

case Report | DOI: https://doi.org/10.31579/ 2834-8532/059
Congenital Facial Palsy in a Neonate: A Case Report and Review of the Literature
- Pauline Kasarachi Akowundu 1*
- Blessing Ebele Kene-Udemezue 2
- Oluwatosin Mosope Akinbi 2
- Josephine C. Ikebudu 2
1 Department of Paediatrics, Redeemers Health Village (RHV), Redemption City, Mowe, Ogun State, Nigeria.
2 Department of Paediatrics, Orile-Agege General Hospital, 3 old Otta road, Orile-Agege, Lagos.
*Corresponding Author: Pauline Kasarachi Akowundu1, Department of Paediatrics, Redeemers Health Village (RHV), Redemption City, Mowe, Ogun State, Nigeria.
Citation: Pauline Kasarachi Akowundu, Blessing Ebele Kene-Udemezue, Oluwatosin Mosope Akinbi, Josephine C. Ikebudu, (2025), Congenital Facial Palsy in a Neonate: A Case Report and Review of the Literature, Clinical Genetic Research; 4(5): DOI: 10.31579/ 2834-8532/059
Copyright: © 2025 Pauline Kasarachi Akowundu, this is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 03 September 2025 | Accepted: 15 September 2025 | Published: 25 September 2025
Keywords: facial palsy; neonate; bell’s palsy; congenital; idiopathic
Abstract
Background: Congenital facial palsy is present at birth or shortly thereafter, with an incidence of 2.1/1000 live births. The majority of cases (78-90%) are associated with birth trauma. However, the most frequent identifiable causes of facial palsy in children are different from those in adults. In children, when not idiopathic, infection, followed by trauma and congenital conditions, are the most common etiologies of facial nerve palsy. Treatment options include steroidsand antiviral agents. The prognosis is generally good, although residual deficits may persist in some children.
Case presentation
A 4-day-old male neonate was noticed to have a right facial deviation, drooling of saliva, inability to close the left eye, and facial asymmetry 12 hours after birth. The blood tests done were all normal. The child was managed conservatively with a gradual resolution of symptoms.
Conclusion
This case report highlights the idiopathic nature of facial palsy (Bell's palsy) and the most likely outcome. We also review the scoring system of Bell's palsy in this report.
Introduction
Idiopathic facial paralysis, another name for Bell's palsy, is one of the most prevalent neurological conditions affecting children. In 1930, Sir Charles Bell was the first to describe unilateral facial weakness. The diagnosis is usually determined when other causes of acute peripheral palsy have been excluded.[1] Steroids and antivirals are among the therapies that remain controversial. [2] The annual incidence of Bell’s palsy is between 15 and 25 per 100,000individuals, including adults.[3] 60–70% of patients with acute unilateral facial paralysis have Bell's palsy; however, over ten years, Folayan et al. in Ile-Ife, Nigeria, observed an incidence of 0.01% over 10 years. The lesion more commonly affected males and the right side of the face. [4,5] Facial nerve paralysis can have a significant effect on the child and cause parents a tremendous amount of distress. The long-term effects on vision, eating, drinking, psychological issues, self-esteem, and quality of life are well-established.[6]
The incidence of facial paralysis in live births is 0.8 to 2.1% per1000 births.[7] There are several possible causes of facial nerve paralysis in children besides idiopathic Bell’s palsy. In newborns, both developmental defects and birth trauma are implicated, with birth trauma being the most common cause. Additionally, other possible risk factors for perinatal traumatic facial nerve paralysis include maternal primiparity, birth weight greater than 3500g, prolonged labor, use of forceps, and prematurity.[8] A definitive diagnosis of idiopathic Bell's palsy would require a thorough review of these factors. [9]
Case Presentation
A term male neonate delivered via spontaneous vaginal delivery, to a 27-year-old primiparous woman, who was noticed to be drooling feeds from one side of the mouth at 12hours of life. On further assessment, he was found to have right facial deviation (figure 1), necessitating admission into the neonatal intensive care unit. There was poor feeding, as the child kept drooling; however, there was no history of fever, seizures, or irritability.
