

Research Article | DOI: https://doi.org/10.31579/2835-9232/087
Epidemiology of The Healthy Average Life Expectancy! A Global Public Health Challenge!
- K. Suresh 1*
*Corresponding Author: K. Suresh*, MD, DIH, DF, FIAP, FIPHA, FISCD, Family Physician & Public Health Consultant, Bengaluru, 560022.
Citation: K. Suresh*, (2025), Epidemiology of The Healthy Average Life Expectancy, International journalof clinical epidemiology 4(3); Doi: 10.31579/2835-9232/087
Copyright: © 2025 K. Suresh, this is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited
Received: 02 June 2025 | Accepted: 09 June 2025 | Published: 20 June 2025
Keywords: ALE= Average Life Expectancy, HALE= Healthy Average Life Expectancy, HICs= High income countries, L&MCs= Low- and Middle-income countries
Abstract
The average life expectancy (ALE) of a country infers the medical and hygiene standards. The oldest people in the world are about 115 years or older. Most of these records are from the US, Japan and a few European countries. The gap in Average life expectancy between men and women varies in each country and has changed over time. Boys have higher death rates than girls in their youth, due to accidents and violence. Men have higher death rates than women in older ages, due to chronic health conditions. Several factors, like geographical extension, size of the population, economic status, educational status of the people, Community systems, infrastructure, and access to healthcare influence ALE.
The Healthy Average Life Expectancy (HALE) is a measure of how many years a person can expect to live in good physical and mental health and independent, free of disease and disability. HALE is a more nuanced way to understand health outcomes than life expectancy alone, as it considers both morbidity and mortality. However, expecting people to be free of disease and disability compared to their own health status before the age of sixty years is over-ambitiousness. This author likes to redefine HALE as Good enough physical, Mental, Social and Spiritual Health, irrespective of implicit or explicit disease or disability - if they allow the individual to lead day-today’s life comfortably without anybody’s support.
Human cells are continuously exposed to stressors like reactive oxygen species, non-enzymatic protein modifications, environmental substances, UV-radiation and genetic impacts of the activation of oncogenes. Throughout the lifetime of every molecule and cell, damage caused by these stressors accumulates gradually. Although cells possess protective and repair mechanisms to counteract, the damage is eventually too exhaustive to be repaired as one ages beyond 65 years.
For example, the best ALE of Japanese men and women were 84.71 and 87.84 years, while their HALE for men of 72.68 and women of 75.38 years, indicated a gap more than 12 years in 2023. Both men and women in Japan require care from others for more than 12 years, clearly a social and economic burden. In 2019, this gap was about 5 years in India as compared to 10 years in Japan. Both individuals and national governments have multiple responsibilities to fulfill the dream HALE of 80 years by 2030. While developed countries are struggling with perishing primary health care and developing countries struggling to provide secondary and Tertiary quality care at affordable cost to all. Universal Health Coverage, Environmental pollution, Climate Challenge, Non-communicable diseases and Pandemics of infectious diseases challenge all countries. Based on this understanding how many countries in the world can achieve HALE of 80 years by 2030 as a first target? is the challenge for Global communities and Country Governments.
Materials & Methods:
This article is a review of available literature on the challenges of HALE and the efforts needed by individual’s and Countries health Systems.
Introduction
The UN Average Life expectancy (ALE) data, in 2023, reported the Global Average Life expectancy as 73.17, 70.55, 75.89 years for general population, male & Female respectively. Looking at the countries’ Hongkong was estimated to have highest average life expectancy of 85.51 82.84 88.13.for general, Male and Female populations. This was followed by Japan GP=84.71, Men=81.69, Female= 87.74. Average life expectancy for men in UK was GP=81.30 Male=79.36 and Female= 83.21 Average life expectancy for men in the USA was GP=79.3, Male=76.86 and Female= 81.85, and India had an estimated life expectancy of 72.0 yrs for GP, Male= 70.52 and Female= 73.60 years. India ranked 131 out of 210 countries [1].
Scientists worldwide are struggling to find definitions and appropriate measurements of aging per se and healthy aging in particular! As the proportion of aging people in our population increases steadily, global strategies accompanied by extensive research are necessary to tackle society and health service challenges. World scientists recommend healthy aging scores as measurements, which combines multiple aspects to avoid a dichotomous categorization and display the bio-psycho-social concept of healthy aging [2].
