

Case Report | DOI: https://doi.org/10.31579/2834-5126/081
Congenital lobar emphysema case report: A frequently misdiagnosed disease and therapeutic challenges, Jimma University Medical Center, Southwest Ethiopia
- Mohammed Beshir *
*Corresponding Author: Mohammed Beshir., Department of Paediatrics, Jimma University, Jimma, Ethiopia.
Citation: Mohammed Beshir, (2024), Congenital lobar emphysema case report: A frequently misdiagnosed disease and therapeutic challenges, Jimma University Medical Center, Southwest Ethiopia, Clinical Trials and Clinical Research,3(6); DOI:10.31579/2834-5126/081
Copyright: © 2024, Mohammed Beshir. This is an open access article distributed under the creative commons’ attribution license, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 04 October 2024 | Accepted: 01 November 2024 | Published: 15 November 2024
Keywords: congenital lobar emphysema; congenital cystic lung lesions; recurrent pneumonia; lobectomy
Abstract
Introduction and importance: Congenital Lobar Emphysema is a rare cystic lesion of the lung which may be misdiagnosed and managed as pneumonia or pneumothorax.
Case presentation: We presented a case of a congenital cystic lung malformation; the case demonstrated a 7-month-old infant boy who presented with persistent wheeze and respiratory distress. He was initially diagnosed as recurrent pneumonia, recurrent wheezing disorder and was given unnecessary IV antibiotic treatment, Salbutamol, steroid in another hospital without improvement. Subsequently, the diagnosis of congenital lobar emphysema was made on the basis of the clinical and radiologic features. The condition wasn’t detected before birth. He underwent a successful conservative treatment.
Clinical discussion: Congenital Lobar Emphysema poses a challenge in diagnosis. It may mimic other causes of respiratory distress.
Conclusion: Congenital Lobar Emphysema requires a high index of clinical and radiological suspicion to make an early diagnosis so that timely treatment will be offered.
Introduction
Congenital lobar emphysema is a pulmonary malformation characterized by progressive distension of one, sometimes several, lobes of the lung, compression, and collapse of the remaining lung parenchyma, and mediastinal shift to the opposite side [1]. About 50% of cases have no identified etiology. Partial or complete obstruction of the lobar bronchus is likely to be the cause. Many extrinsic or intrinsic phenomena have been described: bronchomalacia, flange, stenosis, vascular compression, and bronchogenic cyst. The lung parenchyma is normal [3]. It is diagnosed in most cases after birth but prenatal diagnosis is possible. Cardiovascular abnormalities are associated in 10 - 15% of cases [1] [3]. Congenital lobar emphysema is a rare bronchopulmonary malformation with a prevalence of 1 in 20,000 to 30,000 [1]. It is an important cause of respiratory distress in the neonatal period [2] [4]. It remains a diagnostic and therapeutic challenge in developing countries because of the low level of technical facilities [5]. We report a clinical case of congenital lobar emphysema in a 7-month-old infant diagnosed and treated in the pediatric department of Jimma University Medical Center, Southwest Ethiopia.
Case presentation
This is a 7-month old male infant presented with fast breathing and non-whooping non barking cough of 3 days’ duration. Associated with grunting, low grade intermittent fever, decreased breast feeding, and vomiting of ingested matter 2-3x per day of same duration. presented to our pediatrics emergency ward with progressively increasing respiratory distress for seven days and had worsened two days ago. The child was treated in another hospital and was referred to us. Since the age of 4 months he has similar episodes of illness multiple times for which he has been treated both at Limu genet hospital and private clinics with salbutamol puff, different Iv and PO medications and with some improvement in between the episodes. Otherwise: No history of abnormal body movement, No history chocking episodes. No history of Diaphoresis or interruption during breastfeeding. No family history of asthma, allergy or atopy. No history of contact with chronic cougher or TB diagnosed patient.
