

Review Article | DOI: https://doi.org/10.31579/2834-8664/024
DPP - 4 inhibitors in Type 2 Diabetes mellitus - A Panoramic Review
1 Assistant professor of Surgery, Dhiraj Medical College and Sumandeep Vidyapeeth, Baroda.
2 Superitendent and Professor of Medicine at SAL Institute of Medical Sciences, Ahmedabad).
*Corresponding Author: Devershri Trivedi, Assistant professor of Surgery, Dhiraj Medical College and Sumandeep Vidyapeeth, Baroda.
Citation: Dirgha Gujarathi, Jayesh Trivedi, (2023), DPP - 4 inhibitors in Type 2 Diabetes mellitus - A Panoramic Review, International Journal of clinical and Medical Case Reports, 2(3); Doi:10.31579/2834-8664/024
Copyright: : © 2023 Leonard B. Goldstein, This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 11 May 2023 | Accepted: 23 May 2023 | Published: 30 May 2023
Keywords: heart disease; homelessness; surgeries
Abstract
Patients who are homeless regularly must overcome tremendous barriers to obtain health care post discharge from hospitalizations, surgeries, emergency departments, and urgent care clinics. Lack of health insurance and financial hardship are commonly experienced by many people in the United States living below the poverty line. Often, basic needs such as food and shelter outweigh obtaining proper healthcare. An aspect of healthcare that frequently burdens individuals who are homeless is proper wound care. With many homeless individuals experiencing multiple health comorbidities leading to chronic wounds (diabetic ulcers, chronic ulcers, venous insufficiency, lack of properly fitting shoes, needle injuries, injuries from the environment, mental illness, post-surgical incisions), it appears imperative that we must do a better job at implementing effective wound care strategies when working with this specific population. This review prompts a current analysis of what the standard for wound care is in our homeless population in addition to what means this population has to obtain proper materials and education for wound healing. We propose a call to action for emergency departments, free clinics, and shelters to offer additional education and supplies for chronic wounds seen in patients experiencing homelessness.
Introduction
Diabetes mellitus, commonly referred to as diabetes, is a chronic metabolic disorder characterized by elevated blood glucose levels, known as Hyperglycaemia. Its results from the body’s inability to effectively utilize or produce insulin, a hormone essential for regulating blood sugar. Diabetes is a complex condition with multiple forms, including type 1 diabetes, type 2 diabetes, and gestational diabetes, each with distinct etiologies and pathophysiological mechanisms.
- Type 1 Diabetes: This form of diabetes, often diagnosed in childhood or adolescence, arises due to autoimmune destruction of the insulin – producing beta cells in the pancreas. As a result, individuals with type 1 diabetes must rely on exogenous insulin administration to manage their blood glucose levels effectively.
- Type 2 Diabetes: This is more prevalent among adults, typically develops when the body becomes resistant to the actions of insulin, or when the pancreas fails to produce sufficient insulin to meet the body’s demands. Risk factors for type 2 diabetes include genetics, obesity, sedentary lifestyle, and poor dietary habits. Lifestyle modifications, oral medications, and insulin therapy may be required to control blood sugar in type 2 diabetes.
- Gestational Diabetes: Occurring during pregnancy, gestational diabetes is characterized by elevated blood glucose levels that may pose risks to both the mother and the unborn child. While gestational diabetes often resolves after childbirth, it increases the risk of developing type 2 diabetes later in life.
- LADA: Associated with autoimmune condition where destruction of beta cells of pancreas take place and this is a partial insulin dependent diabetes.
Complications of uncontrolled diabetes can lead to a range of serious medical conditions, including cardiovascular disease, kidney disease, neuropathy, retinopathy, and more. Hence, early diagnosis, appropriate management, and ongoing monitoring are crucial for individuals living with diabetes.
Management of diabetes involves a comprehensive approach encompassing dietary modifications, physical activity, medications, and regular monitoring of blood glucose levels. Advancements in medical technology, such as continuous glucose monitoring and insulin delivery systems, have improved the precision and ease of diabetes management [1,2].
