

Case Report | DOI: https://doi.org/10.31579/2835-2882/038
Complicated sigmoid colon volvulus. Case presentation.
- Javier Estrada López 1
- Yosniel Lugo Echevarria 2
- Anaisa León Mursuli 3
- Pedro Rolando López Rodríguez 4*
1 First-degree specialist in general surgery.
2 First-degree specialists in general surgery, instructor professor.
3 Specialist in comprehensive general stomatology.
4 First- and second-degree specialist in general surgery, assistant researcher and consulting professor.
*Corresponding Author: Pedro Rolando López Rodríguez. Address: Street Continental No. 152.Reparto Sevillano. La Havana. Cuba.
Citation: Javier Estrada López, Yosniel Lugo Echevarria, Anaisa León Mursuli, Pedro Rolando López Rodríguez, (2023), Complicated sigmoid colon volvulus. Case presentation., Clinical Research and Studies, 2(5); DOI:10.31579/2835-2882/038
Copyright: © 2023, Pedro R. L Rodríguez. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 04 October 2023 | Accepted: 16 October 2023 | Published: 30 October 2023
Keywords: intestinal obstruction; small intestine volvulus; ileal volvulus
Abstract
Sigmoid volvulus is a common cause of mechanical intestinal obstruction in surgical services that, if not treated in time, can progress to necrosis and perforation. Objective: To describe the clinical characteristics of a case of intestinal obstruction due to complicated sigmoid volvulus. Clinical case: 21-year-old male patient who comes to the clinic with symptoms of asymmetrical distention and intense, diffuse, colic-like abdominal pain with the association of nausea and profuse vomiting, with a bilious appearance where he reports not expelling gas and feces through the rectum. 5 days ago, evolution. Semiotechnically, the pain was persistent, diffuse throughout the abdomen, intense, stabbing, not relieved with analgesics, without other accompanying symptoms. Laboratory and imaging studies were performed, the results were suggestive of a complicated small bowel mechanical obstructive syndrome. Surgical treatment was decided, almost total ileal volvulus was diagnosed. Conclusions: The diagnosis of small intestine volvulus requires a high index of suspicion. The treatment is eminently surgical; Intestinal resection of the affected segment is required whenever the intestinal tissue is not viable.
Introduction
Sigmoid volvulus is a rare entity; In the West, specifically Central and North America, its incidence is lower in relation to other countries, it represents only 5% of intestinal obstructions. (1,3) The term volvulus derives from the Latin returné, which means “to roll up, to bend.” It refers to the twisting of a loop around itself and its mesentery; In the sigmoid colon, it occurs specifically when the last portion of the colon rotates on its axis, which leads to intestinal occlusion, ischemia and, if not treated promptly, perforation (1,2).It is the third cause of colonic obstruction worldwide. In Western countries, it generally occurs in male patients over 70 years of age. The most commonly affected sites are the sigmoid colon (60-75%), the cecum (25-40%) and rarely in the transverse colon or splenic flexure (2-4%). (1,2,3). It is of multifactorial origin, it is related to a high-fiber diet, chronic constipation, laxative abuse, confinement in nursing homes, diabetes, neuropsychiatric conditions with reduced autonomy, prolonged bed rest and a history of laparotomy. However, the most cited predisposing factor is the presence of long, redundant colonic segments (such as sigmoids), which have elongated mesenteries and a narrow base (4,5,6).
The population that lives above 3,000 meters of altitude tends to have a colon of greater length and diameter than inhabitants who live at lower altitudes; this acquired characteristic is called Andean Dolicomegacolon. It is believed that an important factor in its development is the lower atmospheric pressure at altitude, and according to the physical law of Boyle and Mariotte, the expansion of intraluminal gases could influence the increase in intestinal dimensions. (7,8,9) her diagnosis is clinical, coupled with a high index of suspicion. Among the complementary examinations, a simple abdominal x-ray in the standing and supine position has a diagnostic certainty of close to 90% in cases and presents characteristic signs such as the coffee bean sign. (3)
The objective of this work is to describe the clinical characteristics of a case of intestinal obstruction due to complicated sigmoid volvulus.
Methods
An observational study has been carried out on a case diagnosed and treated with complicated sigmoid volvulus, the clinical history of this patient was reviewed in detail, an adequate application of the clinical method was carried out where it allowed collecting the necessary data for the interrogation and physical examination. Diagnostic-therapeutic means were used, including imaging tests (x-rays, ultrasound), blood tests, and the necessary instruments were used in the operating room to carry out the surgical procedure.
