

Research Article | DOI: https://doi.org/10.31579/ 2834-8788/004
Comparison Of the Effects of Bosentan and Sildenafil in Treatment of Patent Ductus Arteriosus and Pulmonary Arterial Hypertension in Preterm Infants: Randomized Clinical Trial
1 Hazrat Rasoul Akram Hospital, Iran University of Medical Sciences, Tehran, Iran.
2 Shahid Akbarabadi Clinical Research Developmant Unit (ShACRDU), Iran University of Medical Sciences, Tehran, Iran.
3 Department of Anesthesiology, Imam Khomeini Hospital, Ilam University of Medical Sciences, Ilam, Iran.
4 Department of Pediatric, Firouzabadi Clinical Research Development Unit, Iran University of Medical Sciences, Tehran, Iran.
5 Ali Asghar Hospital, Iran University of Medical Sciences, Tehran, Iran.
*Corresponding Author: Elaheh Fathi, Ali Asghar Hospital, Iran University of Medical Sciences, Tehran, Iran.
Citation: Radgoudarzi M., Mazouri A., Taherifard P., Asma, Fath E. (2022). Comparison Of the Effects of Bosentan and Sildenafil in Treatment of Patent Ductus Arteriosus and Pulmonary Arterial Hypertension in Preterm Infants: Randomized Clinical Trial. Journal of Heart and Vasculature.1(1); 10.31579/ 2834-8788/004
Copyright: © 2022 Elaheh Fath, This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 20 September 2022 | Accepted: 23 September 2022 | Published: 04 October 2022
Keywords: PAH; PDA; bosentan, sildenafil; preterm; neonates; echocardiographic index
Abstract
Background: Pulmonary arterial hypertension (PAH) is a common disorder in preterm neonates caused by patent ductus arteriosus (PDA). Although both sildenafil and bosentan have been shown to improve PAH, there is no study to compare the effect of these drugs in improving preterm infants with hemodynamically significant PDA and PAH. This study aimed to compare the therapeutic efficacy, safety, and possible side effects of combined therapies with Apotel + Bosentan, Apotel + Sildenafil, and Apotel alone in treating PDA and PAH in preterm infants.
Methods: This clinical trial was conducted on 150 preterm neonates with PDA and PAH. Neonates were then divided into three groups and orally administrated with Apotel alone (10 mg/kg), Apotel (10 mg/kg) + Sildenafil (1 mg/kg), and Apotel (10 mg/kg) + Bosentan (1 mg/kg). Echocardiographic examination was performed before and 72h after the intervention.
Results: Treatments with Apotel, Apotel + sildenafil, and Apotel + bosentan significantly decreased the mean of RV1, RV2, RV3, RVEDA, RVESA, RV/LV, TR intensity, TR PG, PI PG, and MPA diameter compared to before intervention (p<0.01). The mean of TAPSE after Apotel, Apotel + sildenafil, and Apotel + Bosentan administrations was significantly increased compared to before the study, indicating improvement in RV performance (p<0.01). The frequency of BPD and ROP in Apotel group (7.7% and 19.2%, respectively) was significantly lower than that in Apotel + sildenafil group (30% and 45%, respectively) and Apotel + bosentan (25% and 40%, respectively) groups (p<0.05).
Conclusion: Oral administration of sildenafil and bosentan improved cardiac index beside its side effects in preterm infants PAH and PDA. Future clinical trial studies with larger sample sizes and long-term follow-up on term or near term neonates are recommended.
Trial registration: IR.IUMS.FMD.REC.1399.430
Introduction
Pulmonary arterial hypertension (PAH) is a progressive disorder strongly associated with increased mortality or morbidity rates in preterm infants, especially those under 34 weeks of gestation age [1]. The prevalence of this disorder is reported to be 1 in every 500 live births. The mortality rate of infants with PAH in developing countries is 10-20%; however, it is higher among patients with no access to essential drugs [2]. In the advanced stage, PAH can lead to structural and functional changes in the pulmonary arteries and increase pulmonary vascular resistance, eventually leading to heart failure and increased mortality rate [3,4]. This disorder is usually caused by patent ductus arteriosus (PDA). Limited studies investigate PAH causes, its associated risk factors, complications, and therapeutic strategies [5]. In PAH, the pulmonary artery's inadequate responsiveness to increased oxygen, acute hypoxia, and chronic fetal hypoxia can be associated with increased pulmonary artery smooth muscle [4,6]. Furthermore, it may be related to partial or complete inability of the lungs for proper dilatation and ventilation that is consequently associated with contraction of pulmonary artery smooth muscle and reduced lumen diameter, enhanced pulmonary artery resistance, and higher pulmonary artery pressure [7,8].
