

Case Report | DOI: https://doi.org/10.31579/2835-9232/019
Epidemiology & Manaagement of Insomnia in Smaller Settings
- Suresh Kishanrao *
MD, DIH, DF, FIAP, FIPHA, FISCD, Family Physician & Public Health Consultant Bengaluru & Visiting Professor of Practice-MPH, Schools of Environmental Science, Public Health and Sanitation Management, Karnataka State Rural Development and Panchayat Raj University (KSRDPRU), GADAG, Karnataka India.
*Corresponding Author: Suresh Kishanrao, MD, DIH, DF, FIAP, FIPHA, FISCD, Family Physician & Public Health Consultant Bengaluru & Visiting Professor of Practice-MPH, Schools of Environmental Science, Public Health and Sanitation Management, Karnataka State Rural Development and
Citation: Suresh Kishanrao, (2023), Epidemiology & Manaagement of Insomnia in Smaller Settings, International Journal of Clinical Epidemiology,2(2); DOI:10.31579/2835-9232/019
Copyright: : © 2023 K. Suresh, This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 03 March 2023 | Accepted: 13 March 2023 | Published: 28 March 2023
Keywords: sleep; REM & NREM sleep stages; deep sleep; falling asleep; staying asleep; sleep spnoea; insomnia; stress; anxiety disorders;anti-depressants; benzodiazepines
Abstract
Sleep plays an integral role in health. A good night’s sleep empowers the body to recover and lets us wake up refreshed and ready to take on the day. Wouldn’t it be great if we wake up every morning more refreshed, clear-minded, energetic, and ready to face the challenges we will encounter during the day? Unfortunately, it is not so, as 33-50 % of Indian adult population, struggle to get to sleep, or toss and turn all night, or who suffer from frustrating awakenings. The COVID-19 pandemic has increased the magnitude of insomnia across the world since early 2020. In the last three decades, inadequate sleep among adolescents in all countries has almost doubled.
Based on the National Center for Sleep Disorders Research Classification, insomnia is defined as subjective complaints of difficulty falling asleep, difficulty maintaining sleep, early awakening, and non-refreshing sleep despite an adequate opportunity to sleep. The presence of one or more of these symptoms causes significant impairment to the patient’s social, occupational, or other important areas of functioning.
A recent study suggest that it is important to separate two major sleep problems falling asleep and staying asleep, the former correlates the most with decline of brain health over the years, like a computer when you try to shut down but there are files open or buggy apps that prevent it from happening. Depression, anxiety, pain, and stress impair falling asleep and are independently associated with worsening cognitive function, too.
The ideal management of insomnia consists of a balance of rest, recreational exercise, stress management and a healthy diet but most of the general practitioners in India prescribe a sedating antidepressant medication and the modern psychiatrists tend to prescribe benzodiazepines for insomnia, in patients with mood or anxiety disorders as a routine despite low-quality evidence of effectiveness or safety, for longer-term treatment.
In a general practitioner’s clinical practice patients complaining of their struggle of half the night just to get a few hours of shut eye, and then wake up feeling exhausted is common! The prevalence of chronic insomnia in a family medicine outpatient dept. in Bengaluru was reported to be around 33%, and it was associated with increasing age and diabetes. In the elderly, 15% to 45% had initial insomnia, 20% to 65% middle insomnia, 15% to 54% late insomnia, while s 10% had poor sleep quality. A Sleep Related Disorder (SRD) study in 2011 has reported that nearly 20% of an apparently healthy, productive age group of the Indian population fall in this category. It reported prevalence of insomnia is 9% in the general population and about 30% suffer from occasional insomnia. Apart from frustrating experience, not getting enough sleep can have serious consequences on their health.
Its’ family physician’s job to give appropriate remedy, not just prescribe a sleep inducing medication.
This manuscript is an effort to help the family physicians and general population to understand epidemiology -the different stages of sleep help & how they help our body, 2. the type of sleep that helps restore alertness, 3. how to wake up feeling refreshed. 4. proven ways to fight insomnia, 5. health problems that may be making it tough to sleep, 6. the best treatments for snoring and sleep apnoea and 7. Treating insomnia in practice involves sleep-inducing medication, cognitive behavioural therapy for insomnia (CBT-i), or a combination of both.
Materials & Methods: This article is based on the personal experiences and observations and interactions with multiple family physicians’ and individuals approaching the general practitioners.
Introduction
Sleep plays an integral role in our health. A good night’s sleep empowers the body to recover and lets you wake up refreshed and ready to take on the day. Wouldn’t it be great to wake up every morning more refreshed, clear-minded, energetic, and ready to face the challenges we will encounter during our day? Unfortunately, 33-50 % of Indian adult population, struggle to get to sleep, or toss and turn all night, or suffer from frustrating awakenings [1]. The COVID-19 pandemic has increased the magnitude of insomnia across the world since early 2020. A recent study suggest that it is important to separate two major sleep problems falling asleep and staying asleep, the former correlates the most with decline of brain health over the years, similar to a computer when you try to shut down but there are files open or buggy apps that prevent it from happening. Depression, anxiety, pain, and stress impair falling asleep and are independently associated with worsening cognitive function, too [2]. In the last three decades, inadequate sleep among adolescents in all countries has almost doubled.
Based on the National Center for Sleep Disorders Research Classification, insomnia symptoms can be defined as subjective complaints of difficulty falling asleep, difficulty maintaining sleep, early awakening, and non-refreshing sleep despite an adequate opportunity to sleep. The presence of one or more of these symptoms causes significant impairment to the patient’s social, occupational, or other important areas of functioning [5].
In India a general practitioner’s clinical practice, patients complaining of their struggle of half the night just to get a few hours of shut eye, and then wake up feeling exhausted is common! One in 3-4 patients have this symptom. The prevalence of chronic insomnia in a family medicine outpatient dept, in Bengaluru is reported to be around 33%, and it was associated with increasing age and diabetes. In the elderly, 15% to 45% had initial insomnia, 20% to 65% middle insomnia, 15% to 54% late insomnia, 10% had poor sleep quality [6]. A Sleep Related Disorder (SRD) study in 2011 has reported that nearly 20% of an apparently healthy, productive age group of the Indian population fall in this category. It reported prevalence of insomnia is 9% in the general population and about 30% suffer from occasional insomnia [6].