Although Japanese men live for 84.71 years, but their HALE is around 72,68 a gap of 12 years. and Japanese women have an ALE of 87.74 years and HALE of 75.38 years a gap almost 12 years. Subtracting "average healthy life expectancy" from "average life expectancy", both men and women in Japan have about 12 years of time “requiring care from others". In India this gap was about 5 years in 2019 as compared to 12 years in Japan. Minimizing this time gap must be the core content of Public Health Globally [6].
While many agree that “health span” can be defined as the period of one’s life that one is healthy, However, being “healthy” means different things to different people. A better definition must include being free from serious disease, which leads to disability or death [3]
Aging is the physiological, universal, but not uniform process of getting older, which every person will experience, albeit at an individual rate, but with the variability of aging rates, it is essential to distinguish between chronological and biological age. While chronological age only reflects the time since birth, biological age relates to the wide range of physical, physiological, and cognitive functions and their maintenance, both provoked by molecular and cellular processes and social and spiritual lifestyles. Therefore, it is challenging to find a universal definition of normal aging, The Average Healthy Life Expectancy (HALE) [1].
As the vast majority of variation in how old people live is due to their health behaviors, eating nutritious diet rich in antioxidants and anti-inflammatory polyphenols, that prevent chronic diseases like diabetes, cardiovascular disease, obesity, and cancer, complimented by Regular exercise, Avoiding Smoking, Maintaining a healthy weight (avoiding becoming overweight or undernourished -emaciated), drinking alcohol only in moderation and getting enough sleep (at least 7hrs including half an hour nap in the afternoons) are important for healthy aging. Managing stress through meditation or spiritual leaning, staying in touch with family & friends, and getting regular medical checkups contribute to a longer & healthier life. National authorities must improve healthy average life expectancy by creating programs to address specific health issues, such as cancer, diabetes, cardiovascular diseases, blindness, mental health, and deafness, allocating resources to regions with more older adults to ensure equitable access to healthcare, providing universal health coverage (UHC) so that people have access to quality health services without financial hardship, Providing financial support to develop health facilities and ensure services. Implementing targeted health promotion initiatives, to address health issues like chronic diseases and mental health concerns and Iodine and Iron fortification to the population to address their deficiency. Most importantly the countries must strive for Pollution free air, water and climate change. As of 2024 most countries have given statements of good intentions with not adequate efforts for overall global concerns!
India is with a rapidly growing aging population, has 10.7% a total population of 1457 million with about 150 million over 60 years old in as of 22 December 2024 which is expected to double (20% of the population) by 2050. We are already witnessing that elders face a range of physical, mental and social issues that impair their health and quality of life. With increasing younger populations going abroad or busy facing technological and career challenges, elders find themselves isolated or neglected and need a better environment for better health and quality life.
The infectious (bacterial and fungal) communicable diseases, Nutritional deficiencies, access to health care services due to inadequate healthcare facilities, shortage of healthcare professionals, Pharmaceutical & medical production and supplies, are country specific struggles mainly in low- and middle-income countries including India. The key common health challenges across the globe include:
Pollution: Human activities like using fuel and paint products that contain toxic heavy metals can cause air, water, and soil pollution, are significant threats in developing countries. Climate change: As temperatures increase, the global disease profile and epidemiology is changing. This climate change is a major health threat in the near term. Infectious, perinatal, and nutritional disorders: Poor populations often face a high burden of infectious, perinatal, & nutritional disorders, especially among children, women and elderly. Non-Communicable diseases (NCDs): NCDs like Obesity, Diabetes, Hypertension, CCF and Cancers leading problems in developed countries but are also challenging developing country’s health systems in prioritizing their strategies. Other Public Health Influencing issues: Literacy rate, Infrastructure both health and general, Life expectancy, gender discrimination, and Population growth rate, all of them are better in developed countries and add value to public health achievement.
