

Research Article | DOI: https://doi.org/10.31579/ 2834-8532/055
Covid-19 Reinfections Clinical-Epidemiological Characteristics Trend Between 2020-2022, 2023 And 2024 In A General Medicine Clinic in Toledo (Spain)
- Jose Luis Turabian *
Health Center Santa Maria de Benquerencia. Regional Health Service of Castilla la Mancha (SESCAM), Toledo, Spain
*Corresponding Author: Jose Luis Turabian, Health Center Santa Maria de Benquerencia. Regional Health Service of Castilla la Mancha (SESCAM), Toledo, Spain.
Citation: Jose Luis Turabian, (2025), Covid-19 Reinfections Clinical-Epidemiological Characteristics Trend Between 2020-2022, 2023 And 2024 In A General Medicine Clinic in Toledo (Spain), Clinical Genetic Research; 4(1): DOI: 10.31579/ 2834-8532/055
Copyright: © 2025 Jose Luis Turabian, this is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited
Received: 02 January 2025 | Accepted: 14 January 2025 | Published: 29 January 2025
Keywords: COVID-19; SARS-CoV-2; reinfection; COVID-19 vaccines; boosters; epidemiological characteristic; secondary analysis; general practice
Abstract
Background
Long-term clinical-epidemiological evolution data on SARS-CoV-2 reinfections cases in community settings are scarce.
Objective
To compare clinical-epidemiological characteristics in cases of covid-19 reinfections during 2020-2022 period, with 2023 and 2024 years in the same population in general medicine.
Methodology
Comparison of secondary data among covid-19 cases in 2020-2022, 2023 and 2024 years of previous studies, all of them carried out in the same population of patients treated in a general medicine office in Toledo, Spain.
Results
Reinfections are mild, infrequent in people over 65 years of age (although with a trend towards greater frequency in 2023 and 2024). There is a tendency to increase the frequency in women (predominant in 2020-2022 and 2024) [p= .002663] and chronic diseases presence (higher in 2020-2022 and especially in 2024) [p= .038334] which by groups tend to decrease in 2024 except Musculoskeletal, Nervous and Senses and Digestive system which increase strongly. The frequency of Health Care Workers with reinfections was high, with a peak in 2023 [p= .000978]. 67% of reinfections in 2024 had only 1 , 2 or 3 doses of vaccine. There were no differences between the frequencies of symptoms, but general symptoms always predominated, with a tendency to increase.
Conclusions
The trend of reinfections shows that they are mild, in women, in people under 65 years of age, with chronic diseases, and in healthcare workers. There are no differences between the symptoms, with general symptoms always predominating and tending to increase. Booster doses can be modestly reduce the risk of reinfection.
Introduction
Reinfections with severe acute respiratory syndrome coronavirus (SARS-CoV-2) were rare until late 2021 but became common with the arrival of omicron (1, 2). Reinfections with SARS-CoV-2 are an important aspect of coronavirus disease 2019 (covid-19) and its potential transition to endemicity (3-5). It is currently accepted that it may be normal to be infected by SARS-CoV-2 several times throughout life (6-10).
Furthermore, compared with the absence of reinfection, reinfection appears to contribute to additional risks of death, hospitalization, and sequelae, including pulmonary, cardiovascular, hematologic, diabetes, gastrointestinal, renal, mental health, musculoskeletal, and neurologic disorders. The risks appear to remain evident regardless of vaccination status (11). It has been estimated that after 4-6 months of a first episode of covid-19 or having been vaccinated (or both, (hybrid immunity), a new SARS-CoV-2 infection is expected to be associated with a higher risk of hospitalization and death in the most fragile population (12).
But for many people who get Covid-19 multiple times, subsequent infections will be as mild as the first or more, data show, likely due to partial immunity from previous infections, vaccination, and the fact that the latest circulating variants often cause less severe symptoms (13).
Given the current situation in many places, such as Spain, of not performing diagnostic tests in health services, except for those over 60 years of age and healthcare workers (14), many people with symptoms choose to test at home and the trend of reinfection rate over time is not clear (2). However, estimates of the burden of SARS-CoV-2 reinfections remain crucial to assess new variants with immune escape potential (15) and to help guide public health measures and vaccination strategies (2, 16).
In this context, we present a comparative study based on previously published data, to evaluate the clinical-epidemiological characteristics of reinfections covid-19 cases in the period 2020-2022 (in 2020 without vaccination, in 2021 with 1 or 2 dose vaccination and in 2022 with first booster), in 2023 (with second booster), and 2024 (with third booster), from the same population attended in a general medicine consultation in these time periods.
Material And Methods
Design and emplacement
This study compares data from previous observational, longitudinal and prospective studies of covid-19 reinfections from March, 2020 to October, 2024, already published (17-21). All studies were conducted on the same population: patients saw in a general medicine office in Toledo, Spain, which has a list of 2,000 patients > 14 years of age (in Spain, general practitioner (GP) care for people > 14 years of age, except for exceptions). The GPs in Spain work within the National Health System, which is public in nature, and are the gateway for all patients to the system, and each person is assigned a GP. The methodology of all studies has been previously published and here only the main elements will be repeated for the current study.