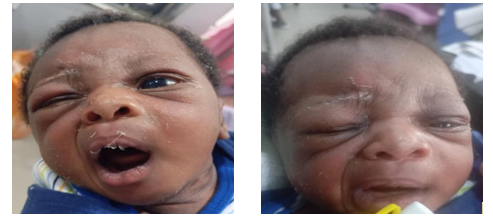
Figure 1: showing loss of left nasolabial folds, deviation of mouth to the right, inability to close the left eye, loss of forehead creases/folds
The mother had an uneventful pregnancy. There was no history of hypertension, diabetes mellitus, genital or oral lesions, or rash in the mother just before delivery. She delivered at term via uncomplicated vaginal delivery; however, labor was prolonged and augmented with oxytocin at 41weeks' gestational age. Delivery was non-instrumental. The infant’s birth weight was 3.1 kg, with Apgar scores of 6 at 1 minute and 8 at 5 minutes. There was no significant edema, caput, or cephalohematoma. There was no notable family history of neurological diseases.
Upon physical assessment, the patient was active and alert. He had a normal pulse rate and blood pressure readings compatible with his age. The pupils were reactive with normal bilateral light reflex. His cardiorespiratory, abdominal, and genital examinations were regular. His head
circumference was 35 cm with a standard head shape and flat anterior fontanel. There was apparent facial asymmetry, with flattening of the nasolabial fold on the left side, incomplete closure of his left eye, and deviation of the mouth towards the right side. All of this was consistent with a left lower cranial nerve VII defect. All other cranial nerves were intact with normal neonatal reflexes and good strength for age. No abnormal neurocutaneous stigmata were elicited.
His basic diagnostic workup was largely non-contributory. He had normal complete hemogram indices, serum electrolytes, urea, creatinine, C-reactive protein, and glucose. A transcranial ultrasound was requested but not performed. The diagnosis of left facial nerve palsy, lower motor neuron type, was then made.

The child received intravenous fluids, and feeds were withheld. The patient had a remarkable rapid improvement over 3-5days and was later discharged home and scheduled for physiotherapy review. The child has been followed up in the clinic and has no residual deficits. He has maintained a routine neurological examination, with complete symmetry upon eye and mouth closure and opening, as well as during crying. The Child has also achieved and maintained a good suck and is thriving well on subsequent follow-ups.
Discussion
The vast majority of causes of neonatal Bell’s palsy are congenital or related to birth trauma, and have to be carefully sought.[10] About 2 in 1000 live births have congenital facial nerve paralysis.[11] In nearly 90% of cases, birth trauma is the most common cause, of which 90?ses are following forceps application. Risk factors for such trauma include pre- and post-maturity, being a first child, being overweight, and the use of forceps in delivery, as well as by cesarean section, [7,12] This contradicts
findings in a retrospective study done in 2010, where forceps delivery accounted for 24% of cases of facial palsy.[8] The compression of the face against the maternal sacral promontory or ischial spine during birth, along with a partially developed mastoid process in neonates, especially preterm, possibly impacts the facial nerve as it exits the stylomastoid foramen.[8] This risk increases with lower gestational age, prolonged labor, and the use of oxytocin for labor augmentation. This could explain facial palsy in this case, who is the first child of the family, with a history of prolonged labor that was augmented with oxytocin; however, the pregnancy was carried to term, and birth weight was normal. Facial palsy is more common in males and typically affects the right side. Though the index case was a male, the palsy was left-sided.