Developed countries are industrialized, have high standards of living, and have strong economic growth. Developing countries are agrarian and are not very industrialized, have lower standards of living, and have a very weak economy with slow growth. Challenges in Healthcare in Developed Countries are a shortage of Primary healthcare professionals, accessibility to primary health care round the clock, and difficulty of those without health insurance and the Cost of health Care in general. Dependency on digital health care is becoming a mechanical solution, with the least attention to human touch in medical care. Most astonishing development is of the progress in tertiary case, Robotics and Artificial Intelligence and research at the cost of Primary Health Care and Infectious Diseases.
Developing Countries: The major health problems in low- and middle-income countries are infectious, perinatal and nutritional disorders, with highest burden of these problems in children, women and elderly. Challenges in Healthcare in these Countries include limited availability of healthcare services especially secondary and Tertiary care because of inadequate healthcare facilities, a shortage of specialists and superspecialist beyond major cities, and a lack of essential medical supplies and drugs of good quality.
This article is an effort to analyze these health situations and efforts by all countries, appreciating on one hand the increasing Life expectancy and the challenge to the Global Goal of Healthy Life Expectancy!
Table .1 Public Health Difference
Developed Countries | Developing Countries |
Lesser to Moderate Populations | Large Populations |
Low population growth rate | High population growth rate |
Advanced Health infrastructure | Less developed Health Infrastructure |
High life expectancy | Lower life expectancy |
High Human Development Index (HDI) | Low Human Development Index (HDI) |
Poor Primary Health Care | Better Primary Health Care |
PHC too Privatised- waiting time days to weeks | States Accountable for PHC- Round the clock free |
Teleconsultation, Robotics &AI | Human touch |
Well-developed Tertiary Care but Costly | Fairly developed Tertiary Care at one third cost |
Greater emphasis on tertiary and quaternary Care | Emphasis on primary and secondary Health Care |
Advanced technology and innovation | Lag in technology and innovation |
Specialists Health Professionals | Multi-tasking health Professionals |
Access: Claim better access to healthcare based on hospital beds and physicians per capita, and better equipment. | In developing countries, healthcare professionals are often in short supply, and infrastructure is inadequate, especially in rural areas. |
Quality: Claim higher quality healthcare services. More comprehensive financing systems and spend more per capita on healthcare. | People pay for healthcare out of pocket, which can create financial barriers, Access to PHC is much better |
Outcomes: Claim better health outcomes and population health indicators due to better access quality services, and higher socioeconomic development | Outcomes: Tertiary care outcome as good as developed country at half the cost. In Public sector health outcomes can be better and population health indicators poor due to lesser investment access & quality services, & lower socioeconomic development |
Medicines: Have both conventional and naturopathic medicines available, but costly | Rely more on naturopathic system (ISM) instead of Allopathic medical system, especially for Minor ailments due to cost |
Table 2. Developmental Differences
Developed Countries | Developing Countries |
High GDP per capita | Low GDP per capita |
High literacy rate | Lower literacy rates |
Advanced infrastructure | Less developed infrastructure |
High life expectancy | Lower life expectancy |
Low population growth rate | High population growth rate |
High Human Development Index (HDI) | Low Human Development Index (HDI) |
Strong and stable political structures | Often unstable political structures |
Diversified economy | Economy largely dependent on a few sectors |
Greater emphasis on tertiary and quaternary sectors | Emphasis on primary and secondary sectors |
Advanced technology and innovation | Lag in technology and innovation |
Table 3. Key Life Expectancy- General, Men & Women by Countries – UN 2023
Sl. No/ Rank | Country | Life expectancy of Gen. Population @ Birth yrs | LE of Men @ Birth yrs | LE of Women @ birth yrs |
1/1 | Hongkong | 85.51 | 82.84 | 88.13 |
2/1 | Japan | 84.71 | 81.69 | 87.74 |
3/39 | Germany | 81.38 | 79.02 | 83.76 |
4/40 | United Kingdom | 81.30 | 79.36 | 83.21 |
5/55 | USA | 79.3 | 76.86 | 81.85 |
6/65 | China | 77.95 | 75.20 | 80.93 |
7/105 | Bangladesh | 74.67 | 73.03 | 76.37 |
8/131 | India | 72.00 | 70.52 | 73.60 |
| WORLD | 73.17 | 70.55 | 75.89 |
In 2023, UN estimated the global average life expectancy for general population as 73.17 yrs, for men as 70.55 years, and for women as 75.89 years. The same by continent was reported to be- Europe: 75 years for men and 81 years for women, Northern America: 74 years for men and 80 years for women, Asia: 72 years for men and 76 years for women.