He was born to a 24 years old para I mother after 9 months of amenorrhea and mother had regular ANC follow at health center. Antenatal history of mother was uneventful. Post-natal period was unremarkable. Mother had several antenatally ultrasound scans but no lung pathology was detected or reported. He is the 1st child for the family. They live in a house of 4rooms with functional window with separate kitchen. He was on exclusive breast feeding for the 1st 6months then started complementary feeding with gruel made of different cereals. He exposed to sunshine at age of 1 month for 20mints without ointment. He vaccinated for his age.
The initial physical examination revealed Acutely Sick Looking in respiratory distress.
His Vital sign: PR=170 RR=50(L) Tº=36.5 RBS=158mg/dl SpO2=85% RA 94%INO2, no anthropometry derangement, WT = 10kg Lt = 72cm MUAC=15cm INDEX =Normal, on respiratory system Nasal flaring, Labored type of breathing, Intercostal and subcostal retractions, Trachea is central, Diffuse wheeze all over the lung, Coarse crepitation right 1/3 of lung field. Other organ systems examination appeared normal. With diagnosis of
Impending respiratory failure 2ndry to severe pneumonia + 1st episode of wheeze the infant ABCD was secured, started on Ceftazidime 50mg/kg/dose, 500mg iv TID
Vancomycin 15mg/kg/dose, 150mg iv TID in 50ml NS over 1hour
Hydrocortisone 4mg/kg/dose, 40mg iv QID
Salbutamol 6puff every 20 min for 1st 1hour, then every 1hour for next 4hours
EBM 150kcal/kg/day, 90ml every 1hour via NG-Tube.
The investigations done
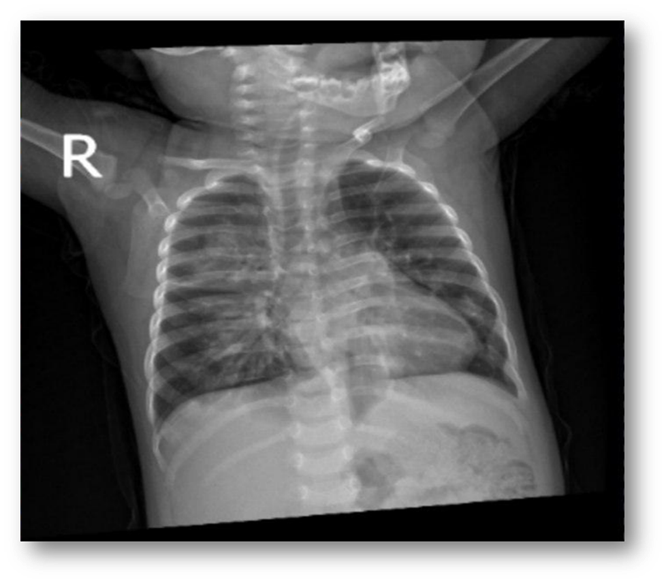
CBC mild anemia, ESR 30 mm/HR, gene expert not detected, HIV Status negative, B/F negative, X-ray of chest revealed perihilar and right lower lung zone airspace opacity with air bronchogram suggestive of Pneumonia, Echocardiography and abdominal ultrasound revealed normal findings.
Salbutamol Challenge Follow up chart at emergency OPD.
The child had no fever, saturation on intranasal oxygen from 92 to 95, RR from 32 to 44, the wheeze persisted with poor response.
The infant Progress note on after three days
P = A 7month old infant kept with the diagnosis of Impending respiratory failure 2ndry to severe pneumonia + 1st episode of wheeze after he presented with fast breathing and grunting of 3days duration, cough and LGIF of 1week duration.