Most of the doctors across the world prescribe pharmacologic treatments containing Benzodiazepines, despite low-quality evidence of effectiveness or safety, particularly for longer-term treatment. Benzodiazepine abuse has reached epidemic levels. An acute overdose occurs when excessive benzodiazepines are taken, intentionally for suicide or accidentally. Most chronic overdoses occur when benzodiazepines are combined with other central nervous system depressant drugs, such as alcohol and opioids! The prevention of chronic insomnia consists of a balance of rest, recreational exercise, stress management and a healthy diet [3,6], Positive lifestyle changes, and cognitive behavioural therapy are the first-line treatments. Treating insomnia in practice involves sleep-inducing medication, cognitive behavioural therapy for insomnia (CBT-i), or a combination of both. The prescribed amount ranges from 0.25 to 0.5 mg daily divided in 2-3 doses, for the shortest period possible, as recommended for 2-4 weeks. Intermittent use may help to avoid addiction. Young people who take benzodiazepines for an extended period are at risk of developing numerous adverse conditions, including tolerance, dependence, and withdrawal upon discontinuation. The classic presentation of an isolated benzodiazepine chronic overdose consists of CNS depression with normal vital signs. If benzodiazepines are taken for 2 weeks or longer, it is recommended that the user should not abruptly stop taking this drug, but gradually taper over an extended period.
Cases of Insomnia & Obstructive Sleep Apnoea:
1. A case of adjustment disorder: Mr Prahalad, a 40-year-old man reported to me with difficulty falling asleep and maintaining sleep in January 2020. The history revealed that it all started after the death of his wife 2 months ago. He has had no previous sleep problems. He was unable to fall sleep until at least an hour after going to bed. A general practitioner (GP) he consulted had prescribed low dose of tricyclic antidepressant (Amitriptyline Tablets BP 25mg) as sedation, but he was unable to tolerate the drowsiness and dry mouth caused by the medication. He consumed 4 cups of coffee during the day to keep alert. Of late he took alcohol at night to aid sleep. The patient’s 15-year-old son noted that his father’s legs jerk occasionally during the sleep though patient was not aware of these movements. My analysis suggested that the insomnia was related to acute stress, conflict, or recent environmental change. The precipitating event in this case is the death of his wife. Called as Adjustment sleep disorder is usually a self-limiting disorder, often resolving once the patient comes to terms and copes with the stressor. The course is usually transient lasting from a few days to less than 2 weeks. However, the sleep difficulty may last up to 3 months. As Prahalad had no previous sleep problems and the onset of his sleep problem after a major stressful event made me to diagnose it as adjustment sleep disorder. Inadequate sleep hygiene (consumption of coffee and alcohol at bedtime, stress at bedtime) contributed to his sleep difficulty. The Periodic limb movements of sleep (PLMS) were considered for exclusion later polysomnographic evaluation. PLMS are involuntary movements of the legs, occurring every 20-40 seconds, consisting of dorsiflexion of the ankle, flaring of the toes and sometimes with flexion of the knee.
Management: I put him on an intermediate-acting benzodiazepine (Restoril) for 2 weeks to relief his sleep difficulty while behavioural measures and counselling were given. The presence of depressive symptoms warranted the use of escitalopram (Cipralex) a selective serotonin inhibitor (SSRI) during daytime fearing aggravation of Insomnia. After 4 weeks counselling, he was fully recovered from his problem of Insomnia and PLMS.
2. A case of Sleep Hygiene correction: Arun a 22 -year-old MPH student, from the University I go as visiting Professor of Practice sought my opinion in visit in November 2022 after taking diazepam 10mg tablets, taken each night for 10 days based on the prescription of local general practitioner. His main complaint was Insomnia for last five weeks. He used to wake up at 7:00am to attend his lectures, but since last 5 weeks he would wake up fully at 4:00am. He had no difficulty to fall asleep, nor did he wake up too frequently during the night. During the day, he felt tired, anxious, and tearful. Despite taking the tablets for 7 days he reported that he is still not able to sleep properly and therefore stopped abruptly.
I tried to analyse the possibilities of depression; as Arun presented, I suspected the existence of an underlying depression. He had recently increased caffeine intake to cope with his pending academic commitments. He appeared to be suffering from a short-term, exam-related, stressful situation. I also suspected delayed sleep phase syndrome due to going to bed too late (past 1100 PM), a first experiences outside the family environment. The prescribed drug a Diazepam is a benzodiazepine, more reliably absorbed following oral rather might have caused by precipitation in the muscle. A second plasma peak occurring four to six hours after initial administration. His roommate was waking up early morning for studies and with the lights on this guy was finding it difficult to sleep after 0400hrs.
I counselled him to reduce coffee intake after 1600hrs, reassured that he is preparations for exams are good enough and he need to worry much and arranged of changing the room partnering him with some other student having similar routine, that helped him in about 2 weeks’ time.
3. A case needing Stimulus Control Therapy: This is case reported by one of practicing doctor in Gadag. Purnima, a 45-year-old cook by profession complained of inability to sleep well for more than 2 years. She regularly goes to bed at 10 pm but is unable to sleep until 1 am. She experiences about 3-5 awakenings every night and with each awakening requires about 30 minutes to fall asleep again. Purnima also experiences daytime fatigue and is unable to concentrate in her work. She cannot and does not take naps during the day due to her professional demand. She does not snore and has no usual limb movements during sleep as reported by her husband. Her general health has been good. She vaguely recalls being involved in a stressful family property dispute just prior to onset of her sleep difficulty. As bedtime approaches, she becomes very tense and worries about the prospect of another sleepless night as “Sleep has become a real frustration. Every night, when she lies on bed, she must try very hard to sleep and keeps watching the clock. She did not take any sleeping pills and has no symptoms of depression. There is no marital conflict. On further questioning, she surprisingly admitted that she sleeps well while on vacations and relatives houses.
