

Research Article | DOI: https://doi.org/10.31579/ 2834-8788/003
Effect Of Preexrcise Increase in Heart Rate on Subsequent Increase in Heart Rate During Different Stages and Maximal Heart Rate During Treadmill Testing in Normal Persons
- S.R. Mittal, D.M.
- Govind Mittal *
Department of Cardiology, Mittal Hospital & Research Centre, Pushkar Road, Ajmer (Raj.) -305001
*Corresponding Author: Govind Mittal. Department of Cardiology, Mittal Hospital & Research Centre, Pushkar Road, Ajmer (Raj.) -305001
Citation: S.R. Mittal, D.M., Mittal G. (2022). Effect Of Preexrcise Increase in Heart Rate on Subsequent Increase in Heart Rate During Different Stages and Maximal Heart Rate During Treadmill Testing in Normal Persons. Journal of Heart and Vasculature.1(2); DOI:10.31579/ 2834-8788/003
Copyright: © 2022 Govind Mittal, This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 31 October 2022 | Accepted: 09 November 2022 | Published: 16 November 2022
Keywords: bruce protocol; coronary artery disease; heart rate; hyperventilation; exercise electrocardiography; prognosis; treadmill testing
Abstract
There is no study on the effect of preexercise(standing from supine position and subsequent hyperventilation) increase in heart rate on increase in heart rate during various stages of stress and maximal heart rate during treadmill testing in normal persons. We evaluated sixty three normal individuals after strictly excluding various confounding factors. There was significant interindividual variability in preexercise increase in heart rate. Individuals who had an increase of more than forty beats per minute during preexercise period had less increase/no increase or even decrease in heart rate during the first stage of Bruce protocol. It was due to cancellation of exercise induced increase in heart rate by settling down of preexercise increase in heart rate. Subsequent increase in heart rate during the second stage and the third stage was normal. Maximal heart rate attained by all individuals was also normal. Inadequate increase in heart rate during the first stage of Bruce protocol should be interpreted in the context of increase in heart rate during the preexercise period .
Introduction
Prior to exercise on treadmill, electrocardiograms are recorded in standing position and after hyperventilation to exclude wrong interpretation of electrocardiographic changes seen during exercise. Standing from supine position as well as active hyperventilation increase heart rate [1,2] We observed significant interindividual variation in increase in heart rate from supine position to pre-exercise stage. (including standing and active hyperventilation) Effect of pre-exercise increase in heart rate on subsequent increase in heart rate during various stages of exercise and on maximal heart rate is not known. This is important because magnitude of increase in heart rate at different levels of exercise has been correlated with cardiovascular or overall mortality. Savonen et al [3] observed that blunted heart rate increase between 40 to 100% of maximal work load was associated with increased cardiovascular mortality. Leeper et al4 observed that heart rate at one third of the total exercise capacity significantly predicted both all cause and cardiovascular risk. Other workers have observed that inability to increase heart rate commensurate with increase in work load is associated with increased overall or cardiovascular mortality [5,6,7] However, none of the previous studies have considered pre-exercise increase in heart rate and it’s impact on increase in heart rate during different stages of stress and on maximal heart rate. We, therefore, studied the effect of pre-exercise increase in heart rate on subsequent increase in heart rate during different stages of exercise and on percentage of age predicted maximal heart rate attained at peak exercise in normal individuals.
Materials and Methods
(a) Inclusion criteria
(i) Absence of any cardiovascular symptoms.
(ii) Normal clinical examination.
(iii) Normal resting twelve lead electrocardiogram.
(iv) Normal 2-dimensional and colour Doppler echocardiographic examination.
(v) No new electrocardiographic changes on standing and during active hyperventilation prior to exercise.
(vi) No clinical or electrocardiographic evidence of myocardial ischemia during exercise or recovery.
(b) Exclusion criteria
(i) Patients with contraindication for exercise stress testing.8
(ii) Conditions that could hamper exercise capacity e.g. debility, orthopaedic problems, haemoglobin concentration less than 10gm % 9, left or right ventricular dysfunction 10 chronic pulmonary disease, systemic or pulmonary hypertension.
(iii) Conditions that could affect the heart rate response to exercise e.g.autonomic neuropathy, paced ventricular rhythm, use of beta-blockers, diltiazem or veropamil.
(iv) Unexplained resting heart rate less than 60 beats per minutes. Such individuals could have sinus node dysfunction or inherently increased parasympathetic activity that could affect the heart rate response to exercise.