Looking at the countries data, Hongkong is estimated to have highest average life expectancy general 85.5 yrs, for men of 82.84 years, and the average for women of 88.13 years. Average life expectancy for men in UK was 79.36 years, and for women was 83.21years. Average life expectancy for men Japan was 81.69 years, and for women was 87.74 years. average life expectancy for men in the USA was 76.8 6years, and for women was 81.85 years. Average life expectancy for men in India was 70.52 years, and for women was 73.6 years.
Current differences in Average Life Expectancy (ALE) and Healthy Average Life Expectancy: The best example of ALE of Japanese men and women were 84.71 and 87.84 years, while their HALE for men of 72.68 and women of 75.38 years, indicated a gap more than 12 years in 2023. Both men and women in Japan require care from others for more than 12 years, clearly a social and economic burden. In 2019, this gap was about 5 years in India as compared to 10 years in Japan. Both individuals and national governments have multiple responsibilities to fulfil the dream HALE of 80 years by 2030. Discussions:
Modern medicine has increased life expectancy over the past 100 years, with the global life expectancy doubling in the last century [2]. But this has not necessarily been accompanied by an equivalent increase in healthy life expectancy [3]. People are living longer but at least 10-12 years of those years are burdened by chronic heart disease, diabetes, Chronic Kidney disease, Rheumatoid arthritis or Osteoporosis, Sarcopenia, Mental health issues and cancer. Lifespan is the total number of years we live whereas health span is how many of those years we remain healthy and free from disease not needing others help [1]
The figures of Life expectancy serve as an indicator of the quality of healthcare in the respective countries and are influenced by various factors, including the prevalence of diseases such as Covid 19, HIV/AIDS CVDs, Cancers and Diabetes etc. There are challenges in comparing life expectancies across countries due to disparities in data reporting and collection standards. As ALE of a country does not indicate the morbidity among elderly, from the beginning of the current century there is a tendency to estimate the healthy life expectancy (HALE), the average number of years that a person can live in "full health".
The Healthy Life Expectancy (HALE) is a measure of how many years a person can expect to live in good physical and Mental health, independently, free of disease and disability. HALE is a more nuanced way to understand health outcomes than life expectancy alone, as it considers both morbidity and mortality. However, this author likes to redefine HALE as Good enough physical, Mental, Social and Spiritual wellbeing, leads a day-today’s life comfortably without anybody’s support irrespective of implicit or explicit disease or disability, if they allow the individual to do so. This modification is suggested because in today’s time there are diagnostic facilities to identify diseases at nascent stage with no signs and symptoms. However, such facilities are available mostly to urban affordable population. Based on this understanding how many countries in the world can achieve HALE of 80 years by 2030 as a first target? is the challenge for Global communities and Country leaders!
While it is a fact that only about 20% of how long we live is dictated by our genes, the other 80 percent is dictated by our lifestyles. This means we have incredible power and control over our health in preventing chronic diseases and increasing our longevity. While increasing the Life expectancy is good but not good enough if this gap is greater than 5 years in the current ear and trying to bridge this gap to 2 years in the next century, must be the core content of Public Health Globally.
Some populations worldwide live for long with lower rates of chronic diseases. These areas called “Blue Zones” are geographic areas in countries like Italy, Greece, Japan, Costa Rica, and the United States. The epidemiological studies indicate that diet, fasting, and exercise are the factors associated with such healthy longevity in Blue Zones. The researchers drew blue circles around them on a map, therefore, this non-scientific term has become popular [5].
The five known Blue Zones include i) Icaria is an island in Greece where people eat a Mediterranean diet rich in olive oil, red wine, and homegrown vegetables ii) The Ogliastra region of Sardinia is home to some of the oldest men in the world. They live in mountainous regions where they typically work on farms and drink lots of red wine iii) Okinawa (Japan) is home to the world’s oldest women, who eat a lot of soy-based foods and practice tai chi, a meditative form of exercise iv) Nicoya Peninsula (Costa Rica) Here the Nicoyan diet is based around beans and corn tortillas and the people regularly perform physical jobs into old age and have a sense of life purpose known as “plan de Vida’s) The Seventh-day Adventists in Loma Linda, California (USA) are a very religious group of people, strict vegetarians and live in tight-knit communities.