Syndromic and genetic causes represent a small yet diverse group of etiologies associated with congenital facial palsy. It can be the result of central brain malformation syndromes, such as Moebius syndrome, Poland syndrome, Goldenhar syndrome, Branchiootorenal (BOR) syndrome, cardiofacial syndrome, CHARGE syndrome, hemifacial microsomia, and Arnold–Chiari disorder.[13] Facial palsy is one of the diagnostic criteria for Möbius syndrome; however, it is typically bilateral. Furthermore, some hereditary neuromuscular disorders (congenital myotonic dystrophy and congenital myasthenic syndromes) can present with facial palsy that is noticeable at birth.[14]
The significant impairment of functional and aesthetic aspects interferes with the affected child’s quality of life.[15] Despite the relatively favorable natural history of this disorder, many caregivers do still consider it one of the true pediatric neurological emergencies, particularly since it can interfere with breastfeeding; the primary activity at that age, and this is in agreement with the index child, whose feeding was interrupted, necessitating admission into the neonatal intensive care unit.[16]
During a thorough physical examination, it is essential to differentiate lower motor facial palsy from upper motor facial palsy and to rule out other differential diagnosis The symptoms of lower motor facial palsy can range from difficulty in closing the eye, absence of forehead wrinkling, absence of nasolabial fold, and asymmetry of the face, especially on crying with deviation of the angle of the mouth toward the normal side, to complete lack of facial movements on the affected side and some of these features were present in the index child.[17]There may be an impairment in sucking, which was also part of the presenting complaints in our case. Other features to look out for on physical examination include abnormalities of the external ears, features of traumatic delivery, such as periauricular or facial ecchymosis or hemotympanum, and dysmorphic features.[17] In the natural history of facial palsy, symptoms usually peak 48 hours after onset. When facial muscles are put into motor action, for example, when the child cries, the features are more pronounced, as was seen in the index case. The diagnosis of facial palsy remains solely clinical because there are no routine laboratory or imaging studies that are diagnostic.

The objective assessment of the extent of facial nerve palsy is done using the House-Brackmann scale (H-B). This scale is a simplified, widely used tool in both neonates and adults.[18] The scale categorizes facial paralysis into six grades, from normal function (Grade I) to complete paralysis (Grade VI). The H-B scale also assesses facial movement at rest and with effort, considering factors such as forehead movement, eye closure, and mouth movement. From the scale in Table 1, the index child had a grade 4 facial palsy. These scales also enable the objective quantification of facial muscle involvement and guide subsequent physiotherapy and follow-up. It is also helpful
for prognostication and aids in appropriate family counseling and further management.[18] Some other clinicians prefer alternative systems, such as the Sunnybrook Facial Grading system, which is more sensitive to subtle facial changes in movement.
The role of medications in the management of Bell's palsy has remained controversial. Most children with Bell’s palsy tend to recover spontaneously without sequelae with or without medical treatment.[19] Early recovery, three weeks after the onset, is associated with a more favorable prognosis, facilitating the family counseling process.[20] A
systematic review by Pitaro and his group of around 3,000 children with Bell’s palsy concluded that evidence of the role of steroids is still inconclusive.[21] However, some studies have stated that steroids can be used within the first 72 hours of the onset of symptoms, and antiviral therapies should be used for patients with Bell’s palsy grade four and above on the severity scale.[22] The debate extends to other modalities of treatment like physiotherapy, laser therapy, and acupuncture, as there is still no consensus about the usefulness and safety of such interventions.[23]Surgical intervention is indicated in cases of severe and persistent dysfunctional signs with variable outcomes.[24]
The resolution of the traumatic lower motor facial nerve palsy in a newborn takes about 3–6 months, and sometimes lasts up to 2 years, occurring spontaneously. However, some identified poor prognostic factors in traumatic facial nerve palsy include unilateral complete paralysis at birth, hemotympanum, displaced temporal bone fracture, absence of voluntary and evoked motor unit responses by 3–5 days of life, and no improvement of facial nerve function by 5 weeks of age.[25] Physiotherapy and rehabilitation in neonatal facial paralysis are debatable, especially in those occurring secondary to traumatic delivery. As there are no significant functional problems during the neonatal period secondary to unilateral facial nerve palsy, aggressive therapy is often not sought, and watchful waiting is done till 3 months of age, our index child was managed as such. A close follow-up is key, and parents should be counselled on the need for continuous close observation. The use of corticosteroids for accelerating facial palsy recovery has not shown consistent benefit, despite the theoretical role of inflammation and edema in some pathogenesis.[26]
Conclusion
Congenital idiopathic Bell’s palsy (facial palsy) can be encountered in neonates. Other possible causes must be excluded. Though the diagnosis is usually clinical, there is controversy about the usefulness of drugs in the treatment of facial palsy, since complete or near-complete recovery is common. This report highlights the importance of considering Bell’s palsy as a potential diagnosis for facial nerve palsy in neonates, as well as the use of the House- Brackmann scoring system for grading, counseling, prognosis, and treatment selection.