Despite the relatively high prevalence of PAH associated with PDA in preterm infants, there is no appropriate therapeutic pattern for managing the disease in these patients. Therefore, finding a suitable treatment option for PAH improvement in premature infants is valuable to prolong their life. Currently, therapeutic options for PAH are increasing, so that multiple drugs have been reported for PAH in different studies. These therapeutic drugs can be classified into main classes, including prostacyclins or prostacyclin derivatives, nitric oxide (NO) pathway regulators, and endothelin-related vasoconstrictors [9]. Sildenafil is a 5-phosphodiesterase (5-PDE) inhibitor, considered the first drug to improve pulmonary arterial pressure [10]. This drug affects cGMP metabolism by inhibiting 5-PDE activity and causes vasodilation, smooth muscle proliferation, platelet aggregation inhibition, pulmonary and systemic tensions, and improvement of cardiac index [11, 12]. Bosentan is another pulmonary anti-hypertensive drug that acts as a specific and competitive antagonist for endothelin-1 (ET-1) receptor [5]. Previous studies showed that endothelin-1 receptor is significantly increased in patients with pulmonary artery hypertension and, therefore, it seems that this receptor has a crucial pathogenic role in PAH [13].
Although both Sildenafil and bosentan have different mechanisms to improve or reduce PAH, their therapeutic effect on PAH treatment has not been compared yet. Therefore, this clinical trial study aimed to compare the efficacy, safety, and side effects of bosentan and Sildenafil compared to the standard drug, Apotel, in preterm neonates with PAH.
Methods
This blinded clinical trial study was conducted to compare the efficacy, safety, and possible side effects of Bosentan and Sildenafil on preterm neonates with PDA and PAH. They were born and admitted to the NICU at Akbar Abadi Hospital (Tehran, Iran) from 2019 to 2021. The study was approved by the Ethics Committee of the Iran University of Medical Sciences and registered in the Iranian Registry of Clinical Trials (IR.IUMS.FMD.REC.1399.430). In preterm infants with respiratory symptoms, arterial oxygen saturation and cyanosis, PDA, and PAH confirmation were performed by echocardiographic examinations. Only preterm neonates with pulmonary artery pressure of ≥25 mmHg and tricuspid valve regurgitation with a gradient of ≥30 mmHg with or without the right to left shunt were included in this survey. Infants with other cyanosis-related diseases and PAH caused by pneumonia or meconium aspiration, seizures, congenital neuropsychiatric disorders, metabolic and genetic syndromes, pulmonary hypoplasia syndrome, congenital heart anomalies, and other fatal abnormalities were excluded from the study. Neonates were then divided into three groups (A, B, and C) after matching based on gestational age, age at admission time, weight, and sex. In-group A, neonates received Apotel (10 mg/kg) by gavage every 6 hours for three days, while infants in-group B received combined therapy with Apotel (10 mg/kg) and Sildenafil (1 mg/kg) every 12 hours -. Preterm neonates in-group C were orally administrated with a combination of Apotel (10 mg/kg) and Bosentan (1 mg/kg) every 12 hours for 3days. To evaluate the safety and tolerability of medications, all neonates were examined daily for adverse effects, including hypertension, gastrointestinal tolerance, pulmonary hemorrhage, and edema until the end of treatment. After 72 hours of the drug administration, echocardiography parameters examination (including RV1, RV2, RV3, RVEDA, RVESA, RV/LV, TR intensity, TR PG, PI PG, and MPA diameter) was performed again in all neonates in three groups. Furthermore, parameters such as duration of oxygen demand, need for aggressive treatments, and course of medication was compared between three groups.