A dietary analysis in the Blue Zones indicate that i) They eat source of fibre and many different vitamins and minerals, through more than five servings of fruits and vegetables a day that significantly reduces the risk of heart disease, cancer, and death , ii) Their diet consists of legumes like beans, peas, lentils, and chickpeas, which are rich in fibre and protein iii) Consume whole grains which are also rich in fibre, A high intake of whole grains fibre reduce blood pressure and is associated with reduced colorectal cancer and death from heart disease iv) Nuts again great sources of fibre, protein, and polyunsaturated and monounsaturated fats combined with a healthy diet, reduce mortality and help reverse metabolic syndrome [3] v) Long-term calorie restriction, intermittent fasting, stopping eating when one feels 80% full, rather than 100% full, vi) eating slowly to reduce hunger and increase feelings of fullness, (compared to eating rapidly) are additional practices that influence dietary control. The hormones that make us feel full only reach their maximum blood levels 20 minutes after we eat. vii) Last not but the least is to eat our smallest meal in the early evening and then not eat for the rest of the day. The other key lifestyles that help in minimizing stress, were moving regularly throughout the day, having a clear sense of purpose and friends to spend time together [5].

To summarize the ten messages of Blue Zones to emulate include i) Move naturally through the day ii) Find a purpose in life iii) Manage stress through relaxation iv) Eat until 80% full only v) Eat mostly plant-based foods vi) Enjoy wine in moderation vii) Build a supportive community and a sense of belonging and viii) Prioritize family and friends ix) Supportive social circles x) Rest and Recovery through Adequate sleep for restorative care, Everyone must listen to their bodies, ensure they get enough rest, and take naps when needed [5].
The decrease in mortality and the subsequent upsurge in life expectancy accompanied by the decline in incidence of morbidity are being made possible by a planned comprehensive health care system with the inclusion of preventive, curative and restorative measures along with adequate care. However, to minimize the gap between average life expectancy (ALE) and healthy life expectancy (HALE), demands two pronged strategies i) Individual efforts like-maintaining a healthy lifestyle including eating a healthy diet supported by prosthetic dental support for good mastication, exercising regularly, especially core muscles strengthening, stop smoking if used to in younger age, avoiding Obesity and Emaciation by maintaining a healthy weight and avoiding alcohol or drinking only moderate amounts of alcohol. Most importantly stimulating our brain by learning a new skill or language or doing other activities that require mental effort and trying to engage fully in life mentally, physically, spiritually and socially ii) The national efforts include providing healthy environment by minimizing Pollution, Climate Change and Human movements, launching programs for community screening for non-communicable diseases, like Cancers, Diabetes, Hypertension for early diagnosis and management closer to the communities. Influencing health behaviours through media and interpersonal communication and community systems strengthening are the needs of all countries [5,6].
The difference between total and healthy life expectancy indicates how many years people spend with a disease or disability. On average, healthy life expectancy is five years shorter than life expectancy at age 60. This means that older people are likely to spend 25% of their life after age 60 in illness or with injury.
How to Recognise the need for support to elderly from Others:
30 Seconds Sit to Stand Test:
The 30 Second Sit to Stand Test is (also known as 30 Second Chair Stand Test -30CST), designed for testing leg strength and endurance in older adults. This test developed to overcome the floor effect of the five or ten repetition sit to stand test in older adults.[8] There is also some consideration for its use as a physical performance test in younger adult and athletic populations and MICU Patients.
Administration: The 30-Second Chair Test is administered using a folding chair without arms, with seat height of 17 inches (43.2 cm). The chair, with rubber tips on the legs, is placed against a wall to prevent it from moving.

- The participant is seated in the middle of the chair, back straight; feet approximately a shoulder width apart and placed on the floor at an angle slightly back from the knees, with one foot slightly in front of the other to help maintain balance. Arms are crossed at the wrists and held against the chest.