Outcome of interest
To know and describe a set of selected clinical-epidemiological characteristics of cases of covid-19 reinfection from 2020-2022 period, in 2023 and 2024, at primary health care level.
Definition of reinfection
SARS-CoV-2 reinfection was defined as a documented infection occurring at least 90 days after a previous infection (22, 23).
Diagnosis of covid-19
The diagnosis was performed with reverse transcriptase polymerase chain reaction oropharyngeal swab tests or antigen testing (24) performed in health services or at home.
Covid-19 vaccination
Patients could have received 1, 2 doses of vaccine, first booster for fall-winter 2021, fourth dose (second booster) for fall-winter 2022 and fifth dose (third booster) for fall-winter 2023. In our study, only Pizfer / BioNTech, Spikevax (mRNA-1273- Moderna), Vaxzevria, Oxford / AstraZeneca and Janssen (Johnson & Johnson) vaccines were used for the first and second doses. For the first booster, only messenger RNA (mRNA) was used. And only Moderna and Pfizer-BioNTech's bivalent covid-19 vaccines were used for the second booster. The omicron-adapted vaccines XBB.1.5 Pizfer / BioNTech and Spikevax (Moderna) were used for the third booster in autumn-winter 2023 (25-28).
Collected variables
The following variables were collected:
-Age and sex
-Chronic diseases (defined as "any alteration or deviation from normal that has one or more of the following characteristics: is permanent, leaves residual impairment, is caused by a non-reversible pathological alteration, requires special training of the patient for rehabilitation, and / or can be expected to require a long period of control, observation or treatment” (29) and symptoms covid-19 infection, both classified according to the International Statistical Classification of Diseases and Health-Related Problems, CD-10 Version: 2019 (30)
-Social-occupancy class (according to the Registrar General's classification of occupations and social status code) (31, 32)
-If they were Health Care Workers
-Problems in the family context based on the genogram. It was understood that "complex" genograms present families with psychosocial problems) (33-35)
-Ethnic minority (defined as a “human group with cultural, linguistic, racial values and geographical origin, numerically inferior compared to the majority group”) (36)
-Disease severity (classified according to: 1. mild cases: clinical symptoms are mild and no manifestation of pneumonia can be found on images; 2. moderate cases: with symptoms such as fever and respiratory tract symptoms and the manifestation of pneumonia can be seen on the imaging tests; and 3. severe cases: respiratory distress, respiratory rate ≥ 30 breaths / min., pulse oxygen saturation ≤ 93% with room air at rest, arterial partial pressure of oxygen / oxygen concentration ≤ 300 mmHg.) (37); to simplify comparison, moderate and severe cases were counted together
-Vaccination status against covid-19 at the date of reinfection: vaccinated with 2 doses of vaccine (24), vaccinated with first booster for fall-winter 2021 (38), vaccinated with fourth dose (second booster) for fall-winter 2022 (39) and vaccinated with fifth dose (third booster) for fall-winter 2023 (40, 41)
Statistical analysis
The comparisons were performed using the Chi Square test (X2) or test of Kruskal-Wallis, when necessary, both with degrees freedom (df)= 2 [df= (número de filas-1) x (número de columnas-1)]
Ethical issues
No personal data of the patients were used, but only group results, which were taken from the clinical history.
Results
Reinfections are mild throughout the period (Not significant at p < .05 [NS]), relatively rare in those over 65 years of age (although with a tendency towards greater frequency in 2023 and 2024 versus the 2020-2022 period) [NS]. There is a tendency towards increasing frequency in women (predominant in 2020-2022 and 2024) [X2 (df = 2) = 11.8565. p = .002663. Significant at p < .05.] and chronic diseases presence (higher in 2020-2022 and especially in 2024) [X2 (df = 2) = 6.5228. p = .038334. Significant at p < .05.], with no statistically significant differences between the frequencies of chronic diseases according to WHO, ICD-10 groups, but all groups tend to decrease in 2024 except Musculo-skeletal, Nervous and Senses and Digestive system which increase strongly. The frequency of Health Care Workers with reinfections was non-negligible throughout the period with a peak in 2023 [X2(df=2)= 13.8594. p= .000978. Significant at p < .05. ]. The frequency of Complex family in reinfections was higher in 2023 [NS]. 67% of reinfections in 2024 had only 1, 2 or 3 doses of vaccine (TABLE 1, TABLE 2, FIGURE 1, FIGURE 2). There were no statistically significant differences between the frequencies of symptoms according to WHO, ICD-10 groups, but general symptoms always predominated, with a tendency to increase; respiratory and ENT symptoms were in second place in frequency and with a tendency to decrease; the rest, Neurological, Digestive, Psychiatric, Skin, Genitourinary, with marginal figures throughout the period (TABLE 3, FIGURE 3).