Dipeptidyl Peptidase – 4 (DPP – 4) inhibitors, also known as gliptins, are a class of medications used in the management of type 2 diabetes mellitus. They act by targeting the enzyme Dipeptidyl peptidase – 4, which plays a role in the degradation of incretin hormones. Incretins are gut hormones, such as glucagon – like peptide – 1 (GLP – 1) and glucose – dependent insulinotropic peptide (GIP), that stimulate insulin release and reduce glucagon secretion in a glucose – dependent manner. By inhibiting DPP -4, these medications prolong the action of incretins, leading to improved blood glucose control.
Mechanism of Action:
DPP -4 inhibitors work by inhibiting the enzymatic activity of Dipeptidyl peptidase -4, which is responsible for rapidly degrading GLP -1 and GIP. These hormones are secreted by the intestines in response to nutrient ingestion and play a crucial role in regulating blood sugar levels. When DPP – 4 activity is inhibited, incretin hormones are protected from degradation, leading to increased insulin secretion and reduced glucagon release from pancreatic islet cells. This results in in improved glucose utilization and reduced blood glucose levels [3].
Pharmacokinetics:
DPP -4 inhibitors are orally administered and are generally well – absorbed from the GIT. They have a relatively short half – life, ranging from 2 to 12 hours, depending on the specific medication. Notable DPP -4 inhibitors include Sitagliptin, Saxagliptin, Linagliptin and Alogliptin, among others. These medications are mainly eliminated via renal excretion, and dosage adjustments may be necessary in patients with renal impairment [4]
Clinical Efficacy:
Clinical trials and real – world studies have demonstrated the effectiveness of DPP – 4 inhibitors in reducing haemoglobin A1C (HbA1c) levels, which reflects long – term blood glucose control. They are typically used as monotherapy or in combination with other oral anti diabetic agents or insulin to achieve glycaemic control in patients with type 2 diabetes. DPP – 4 inhibitors are associated with a lower risk of hypoglycaemia compared to some other diabetes medications, making them an attractive option for individuals who are at risk of low blood sugar.
Safety Profile:
DPP – 4 inhibitors are generally well – tolerated, with few significant side effects. Common adverse events may include upper respiratory tract infections, headache, and GI symptoms such as nausea and diarrhea. These side effects are typically mild and transient. Rare but serious adverse events like pancreatitis and joint pain have been reported, although a direct causal relationship has not been definitively established [5,6].

Figure 1: Structure of Dipeptidyl - peptidase - 4 inhibitors.
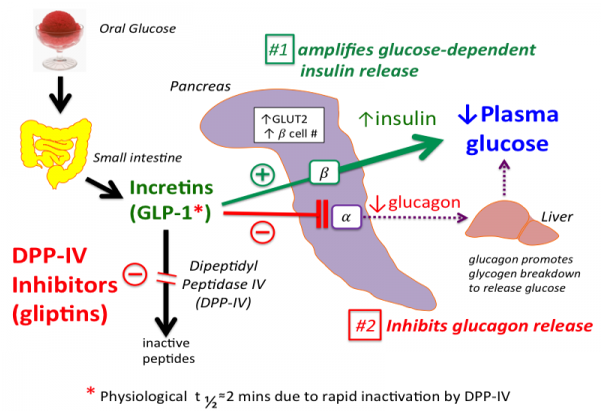
Figure 2: Site of Action of DPP-4 inhibitors.
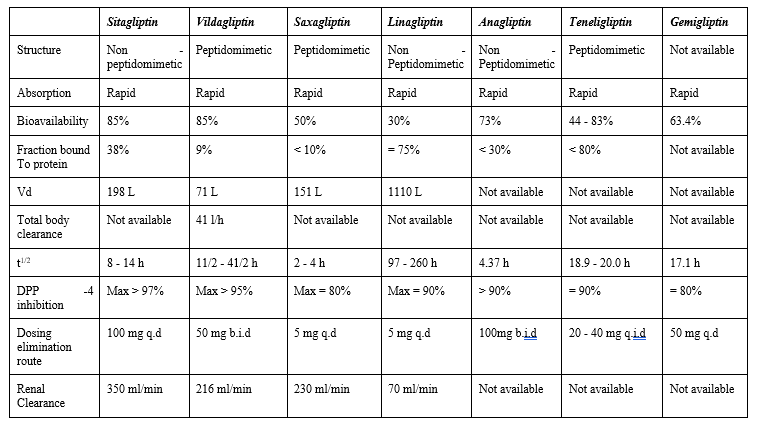
Table 1: Clinical and Pharmacokinetic characteristics of DPP 4 inhibitors
Clinical Pharmacology
- Sitagliptin:
Sitagliptin, commonly marketed under the brand name Januvia, is a medication used to manage type 2 diabetes. It is part of the class of drugs known as Dipeptidyl peptidase - 4 (DPP -4 ) inhibitors or gliptins. Sitagliptin works by inhibiting the enzyme DPP - 4, which in turn increases the levels of incretin hormones like glucagon - like peptide - 1(GLP -1) and glucose - dependent insulinotropic polypeptide (GIP). These hormones help regulate blood sugar levels by increasing insulin release and reducing the release of glucagon [7].