Statistical analysis
The results of this study were analyzed by SPSS software (Version 19). Normalization of data was evaluated using the Kolmogorov-Smirnov test. Quantitative data were reported as Mean ± SD. The percentages and frequencies of each item between the two groups were compared using Crosstabs and Chi-Square tests. Comparison of mean parametric data in case of normal distribution was evaluated using ANOVA test; otherwise, it was analyzed using a non-parametric test. Pearson correlation test was used to examine the relationship between quantitative variables, and Spearman correlation test was used to investigate the ranking variables. Paired t-test was used to compare the mean of parametric data before and after the study in each group. In this study, p-value <0>
Results
In this survey, 150 neonates with confirmed PDA and PAH under echocardiography evaluation were recruited into the study. Patients were then randomly divided into three groups: Apotel, co-treated Apotel + Sildenafil, and Apotel + bosentan. Both groups were matched in terms of gestational age, Apgar scores, weight, gravidity, type of pregnancy, and gender (Table 1).
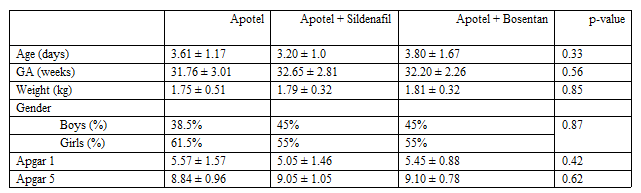
There was no significant difference in medications and respiratory support status between the three groups (Table 2).
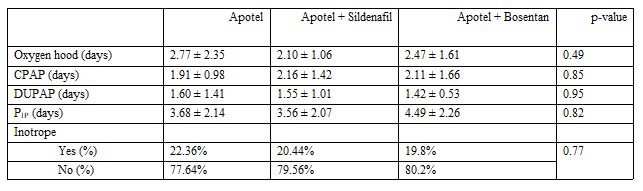
The frequency of inotropic therapy among neonates in all three groups was around 20 Percentage. The average duration of demands for oxygen and CPAP therapies among all three groups was in the range of 2.5 and 2 days, respectively.
There was no significant difference in the mean duration of gaining birth weight (p = 0.63) and complete oral feeding intolerance (p = 0.59) between the three groups (Table 3).

The average duration of reaching birth weight and oral feeding intolerance in neonates of all three groups was in the range of 4-5 days and 13-17 days, respectively. Comparison of the mean of echocardiography parameters before and after intervention between all three groups can be seen in Table 4.
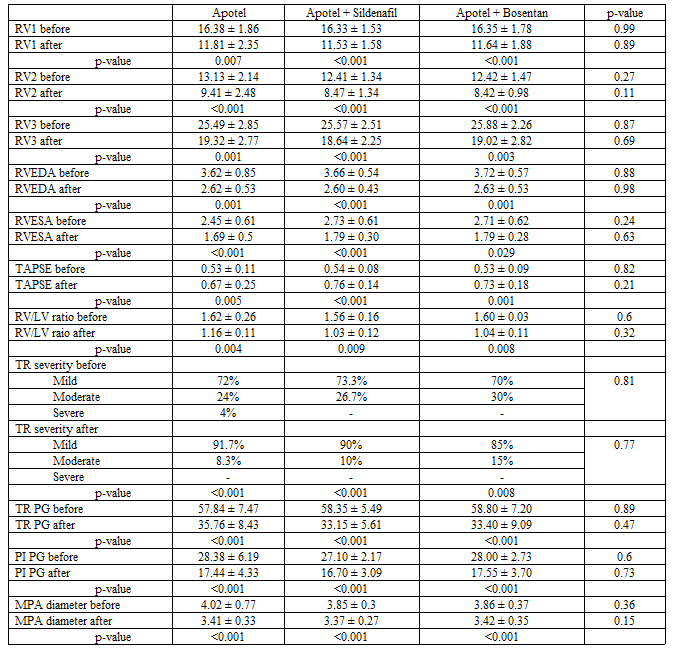
No significant difference was observed in the mean of these parameters before and after intervention between the three groups. Treatment with Apotel, Apotel + Sildenafil, and Apotel + bosentan significantly decreased the mean of RV1, RV2, RV3, RVEDA, RVESA, RV/LV ratio, the intensity of TR, TR PG, PI PG, and MPA diameter compared to before the intervention. In contrast, the mean of TAPSE after Apotel, Apotel + Sildenafil, and Apotel + bosentan administration was significantly increased compared to before the study.