(v) Conditions that could affect correct interpretation of exercise electrocardiogram [11] e.g. intraventricular conduction defects, ST-segment or T wave changes in the resting electrocardiogram, presence of the preexcitation in the resting electrocardiogram, electrocardiographic evidence of left and/or right ventricular hypertrophy.
(vi) Development of any bradyarrhythmia, tachyarrhythmia or frequent premature beats during treadmill test.
(vii) When any possibility of myocardial ischemia could not be excluded with confidence e.g. development of horizontal ST-segment depression of less than 1 mm, upsloping ST-segment depression, ST-segment depression localized to inferior leads with significantly downsloping P-Q segment, new appearance of isolated shallow inversion of T waves inversion, increasing frequency of ventricular premature beats during exercise or new appearance of ventricular premature beats during recovery.
(c) Exercise test protocol
(i) Mason-Likar lead system [12] was used. All twelve leads were recorded simultaneously.
(ii) Bruce protocol [13] was followed.
(iii) Exhaution rather than age adjusted target heart rate was taken as the endpoint to achieve maximal heart rate and exclude any possibility of myocardial ischemia [14].
(iv) Exercise was terminated if there was development of angina, any magnitude of ST-segment elevation, ST-segment depression of 1mm, any bundle branch block, increasing frequency of premature ventricular contractions or inability to exercise from any cause [15]
(v) Ten seconds of post-exercise cool-down walk was practiced to avoid post exertional dizziness or syncope doe to sudden reduction in venous return or a vogal response due to sudden slopping of exercise [16]
(vi) Recovery was usually recorded for six minutes. It was extended if indicated. Sixty three individuals (46 males and 17 females) qualified for final analysis. Age ranged from 20 to 73 years (44.2+8.09 years)
(d) Evaluation of heart rate
Computer derived heart rate was used for analysis. Heart rate was calculated manually if it was felt that there was some error in computer evaluation of heart rate. Age predicted maximal heart rate was calculated by formula of Fox et al (220-age) [17]
(e) Statistical analysis
Individuals were divided into three groups.
Group A- Pre-exercise increase in heart rate less than 30 beats per minute. Group B- Pre-exercise increase in heart rate between 20 to 40 beats per minute. Group C- Pre-exercise increase in heart rate more than 40 beats per minute.Difference between different groups was evaluated using unpaired ‘t’ test [18]
Results
Group A included 21 males and six females. Group B included 14 males and 11 females. Group C had 11 males. Individuals of group C were significantly younger (P less than 0.05) than individuals of group A and B (Table-1). The three groups were comparable (Pgreater than 0.10) regarding resting supine heart rate, resting supine systolic blood pressure and resting supine diastolic blood pressure (Table-1).
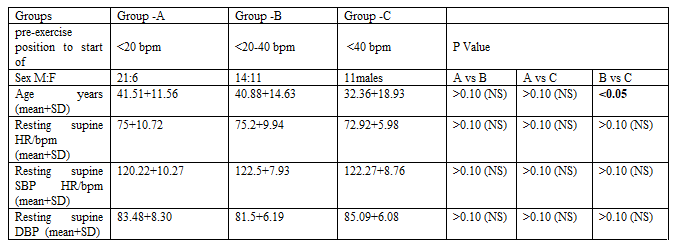
Abbreviation - bpm- beats per minute, HR- heart rate, F- female, M- Male, NS- not significant, SBP- systolic blood pressure, DBP- diastolic blood pressure.
Mean values of pre-exercise increase in heart rate increased significantly from group A to group B (P less than 0.001) and further from group B to group C (P less than 0.001) (Table-2). Increase in heart rate during the first stage of exercise showed a reciprocal change. There was no significant difference in increase in heart rate between Group A & B. However, increase in heart rate in group C was significantly lower (P less than 0.001). There was no significant difference in increase in heart rate between different groups during third stage (Pgreater than 0.10). During stage four, increase in heart rate was lower in group A(P= 0.05) than in group B and C. By the end of exercise, all individuals attained age predicted maximal heart rate. There was no significant difference in the percentage of age predicted maximal heart rate attained by different groups.