- Mode of Action: Sitagliptin inhibits the enzyme DPP - 4, which prolongs the activity of GLP -1 and GIP. This results in increased insulin secretion and decreased glucagon release, helping to lower blood sugar levels.
- Dosage: The typical recommended dosage is 100 mg taken orally once daily. However, dosages may be adjusted based on an individual’s specific needs and health condition.
- Efficacy: Sitagliptin can be effective in lowering HbA1c levels when used as part of a comprehensive diabetes management plan, which includes dietary changes and physical activity.
- Side Effects: Common side effects of Sitagliptin may include upper respiratory tract infections, headache, and stomach discomfort. It is generally well - tolerated, and severe side effects are rare.
- Renal Dosing: Dose adjustments may be necessary for individuals with impaired kidney function. A lower dose is recommended in these cases.
- Availability: It is widely available and has been used as treatment option for type 2 diabetes for several years.
- Combination Therapy: Sitagliptin can be prescribed as a monotherapy or in combination with other diabetes medications, such as metformin or sulfonylureas.
- Hypoglycaemia Risk: Sitagliptin has a low risk of causing hypoglycemia when used as a monotherapy. However, the risk of hypoglycemia may increase when combined with other diabetes medications that can cause low blood sugar.
- Precautions: Patients with a history of pancreatitis should use sitagliptin with caution, as there have been reports of pancreatitis associated with DPP -4 inhibitors [8].
1.2.Vildagliptin:
Vildagliptin, marketed under the brand name Galvus, is a medication used to manage type 2 diabetes type 2 diabetes mellitus. It is classified as DPP -4 inhibitor or gliptin. It helps control blood sugar levels by inhibiting the enzyme DPP - 4, which leads to increased levels of the hormone glucagon - like peptide - 1 (GLP -1) and glucose -dependent insulinotropic polypeptide (GIP). These hormones play a role in regulating blood sugar by increasing insulin secretion and reducing glucagon release from the pancreas[7].
- Mode of Action: Vildagliptin works by inhibiting DPP-4, which prolongs the activity of GLP-1 and GIP, leading to improved glucose regulation.
- Dosage: The typical recommended dosage of vildagliptin is 50 mg taken orally twice daily, usually with meals. However, dosages may be adjusted based on individual needs and health outcomes.
- Efficacy: It can effectively lower HbA1c levels when used as part of a comprehensive diabetes management plan, which may include lifestyle changes, diet and exercise.
- Side Effects: Common side effects of vildagliptin may include headache, upper respiratory tract infections, and GI symptoms like nausea or diarrhea. Overall, it is well - tolerated, and severe side effects are rare.
- Renal Dosing: Dose adjustments are recommended for individuals with kidney impairment. The dosage may need to be reduced in these cases.
- Availability: It is available in many countries, but it may not be available in the United States.
- Combination Therapy: It can be prescribed as a monotherapy or in combination with other diabetes medications, such as metformin or sulfonylureas.
- Hypoglycemia Risk: It has a relatively low risk of causing hypoglycemia when used alone. However, the risk of causing hypoglycemia increase when it is combined with other diabetes medications that can cause low blood sugar.
- Precautions: As with all diabetes medications, individuals with diabetes should work closely with their healthcare provider to determine the most appropriate treatment plan, including medication choice and dosage. Vildagliptin should be used cautiously in individuals with a history of pancreatitis [9].