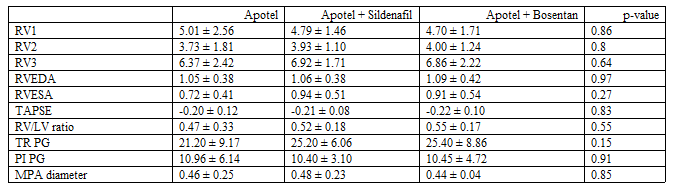
Further analysis revealed no significant difference in the mean difference of each echocardiography parameter between the three groups (Table 5).
The comparison of the frequency of side effects caused by each drug therapy is summarized in Table 6.
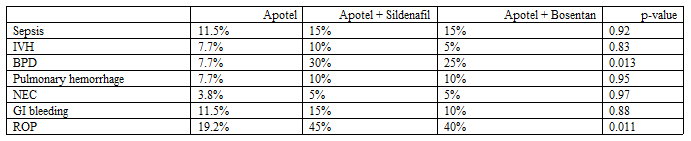
The frequency of BPD and ROP in the Apotel group (7.7 Percentage and 19.2 Percentage, respectively) was significantly lower than that in Apotel + sildenafil group (30 Percentage and 45 Percentage, respectively) and Apotel + bosentan (25 Percentage and 40 Percentage, respectively) groups (p less than 0.05).
Discussion
We designed this clinical trial to find whether co-treatment with Bosentan + Apotel and Sildenafil + Apotel can improve the disease severity in 150 preterm neonates with PDA and PAH who were admitted to the NICU. There was a potential risk of heart failure when the left shunt would rise to the right as the lung pressure decreased. This concern was minimized as the patients were also co-treated with Apotel. Apotel has been used for PDA treatment for several years. For example, in a clinical trial study, Valerio et al. [14] reported the efficacy and safety of Apotel in the treatment of PDA closure in preterms. In another study, Sridharan et al. [15] found that treatment with Apotel (15 mg/kg/dose every 6 hours) was efficacious in 78.2 Percentage of the preterm neonates with PDA. Besides, a lower incidence of hepatotoxicity and AKI was observed after treatment with Apotel in the patients. In addition to Apotel, other drugs such as Bosentan and Sildenafil have also been introduced to control PDA and PAH in preterms. For instance, Zeng et al. [16] demonstrated that Sildenafil therapy is effective and safe for PAH and PDA treatment. In another study, Apostolopoulou et al. [17] showed that bosentan effectively treats PAH. Recent studies have also shown that these drugs can treat other forms of pulmonary heart diseases such as ventricular septal defect and pulmonary atresia [18, 19,20]. We conducted the current survey to find out whether the use of combined therapy with Bosentan + Apotel and Sildenafil + Apotel in ameliorating the PAH would improve the PDA severity or not. We didn't find a significant difference in the mean of echocardiography parameters between all three groups either before or after the intervention. However, our data demonstrated that all three drug classes (Apotel, Apotel + Sildenafil, and Apotel + bosentan) significantly improved echocardiography parameters at the end of the study. This result indicates that treatment with Apotel alone, Apotel + Sildenafil, and Apotel + bosentan has the same effect on improving heart function and pulmonary artery pressure in preterm neonates with PDA though adding these to in PAH treatment have no more positive effect.
In patients with hemodynamically significant PDA, the mechanism of PAH is because of pulmonary overflow. This condition can be similarly seen in VSD patients. The reason that - anti-pulmonary hypertension drugs can be helpful in older VSD patients is that pulmonary overflow causes damage to the arteries and pulmonary arterioles. This process can lead to Eisenmenger if it doesn't control within a maximum of one year. But, in infants with hsPDA, much of the high-pressure flow to the lungs is accompanied by a relative delay in pulmonary artery maturation as long as the duct is open. Once the duct is closed, and the flow is removed, the pressure is relieved. In our study, even in the group where Apotel was administrated, there was still no case of high blood pressure after the duct was closed. We didn't observe certain complications or side effects caused by each drug; however, the frequency of BPD and ROP in the Apotel group was significantly lower than the Apotel + Sildenafil and Apotel + Bosentan groups. Therefore, these findings indicate that treatment with the standard drug, Apotel, is associated with fewer side effects than Sildenafil and Bosentan.