I suspected that she has formed an association between the home bedroom environment and not sleeping. Her sleep environment has therefore become a conditioned stimulus for sleep difficulty. As bedtime approaches, she anticipates another sleepless night that results in increasing tension and arousal. The harder she tries to sleep, the less likely she will fall asleep. Therefore, I diagnosed it as Psychophysiological chronic insomnia as the above learnt behaviours seem to have a dominant role in the insomnia and no other associated medical or psychiatric diseases to explain the insomnia.
The mainstay of management of chronic insomnia is behavioural therapy. The patient was asked to maintain a sleep diary. I asked our doctor to try Stimulus control therapy. Of the behavioural therapies, Stimulus Control Therapy is particularly useful. We asked her to change her sleeping place, mattress and sleep away from her husband for a month. The objective of stimulus control therapy is to help the patient learn to re-associate bedtime and the sleep environment with sleeping and correct learned maladaptive behaviour that disrupt sleep. We prescribed an Intermediate-acting benzodiazepine (lorazepam) for a period of about 2 to relief the patient’s distress and then slowly reduced over another 2 weeks (switching from daily to alternate nights, and twice week and finally as needed) while Behavioural techniques continued for 10 weeks to learn and provide clinical benefit. By end of 3 months, she was fully comfortable and continued to sleep with her husband but in the changed room.
4. Insomnia due to Stress working from Home: Kshama a married, self-employed woman in her 30’s with 1 young child, as she my tenant for last one year in one of my flats in Whitefield in Bengaluru approached me in March 2021 for Insomnia. In our first session, she talked about feeling irritable, tired all the time and not as patient with her kids as she’d liked to be. Her sex life was non-existent. Her family doctor prescribed Xanax (Alprazolam used to treat anxiety disorders and panic disorder) to help her sleep. Even though the Xanax helped her sleep, she didn’t want to rely on it or become addicted to the medication. A detailed interview reviewed that she felt anxious at bedtime. The thought of going to sleep had become very stressful. Falling asleep when anxious is tough, but trying to relax when feeling anxious was worst. Once Kshama fell asleep, she did not stay asleep for long. When she woke, her mind started reeling about a myriad of issues or obsessing about one thing. Her family physician had cleared her of possible physical health issues that could affect her sleep. We talked about her experience of her sleep problems. I educated Kshama about sleep hygiene restricting her caffeine intake, stopped using her computer and watching TV 2 hours before bedtime, and made sure she had some down-time before bedtime to let go of the issues from the day. She also adjusted her bedroom light to be less bright.
Next, I decided to use Brain spotting (BSP) a non-verbal treatment that helps the patient reprocess issues that interfere with your life. With the headphones on (accessing bilateral music and sounds), she thought about how she felt (both emotionally and physically). I noticed that her eyes focused on one spot, her brain spot. The relationship we had built helped Kshama feel safe so that she could reprocess whatever arose for her. Our BSP session that day lasted about 45 minutes. At the end of the session, we talked about her experience during the processing. In our 6th session (Bi-weekly), Kshama said she hardly uses Xanax anymore. Most of the time, she falls asleep easily and sleeps through the night and wakes up feeling rested after 8 hours of uninterrupted sleep. She reported being more patient with her child and husband and can maintain better focus at work and has a sex life again.
5. A case of Insomnia among Elderly lady: This patient is my contemporary (76-year-old) a man with a primary complaint of sleeplessness and sleepiness for approximately 8 months. Initially, he only had difficulty staying asleep 2-3 nights per week and sleep and daytime fatigue have increased in severity and frequency over the past 5 months. He now wakes up 3 or more times per night and on most nights has difficulty falling asleep (taking about 40 minutes to an hour). He has tried to maintain an active social and professional life. He was the executive director of a non-profit organization, and now heads his own consulting company. He noted increased irritability and lack of motivation since last 2 months. He has always been a poor sleeper during times of stress, but always improved after a few days. For this occasionally he used to take over-the-counter medications. History also revealed that he noted an increase in his caffeine intake (6 cups of coffee and 1-3 cups of tea per day). The patient's medical history included hypertension, osteoarthritis, Benign hypertrophy of Prostate and a "mild" stroke about 4 years ago, with no recurrent symptoms since. Due to fatigue, he has been unable to exercise, which has increased his arthritis-related pain, and he has gained over 6Kg during the past 6 months. His medications included atenolol, hydrochlorothiazide, diphenhydramine for sleep, and acetaminophen and ibuprofen for pain. He is married with 3 children (F-2, M-1) and has 1 grandchild from eldest daughter. His wife complained that she, too, was sleeping poorly because she was disturbed by his restlessness. Mental, neurologic, and physical examination was within normal limits, with the exception of a body mass index of 31 and a blood pressure of 135/92 mm Hg.
Based on all the above I diagnosed him having the comorbid type of insomnia. This patient had factors, such as depression, chronic pain, other sleep disorders, and obesity. The patient was educated regarding good sleep hygiene and specifically advised to maintain a regular sleep-wake cycle, reduce his caffeine intake, resume regular exercise (within 3 hours of bedtime), after blood test for a complete blood count, thyroid-stimulating hormone, and routine chemistry was done and most biomarkers were normal. At his follow-up visit, after one month the patient said that he has increased his exercise (walking and weights) level to 5 times per week and has tried to adhere to the sleep hygiene instructions. He has noted improvement in falling asleep but continues to wake up four times during the night and remains sleepy during the day. He continues to take over-the-counter medications to help her fall asleep 2-3 times per week, but they tend to produce a "hang-over" effect. He continues to be irritable, no longer enjoys going out with his friends, and is getting into more arguments with his wife. As he had added another Kg of weight in last one month, I suspected depression and began pharmacologic treatment and referred him to a psychiatrist.
