

Review Article | DOI: https://doi.org/10.31579/2834-8486/001
Considerations and Analysis of the Implementation of Oncogeriatrics in Chile and Its Importance
- Macarena Honorato 1
- Oscar Calderón 1,2
- Verónica Rojas 1
- Gerardo Fasce 3,4
- Constanza Bartolotti 5,6
- Christian Caglevic 7*
1 Geriatrics Department, Clínica Alemana de Santiago, Santiago, Chile.
2 Geriatrics, Complejo Asistencial Dr. Sótero del Río, Santiago, Chile
3 Geriatrics Service, Department of Medicine, Hospital Clínico Universidad de Chile, Santiago, Chile
4 Geriatrics Service, Department of Medicine, Clínica Las Condes, Santiago, Chile
5 Geriatrics, Internal Medicine Department, Universidad de la Frontera, Temuco, Chile
6 Geriatrics, Centro Comunitario Kiműnche, Temuco, Chile
7 Cancer Research Department, Instituto Oncológico Fundación Arturo López Pérez, Santiago, Chile.
*Corresponding Author: Christian Caglevic, Cancer Research Department, Instituto Oncológico Fundación Arturo López Pérez, Santiago, Chile.
Citation: Honorato M., Calderón O, Rojas V., Fasce G, Bartolotti C. , Caglevic C. (2022). Sepsis: Considerations and Analysis of the Implementation of Oncogeriatrics in Chile and Its Importance. Biomedical and Clinical Research. 1(1); DOI:10.31579/2834-8486/001
Copyright: © 2022 Christian Caglevic, This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 08 September 2022 | Accepted: 13 September 2022 | Published: 23 September 2022
Keywords: oncogeriatrics; geriatrics cancer and elderly; cancer in chile
Abstract
The Chilean census of 2017 reported that 11.4% of the local population are 65 years or older, and according to the National Institute of Statistics (INE) by 2025 20% of the Chilean population will be in this group.
Cancer in Chile is a major public health problem. Aging is a significant risk factor for cancer development which added to the improved life expectancy, it increases the incidence of cancer. In 2040, new cancer cases will increase from 19.3 to 30.2 million worldwide.
Older people are a heterogeneous group requiring specialized and individualized management. Chronological age does not necessarily correlate with physiological age. More than half of the geriatric patients with cancer have at least one comorbidity which is relevant when defining a cancer treatment. Likewise, polypharmacy is frequent and is an important issue to consider in people with cancer due to the risk associated with drug interactions.
Oncogeriatric assessment consists of a comprehensive multidimensional evaluation, including functional and biopsychosocial issues, addressing aspects of the neoplastic disease such as the risk of toxicities due to systemic therapy and life expectancy. This tool has proven to be helpful in the diagnosis of conditions that are not evident in a routine oncological evaluation, such as geriatric syndromes, frailty, functional dependence, and cognitive impairment among others, which have an impact when deciding on therapy, predicting risks of treatment toxicity and mortality.
Introduction
The Chilean census of 2017 reported that 11.4% of the local population are 65 years or older, and according to the National Institute of Statistics (INE) by 2025 20% of the Chilean population will be in this group [1].
Cancer in Chile is a major public health problem. Aging is a significant risk factor for cancer development [2] which added to the improved life expectancy, it increases the incidence of cancer. In 2040, new cancer cases will increase from 19.3 to 30.2 million worldwide [3].
Older people are a heterogeneous group requiring specialized and individualized management. Chronological age does not necessarily correlate with physiological age. More than half of the geriatric patients with cancer have at least one comorbidity which is relevant when defining a cancer treatment [4]. Likewise, polypharmacy is frequent and is an important issue to consider in people with cancer due to the risk associated with drug interactions [5].
Oncogeriatric assessment consists of a comprehensive multidimensional evaluation, including functional and biopsychosocial issues, addressing aspects of the neoplastic disease such as the risk of toxicities due to systemic therapy and life expectancy [6]. This tool has proven to be helpful in the diagnosis of conditions that are not evident in a routine oncological evaluation [7], such as geriatric syndromes, frailty, functional dependence, and cognitive impairment among others, which have an impact when deciding on therapy, predicting risks of treatment toxicity and mortality [8].