- Saxagliptin:
Saxagliptin, marketed under the brand name Ongluza, is a medication used for the management of type 2 diabetes mellitus. It belongs to the class of drugs known as DPP - 4 inhibitors or gliptins. Saxagliptin helps control blood sugar levels by inhibiting the enzyme DPP - 4, which leads to increased levels of the hormone glucagon - like peptide - 1 (GLP - 1) and glucose - dependent insulinotropic polypeptide (GIP). These hormones play a role in regulating blood sugar by increasing insulin secretion and decreasing glucagon release from the pancreas [7].
- Mode of Action: Saxagliptin inhibits DPP - 4, which prolongs the action of GLP -1 and GIP, resulting in improved blood sugar control.
- Dosage: The typical recommended dosage of saxagliptin is 5 mg taken orally once daily. However, dosages may be adjusted based on individual needs and health conditions.
- Efficacy: It can effectively lower HbA1c levels when used as part of a comprehensive diabetes management plan, which may include lifestyle changes, diet, and exercise.
- Side Effects: Common side effects of Saxagliptin may include upper respiratory tract infections, urinary tract infections, and headaches. It is generally well - tolerated, and severe side effects are rare.
- Renal Dosing: Dose adjustments are recommended for individuals with kidney impairment. The dosage may need to be reduced in these cases.
- Availability: Saxagliptin is available in several countries, including United States.
- Combination Therapy: Saxagliptin can be prescribed as a monotherapy or in combination with other diabetes medications that can cause low blood sugar.
- Precautions: Individuals with a history of pancreatitis should use saxagliptin with caution, as there have been reports of pancreatitis associated with DPP- 4 inhibitors [10].
- Linagliptin:
Linagliptin, marketed under the brand name Tradjenta, is a medication used to manage type 2 diabetes mellitus. It is a member of the DPP -4 inhibitor class of drugs, also known as gliptins. Linagliptin helps control blood sugar levels by inhibiting the enzyme DPP - 4, which increases the levels of the hormones glucagon - like peptide -1 (GLP - 1) and glucose - dependent insulinotropic polypeptide (GIP). These hormones play a role in regulating blood sugar by stimulating insulin release and inhibiting glucagon release from the pancreas [7].
- Mode of Action: Linagliptin inhibits DPP - 4, which prolongs the action of GLP - 1 and GIP, leading to improved blood sugar control.
- Dosage: The typical recommended dosage of linagliptin is 5 mg taken orally once daily. Linagliptin is unique among DPP - 4 inhibitors in that it does not require dose adjustments based on kidney function. It can be used without dosage modification in patients with both normal and impaired kidney function.
- Efficacy: Linaglitptin can effectively lower Hb1Ac levels when used as part of a comprehensive diabetes management plan, which may include lifestyle changes, diet, and exercise.
- Side Effects: It is generally well - tolerated. Common side effects may include upper respiratory tract infections, nasopharyngitis, and headaches. It has a relatively low risk of causing hypoglycemia when used alone.
- Availability: Linagliptin is available in many countries.
- Combination Therapy: It is prescribed as a monotherapy or in combination with other diabetes medications, such as metformin or sulfonylureas.
- Hypoglycemia Risk: Linagliptin has a low risk of causing hypoglycemia when use as a monotherapy. However, the risk of hypoglycemia may increase when it is combined with other diabetes medications, that can cause low blood sugar.
- Precautions: As with all diabetes medications, individuals with history of pancreatitis should use linagliptin with caution, as there have been reports of pancreatitis associated with DPP -4 inhibitors [11].
- Anagliptin:
Analgliptin is a DPP -4 inhibitor used to manage type 2 diabetes mellitus. Like other DPP -4 inhibitors, Analgliptin works by inhibiting the DPP - 4 enzyme, which increases the levels of certain hormones like GLP - 1 and GIP. These hormones help regulate blood sugar levels by increasing insulin secretion and decreasing glucagon release from the pancreas [7].
- Mode of Action: Analgliptin inhibits DPP -4, which leads to the prolongation of the effects of GLP -1 and GIP, resulting in improved blood sugar control.
- Dosage: The typical recommended dosage of Analgliptin may vary depending in the patient’s specific needs and the country in which it is prescribed. Common dosages may include 25 mg or 50 mg taken orally once daily.