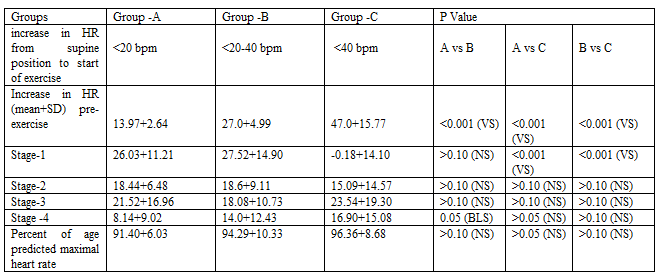
Abbreviation: VS - very significant, NS- Not significant, BLS- Borderline significant.
Discussion
On standing, there is gravity -mediated pooling of about 300 to 800 ml of blood in lower extremities and inferior mesenteric area. This results is decrease in venous return and resltant decrease in stroke volume. There is transient fall in blood pressure which results in reflex increase in sympathetic activity that causes peripheral vasoconstriction and increase in heart rate.19 Normally heart rate increases by 10 to 15 beats per minute [20]. Usually the change in heart rate and blood pressure normalize in one minute [20] However, the whole process is complex and involves several afferent and efferent neuronal pathways and nuclei in tractus solitarius and other areas of medulla. Inability of this complex process to respond adequately can result in greater increase in heart rate and persistence of this increase over a longer period. This results in significant interindividual variation in heart rate response to standing from supine position. Anxiety, inappropriate sinus tachycardia and postural orthostatic tachycardia syndrome 21 also contribute to significant interindividual variability.
Active hyperventilation also result in increase in heart rate [2,22] Release of excitatory neurotransmitters from the brain are probably responsible. Lowered arterial carbon dioxide concentration also results in splanchnic vasodilation via inhibition of vasomotor centre. Resulting drop in venous return results in reduced ventricular filling, decreased stroke volume and reflex increase in heart rate. Increase in heart rate depends on rate, depth and duration of hyperventilation. This contributes to interindividual variation in heart rate response to hyperventilation.
Active hyperventilation soon after standing from supine position results in additive effect on increase in heart rate. This increase in heart rate due to standing and subsequent active hyperventilation gradually settles down to the basal heart rate of the individual. This period extends over the first stage of treadmill test. Magnitude of settling down of the heart rate is proportional to the magnitude of increase during standing and hyperventilation because the heart rate tends to revert back to it’s basal state. As the exercise progresses during stage one, cardiac out put increases to maintain adequate blood supply to the exercising muscles. This occurs due to neural inputs from mechanoreceptors and chemoreceptors within the active skeletal muscles.24 Initially the stroke volume increases but it quickly plateaus and the heart rate rises to maintain progressive increase in cardiac output.25 Heart rate at the end of first stage of treadmill testing is, therefore, a sum total of decline in heart rate that increased due to standing and hyperventilation on one side and increase in heart rate due to exercise on the other side. This explains our observation that the group which had maximal increase in heart rate during pre-exercise period (group C ) had the lowest heart rates at the end of first stage of treadmill testing.
It is believed that a lower heart rate under a standard exercise load suggests better conditioning [26] Our observations show that abnormal increase in heart rate during pre-exercise period can be another cause for less than expected increase in heart rate during the first stage of treadmill testing using Bruce protocol. Leeper et al 4 felt that heart rate rise at one third of the total exercise capacity significantly predicted both all cause and cardiovascular risk. They however did not consider pre-exercise increase in heart rate. Our observations show that less than expected increase in the heart rate by the end of the first stage of treadmill test using Bruce protocol can occur in normal persons show have increase of more than 40 beats per minute in pre-exercise period.
We observed that increase in heart rate during the second and the third stage was similar in all the three groups. This shows that the effect of increased heart rate during the pre-exercise period does not extend beyond the first stage of Bruce protocol,
During fourth stage increase in heart rate was significantly less in group A and was maximum in group C, This had no relation to change in heart rate during the pre-exercise period. It was probably related to the age and gender composition of individuals in the different groups. Persons of group C were significantly younger than individuals in groups A and B. Further, group C had only males. During exercise initial increase in heart rate is due to withdrawal of parasympathetic tone [27] Subsequent increase in heart rate is due to increased sympathetic activity [27] Responsiveness of the sino-atrial node to sympathetic stimulation declines with advancing age due to apoptosis of the sinoatrial node 28 and less calcium influx in the sinoatrial node [29] Aerobic work capacity also declines with advancing age 30,31 due to age related changes in skeletal and cardiac muscles [32,33] All these factors lead to gradual decrease in maximal heart rate with advancing age. Males have greater acrobic capacity and, therefore, can take greater work load and attain greater heart rate [9,34,35].