Variables | Reinfections From March 1, 2020 To September 30, 2022 N=38 | Reinfections From October 1, 2022 To September 30, 2023 N=12 | Reinfections From October 1, 2023 To September 30, 2024 N=15 | Statistical significance |
> = 65 years | 3 (8) | 4 (33) | 4 (27) | X2 (df=2) = 5.5146. p= .063464. NS |
Women | 30 (79) | 3 (25) | 10 (67) | X2 (df=2) = 11.8565. p= .002663. Significant at p < .05. |
Health Care Workers | 7 (18) | 9 (75) | 4 (27) | X2(df=2) = 13.8594. p= .000978. Significant at p < .05. |
Moderate-severe severity of reinfection | 0 | 3 (25) | 0 | Kruskal-Wallis (df=2): H=2.7. p = .259. NS |
Chronic diseases | 25 (66) | 4 (33) | 12 (80) | X2 (df=2) = 6.5228. p= .038334. Significant at p < .05. |
Social-occupancy class of patients (people with some type of labor specialization) | 16 (42) | 1 (8) | 4 (27) | X2 (df=2) =5.0399. P= .080462. NS |
Complex family/ Problems in the family context | 3 (8) | 7 (58) | 2 (13) | X2 (df=2) =15.7538. P= .000379. Significant at p < .05. |
Ethnic minority | 5 (13) | 1 (8) | 1 (7) | X2 (df=2) = 0.5625. p= .754858. NS |
1, 2 ó 3 dose | 38 (100) | 7 (6) | 10 (67) | NR |
4 dose | NR | 5 (42) | 1 (7) | NR |
5 dose | NR | NR | 4 (27) | NR |
Table: Comparison Of Selected Variables Of Covid-19 Reinfections In 2020-2022, 2023 And 2024
(): Denotes percentages; NS: Not significant at p< .05; df= Degrees freedom; NR: Not relevant
Chronic diseases* | Reinfections From March 1, 2020 To September 30, 2022 N=38 | Reinfections From October 1, 2022 To September 30, 2023 N=12 | Reinfections From October 1, 2023 To September 30, 2024 N=15 | Statistical significance |
-I Infectious | 0 | 0 | 0 | Kruskal-Wallis (df=2): H= 0.11. p = .949. NS |
-II Neoplasms | 1 (2) | 2 (8) | 2 (5) | X2 (df=2)= 2.4474. p= .294134. NS |
-III Diseases of the blood | 0 | 0 | 0 | Kruskal-Wallis (df=2): H= 0.11. p = .949. NS |
-IV Endocrine | 11 (15) | 5 (19) | 5 (13) | X2 (df=2) = 0.4913. p= .782214. NS |
-V Mental | 5 (7) | 3 (12) | 4 (10) | X2 (df=2) = 0.6178. p= .734266. NS |
-VI-VIII Nervous and Senses | 6 (8) | 1 (4) | 7 (18) | X2 (df=2) = 3.9064. p= .141817. NS |
-IX Circulatory system | 7 (10) | 3 (12) | 3 (8) | X2 (df=2) = 0.2824. p= .8683. NS |
-X Respiratory system | 11 (16) | 2 (8) | 1 (3) | X2 (df=2) = 4.7922. p= .091071. NS |
-XI Digestive system | 6 (8) | 1 (4) | 4 (10) | X2 (df=2) = 0.8885. p= .641293. NS |
-XII Diseases of the skin | 3 (4) | 3 (11) | 0 | Kruskal-Wallis (df=2): H= 0.51. p = .773. NS |
-XIII Musculo-skeletal | 9 (13) | 3 (11) | 9 (23) | X2 (df=2) = 2.4606. p= .292208. |
-XIV Genitourinary | 12 (17) | 3 (11) | 4 (10) | X2 (df=2) = 1.083. p= .581866. |
TOTAL, chronic diseases* | 71 (100) | 26 (100) | 39 (100) | --- |
Table 2: Comparison Of Chronic Diseases Of Covid-19 Reinfections In 2020-2022, 2023 And 2024
(): Denotes percentages; NS: Not significant; df= Degree’s freedom; *Patients could have more than one chronic disease. The percentages of chronic diseases are over the total of chronic diseases of symptomatic and asymptomatic patients
Symptoms covid-19 reinfection* According to who, Icd-10 groups | Reinfections from march 1, 2020 to september 1, 2022 N=38 | Reinfections from october 1, 2022 to september 30, 2023 N=12 | Reinfections from october 1, 2023 to september 30, 2024 N=15 | Statistical Significance |
General (discomfort, asthenia, myalgia, fever, artralgias) | 42 (40) | 11 (31) | 29 (54) | X2 (df=2) = 4.8005. p= .090696. NS |
Respiratory (cough, dyspnea, chest pain) | 29 (27) | 10 (29) | 13(24) | X2 (df=2) = 0.2964. p= .862259. NS |