S=cough, fast breathing,
O=GA: ASL(RD)
Vital sign: RR 44, PR 120 Temp 37.6
R/S: mild IC/SC retraction and scattered wheezing
Assessment=Severe pneumonia + 1st episode of wheeze(treated)
Plan: INO2
Ceftazidime 50mg/kg/dose, 500mg iv TID
Vancomycin 15mg/kg/dose, 150mg iv TID in 50ml NS over 1hour
Salbutamol 6puff QID
EBM 150kcal/kg/day, 90ml every 1hour via NG-Tube
Follow vital sign strictly
Progress note on after 15 ward stay
Subjectively: weak voice, muffled voice change, labored type of breathing and low grade intermittent fever. He has also associated vomiting and regurgitation
Objectively: G/A: ASL (RD)
Vital sign: PR=128 RR=46(L) Tº=36.8 RBS=158mg/dl SpO2=80%INO2
R/S: labored breathing IC/SC retraction and diffuse wheeze all over lung fields
N/S: irritable
Assessment: Severe pneumonia(treated) +? GERD + R/o laryngeal web +? Fungal sepsis
Plan: INO2 + Omeprazole 1mg/kg, 5mg iv BID
Fluconazole 4mg/kg/day 40mg po daily
CBC has leukocytosis 33,000 (ANC 28850,) his Hct 30, MCV 55, platelet count normal, ESR 50, blood culture no organism isolated,
Chest CT scan revealed Bilateral ground glass opacity likely >bronchopneumonia
Naso-laryngo-trachea-bronchoscopy. Result > Normal
Progress note on after 25 ward stay
Subjectively: high grade fever fast breathing and grunting
Objectively: GA: ASL(RD)
Vital sign: PR=168 RR=68 Tº=38.3SPO2=94%INO2 RBS 153mg/dl
Anthropometry: WT=9.7 LT=72cm MAUC=15cm WFL >median
R/S: IC/SC retraction. Diffuse wheeze and crepitation on bilateral lung fields
N/S: Alert
Assessment: Recurrent wheeze +? fungal sepsis + HAI (chest focus)
His Ward Progress note after 1 month, still the infant has respiratory distress,
P = Recurrent wheeze +? Fungal sepsis + HAI + R/o ILD
S = Fast breathing intermittent cough
= GA: ASL(RD)
V/S: PR=114 RR=48 Tº=36.5 SPO2=95% RBS 124mg/dl
HEENT: PC&NIS
RSP: mild IC/SC retraction scattered wheeze over posterior lung fields and fine crepitation over posterior bilateral chest
N/S: Alert
Plan: to do blood culture, urine culture, Repeat CXR, Chest CT scan, Organ function test normal, serum electrolyte normal.
Repeat Chest x-ray: Revealed Right lower lung zone nodular opacity. Conclusion > pneumonia
Work up for TB, gene expert not detected
Put on INO2(1L/min)
Ceftriaxone 250mg iv BID
Gentamycin 50mg iv daily
Fluconazole 50mg po daily
Hydrocortisone 40mg iv QID
Salbutamol 6puff QID
Mgso4 50mg/kg, 500mg iv over 1hr with 100ml NS
EBM 150kcal/kg/day, 90ml every 1hour
With these treatments the infant improved with RR 38, temp 37, PR 120 SPO2 with room air 92 and scattered wheeze on chest examination. discharged with
Omeprazole 10mg po daily for 1week
Beclomethasone 2puff BID for 2weeks
Prednisolone 10mg po daily for 5days
Salbutamol puff prn
Appointment after 2weeks at chest clinic follow up
Before the follow the infant developed distress after 1-week discharge and at OPD
had fast breathing and HGIF of 1-day duration. Associated with non-whooping, non-barking type of cough. He has also skin rash that started from the face progressed to involve the whole body associated with reddish discoloration of eye of 4 days’ duration.
Objectively: G/A: ASL (in respiratory distress)
V/S: PR=158 RR=89 Tº=38.5 Spo2=85%RA, 95%INO2
WT=9kg LT=74cm MUAC=15cmWFL b/n1&-2,
WFA b/n 0&2, LFA b/n 1&2: INDEX: Normal
HEENT: Pink conjunctiva and NIS, Wet buccal mucosa & tongue.