- Demonstrate the task both slowly and quickly.
- Have the patient practice a repetition or two before completing the test. If a patient must use their arms to complete the test, they are scored 0.
- The participant is encouraged to complete as many full stands as possible within 30 seconds. The participant is instructed to fully sit between each stand.
- While monitoring the participant’s performance to ensure proper form, the tester silently counts the completion of each correct stand. The score is the total number of stands within 30 seconds (more than halfway up at the end of 30 seconds counts as a full stand). Incorrectly executed stands are not counted.
- The 30-second chair stand involves recording the number of stands a person can complete in 30 seconds rather than the amount of time it takes to complete a pre-determined number of repetitions.
The mean number of stands for 30-second sit-to-stand test:
Sl No | Age group | Male | Female |
60-64 | 17 | 15 | |
65-69 | 16 | 15 | |
70-74 | 15 | 14 | |
75-79 | 14 | 13 | |
80-84 | 13 | 12 | |
85-89 | 11 | 11 | |
90+ | 9 | 9 |
Note: A score below average on the sit-to-stand test may indicate a risk of falling.
A study conducted across six MICUs in a tertiary care hospital, with no interventions and included MICU survivors who could perform this task before their hospitalization. The inability to perform a Sit-to-stand (yes/no) was assessed at four points after discharge: upon ICU discharge, and at 1-, 2-, and 3-months post-discharge. Mortality rates were evaluated at 6- and 12-months following MICU discharge [7].
Out of the 194 study participants, 128 (66%) were unable to perform a six-to-stand independently at discharge from the MICU. Of these, 63 were totally dependent and 65 had assisted sit-to-stand function. Recovery was observed, with the sit-to-stand inability rates decreasing to 50% at 1 month, 38% at 2 months, and 36% at 3 months post-discharge, plateauing at 2 months.
Inability to sit-to-stand at 3 months was significantly associated with six-folds increased risk of mortality at 6 months with adjusted hazard ratio (aHR) of 6.01. The mortality was 21% at 12 months with a 4.2-fold increased risk of mortality (aHR 4.2). This heightened risk was independent of age, Sequential Organ Failure Assessment score, and ICU-acquired weakness. Improvement in sit-to-stand ability, even from “totally unable” to “able with assistance,” was associated with a reduced mortality risk.
The inability to perform a Sit-to-stand in MICU survivors even 3 months after ICU discharge, emphasizes the rehabilitation challenges they face. Also, those who could not perform a sit-to-stand at all had the highest mortality hazard, followed by those who required assistance suggesting its significance as a prognostic factor. In contrast, survivors who could sit-to-stand independently demonstrated the lowest risk of mortality. Since recovery appeared to plateau around two months after discharge, it is important to reassess sit-to-stand ability in MICU survivors at this point to initiate timely intervention for those in need [7].
Physical Strength Sustainability among elderly:
Core Muscles exercises strengthen our stomach and back muscles, which can improve our posture, balance, and overall quality of life. Some core exercises that elderly need to practice daily are:
- Quadruped: This core-strength exercise is called the quadruped or the bird dog:
- Start on your hands and knees. Place your hands directly below your shoulders, and line up the head and neck with your back. Tighten the abdominal muscles.
- Raise your right arm off the floor and reach ahead. Hold for three deep breaths. Lower your right arm and repeat with your left arm.
- Raise your right leg off the floor. Tighten the trunk muscles for balance. Hold for three deep breaths. Lower your right leg and repeat with your left leg.
- For added challenge, raise your left arm and your right leg at the same time. Repeat with your right arm and left leg.
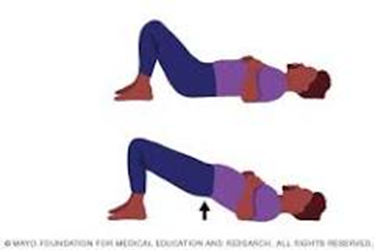
- Bridge: Lie on the back with bent knees, tighten your abs, and raise your hips until they line up with your knees and shoulders.
- Side plank with hip dip: Start in a side plank position, then push hips up toward the ceiling and slowly lower them back down.
