

Letter to Editor | DOI: https://doi.org/10.31579/2834-796X/061
Electrocardiographic Criteria for Diagnosis of Acute Myocardial Infarction in Patients with Left Bundle Branch Block
*Corresponding Author: Mohammed Habib, Head of Cardiology Department, Alshifa Hospital, Gaza, Palestine.
Citation: Mohammed Habib, (2024), Electrocardiographic Criteria for Diagnosis of Acute Myocardial Infarction in Patients with Left Bundle Branch Block, International Journal of Cardiovascular Medicine, 3(3); DOI:10.31579/2834-796X/061
Copyright: © 2024, Mohammed Habib. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 10 April 2024 | Accepted: 17 April 2024 | Published: 02 May 2024
Keywords: amı; lbbb; ecg
Abstract
In patients with normal heart and normal conduction system, the initial depolarized segment in ventricle is interventricular septum which begins with septal fascicle of the left bundle branch from left side and direction to right side followed by a simultaneous depolarization of the remaining ventricular free walls from endocardium to pericardium via the right and left bundle branches. But among patients with left bundle branch block (LBBB), the initial septal activation is changing direction and become from right to left then the left ventricular activation is delayed, ST segment and T wave abnormalities occur, and septal Q waves indicative of an MI are absent in this condition. About 0.5 percent of patients with acute myocardial infarction had left bundle-branch block.
Because this changes the patients with left bundle branch block (LBBB) and acute myocardial infarction (MI) is challenge to the clinician. The diagnosis of MI with electrocardiogram (ECG) is so difficult in the setting of LBBB because of the characteristic ECG changes caused by altered interventricular septal and left ventricle free wall depolarization. Here we review the ECG diagnostic criteria included all criteria until now and short summary of patient with acute MI and LBBB condition.
Diagnostic criteria
The Sgarbossa criteria (1)
The Sgarbossa criteria is the most oldest criteria for the diagnosis of MI in the presence of LBBB. The Sgarbossa criteria were first introduced in 1996 to improve the diagnostic accuracy for acute MI in the presence of LBBB. The confirm diagnosis of MI must be need at least 3 or more points from the following criteria. Figure 1
- ST-elevation of ≥1 mm and concordant with the QRS complex (5 points)
- ST-segment depression ≥1 mm in lead V1-3 (3 points)
- ST elevation ≥5 mm and discordant with the QRS complex (2 points)
The specificity of 98%, but poorer sensitivity of 20%. The third criteria have only 2 point so that no add any significant value as it alone does not confirm diagnosis of acute myocardial infarction.
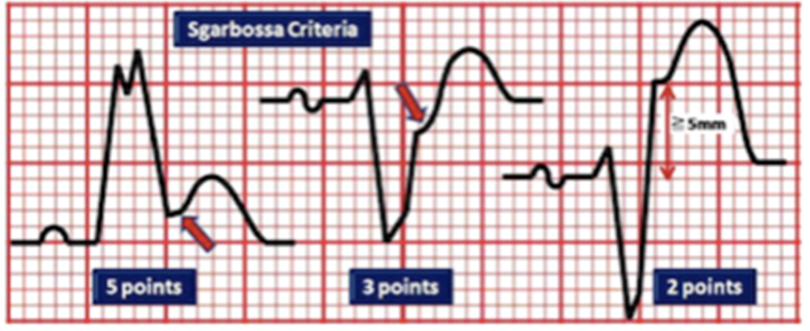
Figure 1: Sgarbossa criteria for myocardial infarction
Modified Sgarbossa ( Smith-Sgarbossa) Criteria (2)
Because of the third criteria of Sagarbossa have only 2 point and does not confirm diagnosis of acute myocardial infarction. The modified Sgarbossa
criteria was used to modified and support the third criteria by calculation the ratio of ST segment elevation to the depth S wave. The discordant ST/S ratio ≥ 0.25 mm in any lead suggested acute MI. Figure 2
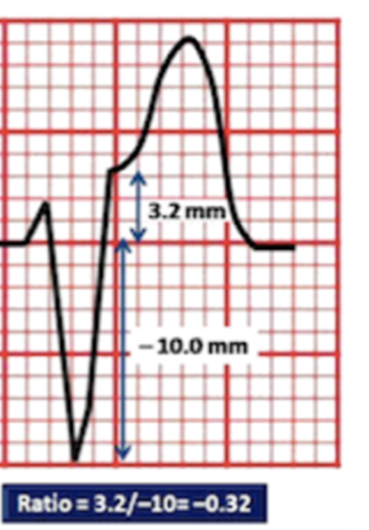
Figure 2: Modified Sgarbossa Criteria for myocardial infarction
The Barcelona Criteria (3)
Barcelona Criteria contains of 3 criteria, As with the prior Sgarbossa criteria , criteria 1 is the same. Criteria 2 is expanded to all leads (but in Sgarbossa just in V1-3). Criteria 3 is specific for the Barcelona criteria and suggested that discordance deviation of ≥ 1mm in any lead with a dominant R or S wave ≤ 6 mm.