According to official data, the elderly population in Chile accounts for 3,348,010 inhabitants, 1,861,067 females, and 1,468,943 males [9], 90 Percentage of them are part of the Chilean public system of health (FONASA) [10], and the rest are treated in the Chilean private system of health (ISAPRES).
Currently, cancer is the main cause of death in Chile. Unfortunately, local statistics were not initially designed thinking of the definition of the geriatric population, therefore the reported incidence of cancer for the group of 50-69 years is unique and does not allow to have confident numbers concerning the 60-69 years subgroup. Also, there is a lack of an integrated national register of tumors, a situation that underestimates the real dimension of the cancer patient among the geriatric population.
Among the 70 years and older Chilean population, the reported incidence rate and percentage for this group of age for the main type of tumors are as follows: prostate cancer (345,3/100,000 male, 22.9 Percentage), gastric cancer (247.7/ 100,000 inhabitants, 16.4 Percentage), and lung cancer (193.1/ 100,000 inhabitants, 12,8 Percentage) for the male population; and gastric cancer (96/100,000 inhabitants, 10,9 Percentage), lung cancer (94,2/100,000 inhabitants, 10.7 Percentage) and breast cancer (83.9/100,000 women, 9.5 Percentage) for the female population [11].
Currently, in Chile as in other developing countries, oncogeriatrics is gaining impact little by little. It is being promoted by trained specialists, giving guidelines and tools to geriatricians, medical oncologists, hematologists, radiotherapists, and palliative care physicians to achieve quality care and individualized therapy for geriatric patients with cancer.
Despite the pathophysiological differences between a normal cell during the aging process and a cancer cell, there is clear scientific evidence that the normal aging of cells is a known risk factor for developing cancer, meaning that at an older age there is a greater risk for developing cancer [12].
Due to efficient health policies in Chile, a significant reduction in the child mortality rate occurred in recent past decades, associated with better control and management of chronic diseases in adults. This equation resulted in a significant increase in the geriatric population achieving a current life expectancy at birth of 77.3 years for men and 82.1 years for women.
These results place Chile, along with Cuba and Uruguay within the countries of America that by 2025 will have approximately 20 Percentage of the elderly population. This not only means a great achievement in the health policies of these countries but at the same time, a great challenge for providing an adequate standard of life and health to this group, optimizing the management of chronic pathologies, including in this concept the multidisciplinary management of cancer in a more frailty population, often affected by limited socioeconomic resources and access to optimal health care [13].
In Chile, awareness has been raised about the importance of the comprehensive management of the elderly patient with cancer and the need to expand knowledge about this topic among general practitioners, family physicians, internists, and surgeons, but also in all the health team [14]. In this country, there is an increase in the cancer rate in part due to the aging of the population. Despite that many cancer registries in Latin America are in process of continuous improvement, there is no exact data on the real number of older people with cancer, often due to insufficient notification, lack of diagnostic verification, or simply limited access of patients to specialized health centers [15].
The Importance of Oncogeriatrics for the Cancer Teams
Cancer treatments include but are not limited to surgery, systemic treatments (cytotoxic chemotherapy, molecular therapies, biological therapies, hormone therapy, immunotherapy), and radiation therapy. Decision-making on how to properly treat a patient is based on multidisciplinary decisions supported by scientific information from clinical studies. Unfortunately, in clinical studies the elderly population tends to be underrepresented, assuming equivocally that the results of these trials always represent this patient´s population [16]. In the decision-making process on cancer treatments, toxicities and potential sequelae must be considered [17]. Due to new drugs and radiotherapy development, rational and precision surgery, and also an earlier diagnosis of cancer, the older people who will survive cancer in the coming decades will increase strongly, however, the effects of these treatments will have repercussions for the survivors with a potential affectation on their quality of life [18]. Therefore, it is necessary to consider that clinical studies should be adapted for the geriatric population, adjusting their inclusion and exclusion criteria and the objectives that are relevant for this group of age [19]. Many times, the decision-making of cancer treatments is mostly based on the medical oncologist’s opinion assuming that are properly trained for treating older patients with cancer [20].