There was no significant difference in percentage of age predicted maximal heart rate in different groups. This shows that pre-exercise increase in heart rate had no effect on maximal heart rate attained by an individual. Pre-exercise increase in heart rate was compensated by less increase in heart rate during the first stage. Subsequently the increase in heart rate was similar in second and third stage.
Conclusion
Standing from supine position and subsequent active hyperventilation increase heart rate prior to start of exercise. Magnitude of this pre-exercise increase in heart rate shows significant interindividual variation. Significant increase in heart rate during pre-exercise period (more than 40 beats per minute) is compensated by less increase/no increase or even decrease in heart rate during the first stage of Bruce protocol. Subsequently in the second and the third stage, increase in heart rate is normal with the result that percentage of age predicted maximal heart rate is normal irrespective of pre-exercise increase in heart rate. Increase in heart rate during the first stage of Bruce protocol should be interpreted in context of the pre-exercise increase in heart rate.
References
- Huang MH, Epey J, Wolf S. (1991). Heart rate - QT interval relationship during postural change and exercise. A possible connection to cardiac contractility. Integi Physiol Behav Sci. 26:5-17.
View at Publisher | View at Google Scholar - Enger GL, Ferris EP, Logan M. (1947). Hyperventilation: Analysis of clinical symptomatology. Anals of Internal Medicine. 27:683-704.
View at Publisher | View at Google Scholar - Savonen KP, Lakka TA, Laukkanen JA, et al. (2006). Heart rate response during exercise test and cardiovascular mortality in middle aged men. Eur Heart J. 27: 582-588.
View at Publisher | View at Google Scholar - Leeper NJ, Dewoy FE, Ashley EA, et al. (2007). Prognostic value of heart rate increae at onset of exercise testing. Circulation. 115: 468-474.
View at Publisher | View at Google Scholar - Lauer MS, Okin PM, Larson MG, et al. (1996). Impaired heart rate response to graded exercise - Prognostic implications of chronotropic incompetence in the Framingham heart study. Circulation. 93:1520-1526.
View at Publisher | View at Google Scholar - Lauer MS, Francis JS, Okin PM, et al. (1999). Impaired chronotropic response to exercise testing as a predictor of mortality. JAMA. 281:524-529.
View at Publisher | View at Google Scholar - Khan MN, Pathier CE, Lauer MS. (2005). Chronotropic incompetence as a predictor of death among patients with normal electrogram taking beta blocker (metoprolal or atenolal). Am J Cardiol. 96:1328-1333.
View at Publisher | View at Google Scholar - Thmos GS, Ellestad MH. (2018). Contraindications and safety for stress testing. In: Thomas GS, Wann LS, Ellestad MH (eds), Ellestad’s Stres Testing. Oxford, 71-81.
View at Publisher | View at Google Scholar - Sharma HB, Kailashiya J. (2016). Gender difference in aerobic capacity and the contribution of body composition and haemoglobin concentration: a study in young Indian national hocky players. J Clin Diagn Res. 10:cc09-cc13.
View at Publisher | View at Google Scholar - Chin CF, Messenger JC, Greenberg PS, Ellestad MH. (1979). Chronotropic incompetence in exercise testing. Clin Cardiol. 2:12-18.
View at Publisher | View at Google Scholar - Gibbons RJ, Balady GJ, Bricker JT, et al. (2002). ACC/AHA 2002 guideline update for exercise testing: A report of the American College of Cardiology/ American Heart Association Task Force on practice guideline committee on exercise testing. J Am Coll Cardiol. 40:1531-1540.
View at Publisher | View at Google Scholar - Mason RE, Likar I. (1966). A new system of multiple lead exercise electrocardiography. Am Heart J. 71:196-205.
View at Publisher | View at Google Scholar - Bruce R, Blackman J, Jones J, Strait J. (1963). Exercise testing in adult normal subjects and cardiac patients. Pediatrics. 32:742-756.
View at Publisher | View at Google Scholar - Jain M, Nikonde C, Lin BA, Walker A, Wackers FJ. (2011). 85% of maximal age predicted heart rate is not a valid end point for exercise treadmill testing. J Nucl Cardiol. 18:1026-1035.
View at Publisher | View at Google Scholar - Fletcher GF, Ades PA, Kligficld P, et al. (2013). Exercise standards for testing and training: a scientific statement from the American Heart Association. Circulation. 128:878-934.