6. A case of Behavioural Insomnia in a Child: Sohil, my grandson is an 8-month-old healthy boy, and his parents (my son and daughter in Law) were in Bangalore in November 2022. His parents reported that since birth, Sohil requires to be put on one of the parents’ chests and a Pink music sound played from a mobile phone to go to sleep. They had a similar approach to elder son until age 3 years. Sohil wakes up frequently during the night, and in each awakening, needs one parent to take on their chest to put him back to sleep. For me this appeared to be typical case of childhood behavioural insomnia, typically characterized by bedtime resistance, inability to sleep independently, and/or frequent night-time awakenings. Suspecting that this may result in behavioural issues like hyperactivity and inability to concentrate, I decided to treat. I advised behavioural interventions starting from improving the bedtime routine, that included activities relating to feeding, morning bathing after a massage, communication such as playing soft music and parents engaging for about 15-20 minutes, and physical contact of taking the boy on their chest. After 2 weeks I introduced graduated extinction, in which the child was “ignored” for specific periods of time on a fixed schedule or with increasing intervals before a caregiver checks in. These check-ins typically involve minimal interactions to avoid reinforcement of crying and tantrums. This routine resulted in earlier bedtime, shorter sleep onset latency, fewer night-time awakenings, and longer sleep duration in about 6 weeks of their stay. The boy now 10 months old has no issues back in Saint Jose, SF, USA.
7. A case of Snoring, Sleep disturbance due to Tonsillar Hypertrophy: Bunty a 6-year-old male recently diagnosed with attention-deficit hyperactivity disorder (ADHD) was referred for snoring to an ENT specialist friend. His parents reported that for the past year, he has snored nightly. His mother recently noticed pauses in his breathing when he sleeps. On examination our friend Paediatric otolaryngologist found that his Tonsils and adenoids had occupied nearly 65% of the oropharynx, that comes under grade 3+. The parents were advised and agreed to go for adenotonsillectomy as there were no contraindication to surgical treatment like active infection, hematologic disorders, and any uncontrolled systemic disease. After the surgery the problem was resolved with no complications.
8. A case of Narcolepsy: Narayana a 10-year-old male with no significant medical history was brought to a paediatrician friend of mine in early 2023 for insomnia. His mother reported that for the past 6 months, he has been falling asleep in school unexpectedly and his academic performance has suffered. He has also had significant unexpected weight gain and several unexplained falls. Keeping the complaint of excessive daytime sleepiness, he was suspected to have Narcolepsy type 1, with cataplexy a chronic sleep disorder. Cataplexy is a brief episode of sudden loss of muscle tone, precipitated by strong emotions, and without loss of consciousness vary from mild weakness to complete collapse, for less than 1 min. It’s estimated prevalence in India is 25 to 50 cases per 100,000 people & an incidences of 0.74 per 100,000 person-years, equally common in boys and girls. He was treated with adherence to good sleep hygiene with a consistent sleep schedule and scheduled daytime naps and Adderall XR Capsules 5 mg (amphetamines) daily. At a follow-up after one months, most of his complaints were reduced and the monitoring continues.
Discussions:
Four stages of sleep and what matters most: There are four stages of sleep, and their Role are:
- NREM Stage 1 sleep: 5-10 minutes of transition between wakefulness & Sleep after hitting bed.
- NREM Stage 2: This stage involves the light sleep just before deep sleep, body Temperature & heart Rates drop, Brain begins to produce sleep spindles, last for approx.20 minutes
- NREM Stage 3: Muscles relax, BP & RR drop & deep sleep begins. Lasts for about 45 minutes after sleeping.
- Stage 4 REM sleep: Brain becomes more active; body is relaxed and immobile. Dreams may occur and eyes move rapidly.
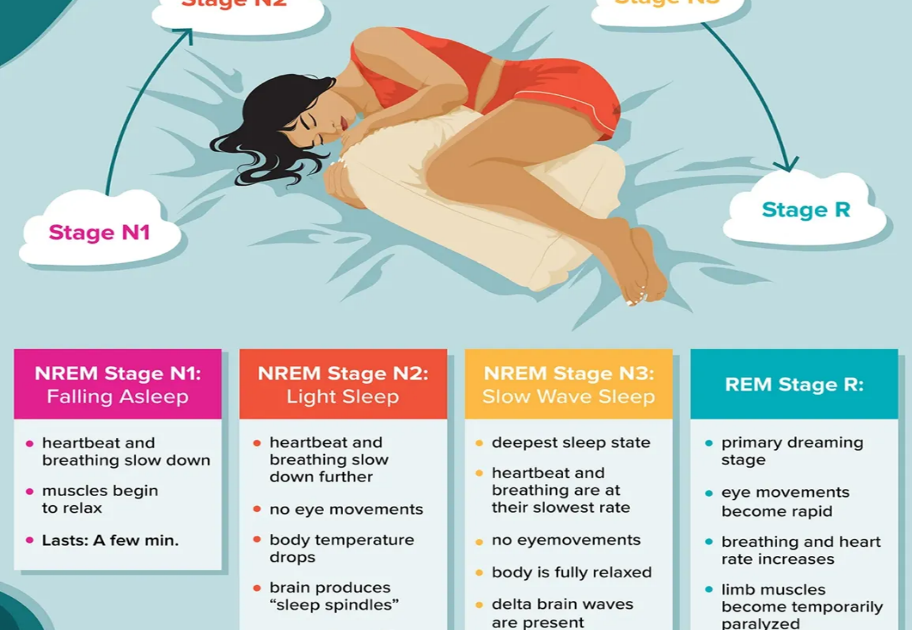
Rapid eye movement (REM) sleep is the deepest stage (4) of sleep. The irises of our eyes move rapidly during this stage. This happens approximately 90 minutes after falling asleep. Our heartbeat is faster and irregular during this stage, body is largely inactive during. Deep sleep is associated with changes in the body rather than the brain. To improve Deep Sleep a conscious effort must be made to: Work Out Daily, Eat More Fiber., find our Inner Yogi, avoid Caffeine 7+ Hours Before Bed, resist that nightcap, create a relaxing bedtime routine. make your bedroom a sleep sanctuary and listen to white and pink noise. White and Pink noises can reduce brain waves, allowing individuals to fall asleep faster. The humming sound masks the loud sounds that disrupt our sleep, allowing us to go to sleep faster and stay asleep longer. White noise has also been shown to improve memory, tinnitus, and concentration. Pink noise is a preferred method by many because it gets deeper sleep than white noise. Brown noise, also known as red or Brownian noise, has higher energy at lower frequencies, which creates an even deeper sound than pink noise [4].