- Deadlift, squat, and bench: These compound lifts can help you lift heavier weights while keeping your back safe.
Elderly must try repeating each exercise about five times and build up to 10–24 repetitions. If there are any health concerns, consult a healthcare professional before doing exercises.
Cognitive Rehabilitation: Cognitive challenges arise because of small blood clots, chronic inflammation, abnormal immune responses, brain injuries such as strokes and haemorrhages, viral persistence, and neurodegeneration triggered by covid. Cognitive rehabilitation therapy (CRT) focuses on restoring, strengthening, and sharpening cognitive functions that have been impaired due to an insult to brain due to injury, stroke, Covid 19 fogging or any another medical incident. Cognitive rehabilitation involves four stages of i) Education ii) Process training iii) Strategy training and iv) Functional activities training [8]. CRT has documented its positive impact for patients with long Covid 19 brain fogging since 2020. There are two different approaches to CRT: restorative and compensatory, rehabilitation therapies that encompass therapeutic techniques, such as computerized cognitive training, neurofeedback, and assistive technology.
Restorative CRT: Restorative CRT’s goal is to improve cognitive function by reinstating or strengthening the functions a person has either lost due to an injury or continues to find challenging after an illness. As an example, if a person finds it difficult to remember what he needs to do in a day or pay attention to tasks given to him by another person, a medical professional may assign different memory tasks to improve their memory, using worksheets or digital exercises that challenge memory functions. It repeatedly challenges a person to practice skills to improve their cognitive deficiencies by using the concept of neuroplasticity.

Compensatory CRT: Compensatory CRT (CCRT) helps an individual work around their injury. This is an assistive device like assistive speech devices, calendars, memory tools, smart devices, alarms to regain a person’s attention in specific contexts. Though CCRT will be temporary until an individual builds up a new skill, sometimes it may be a long-term strategy if it is not possible to restore a person’s functioning fully.
Keeping Stress Away (Meditation):
Meditation is a practice that involves training our mind to focus and redirect thoughts, reports the journal Frontiers in Psychology and many Indian Religious leaders like by Shri Shri Ravi Shankar and Vasudev Jaggi. It is a guided mental workout, where we learn to observe our thoughts without judgment, through various techniques, such as focusing on our breath, repeating a mantra, or simply observing our thoughts as they arise. By regularly practicing one can cultivate a sense of calmness, reduce stress, and improve our overall well-being. Meditation offers a tool for reducing tension by directly targeting the root causes of stress.
How Meditation Helps to Keep Tension Away: Tension has become an unwelcome companion in our hectic world. From the daily grind of work to the endless scrolling through social media, our minds are constantly bombarded with stress and anxiety. This ongoing state of overdrive can lead to tension, burnout, and a range of physical and mental health issues. However, meditation, a simple yet powerful practice, can transform our lives. This ancient technique offers a much-needed break from the chaos, a moment of calm in a world that often feels overwhelming. On World Meditation Day 21 December, millions of people explored these easy techniques to alleviate their tension & restore peace of mind through [9]:
1. Calms the nervous system:
It has been shown to lower the levels of cortisol, the primary stress hormone. “This reduction in cortisol helps to calm the body’s “fight or flight” response, which is often activated during stressful situations,”. It also promotes the activation of the parasympathetic nervous system, responsible for the “rest and digest” response. This shift in nervous system activity induces a state of relaxation and reduces physiological symptoms of stress, such as increased heart rate and muscle tension.
2. Improves focus and mindfulness: It trains the mind to focus on the present moment, reducing the tendency to dwell on past mistakes or future worries. This focused attention helps to break the cycle of negative thoughts that often contribute to tension. By observing thoughts & emotions without judgment, meditation cultivates self-awareness. Heightened awareness allows people to recognise and manage stress triggers more effectively.
3. Enhances emotional regulation: Regular meditation practice helps to develop emotional resilience, and it allows people to respond to stressful situations with a calmer and more balanced perspective, reducing the intensity of emotional reactions. It also fosters positive emotions such as gratitude, compassion, and joy, which can counteract the negative effects of stress and promote overall well-being.