Regardless of the training of cancer specialists, treatment of the elderly is highly complex and requires a vision and assessment by a geriatrician with knowledge of cancer to obtain proper information about the functional and psychological capacities of the patient, helping for therapeutic decision-making by the cancer medical team. The geriatrician dedicated to evaluating and supporting cancer patients, known today as an oncogeriatrician, uses different tools and instruments to perform a comprehensive geriatric report, subdividing patients according to a greater or minor risk of toxicities to therapies and according to the objective expectations of survival with or without systemic treatment, allowing a rational take of decisions [21].
Characteristics of elderly cancer patients
Older people are a group with special characteristics, very different when compared to the younger population. Therefore, it is important to establish some concepts to clarify the differences between geriatrics and non-geriatric adult patients. Briefly, we will explain phycological changes, and geriatric syndromes which include but are not limited to frailty, polypharmacy, and its consequences, fall syndrome, and malnutrition in the elderly and their relationship with cancer treatments.
There are important physiological changes in the aging process. Knowing the heterogeneity of physiological changes in pharmacokinetics, pharmacodynamics, tolerance in different tissues, and how this influences carcinogenesis is essential for understanding the link between cancer and its treatment in older people. Vulnerabilities assessment, the presence or absence of frailty, and comorbidities are associated with life expectancy [22].
The objectives in the management of elderly patients with cancer should be individualized according to the context of each person as an individual with some common goals, such as relieving symptoms and complications cancer-related, preventing and reducing treatment-related toxicities, improving tolerance to therapy, improving communication between patients and health personnel, reducing the emotional burden between patients and caregivers, and optimizing the care of survivors.
Within geriatric syndromes, some of them are associated with worse results in some cancer treatments. Frailty is defined as a cyclical, complex, and multidimensional state of reduction of the physiological reserve, resulting in a lower capacity for resilience, adaptation, and increased vulnerability to stressors. In the general population, its prevalence varies between 10 Percentage to 20 Percentage among people older than 65 years [23] and reaches up to 50 Percentage in those older than 85 years [24].
The prevalence of frailty reported among cancer patients ranges from 6 Percentage to 86 Percentage, with a median of 42 Percentage [25]. Frailty is associated with a worse survival rate with an HR 2.67 (95 Percentage CI 1.11-6.83, p0.029) according to the Linda Fried Frailty phenotype, increasing to an HR 3.39 (95 Percentage CI 1.82-6.29, p <0>
Reported frailty among the Chilean elderly population, based on analysis from the Chilean National Health System, accounts for 10.9 Percentage (7.7 Percentage for males and 14.1 Percentage for females respectively). Depending on the associated morbidity reported frailty was 0 Percentage when no comorbidity exists, 6.2 Percentage when only one comorbidity is present, but it raises to 64 Percentage when 3 or more comorbidities are present. 32.6 Percentage of cancer patients are frailed according to this report [29].
One of the major problems in geriatrics is polypharmacy. There is no consensus for a clear definition for this term [30], then we could assume that the concomitant use of two or more drugs could be included within this definition. Some authors such as Turner consider polypharmacy when a patient uses five or more different drugs [31]. Polypharmacy has been associated with a greater probability of interrupting scheduled surgery [32], an increase in almost double the risk of post-surgical complications [33], a greater need for hospitalizations [34], and an increase of 6 times more grade 3 or greater chemotoxicities [35]. Polypharmacy is also responsible for producing greater functional deterioration, a higher incidence of delirium [36], and an almost 10-fold increase in the 30-day mortality days in selected populations [37].
Another important geriatric syndrome to be considered and prevented is the “fall syndrome”. The current presence or a previous history of cancer increases the risk of falls by 15 Percentage to 20 Percentage [38]. It is essential to ask about the antecedent of falls during the last 6 months, as well as the limitations in activities of daily living, cancer-related fatigue, to assess walking and balance disorders, to request vitamin D plasmatic levels, to review medications in current use, to correct visual disturbances and to carry out close interdisciplinary management with kinesiology and occupational therapy, encouraging and prescribing physical activities with exercises to improve strength and balance.