There are data to suggest that insomnia may be an early indication of depression, but there is currently no evidence that early treatment will prevent depression. A new study provides more evidence that insomnia may contribute to cognitive decline in older adults and shows that difficulty falling asleep in midlife may be most indicative of future cognitive impairment. Investigators found that having trouble falling asleep on most nights (vs rarely/never) was equivalent to the effect of 2 to 3 years of aging across cognitive domains 14 years later. Interventions to reduce insomnia, with a focus on difficulty initiating sleep, may be a target to optimize cognitive aging [8].
Preliminary results from the study presented during SLEEP 2021: 35th Annual Meeting of the Associated Professional Sleep Societies, provides more evidence that insomnia may contribute to cognitive decline in older adults and shows that difficulty falling asleep in midlife may be most indicative of future cognitive impairment. Investigators found that having trouble falling asleep on most nights (vs rarely/never) was equivalent to the effect of 2 to 3 years of aging across cognitive domains 14 years later. Interventions to reduce insomnia, with a focus on difficulty initiating sleep, may be a target to optimize cognitive aging [8].
The researchers analysed data on 2595 adults (mean age, 64 years; 65% women) who were enrolled in the long-running Health and Retirement Study. In 2002, participants were asked about the frequency of their having trouble falling asleep, waking during the night, waking too early, and feeling unrested in the morning. In 2014, depressive symptoms and vascular conditions were assessed. In 2016, participants' cognition was assessed using a battery of neuropsychological tests that gauge episodic memory, executive function, language, visuospatial/construction, and processing speed. The researchers performed a series of analyses in which they controlled for socio-demographics and baseline global cognitive performance and the influence of depressive symptoms and vascular disease. The results showed that frequent difficulty initiating sleep was associated with poorer episodic memory, executive function, language, visuo-construction, and processing speed 14 years later ― equivalent to 2.2 to 3.4 years of aging. No other insomnia symptoms were associated with cognitive decline. This supports that cognitive impairment in older adults is more strongly associated with difficulty initiating sleep rather than difficulty maintaining sleep. The association was not modified by gender. However, women were more likely than men to report frequent trouble falling asleep [8].
Blame It on Depression?
Frequent difficulty initiating sleep was associated with greater depressive symptoms and vascular disease burden. Depressive symptoms accounted for 12% to 20% of variance in these associations, and vascular disease accounted for 6% to 15% of variance in nonmemory associations. Ties between trouble falling sleep and later cognitive problems observed in the current study are in line with growing evidence of a relationship between circadian dysfunction and neurodegenerative diseases. Delayed circadian rhythms, can manifest as difficulty falling asleep or chronic sleep-onset insomnia, were prospectively associated with a nearly twofold greater risk of mild cognitive impairment or dementia over 5 years in a community-dwelling sample of older women.
"These findings have relevant implications for clinical practice, as sleep initiation difficulties may alert providers to patients at heightened risk for subsequent cognitive impairment. Future intervention research is needed to better understand the mechanisms and modifiability of associations between difficulty initiating sleep and cognition later in life. "Sleep has always been thought to be restorative, but only recently has modern day neuroscience shown that quality sleep actually clears the cobwebs that accumulates during wakefulness. Contrary to what many believe, the brain is quite active during sleep and resets itself, and the brain with either clearing or caching memory files and activating different processes. The brain has a garbage disposal system that clears its waste largely in sleep that accumulated during wakefulness. "It is important to separate two major sleep problems falling asleep and staying asleep, the former correlates the most with decline of brain health over the years. Like a computer when you try to shut down but there are files open or buggy apps that prevent it from happening, depression, anxiety, pain, and stress in general all impair falling asleep and are independently associated with worsening cognitive function, too [8].
When and How do patients with Insomnia approach smaller settings in India:
In my own and family Physicians or other specialists experiences majority of our clients of Insomnia approach us only when they find it difficult to fall asleep (taking more than half an hour after hitting the bed), stay asleep, or both. The less common complaints are waking early in the morning and not be able to get back to sleep, the sleep is chronically poor quality, unrefreshing sleep, or they feel constantly tired after waking up. A few complain of feeling saps in energy, mood , health, work performance and quality of life indicating to suspect some type of sleep disorder & Investigate!!
Most common Symptoms for which clients walk into smaller clinics in India include any or many of these complaints: Finding it difficult to fall asleep (taking more than 20 minutes after hitting the bed), stay asleep, or both • Waking too early in the morning and not be able to get back to sleep, • The sleep is chronically poor quality, light and unrefreshing, Feeling tired after waking up or Feel saps not only energy level, mood , health, work performance and quality of life, • unrefreshing sleep , and • Fatigue or daytime sleepiness. Other signs the physician elicits could include: • Poor attention or concentration, • Impaired performance resulting in problems with work or social life, • increased risk for errors or accidents, • Reduced energy or motivation, • Behavioural problems (i.e., hyperactivity, impulsiveness, aggression), • Mood problems, including anxiety or depression or irritability, • Headache and chronic pain • Increased suicide risk [3,5,6]
Diagnosis of Insomnia: A general practitioner or a physician Asks about sleep habits and requests to keep a sleep diary for 2 weeks & bring back in the follow-up visit. As there is no definitive test for insomnia s/he depends upon i) Sleep log/ diary is a simple diary that keeps track of details like bedtime, wake up time, how sleepy you feel at various times during the day, and more. A sleep log can also help the doctor to figure out what might be causing insomnia. Sleep diary /log helps to calculate total sleep time and helps doctor to identify sleep disruptions and other factors that can influence sleep quality. S/He Identifies the patterns that help explain sleeping problems. For healthcare providers, the concrete entries in a sleep diary are more reliable than a general recollection and become trusted Source. S/He uses sleep environment checklist ii) Sleep inventory: A sleep inventory is an extensive questionnaire that gathers information about personal health, medical history, and sleep patterns. iii) Blood tests: Perform blood tests to rule out medical conditions such as thyroid problems iv) sometimes s/he may refer sleep study in the nearest town. This is a non-invasive test and involves an overnight sleep study, or polysomnography, to gather information about your night-time sleep. In this exam, patient sleeps overnight in a lab set up with a comfortable bed and s/he will be connected to an EEG, which monitors the stages of your sleep. It also measures oxygen levels, body movements, and heart and breathing patterns.