ENT (anosmia / ageusia, odynophagia, rhinorrhea, pharyngeal dryness-mucus, epixtasis) | 25 (24) | 10 (29) | 8 (15) | X2 (df=2) = 2.6883. p= .260767. NS |
Digestive (anorexia, nausea / vomiting, diarrhea, abdominal pain) | 3 (3) | 0 | 1 (2) | Kruskal-Wallis (df=2): H= 1.14. p = .565. NS |
Neurological (headache, dizziness, mental confusion -brain fog) | 7 (6) | 4 (11) | 3 (5) | X2 (df=2) = 1.1973. p= .549557. NS |
Psychiatric (anxiety, insomnia) | 0 | 0 | 0 | Kruskal-Wallis (df=2): H=0.32. P = .851. NS |
Skin (chilblains, flictenas, rash) | 0 | 0 | 0 | Kruskal-Wallis (df=2): H= 0.32. p = .851. NS |
Genitourinary | 0 | 0 | 0 | Kruskal-Wallis (df=2): H= 0.32. p = .851. NS |
Total, symptoms* | 105 (100) | 35 (100) | 54 (100) | --- |
Table 3: Comparison Of Covid-19 Reinfection Symptoms In 2020-2022, 2023 And 2024
( ): Denotes percentages; NS: Not significant; df= Degree’s freedom; * Patients could have more than one symptom. The percentages are over the total of symptoms
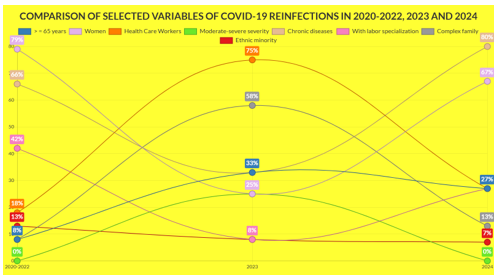
Figure 1: Comparison Of Selected Variables of Covid-19 Reinfections In 2020-2022, 2023 And 2024
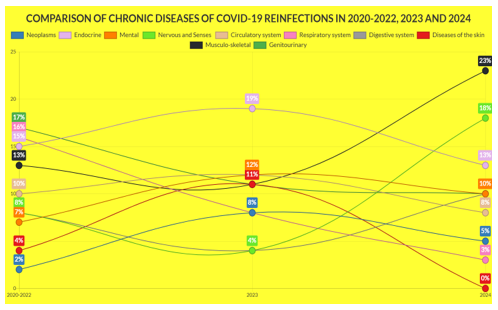
Figure 2: Comparison Of Chronic Diseases Of Covid-19 Reinfections In 2020-2022, 2023 And 2024
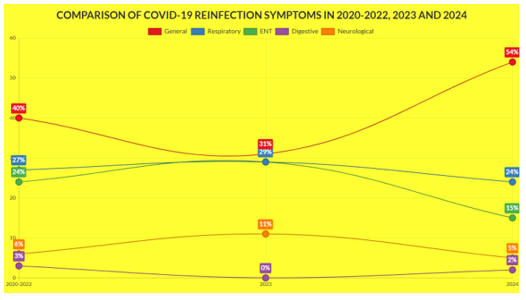
Figure 3: Comparison Of Covid-19 Reinfection Symptoms In 2020-2022, 2023 And 2024
Discussion
1. Main findings
Our main findings were:
1. Covid-19 reinfectons frequently had mild symptoms.
2. They were more frequent in women.
3. Most had chronic diseases, but not the classic comorbidities of the Circulatory system or Respiratory.
4. There is a considerable frequency of reinfections in social-health workers, possibly because they are more exposed and undergo diagnostic testing more frequently.
5. Booster doses can modestly reduce the risk of reinfection.
Three fundamental factors must be taken into account to correctly evaluate our data: the local evolution of SARS-CoV variants, local degree of vaccination, and degree of diagnostic testing when there are symptoms.
a) The predominant variants in Spain during 2023 were those of the XBB family (41-46). In January 2024 in Spain, XBB.1.5-like + F456L accounted for 42% and BA.2.86 for 44% of positive cases (23). In July and August 2024, the KP.3 lineage was detected in 84% of cases (47). In September 2024, the incidence of the XEC variant of the coronavirus, a new omicron subvariant was increasing markedly in Spain. At that time, it was the second most common strain in cases recorded in September, although still far behind the main KP.3.3, with an incidence of 13% (48, 49)
b) On the other hand, in Spain, in November 2022, more than 60% of people over 80 years of age, and 37% of people over 60 years of age, already had the second booster dose of the covid-19 vaccine (50, 51). And 60% of the population over 80 years of age has already received the vaccine adapted against the covid-19 subvariants of the 2023/2024 campaign (52).
c) In any case, the results must be evaluated with caution. In Spain, since April 28, 2022 there was a new "Surveillance and Control Strategy Against Covid-19" that included the non-performance of diagnostic tests, which were focused only on those over 60 years of age (14). This means that positive cases have been counted with tests carried out in health services and with tests carried out at home and later reported to the GP. Thus, there is probably an underreporting. In addition, it is possible that many of the current infections are occurring with few symptoms or are confusing them with those of other mild conditions (43).