Malnutrition is a predictor of mortality and morbidity, being related to up to 20 Percentage of cancer-related deaths and affecting more than a third of cancer patients [39]. It is also related to a higher toxicity rate of cancer therapies [40], lower response rate, poor quality of life, deterioration of functional status, and prolongation of hospital stay. These results must be considered to develop research strategies and assessments by nutritionists to allow a safer cancer treatment or to inform the oncological team if the patient should not undergo treatment. The presence of mood disorders, pain, taste disturbances, and nausea or vomiting should be also assessed. It is essential to determine access to food and activate the social network, implement, and access nutritional supplements, break down diet myths, and emphasize the importance of protein intake in the diet of the elderly globally.
Oncogeriatric evaluation models
International recommendations suggest an oncogeriatric assessment for all cancer patients over 65 years old [41] [42] [43], however, globally there is a lack of geriatricians to achieve this need.
In Spain, after the First National Board of Multidisciplinary Oncogeriatrics Work in 2011, and considering international recommendations as a reference, three ways of evaluating older people with cancer were recommended, depending on the availability and resources of each center [44].
Firstly, the integrated model is considered the gold standard, where a multidisciplinary assessment is carried out involving geriatricians, medical oncologists, radiation oncologists, palliative caregivers, nutritionists, and social workers among other professionals, obtaining a comprehensive diagnosis for making treatment decisions in agreement with the patient. The second form of assessment is the collaborative model which consists of the geriatrician's support to a cancer specialist in the diagnosis and decision-making process, through consultation. The geriatrician performs the oncogeriatric assessment and provides recommendations. In those health centers that do not have geriatricians, the screening model is carried out, focused on the diagnosis of frailty by the oncologist, through an abbreviated comprehensive geriatric evaluation, to recommend the best type of treatment for the patient considering the chances to achieve better results with minor risk of toxicities.
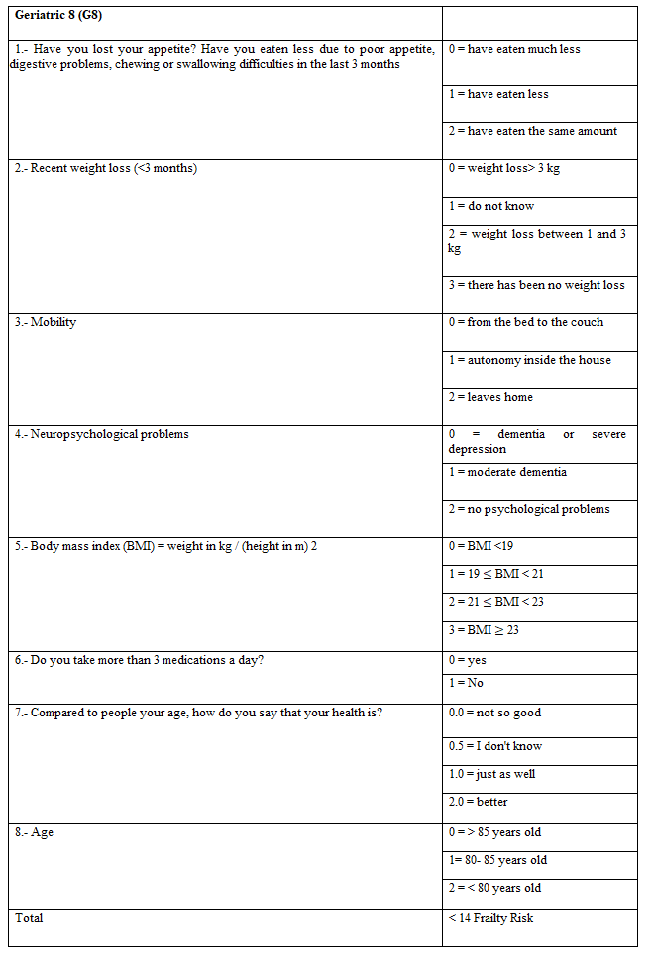
Given the time that is needed for an oncogeriatric evaluation, shortened screening tools have been developed to detect which patients may require an extended geriatric evaluation such as the Geriatric 8 (G8), which consists of 8 questions involving some geriatric domains which have shown to be more sensitive in detecting vulnerable older people [45] (Figure 1).
A recent official Chilean report demonstrated that the first cause of death in this country is cancer and no longer cardiovascular and circulatory diseases [46], concluding also that the Potential Years of Life Lost are higher among adults from 65 to 69 years when compared with the rest of the population.