4. Improves Sleep Cycle: Meditation provides a relaxing remedy for a restless mind & body. It helps to decrease stress, which is a typical cause of lack of sleep. It can also help us sleep better by reducing our insomnia symptoms. When we meditate, we achieve a state of deep relaxation in which our minds calm down and our body relaxes. This restful mood sets us up for a good night’s sleep. It also indirectly reduces tension and stress by promoting better sleep, allowing us to wake up feeling refreshed and ready to face the day.
How to meditate to reduce tension?
Here is a step-by-step guide for keeping tension at bay, as explained by a fitness expert:
- Choose a peaceful environment free from distractions, a quiet room in home, a park, or a studio.
- Sit on ground, a cushion or chair or lie down on a yoga mat in a comfortable position.
- Maintain a straight spine to support our body and prevent strain.
- Take slow, deep breaths through our nose, Exhale slowly through our mouth.
- Pay attention to the sensation of our breath entering and leaving our body.
- As thoughts arise, simply acknowledge them without judgment.
- Gently guide our attention back to our breath.
- Imagine a peaceful scene, such as a serene beach or a lush forest. Visualise oneself feeling calm, relaxed, and content.
- Start with short meditation sessions, gradually increasing the duration as we become more comfortable. Aim for at least 10-20 minutes per day.
- Practice mindfulness throughout our day, such as paying attention to our senses while eating or walking.
Begin with 5-10 minutes of meditation daily and gradually increase the duration. It takes time to develop a regular meditation practice. Don’t get discouraged if mind wanders. Approach it with a gentle and non-judgmental attitude. By practicing regular meditation, one can experience a significant reduction in tension, improved focus, and overall well-being.
Side effects of meditation: While it is generally safe and beneficial, potential side effects, especially if not practiced correctly or have pre-existing mental health conditions include:
- Some experience increased anxiety, fear, or depression, particularly if they delve into deep meditation without proper guidance.
- lead to feelings of detachment from reality or oneself.
- Physical symptoms like headaches, fatigue, or digestive issues, especially if they sit in an uncomfortable position for extended periods.
- Intense meditation can paradoxically lead to increased anxiety or difficulty sleeping.
Conclusion
The gap in Average life expectancy between men and women and the gap between Average Life Expectancy and Healthy Average Life expectancy vary in each country and is changing over time.
HALE can be defined as a good enough physical, Mental, Social and Spiritual wellbeing, allowing to lead a day-today’s life comfortably without anybody’s support irrespective of implicit or explicit disease or disability, if they allow the individual to do so.
We are already witnessing that elders face a range of physical, mental and social issues that impair their health and quality of life. With increasing younger populations going abroad or busy facing technological and career challenges, elders find themselves isolated or neglected and need a better environment for better health and quality life.
Developing elderly-friendly communities and cities and elders-friendly spaces to have a healthy life expectancy and age gracefully is the need of the time
Addressing ageism and ensuring older persons are provided an opportunity to contribute meaning fully to the society are of paramount importance.
As individuals every elderly must cultivate well-structured morning habits which significantly enhance our general well-being. Effective habits such as waking up early, staying hydrated, practicing mindfulness, nourishing our body with a healthy diet, engaging in light exercise, planning our day, reading inspiring content, and limiting screen time, to reduce stress, and increase mood, focus, and general mental and physical health.
Governments must Improve civic facilities and age-friendly institutions and robust implementation of elders-friendly policies across all societal sections.
India is nation with a rich cultural legacy and known for giving respect and care for seniors—let all of work collectively work towards ensuring that people age gracefully, lead healthy and independent life as long as they live.
The list of things to do is long, both individuals and Governments must contribute to minimize the gap between ALE & HALE, which appears to be theoretical concept and the goal of 70-80 yrs of HALE, with equity across the world appears to be an ambitious goal as of now, but efforts need to continue!
References
- undefined
View at Publisher | View at Google Scholar - undefined
View at Publisher | View at Google Scholar - undefined
View at Publisher | View at Google Scholar - undefined
View at Publisher | View at Google Scholar - undefined
View at Publisher | View at Google Scholar - undefined
View at Publisher | View at Google Scholar - undefined
View at Publisher | View at Google Scholar - undefined
View at Publisher | View at Google Scholar - undefined
View at Publisher | View at Google Scholar