Reddish eyes and whitish mucosal oral lesions
LGS: No LAP
R/S: IC/SC retraction, coarse crepitation over right posterior 2/3 of lung fields and diffuse wheeze all over lung
CVS: S1 and S2 well heard. No murmur or gallop
ABD: Full and moves with respiration
No organomegaly
IGS/MSK: Maculopapular rash over whole body
N/S: Alert
Assessment: Complicated measles (severe pneumonia) + Recurrent wheeze + Oral thrush
Plan:
Put on INO2, Isolation room, Salbutamol 6puff every 20 min for 1st 1hour, then every 1hour for next 4hours, Hydrocortisone 4mg/kg, 36mg iv QID, Ceftriaxone 50mg/kg/dose, 250mg iv BID, Pcm 15mg/kg 125mg suppository QID, Miconazole jel apply BID, Vitamin A 100k IU D1 D2 & d14
Follow vital sign closely
Had RR range 42 to 53, temp one record of HGF, still had respiratory distress.
Chest x-ray:
Right lower lung zone nodular opacity. Conclusion > pneumonia
Chest CT scan: revealed
Bilateral ground glass opacity likely >bronchopneumonia
Bedside Echo: No structural lesion, no vegetation
ABD U/S: Unremarkable
Peripheral morphology microcytic, hypochromic anemia, no blast cell seen, the finding suggests Iron deficiency anemia.
After 1 week ward stay of our medical center still the infant had respiratory distress and refractory wheeze, we decide to refer the infant to black lion for further work up and pediatric pulmonologist evaluation. The infant referred with oxygen with referral diagnosis of Persistent wheezing disorder 2ry to r/o Structural lung lesion role out Primary immunodeficiency. At Addis Ababa black lion hospital, the infant Kept at PEOPD for 1weeks then he has been admitted to ward for two weeks. During his stay he was on supportive treatment and further work up was done.
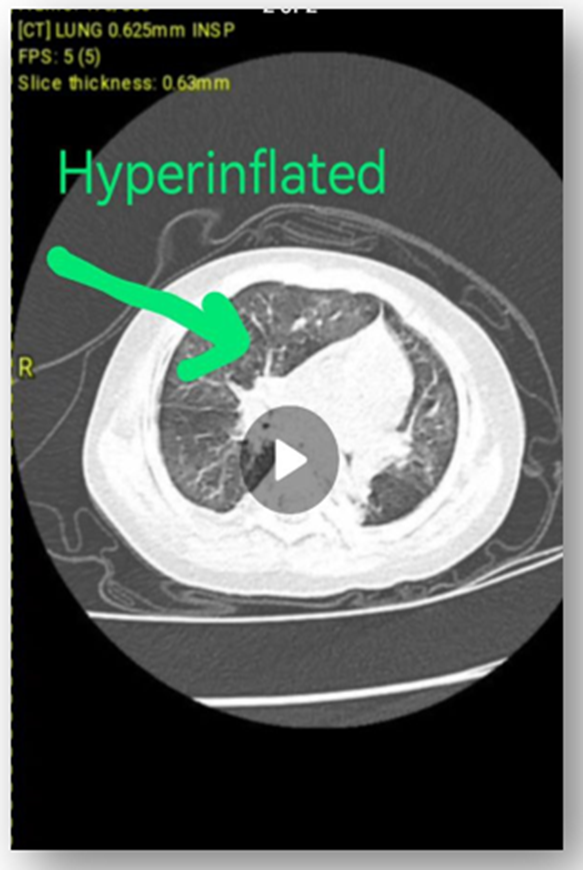
Contrast Enhanced Chest CT Scan: (figure 2)
No strong evidence of infectious process, no sign of interstitial lung disease, no bronchial thickening of bronchiectasis seen, no evidence of mediastinal or hilar lymphadenopathy, no evidence of pleural or pericardial effusion, no evidence of intraluminal obstructive lesion, no sequestration, no CPAM or bronchogenic cyst, heart shows normal size and shape.
