

Research Article | DOI: https://doi.org/10.31579/2834-8486/003
Desmoid tumour Treatment Outcome: A single institution experience
- Mohamed Hegazy *
Section of Radiation Oncology, King Faisal Specialist Hospital and Research Centre, Riyadh, Saudi Arabia.
*Corresponding Author: Section of Radiation Oncology, King Faisal Specialist Hospital and Research Centre, Riyadh, Saudi Arabia.
Citation: Hegazy M. (2022). Desmoid tumour Treatment Outcome: A single institution experience. Biomedical and Clinical Research. 1(1); DOI:10.31579/2834-8486/003
Copyright: © 2022 Mohamed Hegazy, This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 15 October 2022 | Accepted: 19 October 2022 | Published: 30 September 2022
Keywords: desmoid tumour; surgical margin; radiotherapy
Abstract
Desmoid tumour (DT) is a rare locally aggressive disease with tendency for local recurrence and the peak incidence age of 30-40 years.
DT prognostic factors are still conflicting like surgical margin, disease location, age and gender.
The various treatment options including surgery, radiotherapy and systemic agents are generally offered according to the disease presenting symptoms and progressiveness.
Introduction
Desmoid tumour (DT) is a rare locally aggressive disease with tendency for local recurrence [1] and the peak incidence age of 30-40 years [2]
DT prognostic factors are still conflicting like surgical margin [3,4,5-10], disease location [3,5,9,11], age and gender [5,8,12,13].
The various treatment options including surgery, radiotherapy and systemic agents are generally offered according to the disease presenting symptoms and progressiveness [14-20].
Complete surgical resection without causing significant morbidity can be challenging. The administration of adjuvant radiotherapy may improve local control but can cause side effects like fibrosis and wound healing problems [3, 4, 21, 22], rarely there is concerns about development of radiation induced second malignancies.
The aim of this work is to present our experience using multidisciplinary team to reach the best treatment outcome for this locally aggressive disease and report the long-term outcomes of treatment.
Patients and Methods
The medicalrecords of total of 72 consecutive patients diagnosed with DT over a period of 10 years between January 2009 and December 2018 were reviewed at RadiationOncology section, King Faisal Specialist Hospital & Research Centre (KFSH&RC), Riyadh, Saudi Arabia. All the patients had biopsy proven DT at our institution in addition to baseline and periodic follow up CT and/or MRI scans.
Radiotherapy was delivered as definitive, preoperative or postoperative treatment. Radiation doses were 50 - 66 Gy in 2 Gy per fraction as preoperative, postoperative and definitive radiotherapy. Radiation energy was 4-6MeV delivered by either3D-Conformal Radiation Therapy, Tomotherapy or Volumetric Modulated Arc Therapy techniques. Surgery was either wide local excision or intralesional debulking.
Statistical analysis
Continuous data were checked for normality by using Shapiro Walk test. Kruskal Wallis H test was used to compare more than two groups of non-normally distributed data. Percent of categorical variables were compared using Pearson’s Chi-square test or Fisher's exact test when was appropriate. Stratification of Recurrence Free Survival was done according intention to treat (ITT). These time-to-event distributions were estimated using the method of Kaplan-Meier plot, and compared using two-sided exact log-rank test. All tests were two sided. All statistics were performed using SPSS 22.0 for windows (IBM Inc., Chicago, IL, USA) and Med Calc 13 for windows (Med Calc Software bvba, Ostend, Belgium).