Since 2020 periodical lockdowns due to Covid 19 Pandemic, working from home has become norm, and now hybrid working has made more important than ever to have a designated space for rest and personal time. The sleep environment plays a key role. The space to sleep should have conducive temperature between 60-70° Fahrenheit, blacking out curtains or a sleep mask to keep the room dark and free of noise. If living in a noisy area, use earplugs or other noise cancelling devices providing Pink and white music to ensure the sleep is quiet and peaceful. S/He would also assess the habits of cleaning our bedsheets and blankets on a regular basis, and if we ensure that your bed is made before going to sleep. Use a diffuser or incense to create a soothing aroma in your room, like lavender or lemon may also be assessed for well of families.
Then the Clinician Analyses the data for type healthy lifestyle habits such as a regular sleep & waking schedule, diet, exercises & causes of Insomnia. He may talk to parents, spouse or any other attendants to know about patients’ snoring, restless legs or periodic leg movements.
In some metropolitan cities and district headquarters with Medical Colleges functioning, the primary care provider may refer for i) Actigraphy a special device worn on the wrist to monitor movement, including sleep, which is more objective than a sleep diary. The results from sleep logs and actigraphy are often similar, and sleep diaries are simpler and less expensive. Sometimes Sleep questionnaires are used for community studies that involve subjective evaluations of sleep without the detailed recordings made in a sleep diary and they are less precise. ii) Sleep studies: A polysomnography is the gold standard for identifying many sleep disorders, but it is expensive and requires spending at least one night in a sleep clinic. iii) Wearable activity trackers, mobile phones, and other types of consumer sleep trackers can offer data about r sleep. Not been rigorously tested to ensure their accuracy.
Then s/he tries to identify causes as 1) Primary causes: a) adjustment disorders e.g., job loss, brief anxiety states, hospitalization, and other stressful life events b) Psychophysiological insomnia, c) Sleep state misperception and Idiopathic insomnia. Secondary causes may include a) Environmental sleep disorder - noise, temperature, humidity, b) Inadequate sleep hygiene, c) Psychiatric disorders- anxiety, depression, panic attacks, mania, schizophrenia, alcoholism d) Medical illness- respiratory disorders (chronic obstructive airway disease, asthma), rheumatologic disease, neurological disorders (parkinsonism, dementia, fatal familial insomnia), e) Medications – nicotine, bronchodilators, steroids, beta-blockers, alcohol f) Sleep wake cycle disorders- jet-lag, shift work, delayed or advanced sleep phase syndrome g) Sleep-related motor disorders - restless legs and periodic limb movements of sleep and h) Sleep related breathing disorders - sleep apnoea, chronic obstructive pulmonary disease
Clinical classification of Insomnia: Clinicians categroise Insomnia cases to facilitate management as:
- Psychophysiological insomnia: heightened arousal with excessive worry and focus on sleep.
- Idiopathic insomnia: longstanding & genetically derived, beginning in infancy or childhood.
- Paradoxical insomnia: Sleep status misperception or belief that sleep has not occurred.
- Inadequate sleep hygiene: habits that disturb sleep including naps, caffeine intake, a variable sleep schedule, and using the bedroom for non-sleep activities. sleep during the day.
- Behavioural insomnia of childhood: Sleep-onset type in infants or toddlers limit-setting type
Common causes of chronic Primary Insomnia:
From our experience represented by the case studies listed the common causes of Insomnia in preferential order are [3,5, 6]:
Stress: i) Concerns about work, school, health, finances, or family can keep your mind active at night. ii) Stressful life events or trauma -the death or illness of a loved one, divorce, or a job loss
Travel or work schedule. i) Your circadian rhythms act as an internal clock, guiding such things as your sleep-wake cycle, metabolism, and body temperature. Disrupting your body's circadian rhythms can lead to insomnia. a) jet lag from traveling across multiple time zones, b) working a late or early shift, or c) frequently changing shifts.
Poor sleep habits. i)irregular bedtime schedule, naps, stimulating activities before bed, an uncomfortable sleep environment, and using your bed for work, eating, or watching TV. Computers, TVs, video games, smartphones, or other screens just before bed can interfere with your sleep cycle.
Eating too much late in the evening: Having a light snack before bedtime is OK, but eating too much may cause you to feel physically uncomfortable while lying down. Some people experience Oesophagitis (heartburn) due to a backflow of acid and food from the stomach into the oesophagus after eating, that keeps them awake.
Medical Conditions: Acute /Chronic conditions with Cardio-Renal-Respiratory or Mental distress cause Insomnia. chronic pain, cancer, diabetes, heart disease, asthma, gastroesophageal reflux disease (GERD), overactive thyroid, Parkinson's disease, and Alzheimer's disease. Treating the medical condition improve sleep, but the insomnia may persist.
Mental health disorders: anxiety disorders, such as post-traumatic stress disorder, may disrupt our sleep. Medications: Antidepressants and medications for asthma or blood pressure. Some Analgesics, allergy and cold medications, and weight-loss products contain caffeine and other stimulants that can disrupt sleep.
Association of Insomnia with Health Conditions:
Though any acute illness can disturb our sleep for short periods, it may continue even after the condition is cured. The commonest chronic conditions resulting in Insomnia include:
Cardio-vascular diseases (CVD): Obstructive sleep apnoea (OSA) has been associated with many different forms of CVDs like hypertension, stroke, HF, coronary artery disease, and atrial fibrillation (AF). While OSA affects 34% of men and 17% of women in the general population it affects 40% to 60% of patients with CVD.
Hypertension: When a person with obstructive sleep apnoea (OSA) attempts to breathe, forced inhalations cause substantial changes in pressure within the chest cavity. This intrathoracic pressure can lead to atrial fibrillation, problems with blood flow to the heart, and even heart failure.