- Efficacy: Analgliptin, like other DPP -4 inhibitors, can effectively lower Hb1Ac levels when used as part of a comprehensive diabetes management plan, which may include lifestyle changes, diet and exercise.
- Side Effects: Common side effects are generally mild and may include upper respiratory tract infections, headaches, and GI symptoms such as nausea or diarrhea. It is generally well - tolerated, and severe side effects are rare.
- Renal dosing:Dose adjustments may be required for individuals with impaired kidney function. The dosage may need to be reduced in these cases.
- Availability: The availability of Analgliptin may vary by country, and it may not be available in all regions.
- Combination Therapy: Analgliptin can be prescribed as a monotherapy or in combination with other diabetes medications, such as metformin or sulfonylureas.
- Hypoglycemia risk: Analgliptin has a relatively low risk of causing hypoglycemia may increase when it is combined with other diabetes medications that can cause low blood sugar.
- Precautions: As with all diabetes medications, individuals with a history of pancreatitis should use Analgliptin with caution, as there have been reports of pancreatitis associated with DPP - 4 inhibitors [12].
- Teneligliptin:
It is a DPP -4 inhibitor used to manage type 2 diabetes mellitus. Like other DPP -4 inhibitors, teneligliptin works by inhibiting the DPP - 4 enzyme, which increases the levels of certain hormones like GLP - 1 and GIP. These hormones help regulate blood sugar levels by increasing insulin secretion and decreasing glucagon release from the pancreas [7].
- Mode of Action: Teneligliptin inhibits DPP -4, which prolongs the action of GLP -1 and GIP. Resulting in improved blood sugar control.
- Dosage: The typical recommended dosage of teneligliptin may vary depending on the patient’s specific needs and the country in which it is prescribed. Common dosages may include 20 mg or 40 mg taken orally once daily.
- Efficacy: Teneligliptin can effectively lower HbA1c levels when used as part of a comprehensive diabetes management plan, which may include lifestyle changes, diet and exercise.
- Side Effects: Common side effects are generally mild and may include upper respiratory tract infections, headaches, and GI symptoms such as nausea or diarrhea. It is generally well - tolerated, and severe side effects are rare.
- Renal Dosing: Dose adjustments may be required for individuals with impaired kidney function. The dosage may need to be reduced in these cases.
- Availability: Teneligliptin is available in several countries, primarily in Asia. It’s availability may vary by region.
- Combination Therapy: Teneligliptin can be prescribed as a monotherapy or in combination with other diabetes medications, such as metformin or sulfonylureas.
- Hypoglycemia Risk: Teneligliptin has relatively low risk of causing hypoglycemia when used alone. However, the risk of hypoglycemia may increase when it is combined with other diabetes medications that can cause low blood sugar[13].
- Gemigliptin:
Gemigliptin is a medication used for the management of type 2 diabetes mellitus. It is a DPP -4 inhibitor, belonging to the class of drugs known as gliptins. Gemigliptin works by inhibiting the enzyme DPP - 4, which increases the levels of hormones glucagon - like peptide - 1 (GLP-1) and Glucose - dependent insulinotropic polypeptide (GIP). These hormones play a role in regulating blood sugar levels by increasing insulin secretion and reducing glucagon release from the pancreas [7].
- Mode of Action: Gemigliptin inhibits DPP - 4, which prolongs the action of GLP - 1 and GIP, leading to improved blood sugar control.
- Dosage: The typical recommended dosage of gemigliptin may vary depending on the patient’s specific needs and the country in which it is prescribed. Common dosages may include 25 mg or 50 mg taken orally once daily.
- Efficacy: It is effectively lower Hb1Ac levels when used as part of a comprehensive diabetes management plan, which may include lifestyle changes, diet and exercise.
- Side Effects: Common side effects are generally mild and may include upper respiratory tract infections, headaches, and GI symptoms such as nausea or diarrhea. It is generally well - tolerated, and severe side effects are rare.
- Renal Dosing: Dose adjustments may be required for individuals with impaired kidney function. The dosage may need to be reduced in these cases.
- Availability: Gemigliptin is available in several countries, primarily in Asia and the Middle East. Its availability may vary by region.