Results
Patient characteristics
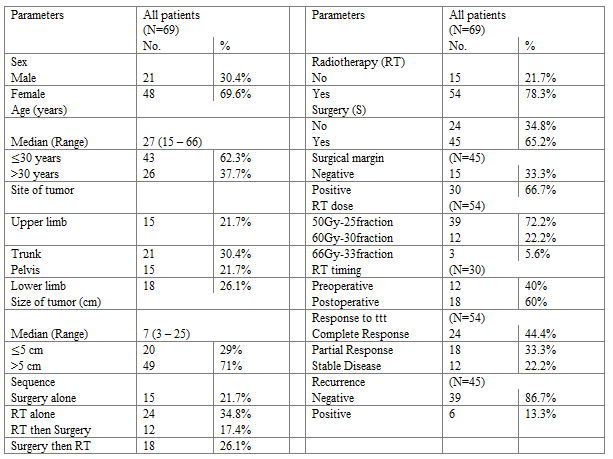
Two patients opted to undergo observation only and 1 patient opted to receive systemic treatment with Sorafenib who were excluded from the study. Therefore, total of 69 patients were evaluated (Table 1).
The median age of patient was 27 years (range 15-66) and approximately two-thirds were females. The majority were younger patients aged less than 30 years (n=43, 62 Percentage).
Tumour characteristics
The median size was 7 cm (range, 3-25cm) and nearly two third of the patients had tumours larger than 5 cm. The most common site was trunk (n=21, 30 Percentage), followed by lower limbs (n=18, 26 Percentage), pelvis (n=15, 22 Percentage), and upper limbs (n=15, 22 Percentage).
Treatment characteristics
Twenty four patients were treated with definitive radiotherapy, 15 patients by surgical resection alone and 30 patients by combination of both surgery and radiotherapy (12 cases had preoperative and 18 cases had postoperative irradiation).
The surgical margin was positive in 30 patients out of total of 45 cases who had surgery (67 Percentage). Radiation was given to total of 54 cases with doses of 50 Gy in 25 fractions delivered in 39 cases (72 Percentage) and 60- 66 Gy in 15 cases (28 Percentage) (Table 2).
Response to treatment
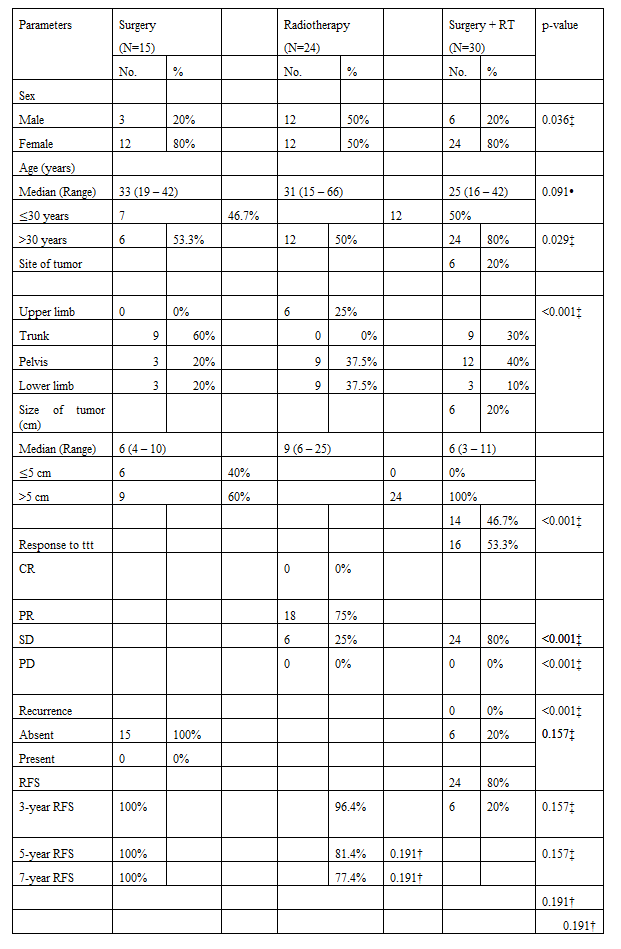
The median follow up was 5.5 years (range 1- 10yrs). The local control in patients who had radiotherapy (n=54 pts) as part of their treatment was 89 Percentage. The patients who had surgery (n=45 pts) as a part of the treatment had local control of 87 Percentage (Table 2).
