

Case Presentation | DOI: https://doi.org/10.31579/2835-785X/080
Dual Left Anterior Descending Coronary Artery (Type IV): An Unusual Coronary Artery Anomaly
- Amit Mandal *
- Oommen K George
Department of Cardiology, Christian Medical College, Vellore, Tamil Nādu, India.
*Corresponding Author: Amit Mandal, Department of Cardiology, Christian Medical College, Vellore, Tamil Nādu, India.
Citation: Amit Mandal, (2025), Dual Left Anterior Descending Coronary Artery (Type IV): An Unusual Coronary Artery Anomaly, International Journal of Clinical Research and Reports. 4(1); DOI:10.31579/2835-785X/080
Copyright: © 2025, Amit Mandal. This is an open-access artic le distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 22 January 2025 | Accepted: 03 February 2025 | Published: 18 February 2025
Keywords: coronary artery (type iv); coronary artery anomaly; LAD; AIVS; CAD; PTCA
Abstract
Congenital coronary anomalies are rare and reported to occur in 0.64 – 1.3% of patients undergoing coronary angiography. Generally, the left anterior descending artery (LAD) follows a predictable course and its congenital abnormalities are less frequent compared to the other coronary arteries.
Introduction
Congenital coronary anomalies are rare and reported to occur in 0.64 – 1.3% of patients undergoing coronary angiography [1]. Generally, the left anterior descending artery (LAD) follows a predictable course and its congenital abnormalities are less frequent compared to the other coronary arteries [2]. Dual LAD is defined as the presence of two LADs in the anterior interventricular sulcus (AIVS). It consists of a short LAD that ends high in the AIVS and a longer LAD that enters the distal AIVS and feeds apex. Type IV dual LAD, in which a short LAD arises from the left main coronary artery and a long LAD arises from the right coronary artery is remarkably rare. Dual LAD is a benign coronary anomaly but should be recognized especially before interventional procedure and all cardiologists must be aware of variants of dual LAD. Herein, we report a rare case of type IV dual LAD with the literature review.
Case Presentation
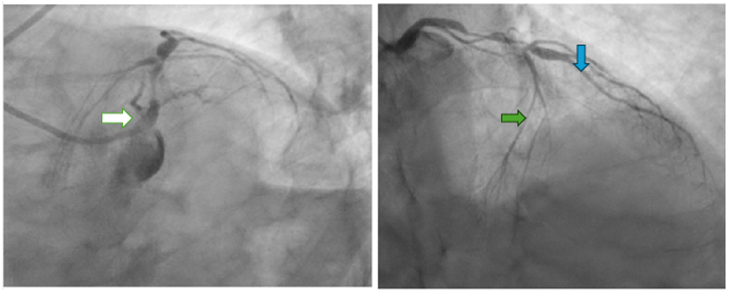
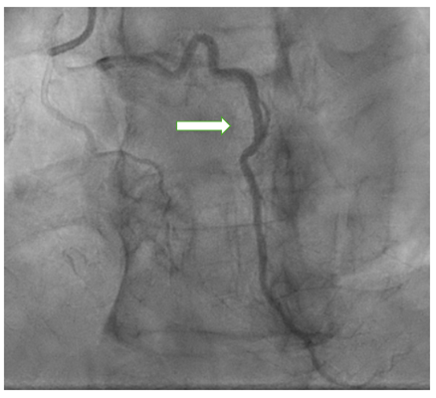
This 63-year-old gentleman presented with effort angina for six months duration. Six months back he underwent PTCA to RCA elsewhere when he was admitted with inferior wall myocardial infarction. He was a long-standing diabetic and chronic smoker with no other risk factors for coronary artery disease (CAD) including no family history of CAD. Because of persistent effort angina, patient was taken for coronary angiography. The left coronary angiogram (LCA) showed the LAD coronary artery arising from the left main coronary artery. This LAD was short and terminated prematurely in the AIVS, creating the suspicion of complete occlusion of the mid-LAD artery. This short LAD gave rise to the first diagonal branch and septal branches. (Fig 1a,1b) Selective right coronary (RCA) angiography showed proximal long segment calcific disease with maximum severity of 90% with Mehran type III ISR of the proximal stent, mid tubular calcific 50-60% stenosis, distal normal vessel and another vessel arising from right coronary artery. This long vessel travelled to the left side and then re-entered the distal AIVS to reach the apex suggestive of it being the (long) LAD (Fig. 2). This was consistent with the type IV variety of dual LAD as per the Spindola-Franco classification, a rare entity. He underwent PTCA to RCA with calcium modification - Intravascular lithotripsy and PTCA to LM-LAD.