2. Comparison with other studies
Five years after the pandemic began, new SARS-CoV-2 infections continue to occur despite advances in vaccines (53). It has been reported that SARS-CoV-2 reinfections, commonly defined by a positive test ≥90 days after the previous episode, were rare until late 2021, but became common with the arrival of omicron; reinfections are mostly mild and hospitalizations are rare (1, 2, 13, 16). Our results are consistent with those findings, not including any severe or hospitalized cases. However, the frequency of cases with chronic diseases tends to increase in 2024, which is an indicator of risk. Moreover, at the population level, its transmissibility more than compensates for any reduction in disease severity or symptoms experienced by the individual (54).
The SARS-CoV-2 human host in 2023/2024 is different from those in 2020 in their vaccination status. Vaccines have been shown to be effective in reducing the severity of SARS-CoV-2 infection (55-57). While it is true that the efficacy of prior SARS-CoV-2 infection in preventing reinfection varies along the spectrum encompassing alpha, beta, delta, and omicron, it is also necessary to draw attention to the role of mutability in the SARS-CoV-2 variant subtypes responsible for prior infection (58). There is increasing scientific evidence that shows that the protection generated by vaccination decreases over time. In addition, the decrease in immunity as a result of the new variants must be taken into account. Although it is reestablished with the inoculation of booster doses (59, 60), the protection conferred by natural immunity, vaccination, and both against SARS-CoV-2 infection with the omicron variant is unclear (23, 61-62).
Unvaccinated and 1- or 2-dose vaccinated individuals have been reported to be slightly more likely to be reinfected compared with individuals who received a third (booster) vaccine dose, i.e., booster doses may modestly reduce the risk of reinfection (16). Likewise, regimens that included a booster dose, compared with no vaccination, offered protection against symptomatic omicron infection (63). These results are replicated in our study, with 67% of reinfections in 2024 having only 1, 2, or 3 vaccine doses.
A higher likelihood of reinfection has been reported for 2021 among younger adults, women, and HCWs; healthcare occupations are among the highest risk for covid-19 infection, possibly due to increased risk of exposure (64, 65). However, in our study, we cannot exclude the possibility that some of these population groups may also have been subjected to more intensive testing than others (16). Factors associated with the excess risk for reinfection in women need further investigation, but may be due to increased home testing (66-68).
In summary, we know that natural immunity is not sufficient against infection with omicron, and that vaccine immunity is also not sufficient to prevent reinfection, although it appears that booster doses may modestly reduce the risk of reinfection.
Limitations and strengths of the study
1. The samples were small, so some data may cause misinterpretation.
2.-Genetic sequencing was not performed.
3.-It must be taken into account that the results may not be applicable to other vaccination regimens different from those of the study
4. Asymptomatic cases were missing because they did not attend in GP consultation, as no surveillance or systematic screening was done. Thus, the number of reinfections has probably been underestimated
5. There may be an underreporting of infections to GP of patients with a positive test at home. But given the situation of the GP as the gateway to the health system, the vast majority of positive covid-19 tests at home, is likely to be reported in GP office.
6. The study has the strength of its longitudinality, characteristic of work in general medicine.
Conclusion
In the context of general medicine in Toledo (Spain), from 2020 to 2024, the trend of reinfections shows that they are mild, relatively rare in people over 65 years of age, most frequent in women, with chronic diseases (with a tendency to increase the frequency of Musculoskeletal, Nervous and Senses and Digestive system), with a non-negligible frequency in social-health workers, and without statistically significant differences between symptoms, with general symptoms always predominating and tending to increase, while respiratory and ENT symptoms are in second place in frequency and tending to decrease. Booster doses can modestly reduce the risk of reinfection.
References
- Zoco M, Jetelina K (2022) Epidemiología de las reinfecciones. Su Epidemiólogo Local; Jul 08.
View at Publisher | View at Google Scholar - Chen Y, Zhu W, ¿Han X, et al. (2024) How does the SARS-CoV-2 reinfection rate change over time? The global evidence from systematic review and meta-analysis. BMC Infect Dis; 24(1): 339.
View at Publisher | View at Google Scholar - European Centre for Disease Prevention and Control (2020) Reinfection with SARSCoV-2: considerations for public health response. ECDC; 21 September.
View at Publisher | View at Google Scholar - Yahav D, Yelin D, Eckerle I, et al. (2021) Definitions for coronavirus disease 2019 reinfection, relapse and PCR re-positivity. Clin Microbiol Infect; 27: 315-8.