Weight Gain: Sleep apnoea patients have significantly higher Ghrelin levels, a hormone that makes us feel hungry, and significantly lower Leptin levels, the hormone that makes us feel full. Therefore, the individuals with obstructive sleep apnoea are more likely to feel hungry and consume more calories resulting in gaining weight, more fat accumulates around the throat, and this extra weight makes the soft palate collapse, causing worsening of an apnoea event.
Diabetes: Obstructive sleep apnoea (OSA) alters glucose metabolism, promotes insulin resistance, and is associated with development of type 2 diabetes. Chronic exposure to intermittent hypoxia and other pathophysiological effects of OSA affect glucose metabolism directly. The treatment of OSA can improve glucose homeostasis.
For academic consideration Primary sleep disorders are classified as
1.Parasomnia sleep disorders, that cause abnormal activities during sleep, such as sleep terrors or sleep walking.
2. Dyssomnia sleep disorders, that cause trouble falling asleep or staying asleep. E.g., obstructive sleep apnoea. Obstructive sleep apnoea’s may further be classified as:
- Abnormalities of the central nervous system: Central sleep apnoea occurs when breathing temporarily stops for 10 seconds or more many times during a night's sleep. It can also be caused by problems in carbon dioxide regulation. This is caused by an abnormality in the brain, which prevents it from regulating oxygen levels and automatically triggering breathing resulting in hypoxia. It can worsen conditions such as epilepsy, or lead to problems such as chest pain or heart attack in people with CAD.
- Periodic limb movements in sleep (PLMS): Involuntary movement of the arms and legs frequently during sleep. It can cause the arms and legs to twitch, jerk, or flex, as often as several times per minute for up to several hours. The cause of PLMS is unknown. It can cause daytime sleepiness and fatigue because the symptoms interrupt sleep.
- Restless legs syndrome (RLS): Restless legs syndrome is a neurological disorder. It causes leg pain, a crawling feeling in the legs, or an urge to move the legs when trying to go to sleep. The symptoms tend to occur when we sit or lie down. They are relieved by walking or moving the legs. The symptoms are worse at night. RLS may make it hard to fall asleep or stay asleep and causes excessive sleepiness during the daytime.
- Sleep apnoea (SA): SA causes you to stop breathing periodically throughout the night, & Restless legs syndrome causes unpleasant sensations in our legs and an almost irresistible desire to move them, Causing of Insomnia
- Stimulants drinking closer to bedtime: Caffeine, Nicotine, and alcohol: Coffee, tea, cola, and other caffeinated drinks are stimulants. Drinking them in the late evening or before going to bed can keep us away from falling asleep at night. Alcohol may help you fall asleep, but it prevents deeper stages of sleep and often causes awakening in the middle of the night.
- Insomnia and Ageing: Insomnia becomes more common with age. As we get older, we may experience:
- Changes in sleep patterns: Sleep often becomes less restful as we age, noise or other changes in your environment are more likely to wake you. As our internal clock advances, we get tired earlier in the evening and wake up earlier in the morning. Older people generally need the same hours of sleep (7-8) as younger people do.
- Changes in activity: As we become less physically or socially active, it can interfere with a good night's sleep. Taking a daytime nap, interferes with sleep at night.
- Changes in health: Chronic pain from conditions such as arthritis or back problems as well as depression or anxiety interfere with sleep.
- Nocturia: Benign prostate Hypertrophy or bladder problems keep waking frequently.
- Sleep apnoea and restless legs syndrome become more common with age.
- More medications: As older people use more prescription drugs, increasing the chance of insomnia associated with medications.
Sleep Apnoeas (SA):
Sleep apnoea is a serious sleep disorder in which breathing repeatedly stops and starts. The main types of sleep apnoea are:
- Obstructive sleep apnoea (OSA), the more common form occurs when throat muscles relax and block the flow of air into the lungs.
- Central sleep apnoea (CSA) occurs when the brain doesn't send proper signals to the muscles that control breathing.
- Treatment-emergent central sleep apnoea (TECSA), commonly known as complex sleep apnoea (CSA), is a case of CSA therapy for OSA.
Available data in India, obstructive sleep apnoea prevalence rate is at 14 per cent in men and 12 per cent in women. SA causes you to stop breathing periodically throughout the night, & Restless legs syndrome causes unpleasant sensations in your legs and an almost irresistible desire to move them, Causing of Insomnia.
Clinicians currently diagnose OSA by scoring partial (hypopneas) and full (apnoea's) "obstructions" to breathing during sleep. The number of hypopneas and apnoea per hour are added together to form what's called the apnoea and hypopnea index (AHI). Using American Academy of Sleep Medicine (AASM), criteria It is categorized into mild (5-15 events/hour), moderate (15-30 events/hr), and severe (> 30 events/hr). Since in many cases, hypopneas constitute most of the AHI, no one, is clear as to what a hypopnea is [9,10]. As there are more than 13 separate definitions for AHI used in the literature it varies widely by the definition employed, though OSA has dominated for 20 years, a common epistemological definition is elusive The Agency for Healthcare Research and Quality (AHRQ) has issued a statement that for want of sufficient evidence to weigh the balance of benefits and harms of screening for obstructive sleep apnoea (OSA) among asymptomatic adults and those with unrecognized symptoms, cannot be at this time recommend for or against OSA screening[10]. However, most practicing doctors identify four categories of OSA:

1. Snoring: Snoring is simply a sound made due to vibration when there is a minor blockage of our airway when we breathe while asleep. This benign blockage may be caused due to congestion, weak muscle tone, excess alcohol, or a deviated nasal septum (DNS). Snore is most common early warning signs of the condition, and people sleeping alone, may not even realize they are snoring. Someone sleeping with the clients at night (parents, spouse etc), can see and hear and inform that the client periodically stops breathing, gasp for air, and snore loudly, alerting to seek medical help. Many studies put that 20% of men and 12% of women over age 30 have been diagnosed with OSA, and up to 90% of them don’t even know it.