- ST deviation ≥1 mm concordant with QRS complex in any lead;
- Concordant with QRS complex and ST depression ≥1 mm
- Concordant with QRS complex and ST elevation ≥1 mm
- Discordant ST deviation ≥ 1mm with QRS complex in any lead where the R or S is ≤ 6 mm.
For example, in aVR lead, with an S wave of 5 mm, with discordant elevation of 1mm this would meet criteria. Figure 3
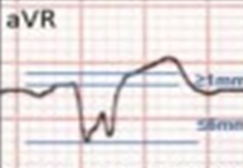
Figure 3: aVR lead ST elevation ≥1 mm discordant with QRS complex, and (S) wave voltage ≤ 6 mm.
Summary of electrocardiographic criteria;
This is simple 6 steps for diagnosis patient with LBBB and suspected acute MI. Figure 4
- Confirm diagnosis of LBBB. If yes go to 2nd step
- Calculate ST segment deviation ≥ 1 mm in any lead If yes go to 3nd step
- Concordant or Discordant with QRS complex?
- If concordant and ≥ 1 mm ST segment deviation in any lead; Acute MI
- If discordant in any lead with R or S is ≤ 6 mm; Acute MI
- If discordant in any lead with R or S is ≥ 6 mm; calculate the ratio of ST segment elevation to the depth S wave. If ≥ 25%; Acute MI
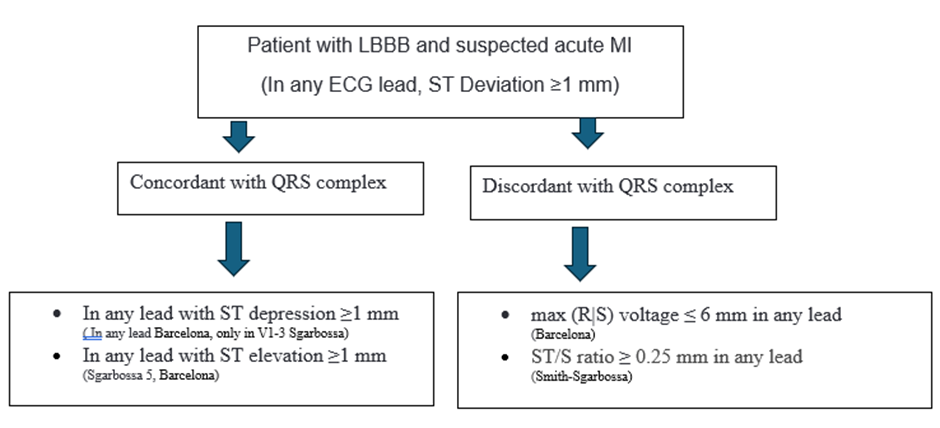
Figure 4: Summary of electrocardiographic criteria; ECG; Electrocardiogram, MI; myocardial infraction
References
- Sgarbossa EB, Pinski SL, Barbagelata A, et al. Electrocardiographic diagnosis of evolving acute myocardial infarction in the presence of left bundle-branch block. GUSTO-1 (Global Utilization of Streptokinase and Tissue Plasminogen Activator for Occluded Coronary Arteries) Investigators. N Engl J Med 1996;334:481-7.
View at Publisher | View at Google Scholar - Smith SW, Dodd KW, Henry TD, Dvorak DM, Pearce LA. Diagnosis of ST-elevation myocardial infarction in the presence of left bundle branch block with the ST-elevation to S-wave ratio in a modified Sgarbossa rule. Ann Emerg Med 2012;60:766-76
View at Publisher | View at Google Scholar - Andrea Di Marco,Marcos Rodriguez,Juan Cinca et al. New Electrocardiographic Algorithm for the Diagnosis of Acute Myocardial Infarction in Patients With Left Bundle Branch Block. J Am Heart Assoc. 2020;9:e015573.
View at Publisher | View at Google Scholar
