

Commentary | DOI: https://doi.org/10.31579/2834-796X/006
Commentary on the use of Magnesium Sulphate in Hypoxic Ischaemic Encephalopathy in the Newborn in Low-Middle-Income Countries (LMIC)
*Corresponding Author: Khalid N. Haque, FRCPCH, FRCP (Lond, Edin, Ire) DCH (Lond), MBA, DTM&H Visiting Faculty Professor University of Child Health sciences The Children’s Hospital, Lahore.
Citation: Richmond Ronald Gomes (2022). Commentary on the use of Magnesium Sulphate in Hypoxic Ischaemic Encephalopathy in the Newborn in Low-Middle-Income Countries (LMIC). International Journal of Cardiovascular Medicine, 1(1) DOI:10.31579/2834-796X/006
Copyright: © 2022 Khalid N. Haque, This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 26 September 2022 | Accepted: 05 October 2022 | Published: 11 October 2022
Keywords: hypoxic ischaemic; encephalopathy; low-middle-income countries
Abstract
Whole body hypothermia is now standard therapy for severe hypoxic-ischaemic encephalopathy (HIE) in economically advanced countries. However, similar benefits have not been evident from many small and the very large multinational Helix study
Introduction
Whole body hypothermia is now standard therapy for severe hypoxic-ischaemic encephalopathy (HIE) in economically advanced countries. However, similar benefits have not been evident from many small and the very large multinational Helix study [1, 2]. This has lead to rejuvenation of interest in the therapeutic use of other modalities including Magnesium Sulphate (MgSO4 ) as a neuroprotective therapy for HIE in low-middle-income countries.
It is estimated that around 80 to 120,000 neonates either suffer from or die from HIE every year and more than 80% of these deaths occur in LMICs. In addition to the large number of deaths nearly 50% of babies who survive (even after total body hypothermia) suffer from neuro-developmental disorders making HIE a significant public health issue with heavy burden of care on the state and the affected families.
Magnesium sulphate (MgSO4) has been used in obstetric practice since 1925 to control eclamptic seizures, its pharmacokinetics, safety profile are well known. It is cheap and universally available. As, an incidental finding antenatal MgSO4 therapy was found to be associated with modest effect on reducing cerebral palsy and motor dysfunction in premature infants [3]. The exact mechanism by which MgSO4 confers neuroprotection is unclear [4]
The process leading to HIE are heterogeneous starting either preconceptionally or in the antepartum period. It is now recognized that there are two distinct periods when neuronal damage occurs. The immediate (primary) hypoxic insult followed by a latent period and then profound and a much longer period of secondary neuronal damage due to the release of chemical mediators and calcium gating mechanisms and failure of auto-regulatory mechanism that causes cerebral ischemia, neuronal cell hypoxia and intracellular energy failure (primary energy failure). This is due to release of inhibitory neurotransmitters like GABA (Gamma Amino Butyric Acid) as a protective mechanism to decrease oxygen demand of neuronal cells and minimize the effects of hypoxia.
Secondary energy failure; This is believed to be due to oxygen free radical production; intracellular calcium entry into the cells (gating mechanism) and increased apoptosis and neuronal cell death (necroptosis).
Magnesium Sulphate, is thought to act by reducing neuronal excitotoxicity. Secondary neuronal injury is due to accumulation of excessive amounts of intra-neuronal calcium as a result of excitatory amino acid stimulation of the N-methyl-D-aspartate (NMDA) cell receptors. It is hypothesised that Magnesium ion gates the NMDA channels in a voltage-dependent manner and protect the brain from NMDA receptor-mediated injury. It has also been suggested that magnesium sulphate may be neuro-protective by other mechanism e.g., anti-excitotoxic, antioxidant, anti-cytokine and antiplatelet effects.