Surgery alone group
The patients who had surgery (n=15) alone had no recurrence.
Radiotherapy alone group
The local control in patients who had definite radiotherapy (n=24) was 100 Percentage with partial response in 18 pts (75 Percentage) and stable disease in 6 pts (25 Percentage). All the patients who had definite radiotherapy had size greater than 5cm.
Combined Surgery and radiotherapy group
All the patients who had combined surgery and radiotherapy (either pre or post-operative) had positive margins. The local control in patients with positive surgical margin (n=30 pts) and radiotherapy was 80 Percentage (n=6 patients developed recurrence). All the recurrences happened in the lower radiotherapy dose of 50 Gy and those who had post operative radiotherapy. There was no recurrence in the higher radiotherapy dose of 60 Gy (p= 0.05) and those who had pre operative radiotherapy (p=0.05). The patients group treated with surgery plus radiotherapy most of the recurrence was in patients with tumour size less than 5 cm (5 out of total of 6 recurrent patients). There was no recurrence in the patients with trunk site and all the recurrences happened in the extremities group. All the recurrences were in the less than 30 years group (Table 2).
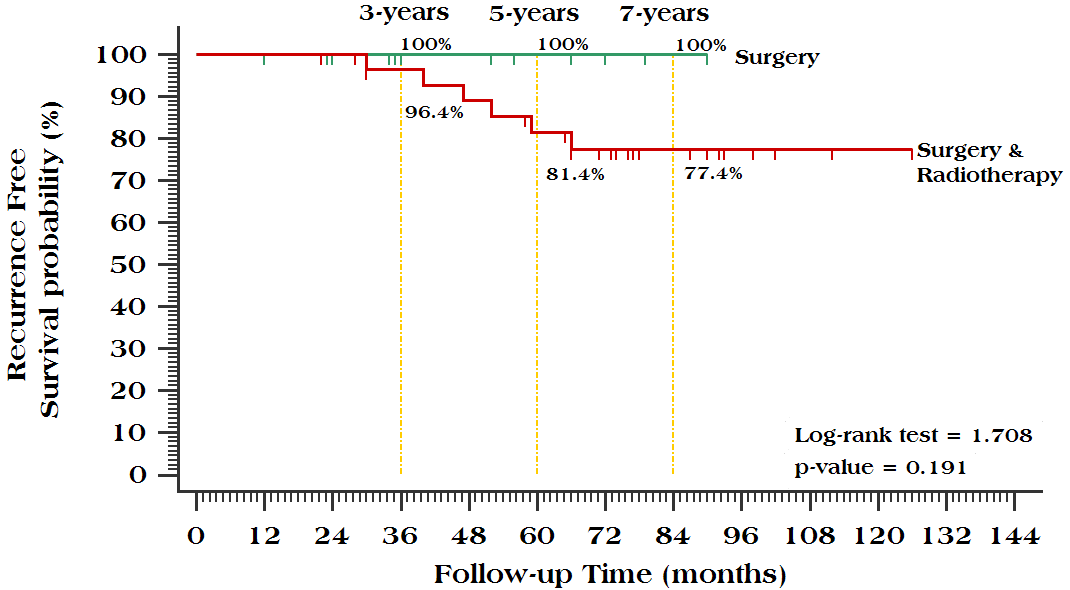
Survival and long term side effects
The 3yrs, 5yrs and 7yrs recurrence free survival in patients who had both surgery and radiotherapy was 96.4 Percentage, 81.4 Percentage and 77.4 Percentage respectively. There was no grade 3 or 4 acute or late toxicity in all the groups of patients. There was no incidence of second malignancy in this cohort of patients at median follow up of 5.5 years (Figure 1).