To the best of our knowledge, this is the first study that compared the effects of combined therapies with Apotel + Sildenafil and Apotel + bosentan in improving PAH and PDA in preterm neonates. Most of the available studies have been conducted to investigate the effect of Bosentan and Sildenafil therapies in treating idiopathic PAH in preterm neonates. For example, Maneenil et al. [21] examined the oral administration of bosentan on improving pulmonary hypertension in 38 newborns. They found that Bosentan therapy caused a significant improvement in AaDO2 and SpO2 2 hours after the treatment. The oxygen index was significantly reduced in 47.5 Percentage of neonates who received bosentan after 2 hours. Systolic and diastolic blood pressures didn't show significant changes before and after Bosentan therapy. The mortality rate in neonates was reported to be 12.5 Percentage. Therefore, these researchers concluded that oral administration of bosentan effectively improves oxygenation status in infants with PH without any specific side effects. More recently, Farhangdoust et al. [22] compared the effects of bosentan and Sildenafil in treating persistent PAH in neonates. They found that bosentan was more effective in treating persistent PAH in neonates and reduced the severity of tricuspid valve insufficiency over a shorter period than Sildenafil. In another clinical trial study, Steinhorn et al. [23] investigated the therapeutic effects of bosentan in improving PAH in infants over 34 weeks of age. They observed that bosentan effectively improved oxygenation in infants without affecting systolic and diastolic pressures compared to placebo. However, anemia was found in some infants. The results of this research are somewhat in line with the findings of our survey. In our study, Bosentan and Sildenafil effectively improved the echocardiography index in preterm infants without serious side effects. Mohamed et al. [2] evaluated the effect of bosentan on improving PAH in 47 newborns compared to placebo. They demonstrated that Bosentan administration significantly improved PAH in newborns compared with the placebo group (87.5 Percentage vs. 20 Percentage). No specific side effects were reported in newborns after Bosentan therapy. Thus, they found bosentan as an effective and uncomplicated treatment option for PAH in infants. The results of this study are in line with our research findings. In our research, bosentan improved PAH in infants. A recent meta-analysis study evaluated the effect of Sildenafil in improving the PAH in neonates [24]. The results showed that Sildenafil has a potential role in reducing mortality rate and improving oxygenation in infants with PH, which is in line with our findings.
Similarly, Baquero et al. [25] found that oral administration of Sildenafil (1 mg/kg) significantly improved oxygenation and decreased mortality rate in infants with persistent PH, without a significant effect on blood pressures. More recently, Fatima et al. [26] investigated the effect of Sildenafil (2 mg/kg) alone or in combination with bosentan (1 mg/kg) for improving persistent PH in newborns. They observed that combined therapy with Sildenafil and bosentan significantly reduced TR severity compared to Sildenafil alone. The mean hospital stays in the Sildenafil + bosentan group was markedly lower than neonates in Sildenafil alone group (7.56 days vs. 10.12 days). Therefore, these data indicate that although both drugs positively improve PH in infants, combined therapy with Sildenafil and bosentan exhibited more potent effects. In our study, no significant difference was observed in the efficacy of Sildenafil + Apotel and Bosentan + Apotel in reducing TR severity. In another study, Dardi et al. [27] investigated the effect of Sildenafil, bosentan, and Sildenafil + bosentan on PAH treatment in adult patients. The results of 3-4 months follow-up showed that combined therapy with Sildenafil + bosentan had a more substantial effect in improving PAH, hemodynamic and clinical parameters, and patients' life expectancy compared to those who received bosentan and Sildenafil alone. Therefore, these data emphasize that a combination of bosentan and Sildenafil is more effective in treating PAH. In our study, combined therapy with sildenafil + bosentan was not investigated, but we didn't find a significant difference in Sildenafil + Apotel, bosentan + Apotel's efficacy, and Apostel alone. Therefore, according to the results of our research and previous accomplished data, oral administration of Sildenafil and bosentan has similar efficacy without serious side effects in the treatment of PAH in preterm infants.