Conflict Of Interest
The authors declared they have no conflict of interest.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.”
Consent
This was obtained from the child's caregivers.
References
- Hashisaki GT. Medical management of Bell’s palsy. Compr Ther 1997. Nov;23(11):715-718.PMID: 9360798.
View at Publisher | View at Google Scholar - Sullivan FM, Swan IR, Donnan PT, Morrison JM, Smith BH, McKinstry B, et al. Early treatment with prednisolone or acyclovir in Bell’s palsy. N Engl J Med 2007. Oct;357(16): 1598-1607.doi: 10.1056/NEJMoa072006.
View at Publisher | View at Google Scholar - Jackson CG, von Doersten PG. The facial nerve. Current trends in diagnosis, treatment, and rehabilitation. Med Clin North Am 1999. Jan;83(1):179-195, x. 10.1016/S0025- 7125(05)70096-1.
View at Publisher | View at Google Scholar - Peitersen E. The natural history of Bell’s palsy. Am J Otol 1982. Oct;4(2):107-111. PMID: 7148998.
View at Publisher | View at Google Scholar - Folayan MO, Arobieke RI, Eziyi E, Oyetola EO, Elusiyan J. Facial nerve palsy: Analysis of cases reported in children in a suburban hospital in Nigeria. Niger J Clin Pract2014;17: 23-7.doi: 10.4103/1119-3077.122828.
View at Publisher | View at Google Scholar - Fu L, Bundy C, Sadiq SA. Psychological distress in people with disfigurement from facial palsy. Eye (Lond). 2011 Oct;25(10): 1322-6.doi: 10.1038/eye.2011.158.
View at Publisher | View at Google Scholar - Pavlou E, Gkampeta A, Arampatzi M. Facial nerve palsy in childhood. Brain Dev. 2011 Sep;33(8): 644-50.doi: 10.1016/j.braindev.2010.11.001.
View at Publisher | View at Google Scholar - Al Tawil K, Saleem N, Kadri H, Rifae MT, Tawakol H. Traumatic facial nerve palsy in newborns: is it always iatrogenic? Am J Perinatol. 2010 Oct;27(9):711-3. doi: 10.1055/s-0030-1253097.
View at Publisher | View at Google Scholar - Shargorodsky J, Lin HW, Gopen Q. Facial nerve palsy in the pediatric population. Clin Pediatr (Phila) 2010. May;49(5): 411-417.doi: 10.1177/0009922809347798.
View at Publisher | View at Google Scholar - Sharma D, Murki S, Dhanraj G. Traumatic facial nerve palsy in newborn: a benign condition. Images Clin Neonatol. 2015; 4:213-214. DOI:10.4103/2249-4847.154135
View at Publisher | View at Google Scholar - Varanasi VK. Congenital facial paralysis. Anaplastology. 2012; 1:1000e101. DOI: 10.4172/2161-1173.1000e101
View at Publisher | View at Google Scholar - [12]. Malik S, Bhandekar HS, Korday CS. Traumatic peripheral neuropraxias in neonates: a case series. J Clin Diagn Res 2014.