View at Publisher | View at Google Scholar - Pilz S, Theiler-Schwetz V, Trummer C, et al. (2022) SARS-CoV-2 reinfections: overview of efficacy and duration of natural and hybrid immunity. Environ Res; 209, 112911.
View at Publisher | View at Google Scholar - Crist C (2021) Unvaccinated People Likely to Catch COVID Repeatedly. Medscape; Oct 25.
View at Publisher | View at Google Scholar - Kojima N, Klausner JD (2021) Protective immunity after recovery from infection. Lancet Infect Dis; 22(1): 12-4.
View at Publisher | View at Google Scholar - Goldberg Y, Mandel M, Bar-On YM, et al. (2022) Protection and Waning of Natural and Hybrid Immunity to SARS-CoV-2. N Engld J Med; 386:2201-12.
View at Publisher | View at Google Scholar - Williams S (2020) Cold-Causing Coronaviruses Don’t Seem to Confer Lasting Immunity. The Scientist; Aug 18.
View at Publisher | View at Google Scholar - Johnston C, Hughes H, Lingard S, Hailey S, Healy B (2022) Immunity and infectivity in covid-19. BMJ; 378: 061402.
View at Publisher | View at Google Scholar - Bowe B, Xie Y, Al-Aly Z (2022) Acute and postacute sequelae associated with SARS-CoV-2 reinfection. Nat Med; 28: 2398–405.
View at Publisher | View at Google Scholar - Soriano V (2022) COVID de repetición: ¿peor que la primera vez? Blog; 14/11.
View at Publisher | View at Google Scholar - Blum D (2023) How Bad Is a Second (or Third or Fourth) Case of Covid? The New York Times; 17 ago. https://www.nytimes.com/2023/08/17/well/live/covid-reinfection.html
View at Publisher | View at Google Scholar - Turabian JL (2022) An ostrich strategy for covid-19 is too risky. BMJ; 377: o1112.
View at Publisher | View at Google Scholar - Planas D, Saunders N, Maes P, et al. (2022) Considerable escape of SARS-CoV-2 Omicron to antibody neutralization. Nature; 602: 671-5.
View at Publisher | View at Google Scholar - Medić S, Anastassopoulou C, Lozanov-Crvenković Z, et al. (2022) Risk and severity of SARS-CoV-2 reinfections during 2020–2022 in Vojvodina, Serbia: A population-level observational study. Lancet Regional Health – Europe; 20.
View at Publisher | View at Google Scholar - Turabian JL (2022) Does the Booster Vaccination Provide Advantages to Prevent Reinfection Over 1 or 2 Doses of COVID–19 Vaccine? Medp Public Health Epidemiol. 2022; 1(1): mpphe–202209003.
View at Publisher | View at Google Scholar - Turabian JL (2024) Reinfections of Covid-19 with and Without Fourth Dose of Bivalent mRNA Vaccine in the Period from October 2022 to October 2023 in a General Medicine Office in Toledo (Spain). J Dise Dis Tre; SRC/JDDT-129.
View at Publisher | View at Google Scholar - Turabian JL (2024) What are the risk factors of covid-19 reinfection in people with 4th dose of bivalent mrna vaccines? A study in general medicine from october 2022 to october 2023. International Journal of Clinical Epidemiology; 3(3).
View at Publisher | View at Google Scholar - Turabian JL (2024) What are the Clinical-Epidemiological Differences between Initial Infection and Reinfection Covid-19 with Fourth Dose of Bivalent mRNA Vaccine? A Study in the Period from October 2022 to October 2023, In a General Medicine Office (Toledo, Spain). J Inf Dis Trav Med; 8(1): 000183.
View at Publisher | View at Google Scholar - Turabian JL (2024) Covid-19 reinfections case series from October 2023 to October 2024 in a general medicine office in toledo (Spain). Epidemiology International Journal, In Press.
View at Publisher | View at Google Scholar - Slezak J, Bruxvoort K, Fischer H, Broder B, Ackerson B, Tartof S (2021) Rate and severity of suspected SARS-Cov-2 reinfection in a cohort of PCR-positive COVID-19 patients. Clin Microbiol Infect; 27(12): 1860.E7-E10.
View at Publisher | View at Google Scholar - Altarawneh HN, Chemaitelly H, Ayoub Hh, et al. (2022) Effects of Previous Infection and Vaccination on Symptomatic Omicron Infections. N Engl J Med; 387: 21-34.
View at Publisher | View at Google Scholar - Ministerio de Sanidad (2021) [COVID-19 early detection, surveillance and control strategy. Updated December 1].
View at Publisher | View at Google Scholar - Consejo Interterritorial de Salud (2022) [COMIRNATY BIVALENTE, Original/Omicron BA.4-5 (COVID-19 mRNA Vaccine, Pfizer-BioNTech) Technical Guide December 27, 2022].
View at Publisher | View at Google Scholar - Consejo Interterritorial de Salud (2023) [BIVALENT SPIKEVAX, Original/Omicron BA.1 and Original/Omicron BA.4-5 (Modern COVID-19 mRNA Vaccine) Technical Guide January 23, 2023].