Conclusion
In summary, our findings showed that oral administration of Sildenafil and bosentan improves cardiac index without serious side effects in preterm infants PAH and PDA. Although BPD and ROP were among the most common side effects caused by Apotel + Sildenafil and Apotel + Bosentan, no difference was observed in the effectiveness of these drugs in treating the disease. Both Apotel + Sildenafil and Apotel + Bosentan groups exhibited similar efficacy as Apotel in treating PAH and PDA in preterm infants. So pulmonary antihypertensive administration in hs-PDA, even in developed symptoms, do not suggested and monotherapy with apotel seems sufitient.
Small sample size and short follow-up might be the limitations of this study. Future clinical trial studies with larger samples and long-term follow-up on term or near-term neonates are recommended.
Declarations
Ethics approval and consent to participate: All methods were performed in accordance with the Declaration of Helsinki (the Ethics Committee of the Iran University of Medical Sciences approved the study (IR.IUMS.FMD.REC.1399.430)). legal guardians accomplished informed consent.
Consent for publication
Not applicable
Availability of data and materials
The datasets generated during and/or analyzed during the current study are available from the corresponding author on reasonable request.
Competing interests
The authors declare that they have no competing interests.
Funding
There is no funding support.
Authors' contributions
A.B. and C.D. wrote the main manuscript text and E. collect the data. All authors reviewed the manuscript.
Acknowledgements
Not applicable.
References
- Ali ZS et al. (2013). Predictors of bronchopulmonary dysplasia and pulmoanry hypertension in newborn children. Danish Medical Journal. 60(8):1–5.
View at Publisher | View at Google Scholar - Mohamed WA et al. (2012). A randomized, double-blind, placebo-controlled, prospective study of bosentan for the treatment of persistent pulmonary hypertension of the newborn. J Perinatol. 32(8):608-613.
View at Publisher | View at Google Scholar - Delsing B et al. (2007). Risk of persistent pulmonary hypertension of the neonate in twin-to-twin transfusion syndrome. Neonatology. 92(2): 134-138.
View at Publisher | View at Google Scholar - Wedgwood S, Steinhorn RH, Lakshminrusimha S. (2019). Optimal oxygenation and role of free radicals in PPHN. Free radical biology & medicine. 142:97-106.
View at Publisher | View at Google Scholar - Gabbay E et al. (2007). Review of bosentan in the management of pulmonary arterial hypertension. Vasc Health Risk Manag. 3(6): 887–900.
View at Publisher | View at Google Scholar - Aswani R et al. (2015). Oxygen requirement as a screening tool for the detection of late pulmonary hypertension in extremely low birth weight infants. Cardiology in the young.1–7.
View at Publisher | View at Google Scholar - Mourani PM et al. (2015). Pulmonary Hypertension and Vascular Abnormalities in Bronchopulmonary Dysplasia. Clin Perinatol. 42(4):839-855.
View at Publisher | View at Google Scholar - Mourani PM, et al. (2015). Early pulmonary vascular disease in preterm infants at risk for bronchopulmonary dysplasia. American journal of respiratory and critical care medicine. 191(1):87–95.
View at Publisher | View at Google Scholar - O’Connor MG, et al. (2016). PULMONARY HYPERTENSION IN THE PREMATURE INFANT: A CHALLENGING COMORBIDITY IN A VULNERABLE POPULATION. Curr Opin Pediatr. 28(3): 324–330.
View at Publisher | View at Google Scholar - Sabri MR et al. (2014). Comparison of the therapeutic and side effects of tadalafil and sildenafil in children and adolescents with pulmonary arterial hypertension. Pediatr Cardiol. 35(4): 699-704.
View at Publisher | View at Google Scholar - Barnett CF et al. (2016). Sildenafil in the treatment of pulmonary hypertension. Vasc Health Risk Manag. 2(4): 411–422.
View at Publisher | View at Google Scholar - Galie N et al. (2005). Sildenafil citrate therapy for pulmonary arterial hypertension. N Engl J Med. 353(20): 2148-2157.
View at Publisher | View at Google Scholar - Humbert M et al. (2004). Combination of bosentan with epoprostenol in pulmonary arterial hypertension: BREATHE-2. Eur Respir J. 24(3):353-359.