View at Publisher | View at Google Scholar - Thomas GS, Ellestad MH. (2017). Electrocardiographic exercise testing. In: Fuster VF, Harrington RA, Narula J, Eapen ZJ (eds). Hurst’s The Heart. Mc Graw Hill Education, 318-334.
View at Publisher | View at Google Scholar - Fox S III, Naughton JP, Haskell WL. (1971). Physical activity and the prevention of coronary heart disease. Ann Clin Res. 3:404-432.
View at Publisher | View at Google Scholar - Student ‘T’ test - an overview. https ://www.science direct.co
View at Publisher | View at Google Scholar - Calkins H, Zipes DP. (2019). Hypotension and syncope. In: Zipes DP, Libby P, Bonow RO, Mann DL, Tomaselli GF. (eds). Braunwald’s Heart Disease. 848-858.
View at Publisher | View at Google Scholar - Grubb BP. (2013). Diagnosis and management of syncope. In: Fuster V, Harrington RA, Narula J, Eapen ZJ. (eds). Hurst’s The Heart. Mc Graw Hill. New York; 2098-2112.
View at Publisher | View at Google Scholar - Tomaselli GF, Zipes DP. (2019). Approach to the patient with cardiac arrhythmias. In: Zipes DP, Libby P, Bonow RO, Mann DL, Tomaselli GF (eds). Braunwald’s Heart Disease. Elsevier, Philadelphia: 597-603.
View at Publisher | View at Google Scholar - Kein B. (2021). Hyperventilation syndrome. Med scape.
View at Publisher | View at Google Scholar - Lewis BI. (1953). The hyperventilation syndrome. Annals of internal medicine. 43:918-927.
View at Publisher | View at Google Scholar - Sylvies FR, Ellestad MH. (2008). Cardiovascular and pulmonary responses to exercise. In: Thomas GS, Wann LS, Ellestad MH (eds). Ellestad’s Stress Testing. Oxford, UK; 373-412.
View at Publisher | View at Google Scholar - Kao A. (2018). Cardiopulmonary exercise testing. In: Thomas GS, Wann LS, Ellestad MH (eds). Ellestad’s Stress Testing. Oxford, UK; 413-436.
View at Publisher | View at Google Scholar - Thomas GS, Ellestad MH. (2018). Parameters to be measured during exercise. In: Thomas GS, Wann LS, Ellestad MH (eds). Ellestad’s Strss Testing. Oxford, UK; 82-105.
View at Publisher | View at Google Scholar - Lipinski MJ, Froelicher VF. (2011). ECG exercise testing. In: Fuster V, Walsh RA, Harrington RA (eds). Hurst’s The Heart. Mc Graw Hill, New York; 371-387,
View at Publisher | View at Google Scholar - Cheitlin MD. (2003). Cardiovascular physiology - changes with aging. Am J Geriatr Cardiol. 12:9-13.
View at Publisher | View at Google Scholar - Gellish RL, Goslin BR, Olson RE, et al. (2007). Longitudinal modelling of the relationship between age and maximal heart rate. Med Sci Exer. 39: 822-829.
View at Publisher | View at Google Scholar - Higginbotham MB, Morris KG, Williams RS. (1986). Physiologic basis for the age- related decline in aerobic work capacity. Am J Cardiol. 57: 1374-1379.
View at Publisher | View at Google Scholar - Fleg JL, Morrell CH, Bos AG, et al. (2005). Accelerated longitudinal decline of aerobic capacity in healthy older adults. Circulation. 112: 674-682.
View at Publisher | View at Google Scholar - Laurctani F, Russo CR, Bandinelli S, et al. (2003). Age associated changes in skeletal muscles and their effect on mobility: an operational diagnosis of sarcopenia. J Appl Physiol. 95: 1851-1860.
View at Publisher | View at Google Scholar - Olivetti G, Melissari M, Capasso JM, Anversa P. (1991). Cardiomyopathy of the aging human heart. Myocyte loss and reactive cellular hypertrophy. Circ Res. 68:1560-1568.
View at Publisher | View at Google Scholar - Cureton K, Bishop P, Hutchinson P, et al. (1986). Sex difference in maximal oxygen uptake. Effect of equating haemoglobin concentration. Eur J Appl Physiol. 54: 656-660.
View at Publisher | View at Google Scholar - Whaley MH, Kaminsky LA, Dwyer GB, et al. (1992). Prediction of over and under achievement of age predicted maximal heart rate. Med Sci Sprots Exer. 10: 1173-1179.
View at Publisher | View at Google Scholar