View at Publisher | View at Google Scholar - Lin D-Y, Xu Y, Gu Y, et al. (2023) Effectiveness of Bivalent Boosters against Severe Omicron Infection. N Engl J Med; 388: 764-6.
View at Publisher | View at Google Scholar - Consejo Interterritorial (2022) [Update of the vaccination recommendations against COVID-19 for autumn-winter in Spain Approved by the Public Health Commission on December 15, 2022. Prepared by the Report on the Vaccination Program and Registry]. Sistema Nacional de Salud. España.
View at Publisher | View at Google Scholar - Strauss AL (1984) Chronic illness and the quality of life. St Louis: The C.V. Mosby Company.
View at Publisher | View at Google Scholar - 30.-WHO (2024) International Statistical Classification of Diseases and Health-Related Problems. ICD-10 Version: 2019.
View at Publisher | View at Google Scholar - Royal Collage of General Practitioners (1986) The Classification and Analysis of General Practice Data. Occasional Paper 26.
View at Publisher | View at Google Scholar - Donaldson RJ, Donaldson LJ (1983) Essential Community Medicine. Lancaster: MTP Press.
View at Publisher | View at Google Scholar - Turabian JL (2017) Family Genogram in General Medicine: A Soft Technology that can be Strong. An Update. Res Med Eng Sci; 3(1).
View at Publisher | View at Google Scholar - Russell LT (2020) Capturing Family Complexity in Family Nursing Research and Practice. J Fam Nurs; 26(4): 287-93.
View at Publisher | View at Google Scholar - Watts C, Shrader E (1998) How to do (or not to do). The genogram: a new research tool to document patterns of decision-making, conflict and vulnerability within households. Health Policy Plan; 13: 459-64.
View at Publisher | View at Google Scholar - Diccionario panhispánico del español jurídico (2022) [Ethnic minority].
View at Publisher | View at Google Scholar - Mao S, Huang T, Yuan H, et al. (2020) Epidemiological analysis of 67 local COVID-19 clusters in Sichuan Province, China. BMC Public Health; 20: 1525.
View at Publisher | View at Google Scholar - [Update 10 Vaccination strategy against COVID-19 in Spain. Recommendations agreed upon in the Public Health Commission after review and proposal made by the Vaccination Program and Registry Report together with the COVID-19 Vaccination Technical Working Group and the COVID-19 Vaccination Working Group in the Child Population December 2021].
View at Publisher | View at Google Scholar - Consejo Interterritorial (2022) [COVID-19 vaccination recommendations for autumn in Spain. Approved by the Public Health Commission on 22 September 2022. Prepared by the Vaccination Programme and Registry Committee]. Sistema Nacional de Salud. España.
View at Publisher | View at Google Scholar - 40.-Grupo de Trabajo sobre Vacunaciones de la Sociedad Española de Epidemiología (2023) [COVID-19 AND FLU VACCINATION GUIDE, AUTUMN 2023]. Sociedad Española de Epidemiología. https://seepidemiologia.es/wp-content/uploads/2023/09/Guia-recomendaciones-vacunacion-covid-gripe.pdf
View at Publisher | View at Google Scholar - Rodríguez-Artalejo FJ, Ruiz-Galiana J, Cantón R, et al. (2023) COVID-19: On the threshold of the fifth year. The situation in Spain. Rev Esp Quimioter; 37(1): 17-28.
View at Publisher | View at Google Scholar - Centro de Coordinación de Alertas y Emergencias Sanitarias (2023) [May 22, 2023 Update on the epidemiological situation of SARS-CoV-2 variants in Spain]. Ministry of Health. Spain.
View at Publisher | View at Google Scholar - Viciosa M (2023) [If you have covid today, the new variant O EG.5 or 'Eris' may have something to do with it (and it is not more serious)]. Newtral; 11 agosto.
View at Publisher | View at Google Scholar - Pérez B (2023) [The new eris variant, more contagious, already alerts doctors to the rebound in covid]. El Periódico; 10 de agosto.
View at Publisher | View at Google Scholar - Looi M (2023) Covid-19: Hospital admissions rise in England amid fears of new variant and waning immunity. BMJ; 382: p1833.
View at Publisher | View at Google Scholar - Smith DG (2023) What to Know About the New Dominant Covid Variant. EG.5 is spreading quickly, but experts say it’s no more dangerous than previous versions. Another new variant, called BA.2.86, is being closely watched because of its mutations. The New York Times; Aug. 11.
View at Publisher | View at Google Scholar - [WEEKLY EPIDEMIOLOGICAL REPORT COMMUNITY OF MADRID. Week 40] (2024). SG de Vigilancia en Salud Pública. Dirección General de Salud Pública CONSEJERÍA DE SANIDAD – COMUNIDAD DE MADRID. 8 de Octubre.