- Combination Therapy: Gemigliptin has a relatively low risk of causing hypoglycemia when used alone. However, the risk of hypoglycemia may increase when it is combined with other diabetes medications that can cause low blood sugar.
- Precautions: As with all diabetes medications, individuals with a history of pancreatitis should use gemigliptin with caution, as there have been reports of pancreatitis associated with DPP-4 inhibitors [14].
Adverse Effects of DPP - 4 inhibitors
2.1 Hypoglycemia:
DPP - 4 inhibitors are not known to cause hypoglycemia when used as monotherapy. However, when used in combination with other anti - diabetic medications, such as sulfonylureas or insulin, there may be an increased risk of hypoglycemia, especially if the doses of these medications are not adjusted properly.
2.2 Nasopharyngitis:
Some patients may experience symptoms such as a runny or stuffy nose, sneezing, sore throat, or cough while taking DPP - 4 inhibitors. This side effect is usually mild and not a cause for concern.
2.3 Headache:
Headaches are a relatively common side effect of DPP - 4 inhibitors. They are usually mild and transient.
2.4 Gastrointestinal Disturbances:
Some people may experience gastrointestinal symptoms, such as abdominal pain, nausea, diarrhea, or constipation while taking DPP - 4 inhibitors. These symptoms are generally mild and may improve over time.
2.5 Pancreatitis:
There have been reports of pancreatitis (inflammation of the pancreas) associated with DPP - 4 inhibitors, although there is a rare side effect. Patients taking these medications should be aware of the symptoms of pancreatitis, such as severe abdominal pain that may radiate to the back, and seek medical attention if they occur.
2.6 Allergic Reactions:
While rare, some individuals may experience allergic reactions to DPP - 4 inhibitors. Symptoms of an allergic reaction may include rash, itching, swelling, severe dizziness, or difficulty breathing. Any signs of an allergic reaction should prompt immediate medical attention.
2.7 Join Pain:
Some patients on DPP - 4 inhibitors have reported joint pain. This side effect is generally mild and reversible upon discontinuation of the medication.
2.8 Skin Reactions:
In rare cases, DPP - 4 inhibitors have been associated with skin reactions, including bullous pemphigoid, a blistering skin disorder. Patients should report any unusual skin symptoms to their healthcare provider.
2.9 Heart Failure:
Some studies have raised concerns about a potential increased risk of heart failure associated with DPP - 4 inhibitors particularly with Saxagliptin. Teneligliptin is known to prolong QT interval.While more research is needed to clarify this risk, individuals with a history of heat failure should discuss the potential benefits and risks of these medications with their healthcare provider. Incidences of hospitalization for cardiac failure on account of usage of this molecule is been recorded but mortality is not increased.
2.10 Musculoskeletal Pain:
Musculoskeletal pain, including back pain and arthralgia (joint pain), has been reported as a side effect of DPP - 4 inhibitors in some studies. It is generally mild and reversible upon discontinuation.
Conclusion
The pharmacokinetic characteristics of DPP-4 inhibitors are very similar and have a comparable mode of action. The pharmacokinetic features of these drugs vary, nevertheless, depending on the chemical. These variations include the half-life, bioavailability, protein binding, metabolism to active metabolites, and elimination pathways. For instance, all medications, with the exception of linagliptin and teneligliptin, should have their dosages adjusted in patients with chronic renal disease. Saxagliptin has the highest likelihood of interacting with other medications among DPP-4 inhibitors, which typically have a minimal risk of doing so. When selecting a DPP-4 inhibitor for each patient, the clinician should take into account the variations in the pharmacokinetic profile discussed analytically above.
Although there have only been a few head-to-head comparison studies, DPP-4 inhibitors show similar adverse effect profiles in clinical trials and seem to be linked to low rates of major adverse events. Nasopharyngitis, headaches, and perhaps urinary tract infections are among the side effects that DPP-4 inhibitors are associated with more frequently than placebo. However, post-marketing surveillance has shown less frequent adverse events that need more examination, including those related to pancreatic inflammation and cancer as well as skin and immune-associated consequences. In general, more study is required to understand these uncommon side effects, especially for the more recent DPP-4 inhibitors.