Right upper lobe anterior and apical segment hyperinflation + collapsed right upper lobe posterior segment and bibasilar medial segment could suggest Congenital Lobar Over inflation
Immunology assay:
IgA: 33 (N)
IgG: 1233 (N)
IgM: 299 (high)
IgM: 299 (N)

After 3 weeks ward stay the infant Discharged with: Amoxicillin syrup 125mg/5ml, 5ml po BID for 1month Salbutamol puff, Beclometasone puff, Eleron iron drop. Currently he is a 1 year and 5-month old age in good health condition and recovering well. He can walk, say baba, mama, and play with his peers. Has no anthropometry derangement, has regular follow up at the hospital. On follow-up, he continues to feed well and is thriving nicely with appropriate growth for age.
3. Discussion
CLE is a rare malformation of lung development; its estimated incidence is approximately 1/20,000–1/30,000. It often occurs in the neonatal period with hyperinflation of one or more pulmonary lobes. The left upper lobe is the most frequently involved lobe [5]. In our case, the affected lobe was the right upper lobe. The etiologies of CLE are either intrinsic included bronchomalacia and mucosal plugging or they are extrinsic included vascular malformation, tumors and cysts, the factors that leading to a subtotal closure of the bronchus and valve effect with air trapping in the affected lobe [6]. The spectrum of clinical symptoms of CLE is broad ranging from very mild symptoms to acute respiratory distress syndrome and depending upon: the age of the patient; size and location of the anomaly; and associated malformations. Symptoms can start at birth in 25% of cases, within the first month of life in 50% of cases or sporadically after 6 months of age [7]. In our case the patient presented with respiratory distress, recurrent chest infection the symptoms started within the first month of life. CLE may be misdiagnosed as pneumothorax and in such cases insertion of an intercostal drainage tube may be done. On the other hand, like our case many children may be misdiagnosed as pneumonia, wheezing disorder leading to unnecessary antibiotic treatment and loss of valuable time in diagnosis. A retrospective analysis was done on forty patients with cystic lung lesions. The final diagnosis was CCAM in 19 patients, CLE in 11 patients, and bronchogenic cysts and pulmonary sequestration in 5 patients each. Of these, 20% had received a course of prior antitubercular therapy and 30% had an intercostal drain inserted [8]. Prabhu SM et al. reviewed 54 children operated
for congenital cystic lung lesion, 15 children (27%) with an inadvertent chest tube insertion preoperatively based on plain radiograph findings. The patients comprising 10 cases of CCAM and 5 cases of CLE. CCAM was misdiagnosed as complicated pneumatocele and pneumothorax, while CLE was misdiagnosed as tension pneumothorax. They concluded that chest tube insertion in congenital cystic malformations increases the rate of associated complications, and chest CT has a definite role in early diagnosis and deciding appropriate management in these cases [9]. In a 30-year case series in two university hospitals, 20 children with CLE underwent surgery. One patient with severe respiratory distress was misdiagnosed with hypertensive pneumothorax and underwent chest tube drainage [10]. Ten children with CLE were reviewed in order to emphasize the importance of differential diagnosis with pneumothorax. In this series, three patients were mistakenly diagnosed as pneumothorax and intercostal drains were inserted in the emergency department [9]. In our case, the child was being treated for pneumonia without improvement until the right diagnosis was established, and he received the appropriate treatment. The prenatal diagnosis of CLE is established through the ultrasound scan or MRI. With these investigations CLE can be differentiated from other congenital lung lesions. Postnatal diagnoses are made directly after birth in approximately 25–50% of all cases. Where the diagnostic tools are chest X-ray and CT scan. Echocardiography is essential to exclude cardiac anomalies [8]. In our case, the condition wasn’t detected before birth. The diagnosis of CLE was made after birth on the basis of the clinical symptoms and radiologic features, and was confirmed with histologic examination. Echocardiography was normal. Cardiac anomalies occurring in 14–20% of the patients with CLE. Other systems anomalies (renal anomalies, musculoskeletal anomalies, gastrointestinal tract, and others) and syndromes (Williams–Beuren syndrome, Miller–Dieker syndrome, Niemann–Pick disease, Fanconi aplastic anemia). may accompany CLE rarely [7]. In our case, there wasn’t any other systems malformations or accompanied syndromes. Management of patients with CLE consists of dealing with the underlying mechanism. Those with minor symptoms may be treated expectantly like our case whereas those who more severely affected will require lobectomy, which is often curative and it allows the surrounding compressed lung to expand [6]. In our case the decision of conservative treatment was made after a case discussion with pediatric pulmonologist and thoracic surgeon.