Case presentation
A 21-year-old black male patient who attended the general surgery service of the Sambwweni Hospital in the city of Ukunda, Kwale County, Kenya. He comes to our office with symptoms of distension and intense, diffuse, colic-like abdominal pain with the association of nausea and profuse vomiting, with a bilious appearance, where he reports not passing gas and feces through the rectum for 5 days. In addition, he takes a general fever of 38 degrees. In his general examination we found a patient with severe dehydration, peritoneal facies, accelerated radial pulse, hypotensive, with thermal gradient, oligoanuric, with slight seizure of the sensorium. It is decided to admit him, an emergency preoperative is performed where the hydromineral and acid-base disorders are confirmed, which are brought to stability values, complemented with antibiotic-parenteral therapy, decompressive measures and hydroelectrolyte resuscitation. On radiological examination we found a pattern of mechanical intestinal occlusion of the small intestine with central staircase fluid-air levels, with a rosary sign. The abdominal ultrasound confirmed the presence of distended loops without peristalsis accompanied by free fluid in the peritoneal cavity. He is taken to the operating room where the distention of the thin loops with suffering fluid is confirmed where we find a giant sigmoid volvulus with vascular compromise with the association of a partial volvulus of the small intestine (terminal ileum) that compromised the blood supply, forming part of the strangulating element. of the sigma rotation. Initially, control and reception of the almost completely compromised sigmoid is carried out with subsequent anastomosis in a discontinuous plane with 3/0 polyglycolic acid suture. Subsequently, the reception and anastomosis of almost 15 cm of small intestine is evaluated and decided, where we perform an end-to-lateral ileoascendenteostomy in a discontinuous plane with 3/0 polyglycolic acid suture (reimplantation of the ileocecal valve). In addition, regulated peritoneal lavage is performed and two abdominal tubular drains are left with the modality of relaparotomy on demand. On the fifth day, the patient progressed favorably, complying with antibiotic therapy, total parenteral nutrition, maintenance hydration and supplementary measures. The patient was discharged after 10 days with a favorable evolution.
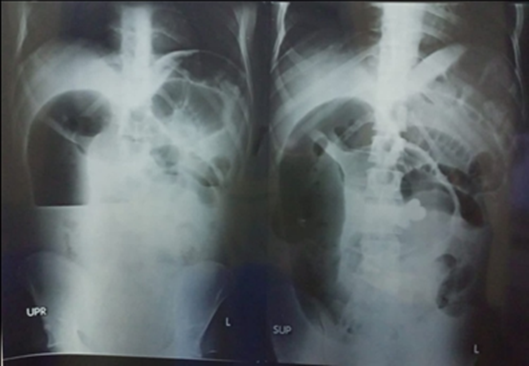
Figure 1: Shows preoperative radiological study

Figure 2: Initial image during laparotomy

Figure 3: Necrotic terminal ileum
Discussion
Volvulus occurs when a loop of the intestine twists around itself and the mesentery that supports it, causing an intestinal obstruction, as a consequence blood flow decreases, which produces an ischemic intestine. The first reported case of volvulus in the literature is from 1841 when Rokitansky described it as a cause of intestinal strangulation. (10). The clinical presentation of this entity corresponds to an acute occlusive abdominal condition. It is demonstrated both by the elements of the physical examination and in simple abdominal x-rays.The latter helps determine the site of the obstruction, usually discovers abnormal amounts of gas, liquid and determines if there is distention, shows air-fluid levels within the obstructed loops, which constitutes a late sign (11,12), as was observed in the studies of this patient. Treatment is discussed in the case presentation. Within surgical practice, various modalities are proposed, one of them is endoscopic treatment (13) in the acute phase and then definitive surgery, others perform segmental resections and primary anastomoses, some authors lean towards resection and emergency Rankin colostomy. Mickulicz for restitution in the second half. (14) Others proscribe endoscopic devolvulation or saline enemas, a technique that has ceased to be used because the intestine can become necrotic, subsequently perforate and cure is not obtained (15). This is why it is considered that it should be indicated on a temporary basis until perform the definitive procedure.
When bowel volvulus is suspected, regardless of the results of the imaging study, surgery should be performed immediately, as in the present case. The entire intestine is visualized in search of points of obstruction; subsequently, resection of the affected segments with primary anastomosis is the surgical method of choice.
Conclusions
It is concluded that the appearance of sigmoid volvulus associated with a volvulus of the small intestine is rare, it is also difficult to diagnose, which is why it requires high skill of the surgeon and a high index of suspicion. The clinical manifestations and imaging findings They are very useful in early diagnosis. Surgical treatment is primarily intestinal resection of the affected segment whenever the intestinal tissue is not viable.