Discussion
Desmoid tumour is benign tumour of connective tissue but with high chances of local recurrence. Surgery is the main treatment modality of therapy if it can be done with acceptable morbidity. Radiotherapy is given in locally advanced inoperable tumours as definitive therapy or in combination with surgery in high risk tumours. The radiation dose used is 50-66 Gy depending on the tolerance dose to the surrounding organs of risk. The clinical course can be variable and rarely may undergo spontaneous regression. Therefore, close observation to monitor the rate of growth is a reasonable option if patient is minimally symptomatic or even when the surgical margins are positive when reresection is possible without significant morbidity.
In our cohort regarding to gender and age, females have aggressive disease similar to studies reported by [5, 8, 12 & 13] while age 30 years or less has poor prognosis as in series by [5, 8& 12] while aggressive in age more than 30 years in series by Rock et al [11] and less than 32 years by Sorensen et al [13].
In our study regarding to site, the extremities have a worse disease while the trunk has a more favorable outcome similar to Ballo et al [3], Broekhoven et al [8], Huang [9] and Rock et al [11] while non-significant in Merchant et al [5].
References
- Penel N, Coindre JM, Bonvalot S, Italiano A, Neuville A, et al. (2016) Management of desmoid tumours: a nationwide survey of labelled reference centre networks in France. Eur J Cancer. 58. 90-96.
View at Publisher | View at Google Scholar - Kasper B, Stroebel P, Hohenberger P. (2011) Desmoid tumors – clinical features and treatment options for advanced disease. The Oncologist. 16:682-693.
View at Publisher | View at Google Scholar - M.T. Ballo, G.K. Zagars, A. (1999). Pollack, P.W. Pisters, R.A. Pollack, Desmoid tumor: Prognostic factors and outcome after surgery, radiation therapy, or combined surgery and radiation therapy, J. Clin. Oncol. 17. 158-167.
View at Publisher | View at Google Scholar - B.W. Goy, S.P. Lee, F. Eilber, F. Dorey, J. Eckardt, et al. (1997). The role of adjuvant radiotherapy in the treatment of resectable desmoid tumors, Int. J. Radiat. Oncol. Biol. Phys. 39. 659-665.
View at Publisher | View at Google Scholar - N.B. Merchant, J.J. Lewis, J.M. Woodruff, D.H. Leung, M.F. Brennan, (1999). Extremity and trunk desmoid tumors: a multifactorial analysis of outcome, Cancer 86. 2045-2052.
View at Publisher | View at Google Scholar - A. Gronchi, P.G. Casali, L. Mariani, S. Lo Vullo, M. Colecchia, et al., J. Rosai, (2003). Quality of surgery and outcome in extra-abdominal aggressive fibromatosis: a series of patients surgically treated at a single institution, J. Clin. Oncol. Off. J. Am. Soc. Clin. Oncol. 21. 1390-1397.
View at Publisher | View at Google Scholar - K. Huang, H. Fu, Y.-Q. Shi, Y. Zhou, C.-Y. Du, (2009). Prognostic factors for extraabdominal and abdominal wall desmoids: a 20-year experience at a single institution, J. Surg. Oncol. 100. 563-569.
View at Publisher | View at Google Scholar - D.L.M. van Broekhoven, C. Verhoef, S.G. Elias, A.J. Witkamp, J.M.H.H. van Gorp, et al. (2013). Local recurrence after surgery for primary extra-abdominal desmoid-type fibromatosis, Br. J. Surg. 100. 1214-1219.
View at Publisher | View at Google Scholar - K. Huang, C.M. Wang, J.G. Chen, C.Y. Du, Y. Zhou, et al., (2014). Prognostic factors influencing event-free survival and treatments in desmoid-type fibromatosis: analysis from a large institution, Am. J. Surg. 207. 847-854.
View at Publisher | View at Google Scholar - W.-G. Zeng, Z.-X. Zhou, J.-W. Liang, H.-R. Hou, Z. Wang, et al. (2014). Prognostic factors for desmoid tumor: a surgical series of 233 patients at a single institution, Tumour Biol. J. Int. Soc. Oncodevel. Biol.Med. 35. 7513-7521.