To ensure strategies looking for increasing the number of geriatric patients with cancer that may undergo a global assessment, in 2019 the first Oncogeriatrics Update Workshop was held in Chile with the support of the Chilean Geriatrics and Gerontology Society, becoming this meeting the first step of oncogeriatrics in Chile.
Unfortunately, only a few months later, the world started to be badly attacked by the SARS-COV-2 pandemic avoiding wider dissemination of this specialty in Chile.
A report from the United Kingdom showed that patients older than 60 years old with active COVID-19 infection have a significantly higher chance to die of cancer when compared with the younger population [47]. As in the rest of the world, in Chile, the pandemic has delayed the diagnosis and treatment of cancer patients resulting in an excess of cancer-related deaths [48].
Currently, in Chile there are only 173 geriatricians recognized by the Superintendency of Health, most of them are practicing in the Metropolitan Region, which includes nearly half of the country’s population [49]. This deficit of specialists makes it impossible to follow the international recommendations, nevertheless, some health centers in Chile are already practicing oncogeriatrics.
Conclusions
The increase in the number of elderly people with cancer in Chile is a recognized fact and we must be prepared to face and carry out a multidimensional diagnosis and offer them quality care and appropriate and individualized treatment.
Older people are per se a heterogeneous population. Despite the high incidence of cancer among this population, it has historically been an underrepresented group in clinical trials, and we have less data to define a beneficial therapy that implies less toxicity, better tolerance, and quality of life. There are special conditions such as geriatric syndromes that have been associated with undesirable events treatment-related that can be prevented and recognized in a comprehensive geriatric assessment allowing its early management to avoid a worsening in quality of life when possible.
Beyond the challenges that the elderly represent and its relationship with higher chances to develop cancer, there is a lack of trustable information that allows correct comparisons between different Latin American countries to estimate the real burden of cancer among the geriatric population of this part of the world. Currently, Latin America and the Caribbean have 1.5 million new cases per year, but it is expected that by 2040 this number will be increased to 2.4 million new cases per year, and most of these patients will be 65 years and older [50]. In the region, the most frequent types of cancer are prostate (15 Percentage), breast (14 Percentage), colorectal (9 Percentage), lung (7 Percentage), and gastric cancer (5 Percentage). Lung tumor is still the leading cause of mortality cancer-related. In 2020, the Incidence Age Standardized Rate (ASR) for Latin America and the Caribbean, and Chile was 186.5 and 180.9/100,000 inhabitants, and the Mortality ASR was 86.6 and 87.4/100,000 inhabitants respectively. Despite the relevance of the need for oncogeriatric services in Latin America, there are only 3 countries with representatives of the International Society of Geriatric Oncology: Mexico, Brazil, and Chile [51].
Today in Chile there are a dozen of geriatricians with some degree of training in oncogeriatrics but there is not a recognized oncogeriatric unit yet. Half of these professionals work, completely or partially, with an oncological group. 50 Percentage of them work in the private system of health, and the rest of them support cancer patients without being integrated into a cancer team. Due to the increase in the elderly population in Chile and the increase in cancer rate among this group, it is essential to promote the development of oncogeriatrics and to create units of this specialty in the country. Spain has created oncogeriatrics units, which will serve as an example to develop similar units in Chile [52], nevertheless, only 14 Percentage of the oncological departments account for an oncogeriatrician [53]. In the USA, where 50 Percentage of cancer patients are 65 years or older, the need to integrate practice nurses into ambulatory care shows to be an effective tool to support oncogeriatric teams [54].
Considering that in Chile currently there are 25 public oncology services for adults we aim that it should be at least one oncogeriatrician per service.
Interdisciplinary collaborative work is required for subsequent updates and for the creation of local guidelines looking to support the different specialists who increasingly treat more elderly people with cancer in Chile. In addition, we must work to develop an adequate follow-up plan facing early possible difficulties as a result of the treatment complications and the early detection of other oncological pathologies in cancer survivors.
References
- (2022). Instituto Nacional de Estadísticas de Chile INE.
View at Publisher | View at Google Scholar - Hoffe S, Balducci L. (2012). Cancer and age: general considerations. Clin Geriatr Med. 28(1):1-18.
View at Publisher | View at Google Scholar - (2022). International Agency for Research on Cancer, Cancer Tomorrow.