Conflict of Interests
The authors declare that does not exist any interest conflict.
Authors' contributions
Javier Estrada López: he made the surveys and searched the bibliography. He chose the sampling method by selecting the study population and analyzed and discussed the content of the tables.
Yosniel Lugo Echevarria: He stated the objectives of the study, selected and triangulated the variables and performed the translation into English and the final revision of the manuscript.
Anaisa León Mursuli: she helped fill out surveys and search bibliography, performed statistical processing, calculated arithmetic means and standard deviation of the quantitative variables She applied the Family Functioning Perception Test or the FF-Sil Test.
Pedro Rolando López Rodríguez: Performed the statistical processing, calculated and He interpreted the chi-square and associated variables according to Duncan's twelfth. He wrote the document.
References
- Beyuma-Mora Hugo E., Labastida-Ramírez Diana L., Vera-Bernal José A., Murguía-Zamora Laura M., Guevara-Valmaña Osvaldo I. (2022). “Sigma Volvere” acerca del vólvulo de sigmoides, diagnóstico y manejo quirúrgico, reporte de serie de casos. Rev.
View at Publisher | View at Google Scholar - Aulestia D, Sánchez B, Vega Cueva C. (2018). Presentación infrecuente de Vólvulo del Sigmoides en 2 casos. Mediciencias UTA [Internet]. 2(1). Disponible en:
View at Publisher | View at Google Scholar - González Cornejo A, Bruno V. (2021). Vólvulo de sigmoides: Experiencia de 5 años en el hospital regional Rafael Hernández. david, Chiriquí. Enero 2013- diciembre Revista Médico Científica. 33(2):13–19.
View at Publisher | View at Google Scholar - Sierra Enrique Eddy, Bermúdez Chávez Francisco, Almenares Lombillo Niurka. (1997). Vólvulo del sigmoides: Morbilidad y mortalidad. Estudio de 63 pacientes. Rev Cubana Cir [Internet]. [citado 2023 Abr 10]; 36(2): 147-152. Disponible
View at Publisher | View at Google Scholar - Quevedo Guanche Lázaro. (2007). Vólvulo del sigmoides: diagnóstico y tratamiento. Rev Cubana Cir.
View at Publisher | View at Google Scholar - Alejandra BC. (2019). Vólvulo de sigmoides. Revista Médica Panacea. 7(3).
View at Publisher | View at Google Scholar - Pinto Monrroy FR, (2019). Portugal Gallegos LY. Volvulo de sigmoides en el hospital de apoyo departametal Hipolito Unanue de Tacna 1996- 2000. Revista Médica Basadrina. 1(1):18–21.
View at Publisher | View at Google Scholar - Rivera-Nava JC. (2015). Vólvulo Simultáneo de íleon y sigmoides. Revista de Gastroenterología de México. 80(1):115–116.
View at Publisher | View at Google Scholar - Sacta Rivera DE, Ocampo Ocampo AM, Lozado Munzón AM. (2022). Vólvulo del Sigmoides. suturando conocimientos en el arte de la cirugía.
View at Publisher | View at Google Scholar - Obando A, Reyna R. (2021). Vólvulo de sigmoides: Reporte de Caso. Revista Médica de Panamá - ISSN 2412-642X. 26–29.
View at Publisher | View at Google Scholar - López-Casillas N, Cuevas-González A, Zambrano-Lechuga R. (2017). Vólvulo Primario de íleon: Una rara forma de obstrucción intestinal en el adulto. Reporte de Caso y Revisión de la Literatura. Revista Chilena de Cirugía.
View at Publisher | View at Google Scholar - Dhatt HS, Berh SC, Miracle A, Wang ZJ, Yeh BM. (2015). Radiological evaluation of bowel ischemia. Radiol Clin North Am [Internet]. 53(6):1241-54.
View at Publisher | View at Google Scholar - Muñoz García D, Cardona Gomez D, Hoyos Mendez Y. (2020). Volvulo del sigmoides. Rev Cie sal [Internet]
View at Publisher | View at Google Scholar - Altadill R, Barbastro N, Fumanal B, Castán M. (2023). Vólvulo de colón sigmoides. Rev Sanit Invest
View at Publisher | View at Google Scholar - Batista Ramiréz A, Kedisobua E, Ramiréz J. (2014). Vólvulo de Sigmoides. Presentación de caso. Mediciego.
View at Publisher | View at Google Scholar