2. Morning headaches: A pattern of morning headaches is another sign of sleep apnoea. When there is a physical blocking of airway or brain and nerves have no control our breathing, the patient in each episode wakes up and restore breathing and oxygen levels, leading to headaches.
3. Lingering fatigue & sleepiness: A constant fatigue and tiredness is a sign of insomnia due to sleep apnoea. As the sleep cycle is being interrupted, such person doesn’t have full rest leading to Chronic sleepiness affecting the concentration ability next day at work or school. Inability to focus could lead to serious accidents, while driving, operating machinery, or any activity requiring concentration.
4. Waking up suddenly and out of breath: An unexplained jolt that wakes us up in the middle of the night with heartbeat increase and feeling of hypoxia is, yet another symptom of sleep apnoea is
Sleep apnoea left untreated can have serious health consequences [9,10].
Treatment of insomnia: The common approach for treatment of Insomnia in general practice is to prescribe medications and apply Cognitive & Behavioural Treatments gaining confidence of the client:
Most clinicians straight away start with medicines to help immediate management of insomnia. While majority of general practitioners in India prescribe a sedating antidepressant medication like Trazodone, Dioxepine, and Elavil, the modern psychiatrists tend to prescribe benzodiazepines such as diazepam, alprazolam, lorazepam, and clonazepam for insomnia, especially in patients with mood or anxiety disorders. The prescribed amount ranges from 0.25 to 0.5 mg daily divided in 2-3 doses, the duration depends upon the patients age and other factors of causes as assessed by the clinicians.
However, given the effectiveness of benzodiazepines, some people especially the younger population tend to continue to take the drugs for longer duration than recommended for 2-4 weeks. This is leading to Benzodiazepines overdose in recent years, Benzodiazepines are relatively safe medications, acute overdose is rare except taken with suicidal intention, but isolated chronic benzodiazepine overdose is not uncommon. Young people who take benzodiazepines for an extended period are at risk of developing numerous adverse conditions, including tolerance, dependence, and withdrawal upon discontinuation. The classic presentation of an isolated benzodiazepine chronic overdose consists of CNS depression with normal vital signs. This elevated risk of drug overdose with benzodiazepine compared to alternative pharmacologic treatments for sleep disorders is an important safety consideration when treating young people [15]
If benzodiazepines are taken for more than 2 weeks, it is recommended that the user should gradually taper over an extended period. If stopped abruptly, symptoms of benzodiazepine withdrawal can occur, which include headache, sleep disturbances, irritability, agitation, convulsions, tremors, nausea and vomiting and psychosocial episodes like severe panic attacks, psychosis, hallucinations, and seizures. The latest guidelines for minimizing withdrawal symptoms suggest [16]:
• For chronic users: An initial reduction of 25-30% for high dosage, followed by a 5-10
Conclusion
This article is an effort to infuse right practices of managing Insomnia by general practitioners and alert when to refer cases to sleep specialists. It also describes the role of common people in tackling Insomnia and when to approach a physician or a sleep specialist.
References
- Sleep Statistics, Updated December 15, 2022. https://www.sleepfoundation.org/.
View at Publisher | View at Google Scholar - Sleep Statistics, Updated December 15, 2022. https://www.sleepfoundation.org/.
View at Publisher | View at Google Scholar - More Evidence Insomnia Contributes to Cognitive Decline, Megan Brooks, November 22, 2022, https://www.medscape.com/viewarticle
View at Publisher | View at Google Scholar - Guidelines of the Indian Society for Sleep Research (ISSR) for Practice of Sleep Medicine during COVID-19, Ravi Gupta, et.al, Sleep Vigil. 2020; 4(2): 61–72.
View at Publisher | View at Google Scholar - What Colour Noise Will Help You Sleep Better at Night? April 5, 2022, by Ann Ferguson, https://www.actionmaytag.com/blog/what-color-noise-improves-sleep
View at Publisher | View at Google Scholar - Prevalence of chronic insomnia in adult patients and its correlation with medical comorbidities, Swapna Bhaskar et.al, J Family Med Prim Care. 2016 Oct-Dec; 5(4): 780–784.
View at Publisher | View at Google Scholar - Sleep-related disorders among a healthy population in South India, Samhita Panda et.al, Neurol India [serial online] 2012 [cited 2023 Feb 20];60:68-74.
View at Publisher | View at Google Scholar - Insomnia: Case Studies in Family Practice, Kamil Mohd Ariff et.al, https://www.ncbi.nlm.nih. gov/ PMC4797034
View at Publisher | View at Google Scholar - More Evidence Insomnia Contributes to Cognitive Decline, Megan Brooks, November 22, 2022,
View at Publisher | View at Google Scholar - Is Apnoea-Hypopnea Index a proper measure for Obstructive Sleep Apnoea severity? Ali Mohamad Asghari et.al,
View at Publisher | View at Google Scholar - Jury Still Out on Obstructive Sleep Apnoea Screening, Megan Brooks, November 17, 2022
View at Publisher | View at Google Scholar - Treatments for Insomnia, Austin Meadows, Sleep Product Tester, Medically Reviewed by Alex Dimitriu, Psychiatrist. Available at: https://www.sleepfoundation.org 6 Jan 2023.
View at Publisher | View at Google Scholar - Bushnell GA, et al. Association of benzodiazepine treatment for sleep disorders with drug overdose risk among young people. JAMA Netw Open. 2022;5(11): e2243215.
View at Publisher | View at Google Scholar - Chaudhury S, et al. Chronic insomnia: A review. Med J DY Patil Vidyapeeth 2019; 12:193-201.
View at Publisher | View at Google Scholar - de Zambotti M, et al. Insomnia disorder in adolescence: diagnosis, impact, and treatment. Sleep Med Rev. 2018; 39:12-24,
View at Publisher | View at Google Scholar - Management of overdose of benzodiazepines among young people, guest editorial, Suresh Kishanrao, https://www.emedinexus.com/post/35549/01 February 2023
View at Publisher | View at Google Scholar - How to taper off benzodiazepines, Michael Kaliszewski. https://americanaddictioncenters.org, 19/07/22.
View at Publisher | View at Google Scholar