View at Publisher | View at Google Scholar - Williams GR, Mackenzie A, Magnuson A, et al. (2016). Comorbidity in older adults with cancer. J Geriatr Oncol. 7(4):249-257.
View at Publisher | View at Google Scholar - Whitman, A., DeGregory, K., Morris, A. et al. (2018). Pharmacist-led medication assessment and deprescribing intervention for older adults with cancer and polypharmacy: a pilot study. Support Care Cancer. 26, 4105–4113.
View at Publisher | View at Google Scholar - Hurria A, Wildes T, Blair SL, et al. (2014). Senior adult oncology, version 2.2014: clinical practice guidelines in oncology. J Natl Compr Canc Netw. 12(1):82-126.
View at Publisher | View at Google Scholar - Loh KP, Soto-Perez-de-Celis E, Hsu T, et al. (2018). What Every Oncologist Should Know About Geriatric Assessment for Older PatientsWith Cancer: Young International Society of Geriatric Oncology Position Paper. J Oncol Pract. 14(2):85-94.
View at Publisher | View at Google Scholar - Molina-Garrido MJ, M. C. Soriano-Rodríguez MC, and C. Guillén-Ponce C., (2019). “¿Cuál es el papel de la valoración geriátrica integral en Oncogeriatría?,” Rev. Esp. Geriatr. Gerontol. 54(01).
View at Publisher | View at Google Scholar - (2022). Instituto Nacional de Estadísticas, Características de la Población.
View at Publisher | View at Google Scholar - (2022). FONASA, Conoce FONASA.
View at Publisher | View at Google Scholar - MINSAL, (2018). Informe de Vigilancia Epidemiológica de Cáncer, Análisis de Mortalidad, Década 2009-2018, Departamento de Epidemiología.
View at Publisher | View at Google Scholar - Aunan JR, Cho WC, Søreide K. (2017). The Biology of Aging and Cancer: A Brief Overview of Shared and Divergent Molecular Hallmarks. Aging Dis. 8(5):628-642.
View at Publisher | View at Google Scholar - Ortega-Gonzalez D. (2018). Envejecimiento y trato hacia las personas mayores en Chile: una ruta de la desigualdad persistente. Sophia Austral, Punta Arenas, n. 22, p. 223-246.
View at Publisher | View at Google Scholar - (2022). MINSAL, Actualización Manual de Geriatría Para Médicos.
View at Publisher | View at Google Scholar - Rolfo C, Caglevic C, Bretel D, et al. (2016). Cancer clinical research in Latin America: current situation and opportunities. Expert opinion from the first ESMO workshop on clinical trials, Lima, 2015. ESMO Open. 1(4): e000055.
View at Publisher | View at Google Scholar - Denson A.C., Mahipal A. (2014). Participation of the elderly population in clinical trials: barriers and solutions. Cancer Control. 21:209–214.
View at Publisher | View at Google Scholar - Nurgali K, Jagoe RT, Abalo R. (2018). Editorial: Adverse Effects of Cancer Chemotherapy: Anything New to Improve Tolerance and Reduce Sequelae? Front Pharmacol. 9:245.
View at Publisher | View at Google Scholar - Shahrokni A, Wu AJ, Carter J, et al. (2016). Long-term Toxicity of Cancer Treatment in Older Patients. Clin Geriatr Med. 32(1):63-80.
View at Publisher | View at Google Scholar - Whelehan S, Lynch O, Treacy N, et al. (2018). Optimising Clinical Trial Design in Older Cancer Patients. Geriatrics. 3(3):34.
View at Publisher | View at Google Scholar - Lichtman S. (2022). All Oncologists Are Geriatric Oncologists...They Just Don’t Know It Yet, The ASCO Post.
View at Publisher | View at Google Scholar - Mohile S G, Magnuson A. (2013). Extermann M (ed): Cancer and Aging. From Bench to Clinics. Interdiscipl Top Gerontol. Basel, Karger, vol 38, pp 85–103.
View at Publisher | View at Google Scholar - Balducci L, Extermann M. (2000). Management of cancer in the older person: a practical approach. Oncologist. 5(3):224-237.
View at Publisher | View at Google Scholar - Collard RM, Boter H, Schoevers RA, et al. (2012). Prevalence of frailty in community-dwelling older persons: a systematic review. J Am Geriatr Soc. 60(8):1487-1492.