View at Publisher | View at Google Scholar - Valerio E, Valente MR, Salvadori S, Frigo AC, Baraldi E et al. (2016). Intravenous paracetamol for PDA closure in the preterm: a single-center experience. European journal of pediatrics. 175(7):953-966.
View at Publisher | View at Google Scholar - Sridharan K, Al Jufairi M, Al Ansari E, Al Marzooq R, Hubail Z, et al. (2021) Intravenous acetaminophen (at 15 mg/kg/dose every 6 hours) in critically ill preterm neonates with patent ductus arteriosus: A prospective study. Journal of clinical pharmacy and therapeutics. 46(4):1010-1019.
View at Publisher | View at Google Scholar - Zeng WJ, Lu XL, Xiong CM, Shan GL, Liu ZH, et al. (2011). The efficacy and safety of sildenafil in patients with pulmonary arterial hypertension associated with the different types of congenital heart disease. Clinical cardiology. 34(8):513-518.
View at Publisher | View at Google Scholar - Apostolopoulou SC, Manginas A, Cokkinos DV, Rammos S. (2007). Long-term oral bosentan treatment in patients with pulmonary arterial hypertension related to congenital heart disease: a 2-year study. Heart (British Cardiac Society). 93(3):350-354.
View at Publisher | View at Google Scholar - Kaneko Y, Achiwa I, Kondo R, Takei T. (2019). [Total Repair of Pulmonary Atresia, Ventricular Septal Defect, and Major Aorto-pulmonary Collateral Arteries That were Deemed Unrepairable in an Adolescent and Adults]. Kyobu geka The Japanese journal of thoracic surgery. 72(4):263-268.
View at Publisher | View at Google Scholar - Martínez-Quintana E, Rodríguez-González F, Medina-Gil JM, Agredo-Muñoz J, Nieto-Lago V. (2010). Clinical outcome in Down syndrome patients with congenital heart disease. Cirugia y cirujanos. 78(3):245-250.
View at Publisher | View at Google Scholar - Bialkowski A, Moenkemeyer F, Patel N. (2015). Intravenous sildenafil in the management of pulmonary hypertension associated with congenital diaphragmatic hernia. European journal of pediatric surgery: official journal of Austrian Association of Pediatric Surgery [et al] = Zeitschrift fur Kinderchirurgie. 25(2):171-176.
View at Publisher | View at Google Scholar - Maneenil G et al. (2017). Effect of Bosentan Therapy in Persistent Pulmonary Hypertension of the Newborn. Pediatrics & Neonatology. 4:1-26.
View at Publisher | View at Google Scholar - Farhangdoust S, Mehralizadeh S, Bordbar A. (2020). Comparison of the effects of bosentan and sildenafil in the treatment of persistent pulmonary arterial hypertension in infants. Journal of Clinical Neonatology. 9(4):249-254.
View at Publisher | View at Google Scholar - Steinhorn RH et al. (2016). Bosentan as Adjunctive Therapy for Persistent Pulmonary Hypertension of the Newborn: Results of the Randomized Multicenter Placebo-Controlled Exploratory Trial. J Pediatr. 177:90-96e3.
View at Publisher | View at Google Scholar - Kelly LE et al. (2017). Sildenafil for pulmonary hypertension in neonates. Cochrane Database Syst Rev. 8:CD005494.
View at Publisher | View at Google Scholar - Baquero H et al. (2006). Oral sildenafil in infants with persistent pulmonary hypertension of the newborn: a pilot randomized blinded study. Pediatrics. 117(4):1077-1083.
View at Publisher | View at Google Scholar - Fatima N et al. (2018). Comparison Of The Efficacy Of Sildenafil Alone Versus Sildenafil Plus Bosentan In Newborns With Persistent Pulmonary Hypertension. J Ayub Med Coll Abbottabad. 30:333-336.
View at Publisher | View at Google Scholar - Dardi F, Manes A, Palazzini M, Bachetti C, Mazzanti G et al. (2015). Combining bosentan and sildenafil in pulmonary arterial hypertension patients failing monotherapy: real-world insights. The European respiratory journal.46(2):414-421.
View at Publisher | View at Google Scholar