View at Publisher | View at Google Scholar - Decraene L, Boudewyns A, Venstermans C, Ceulemans B. D evelopmental unilateral facial palsy in a newborn: Six cases and literature review. Eur J Pediatr. 2020;179: 367-75.doi: 10.1007/s00431-019-03484-8.
View at Publisher | View at Google Scholar - Clark GD, Nordli DR, Dashe JF. Facial nerve palsy in children. Wolters Kluwer UpToDate® 2014.
View at Publisher | View at Google Scholar - Ciorba A, Corazzi V, Conz V, Bianchini C, Aimoni C. Facial nerve paralysis in children. World J Clin Cases 2015. Dec;3(12):973-979. doi: 10.12998/wjcc. v3.i12.973.
View at Publisher | View at Google Scholar - Dushyant B. Management of facial nerve palsy in the newborn period. UK: Nottingham Neonatal Service - Clinical Guidelines (No. F16); 2013.
View at Publisher | View at Google Scholar - Goyal M, Prashanth RR, Shah S, Mujeeb AA, Mhatre S, Haribalakrishna A. Deciphering unilateral congenital facial palsy in neonates: A case series and literature review. Wadia J Women Child Health. 2023;2(3):116-20. doi: 10.25259/WJWCH_1_2024
View at Publisher | View at Google Scholar - Vrabec JT, Backous DD, Djalilian HR, Gidley PW, Leonetti JP, Marzo SJ, et al. Facial Nerve Disorders Committee Facial Nerve Grading System 2.0. Otolaryngol Head Neck Surg, 2009.
View at Publisher | View at Google Scholar - Ismail AQ, Alake O, Kallappa C. Do oral steroids aid recovery in children with Bell’s palsy? J Child Neurol 2014. Oct;29(10): NP96-NP97.doi: 10.1177/0883073813504624.
View at Publisher | View at Google Scholar - Biebl A, Lechner E, Hroncek K, Preisinger A, Eisenkölbl A, Schmitt K, et al. Facial nerve paralysis in children: is it as benign as supposed? Pediatr Neurol 2013. Sep;49(3): 178-181.doi: 10.1016/j.pediatrneurol.2013.03.013.
View at Publisher | View at Google Scholar - Pitaro J, Waissbluth S, Daniel SJ. Do children with Bell’s palsy benefit from steroid treatment? A systematic review. Int J PediatrOtorhinolaryngol 2012. Jul;76(7): 921-926.doi: 10.1016/j.ijporl.2012.02.044.
View at Publisher | View at Google Scholar - Youshani AS, Mehta B, Davies K, Beer H, De S. Management of Bell’s palsy in children: an audit of current practice, review of the literature and a proposed management algorithm. Emerg Med J 2015. Apr;32(4): 274-280.doi: 10.1136/emermed-2013-202385.
View at Publisher | View at Google Scholar - Li P, Qiu T, Qin C. Efficacy of Acupuncture for Bell’s Palsy: A Systematic Review and Meta-Analysis of Randomized Controlled Trials. PLoS One 2015. May;10(5): e0121880.doi: 10.1371/journal.pone.0121880.
View at Publisher | View at Google Scholar - Yi H, Liu P, Guo H, Wang C, Ni F. [Surgical treatment to facial nerve paralysis of different pathogeny]. Lin Chung Er Bi Yan Hou Tou Jing Wai Ke Za Zhi 2011. Feb;25(4):154- 157.
View at Publisher | View at Google Scholar - Bergman I, May M, Wessel HB, Stool SE. Management of facial palsy caused by birth trauma. Laryngoscope. 1986; 96:381-4. doi: 10.1288/00005537-198604000-00008.
View at Publisher | View at Google Scholar - Madhok VB, Gagyor I, Daly F, Somasundara D, Sullivan M, Gammie F, et al. Corticosteroids for bell's palsy (idiopathic facial
View at Publisher | View at Google Scholar