Discussion
Congenital coronary anomalies are rare and reported to occur in 0.64 – 1.3% of patients undergoing coronary angiography.[1] The LAD normally arises from the left main coronary artery, courses in the anterior interventricular groove, and extends toward the cardiac apex. It gives rise to diagonal branches and septal perforators. Dual left anterior descending (LAD) artery is a rarely reported coronary anomaly, consisting of two branches supplying the usual distribution of the LAD. Prevalence of dual LAD is 1% in patients of all coronary anomalies [3]. Dual LAD may be associated with Congenital heart disease like tetralogy of Fallot and transposition of great arteries, where it of surgical importance [4]. The dual LAD coronary anomaly, consists of two branches short and long supplying the usual distribution of the LAD. While the short-LAD terminates in the proximal aspect of the anterior interventricular sulcus (AIVS), the long LAD has a variable course outside the AIVS and returns to the inside distally.
Based on the origin, course, and termination of the short and long LAD, dual LAD has been classified into 4 angiographic subtypes by Spindola-Franco et al., [5].
- Type I: The short LAD runs in the AIVS and is generally the source of all major proximal septal perforators. The long LAD also runs in the AIVS, descending on the left ventricular side of the AIVS, re-entering the distal AIVS to reach the apex.
- Type II: The short LAD is the same as in type 1, but the long LAD descends over the right ventricular side before re-entering the AIVS.
- Type III: The short LAD is consistent with that in types 1 and 2. The long LAD travels intramyocardially in the ventricular septum.
- Type IV: The short LAD originates from the LMCA. The major septal perforators and the diagonal branches originate from this vessel. The long LAD arises from the RCA. It is extremely rare among the four types.
Identification of the presence of a double left anterior descending artery is important both for diagnostic and therapeutic reasons [6–8].
Whenever a short or hypoplastic LAD is encountered, differential diagnosis of a long-dominant posterior descending branch of the RCA, terminating in the AIVS beyond the apex; a long parallel diagonal branch; or a dual LAD should be considered. Short LAD should not be misdiagnosed as total occlusion, and a long LAD should not be misdiagnosed as a conus branch. If a paucity of distribution of vessels in the apical LAD territory with a small LAD proper during coronary angiography is found, the cardiologist should keep in mind about possibility of dual LAD.
We describe a case with unique variation of dual LAD type IV, which shows a separate origin of a short LAD arising from LMCA up to first septal and diagonal branch, and long LAD originating from right coronary sinus and reaching to the apex.
Conclusion
In conclusion, we report a type IV dual LAD coronary artery, which is a rare coronary anomaly. It is important for cardiologists to be aware of this variant of dual LAD anomaly while interpreting the coronary angiogram which will help them to make the right decision regarding management.
References
- Yamanaka O, Hobbs RE. Coronary artery anomalies in 126,595 patients undergoing coronary arteriography. Cathet Cardiovasc Diagn. 1990; 21(1):28–40.
View at Publisher | View at Google Scholar - Tuncer C, Batyraliev T, Yilmaz R, Gokce M, Eryonucu B, Koroglu S. Origin and distribution anomalies of the left anterior descending artery in 70,850 adult patients: multicenter data collection. Catheter Cardiovasc Interv Off J Soc Card Angiogr Interv. 2006 Oct; 68(4):574–585.
View at Publisher | View at Google Scholar - Nasrin S, Cader FA, Haq MM, Shafi MJ. Type IV dual left anterior descending coronary artery: a case report. BMC Res Notes. 2017 Dec 1; 10(1):659.
View at Publisher | View at Google Scholar - Sajja LR, Farooqi A, Shaik MS, Yarlagadda RB, Baruah DK, Pothineni RB. Dual left anterior descending coronary artery: surgical revascularization in 4 patients. Tex Heart Inst J. 2000; 27(3):292–306.
View at Publisher | View at Google Scholar - Spindola-Franco H, Grose R, Solomon N. Dual left anterior descending coronary artery: angiographic description of important variants and surgical implications. Am Heart J. 1983 Mar; 105(3):445–455.
View at Publisher | View at Google Scholar - Akbarzadeh F, Shadravan S, Ghorbanian M, Piri R, Naghavi-Behzad M. Double Left Anterior Descending Coronary Artery Originating from Left Main Coronary Stem and Right Coronary Artery. J Cardiovasc Thorac Res. 2013; 5(2):73–75.
View at Publisher | View at Google Scholar - Oncel G, Oncel D. A Rare Coronary Artery Anomaly: Double Left Anterior Descending Artery. J Clin Imaging Sci. 2012 Dec 27; 2:83.
View at Publisher | View at Google Scholar - Kosar F. An unusual case of double anterior descending artery originating from the left and right coronary arteries. Heart Vessels. 2006 Nov 1; 21(6):385–387.
View at Publisher | View at Google Scholar