View at Publisher | View at Google Scholar - AM (2024) [XEC Covid variant: this is the new strain that is spreading across Europe and what its symptoms are]. Onda Cero; Madrid; 09.10. https://www.ondacero.es/noticias/salud/variante-xec-covid-asi-nueva-cepa-que-extiende-europa-cuales-son-sus-sintomas_20241009670664b4077ed10001ea6bc1.html
View at Publisher | View at Google Scholar - Córdoba Jiménez P (2024) [XEC: New COVID variant threatens Europe, leaving 1,115 cases worldwide]. Gaceta Médica; 10 octubre.
View at Publisher | View at Google Scholar - Vacuna Covid-19 (2021) [Covid-19 vaccination strategy in Spain]. Ministerio de sanidad.
View at Publisher | View at Google Scholar - Notas de Prensa (2022) [More than 60% of people over 80 years of age now have a second booster dose against COVID-19]. Ministerio de Sanidad. España; 11.11.
View at Publisher | View at Google Scholar - Noticias (2023) [60% of the population over 80 years old has already been vaccinated against Covid 19 in 2023]. Ministerio de Sanidad, Gobierno de España; 15 de diciembre.
View at Publisher | View at Google Scholar - World Health Organization (2024) COVID-19 epidemiological update. No. 168. June 17, 2024. https://www.who.int/publications/m/item/covid-19-epidemiological-update-edition-168).
View at Publisher | View at Google Scholar - Wise J (2022) Covid-19: Omicron sub variants driving new wave of infections in UK. BMJ; 377: o1506 doi:10.1136/bmj. o1506.
View at Publisher | View at Google Scholar - Dagan N, Barda N (2021) BNT162b2 mRNA Covid-19 Vaccine in a Nationwide Mass Vaccination Setting. N Engl J Med; 384(15): 1412–23.
View at Publisher | View at Google Scholar - Grange Z, Buelo A, Sullivan C, et al. (2021) Characteristics and risk of COVID-19-related death in fully vaccinated people in Scotland. Lancet; 398(10313): 1799-800.
View at Publisher | View at Google Scholar - Mayor SJ, Welte T (2023) From Pandemic to Endemic: How Do Influenza and SARS-CoV-2 Compare? Medscape CME & EDUCATION.
View at Publisher | View at Google Scholar - Jolobe OMP (2022) Protection Due to Previous SARS-CoV-2 Infection. N Engl J Med.
View at Publisher | View at Google Scholar - Pérez-Cortés Villalobos A (2021) [A new disease that we must know: COVID-19 after being vaccinated]. Medscape; 28 de sep.
View at Publisher | View at Google Scholar - Feikin DR, Higdon MM, Abu-Raddad LJ, et al. (2022) Duration of effectiveness of vaccines against SARS-CoV-2 infection and COVID-19 disease: results of a systematic review and meta-regression. Lancet; 399(10328): 924-44.
View at Publisher | View at Google Scholar - Wise J (2022) Covid-19: Omicron infection is poor booster to immunity, study finds. BMJ; 377: o1474 doi:10.1136/bmj. o147.
View at Publisher | View at Google Scholar - Hachmann NP, Miller J, Collier AY, et al. (2022) Neutralization Escape by SARS-CoV-2 Omicron Subvariants BA.2.12.1, BA.4, and BA.5. N Engl J Med; 387:86-8.
View at Publisher | View at Google Scholar - Accorsi EK, Britton A, Shang N, et al. (2022) Effectiveness of Homologous and Heterologous Covid-19 Boosters against Omicron. N Engl J Med; 386:2433-5.
View at Publisher | View at Google Scholar - Dhumal S, Patil A, More A, et al. (2022) SARS-COV-2 reinfection after previous infection and vaccine breakthrough infection through the second wave of pandemic in india: An observational study. IJID; 118: 95 – 103.
View at Publisher | View at Google Scholar - Romero Starke K, Mauer R, Hegewald J, et al. (2024) Occupational risks of COVID-19: a case-cohort study using health insurance claims data in Germany. BMC Public Health; 24: 3235.
View at Publisher | View at Google Scholar - Turabian JL (2024) Covid-19 Infections with Positive Test at Home Versus in Health Services, In the Period from October 2022 to October 2023, In the General Medicine Office, In Toledo (Spain). J General Medicine and Clinical Practice; 7(8).
View at Publisher | View at Google Scholar - Slezak J, Bruxvoort K, Fischer H, Broder B, Ackerson B, Tartof S (2021) Rate and severity of suspected SARS-Cov-2 reinfection in a cohort of PCR-positive COVID-19 patients. Clin Microbiol Infect; 27(12): 1860.e7-1860.e10.
View at Publisher | View at Google Scholar - Peghin M, Bouza E, Fabris M, et al. (2021) Low risk of reinfections and relation with serological response after recovery from the first wave of COVID-19. Eur J Clin Microbiol Infect Dis; 40, 2597–604.
View at Publisher | View at Google Scholar