View at Publisher | View at Google Scholar - Song X, Mitnitski A, Rockwood K. (2010). Prevalence and 10-year outcomes of frailty in older adults in relation to deficit accumulation. J Am Geriatr Soc. (4):681-687.
View at Publisher | View at Google Scholar - Handforth C, Clegg A, Young C, et al. (2015). The prevalence and outcomes of frailty in older cancer patients: a systematic review. Ann Oncol. 26(6):1091-1101.
View at Publisher | View at Google Scholar - Kristjansson SR, Nesbakken A, Jordhøy MS, et al. (2010). Comprehensive geriatric assessment can predict complications in elderly patients after elective surgery for colorectal cancer: a prospective observational cohort study. Crit Rev Oncol Hematol. 76(3):208-217.
View at Publisher | View at Google Scholar - Tan KY, Kawamura YJ, Tokomitsu A, et al. (2012). Assessment for frailty is useful for predicting morbidity in elderly patients undergoing colorectal cancer resection whose comorbidities are already optimized. Am J Surg. 204(2):139-143.
View at Publisher | View at Google Scholar - Lu J, Cao LL, Zheng Ch et al. (2017). The Preoperative Frailty Versus Inflammation-Based Prognostic Score: Which is Better as an Objective Predictor for Gastric Cancer Patients 80 Years and Older? Ann Surg Oncol. 24(3):754-762.
View at Publisher | View at Google Scholar - Troncoso-Pantoja C, Concha-Cisternas Y, Leiva-Ordoñez A M et al. (2020). Prevalencia de fragilidad en personas mayores de Chile: resultados de la Encuesta Nacional de Salud 2016-2017. Revista médica de Chile. 148(10), 1418-1426.
View at Publisher | View at Google Scholar - Masnoon N, Shakib S, Kalisch-Ellett L., et al. (2017). What is polypharmacy? A systematic review of definitions. BMC Geriatr. 17, 230.
View at Publisher | View at Google Scholar - Turner JP, Shakib S, Singhal N, et al. (2014). Prevalence and factors associated with polypharmacy in older people with cancer. Support Care Cancer. 22(7):1727-1734.
View at Publisher | View at Google Scholar - Parks RM, Hall L, Tang SW, et al. (2015). The potential value of comprehensive geriatric assessment in evaluating older women with primary operable breast cancer undergoing surgery or non-operative treatment--a pilot study. J Geriatr Oncol. (1):46-51.
View at Publisher | View at Google Scholar - de Glas NA, Kiderlen M, Bastiaannet E, et al. (2013). Postoperative complications and survival of elderly breast cancer patients: a FOCUS study analysis. Breast Cancer Res Treat. 138(2):561-569.
View at Publisher | View at Google Scholar - Badgwell B, Stanley J, Chang GJ, et al. (2013). Comprehensive geriatric assessment of risk factors associated with adverse outcomes and resource utilization in cancer patients undergoing abdominal surgery. Journal of Surgical Oncology. 108(3):182-186.
View at Publisher | View at Google Scholar - Hamaker ME, Schiphorst AH, ten Bokkel Huinink D, Schaar C, van Munster BC. (2014). The effect of a geriatric evaluation on treatment decisions for older cancer patients--a systematic review. Acta Oncol. 53(3):289-296.
View at Publisher | View at Google Scholar - Şenel G, Uysal N, Oguz G, et al. (2017). Delirium Frequency and Risk Factors Among Patients with Cancer in Palliative Care Unit. Am J Hosp Palliat Care. 34(3):282-286.
View at Publisher | View at Google Scholar - Elliot K, Tooze JA, Geller R, et al. (2014). The prognostic importance of polypharmacy in older adults treated for acute myelogenous leukemia (AML). Leuk Res. 38(10):1184-1190.
View at Publisher | View at Google Scholar - Mohile SG, Fan L, Reeve E, et al. (2011). Association of cancer with geriatric syndromes in older Medicare beneficiaries. J Clin Oncol. 29(11):1458-1464.
View at Publisher | View at Google Scholar - Soubeyran P, Fonck M, Blanc-Bisson C, et al. (2012). Predictors of early death risk in older patients treated with first-line chemotherapy for cancer. J Clin Oncol. 30(15):1829-1834.
