie CR. A new method of classifying prognostic comorbidity in longitudinal studies: development and validation. J ChronDis. 1987; 40(5):373-383.
View at Publisher | View at Google Scholar - Vangorodskaya S.A. Dynamics of mortality of the population of the Central Federal District from the main classes of causes in 2000-2016. Voronezh State University Bulletin. Series: history, political science, sociology. 2019;1 :31-39.
View at Publisher | View at Google Scholar - Williams B, Mancia G, Spiering W, et al. 2018 ESC/ESH Guidelines for the management of arterial hypertension. European Heart Journal. 2018;39(33):3021-3104.
View at Publisher | View at Google Scholar - Erina AM, Rotar OP, Solntsev VN, et al. Epidemiology of Arterial Hypertension in Russian Federation – Importance of Choice of Criteria of Diagnosis. cardiology. 2019;59(6):5-11.
View at Publisher | View at Google Scholar - Shalnova SA, Drapkina OM. Contribution of the ESSE-RF study to preventive healthcare in Russia. Cardiovascular Therapy and Prevention. 2020;19(3):2602.
View at Publisher | View at Google Scholar - Kayumova MM, Gakova EI, Senatorova OV. Epidemiological aspects of the prevalence of coronary heart disease in an open urban population: gender differences. Siberian Medical Journal. 2019;34(2):146-151.
View at Publisher | View at Google Scholar - Andreenko EYu, Lukyanov MM, Yakushin SS, et al. Young ambulatory patients with cardiovascular diseases: age and gender characteristics, comorbidity, medication and outcomes (according to RECVASA register). Cardiovascular Therapy and Prevention. 2019;18(6):99-106.
View at Publisher | View at Google Scholar - Hautamäki M, Lyytikäinen L-P, Mahdiani S, et al. The association between charlson comorbidity index and mortality in acute coronary syndrome – the MADDEC study. Scand Cardiovasc J. 2020;54(3):146-152.
View at Publisher | View at Google Scholar - Rymkiewicz P, Ravani P, Hemmelgarn BR, et al. Effects of longitudinal changes in Charlson comorbidity on prognostic survival model performance among newly diagnosed patients with hypertension. Comparative Study BMC Health Serv Res. 2016;16(1):671.
View at Publisher | View at Google Scholar - Lee JH, Han K, Huh JH. The sweet spot: fasting glucose, cardiovascular disease, and mortality in older adults with diabetes: a nationwide population-based study. Cardiovasc Diabetol. 2020;19(1):44.
View at Publisher | View at Google Scholar