Take home massage
Common manifestation of rare diseases should also be considered in patients presented with persistent respiratory distress. Since the diagnosis of CLE is cannot be easily made, high index of suspicion is very important in diagnosing it. Care full investigation including imaging and interpretation is very important to reach at diagnosis.CLE is manageable and has good prognosis, so once the diagnosis is made, early consultation is necessary. In case of dilemma in reaching to diagnosis, early referral is very important.
Declaration of Patient Consent
The authors certify that they have obtained all appropriate patient consent forms. In the form the patient(s) has/have given his/her/their consent for his/her/their images and other clinical information to be reported in the journal. The patients understand that their names and initials will not be published and due efforts will be made to conceal their identity, but anonymity cannot be guaranteed.
Acknowledgement Special thanks to Dr rahel, argaw. pediatric pulmonologist, black lion hospital for the infant management.
References
- C.M. Shanti, M.D. Klein, (2008). Cystic lung disease, 1, in: Seminars in Pediatric Surgery, vol. 17WB Saunders, pp. 2–8.
View at Publisher | View at Google Scholar - J.C. Silva, S.Z. Rocha, J.V. Solís, (2020). Congenital lung malformations, in: Pediatric Respiratory Diseases, Springer, Cham, pp. 551–559.
View at Publisher | View at Google Scholar - David S. Riley, et al., (2017). CARE guidelines for case reports: explanation and elaboration document, J. Clin. Epidemiol. 89 218–235.
View at Publisher | View at Google Scholar - R.A. Agha, T. Franchi, C. Sohrabi, G. Mathew, (2020). for the SCARE Group, The SCARE 2020 guideline: updating consensus surgical CAse REport (SCARE) guidelines, Int. J. Surg. 84 226–230.
View at Publisher | View at Google Scholar - S.S. Rothenberg, (2009). Congenital lobar emphysema, in: Pediatric Thoracic Surgery, Springer, London, , pp. 407–410.
View at Publisher | View at Google Scholar - B. P¨osentrup, A. Leutner, J.G. Riedel, M. Reichert, (2020). Congenital malformations of the lung, in: Thoracic Surgery, Springer, Cham, pp. 265–280.
View at Publisher | View at Google Scholar - G. Ruggeri, M. Maffi, F. Destro, M. Lima, (2013). Congenital lobar emphysema, in: Pediatric Thoracic Surgery, Springer, Milano, , pp. 263–267.
View at Publisher | View at Google Scholar - V.S. Raman, S. Agarwala, V. Bhatnagar, S.S. Panda, A.K. Gupta, (2015). Congenital cystic lesions of the lungs: the perils of misdiagnosis-A single-center experience, Lung India: Off. Organ Indian Chest Soc. 32 (2) 116.
View at Publisher | View at Google Scholar - S.M. Prabhu, S.R. Choudhury, R.S. Solanki, G.S. Shetty, S. Agarwala, (2013). Inadvertent chest tube insertion in congenital cystic adenomatoid malformation and congenital lobar emphysema-highlighting an important problem, Indian J. Radiol. Imag. 23 (1) 8.
View at Publisher | View at Google Scholar - D.C. Cataneo, O.R. Rodrigues, E.N. Hasimoto, A.F. Schmidt, A.J. Cataneo, (2013). Congenital lobar emphysema: 30-year case series in two university hospitals, J. Bras. Pneumol. 39 418–426.
View at Publisher | View at Google Scholar