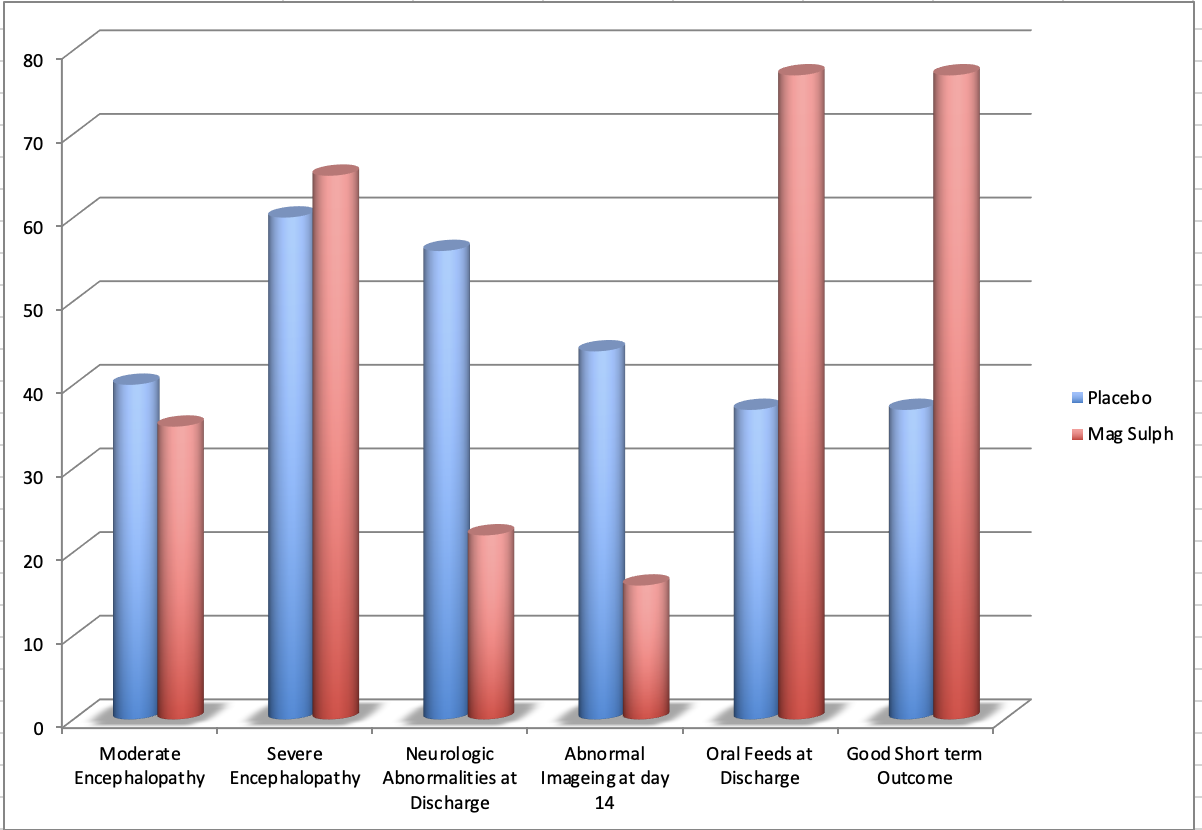
A small number of human studies that have been published have reported either the effect of antenatal magnesium sulphate on the newborn or when magnesium sulphate has been given in association with hypothermia [5]. The studies from high income countries suggest that Magnesium Sulphate in HIE has short term beneficial effect which is lost by school age [6]. However, Bhatt, Gathwala [7-9] from LMIC have shown clear good short term outcome outcome following magnesium sulphate therapy following birth asphyxia (Figure 1).
A small pragmatic study from Pakistan [9] concluded “ Postnatal magnesium sulphate therapy appears to be neuroprotective in term/near term neonates with moderate to severe birth asphyxia in terms of seizure control, duration of stay and initiation of feeding. However, no improvement was seen as regards mortality, cranial USG changes and long-term neurodevelopmental outcome”.
Taking all the human studies from high and LMIC countries of magnesium sulphate therapy in HIE further large multicentre randomised controlled trails are warranted to determine the efficacy of MgSO4, optimal dose, duration, timing and safety along with long-term functional outcomes and its neuroprotective ability in neonatal hypoxic ischaemic encephalopathy.
Khalid N. Haque, FRCPCH, FRCP (Lond, Edin, Ire) DCH (Lond), MBA, DTM&H Visiting Faculty Professor University of Child Health sciences The Children’s Hospital, Lahore
References
- Montaldo P et al. Hypothermic Neuroprotection for Neonatal Encephalopathy in Low-Middle-Income Countries: A New Approach to an Old Problem. Neoreviews 2018; 19(12): e735-741
View at Publisher | View at Google Scholar - Thayyil S et al. Hypothermia for moderate or severe neonatal encephalopathy in low-income and middle-income countries (HELIX): a randomized controlled trial in India, Sri Lanka and Bangladesh. Lancet Global Health. Doi.org/10.1016/S2214-109X(21)00274-3
View at Publisher | View at Google Scholar - Doyle LW et al. Antenatal magnesium sulphate and neurologic outcome in preterm infants: a systematic review. Obstet Gynecol. 2009; 113:1327–33. doi: 10.1097/AOG.0b013e3181a60495
View at Publisher | View at Google Scholar - Galinsky R et al. Magnesium is not consistently neuroprotective for perinatal hypoxia- ischemia in term-equivalent models in preclinical studies: a systematic review. Dev Neurosci. 2014; 36:73–82. doi: 10.1159/000362206
View at Publisher | View at Google Scholar - Galinsky R et al. A systematic review of Magnesium Sulfate for Perinatal Neuroprotection: What have we learnt from the past decade? Frontiers in Neurology 2020; 11:449: doi: 10.3389/fneur.2020.00449.
View at Publisher | View at Google Scholar - Chollat C et al. School-age outcomes following a randomized controlled trial of magnesium sulfate for neuroprotection of preterm infants. J Pediatr. (2014) 165:398– 400.e393. doi: 10.1016/j.jpeds.2014.04.007
View at Publisher | View at Google Scholar - Bhat MA, et al.: Magnesium sulfate in severe perinatal asphyxia: a randomized, placebo-controlled trial. Pediatrics. 2009, 123:764-9. 10.1542/peds.2007-3642
View at Publisher | View at Google Scholar - Bhatt a, et al. Magnesium sulfate in severe perinatal birth asphyxia: A randomised placebo-controlled trial. Obstetrical & Gynecological Survey: September 2009 - Volume 64 - Issue 9 - p 573-574 doi: 10.1097/01.ogx.0000358028.38402.ff
View at Publisher | View at Google Scholar - Gathwala G, et al.: Magnesium for neuroprotection in birth asphyxia. J Pediatr Neurosci. 2010, 5:102-4. 18.10.4103/1817-1745.76094
View at Publisher | View at Google Scholar - Iqbal N, et al. The neuro-protective efficacy of post-natal magnesium sulphate in term or near term infants with moderate to severe birth asphyxia. Cureus 2021; 13(8): e16826. DOI 10.7759/cureus.16826
View at Publisher | View at Google Scholar