Declaration of Interest
No organization or firm provided financial support for this review; it was completed independently.
Abbreviations
DPP - 4: Dipeptidyl Peptidase
GIP: Glucose - dependent insulinotropic polypeptide
GLP -1: glucagon - like peptide - 1
GIT: Gastrointestinal Tract
HbA1c: Glycated Haemoglobin
Vd: Volume of Distribution
t1/2: Half - life (refers to the time required for plasma concentration of a drug to decrease by 50%).
LADA: Latent autoimmune diabetes in adults.
References
- American Diabetes Association. (2020). “2. Classification and Diagnosis of Diabetes: Standards of Medical Care in Diabetes – 2020.” Diabetes Care, 43 (Supplement 1), S14 –S31.
View at Publisher | View at Google Scholar - American Diabetes Association. (2021).”1. Improving Care and Promoting Health in Populations: Standards of Medical Care in Diabetes – 2021.” Diabetes Care, 44 (Supplement 1), S7 – S14.
View at Publisher | View at Google Scholar - Drucker, D.J., & Nauck, M.A. (2006). The incretin system: glucagon – like peptide – 1 receptor agonists and Dipeptidyl peptidase – 4 inhibitors in type 2 diabetes. The Lancet, 368 (9548), 1696 – 1705.
View at Publisher | View at Google Scholar - Scheen, A.J. (2018). Cardiovascular effects of new oral glucose – lowering agents: DPP – 4 and SGLT – 2 inhibitors. Circulation Research, 122(10), 1439 – 1459.
View at Publisher | View at Google Scholar - American Diabetes Association. (2021). Standards of Medical Care in Diabetes – 2021. Diabetes Care, 44(Supplement _1), S1 – S232.
View at Publisher | View at Google Scholar - Nauck, M.A., & Meier, J.J. (2018). Incretin hormones: their role in health and disease. Diabetes, Obesity and Metabolism, 20(Suppl 1), 5 -21.
View at Publisher | View at Google Scholar - Vincent SH, Reed JR, Bergman AJ, et al. Metabolism and excretion of the dipeptidyl peptidase 4 inhibitor [14C] sitagliptin in humans. Drug Metab Dispos 2007;35:533-8.
View at Publisher | View at Google Scholar - Migoya EM, Stevens CH, Bergman AJ, et al. Effect of moderate hepatic insufficiency on the pharmacokinetics of sitagliptin. Can J Clin Pharmacol 2009;16:e165-70.
View at Publisher | View at Google Scholar - Augeri DJ, Robl JA, Betebenner DA, et al. Discovery and preclinical profile of saxagliptin (BMS-477118): a highly potent, long-acting, orally active dipeptidyl peptidase IV inhibitor for the treatment of type 2 diabetes. J Med Chem 2005;48:5025-37.
View at Publisher | View at Google Scholar - Wang A, Dorso C, Kopcho L, et al. Potency, selectivity and prolonged binding of saxagliptin to DPP4: maintenance of DPP4 inhibition by saxagliptin in vitro and ex vivo when compared to a rapidly-dissociating DPP4 inhibitor.
View at Publisher | View at Google Scholar - general.takedapharm.com/content/file/pi.pdf?applicationcode=66B0B942-E82B46AD-886A-F4AA59F5F33C&File TypeCode=NESINAPI [Accessed at 24 December 2013].
View at Publisher | View at Google Scholar - Blech S, Ludwig-Schwellinger E, Grafe-Mody EU, et al. The metabolism and disposition of the oral dipeptidyl peptidase-4 inhibitor, linagliptin, in humans. Drug Metab Dispos 2010;38:667-78.
View at Publisher | View at Google Scholar - Fuchs H, Runge F, Held HD. Excretion of the dipeptidyl peptidase-4 inhibitor linagliptin in rats is primarily by biliary excretion and P-gp-mediated efflux. Eur J Pharm Sci 2012;45:533-8.
View at Publisher | View at Google Scholar - Linagliptin EMEA EPAR. Available from: http://www.ema.europa.eu/docs/ en_GB/document_library/EPAR_-_Product_Information/human/002110/ WC500115745.pdf [Accessed at 24 December 2013].
View at Publisher | View at Google Scholar