View at Publisher | View at Google Scholar - Aaldriks AA, van der Geest LG, Giltay EJ, et al. (2013). Frailty and malnutrition predictive of mortality risk in older patients with advanced colorectal cancer receiving chemotherapy. J Geriatr Oncol. 4(3):218-226.
View at Publisher | View at Google Scholar - Wildiers H, Heeren P, Puts M et al. (2014). International Society of Geriatric Oncology consensus on geriatric assessment in older patients with cancer. J Clin Oncol. 32(24):2595-2603.
View at Publisher | View at Google Scholar - Gironés Sarrió R, Antonio Rebollo M, Molina Garrido M.J. et al. (2018). General recommendations paper on the management of older patients with cancer: the SEOM geriatric oncology task force’s position statement. Clin Transl Oncol. 20, 1246–1251.
View at Publisher | View at Google Scholar - Mohile SG, Dale W, Somerfield MR, et al. (2018). Practical Assessment and Management of Vulnerabilities in Older Patients Receiving Chemotherapy: ASCO Guideline for Geriatric Oncology Summary. J Oncol Pract. 14(7):442-446.
View at Publisher | View at Google Scholar - Antonio M, Saldaña J, Formiga F et al. (2012). a Reunión Nacional de Trabajo Multidisciplinar en Oncogeriatría: documento de consenso. Rev Esp Geriatr Gerontol. 47(6):279-283.
View at Publisher | View at Google Scholar - van Walree IC, Scheepers E, van Huis-Tanja L, et al. (2019). A systematic review on the association of the G8 with geriatric assessment, prognosis and course of treatment in older patients with cancer. J Geriatr Oncol. 10(6):847-858.
View at Publisher | View at Google Scholar - Ministerio de Salud. (2021). Departamento de Epidemiología. Informe de Vigilancia de Cáncer. Análisis de Mortalidad Prematura y AVPP por Cáncer. Década 2009-2018.
View at Publisher | View at Google Scholar - Russell B, Moss CL, Shah V, et al. (2021). Guy’s Cancer Real World Evidence, Dolly S, Van Hemelrijck M. Risk of COVID-19 death in cancer patients: an analysis from Guy's Cancer Centre and King's College Hospital in London. Br J Cancer. 125(7):939-947.
View at Publisher | View at Google Scholar - Ward ZJ, Walbaum M, Walbaum B, et al. (2021). Estimating the impact of the COVID-19 pandemic on diagnosis and survival of five cancers in Chile from 2020 to 2030: a simulation-based analysis. Lancet Oncol. 22(10):1427-1437.
View at Publisher | View at Google Scholar - Superintendencia de Salud de Chile. Registro de Prestadores Individuales en Salud.
View at Publisher | View at Google Scholar - Piñeros M, Laversanne M, Barrios E et al. (2022). An updated profile of the cancer burden, patterns and trends in Latin America and the Caribbean. Lancet Reg Health. 13100294.
View at Publisher | View at Google Scholar - Verduzco-Aguirre H.C, Navarrete- Reyes A.P, Negrete-Najar J.P, et al. (2020). Cancer in older adults in Latin America: interdisciplinary cooperation between oncology and geriatrics. Rev. salud pública [online]. 22(3). e303.
View at Publisher | View at Google Scholar - Martínez-Peromingo F J, Oñoro-Algar C, Baeza-Monedero M E, et al. (2018). Propuesta de desarrollo de una unidad de oncogeriatría. Tiempos de cambio: nuestra realidad,” Rev. Esp. Geriatr. Gerontol. 53(3).
View at Publisher | View at Google Scholar - Gironés R, Morilla I, Guillen-Ponce C, et al. (2018). Spanish Working Group on Geriatric Oncology of the Spanish Society of Medical Oncology (SEOM). Geriatric oncology in Spain: survey results and analysis of the current situation. Clin Transl Oncol. 20(8):1087-1092.
View at Publisher | View at Google Scholar - Overcash J. (2015). Integrating Geriatrics in to Oncology Ambulatory Care Clinics. Clin J Oncol Nurs. 19(4): E80-86.
View at Publisher | View at Google Scholar