View at Publisher | View at Google Scholar - M.G. Rock, D.J. Pritchard, H.M. Reiman, E.H. Soule, R.C. Brewster, (1984). Extraabdominal desmoid tumors, J. Bone Jt. Surg. Am. 66. 1369-1374.
View at Publisher | View at Google Scholar - Y. Shido, Y. Nishida, H. Nakashima, H. Katagiri, H. Sugiura, et al., Surgical treatment for local control of extremity and trunk desmoid tumors, Arch. Orthop. Trauma Surg. 129. 929-933.
View at Publisher | View at Google Scholar - A. Sørensen, J. Keller, O.S. Nielsen, O.M. Jensen, (2009). Treatment of aggressive fibromatosis: a retrospective study of 72 patients followed for 1-27 years, Acta Orthop. Scand. 73. 213-219.
View at Publisher | View at Google Scholar - A. Hansmann, C. Adolph, T. Vogel, A. Unger, G. Moeslein, (2004). High-dose tamoxifen and sulindac as first-line treatment for desmoid tumors, Cancer. 100. 612-620.
View at Publisher | View at Google Scholar - J. Janinis, M. Patriki, L. Vini, G. Aravantinos, J.S. Whelan, (2003). The pharmacological treatment of aggressive fibromatosis: a systematic review, Ann. Oncol. Off. J. Eur. Soc. Med. Oncol. ESMO. 14. 181-190.
View at Publisher | View at Google Scholar - N. Penel, A. Le Cesne, B.N. Bui, D. Perol, E.G. Brain, et al., (2011). Imatinib for progressive and recurrent aggressive fibromatosis (desmoid tumors): an FNCLCC/French Sarcoma Group phase II trial with a long-term follow-up, Ann. Oncol. Off. J. Eur. Soc. Med. Oncol. ESMO 22. 452-457.
View at Publisher | View at Google Scholar - B. Kasper, P. Str€obel, P. Hohenberger, (2011). Desmoid tumors: clinical features and treatment options for advanced disease, Oncology. 16. 682-693.
View at Publisher | View at Google Scholar - S. Bonvalot, H. Eldweny, V. Haddad, F. Rimareix, G. Missenard, et al. (2008). Extra-abdominal primary fibromatosis: aggressive management could be avoided in a subgroup of patients, Eur. J. Surg. Oncol. J. Eur. Soc. Surg. Oncol. Br. Assoc. Surg. Oncol. 34 462-468.
View at Publisher | View at Google Scholar - N. Eastley, R. Aujla, R. Silk, C.J. Richards, T.A. McCulloch, et al.. (2014). Ashford, Extra-abdominal desmoid fibromatosisea sarcoma unit review of practice, long term recurrence rates and survival, Eur. J. Surg. Oncol. J. Eur. Soc. Surg. Oncol. Br. Assoc. Surg. Oncol. 40. 1125-1130.
View at Publisher | View at Google Scholar - E. Stoeckle, J.M. Coindre, M. Longy, M.B.N. Binh, G. Kantor, et al. (2009). critical analysis of treatment strategies in desmoid tumours: a review of a series of 106 cases, Eur. J. Surg. Oncol. J. Eur.Soc. Surg. Oncol. Br. Assoc. Surg. Oncol. 35. 129-134.
View at Publisher | View at Google Scholar - O. Micke, M.H. Seegenschmiedt, (2005). German cooperative group on radiotherapy for benign diseases, radiation therapy for aggressive fibromatosis (desmoid tumors): results of a national patterns of care study, Int. J. Radiat. Oncol. Biol. Phys. 61. 882-891.
View at Publisher | View at Google Scholar - J.J. Nuyttens, P.F. Rust, C.R. Thomas, A.T. Turrisi, (2000). Surgery versus radiation therapy for patients with aggressive fibromatosis or desmoid tumors: a comparative review of 22 articles, Cancer. 88. 1517-1523.
View at Publisher | View at Google Scholar
