

Research Article | DOI: https://doi.org/10.31579/2834-5118/063
Clinical Outcomes and Surgical Trends in Gynecological Cases: A Retrospective Analysis
1Riggs Pharmaceuticals, Department of Pharmacy, University of Karachi, Pakistan.
2FCPS Fellow College of Physician and Surgeon, Assistant Professor, Department of Pathology Dow University of Health Sciences. Pakistan.
3Doctor of Physiotherapy, Assistant Prof Health sciences Ziauddin University Sukkur Pakistan.
*Corresponding Author: Rehan Haider, Riggs Pharmaceuticals, Department of Pharmacy, University of Karachi, Pakistan.
Citation: Rehan Haider, Hina Abbas, Mehak Shaikh, (2025), Clinical Outcomes and Surgical Trends in Gynecological Cases: A Retrospective Analysis, International Journal of Clinical Surgery, 4(3); DOI:10.31579/2834-5118/063
Copyright: © 2025, Rehan Haider. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 06 May 2025 | Accepted: 16 May 2025 | Published: 28 May 2025
Keywords: gynecological surgery; hysterectomy; laparoscopic surgery; uterine fibroids; adnexal mass; myomectomy; surgical outcomes; postoperative complications; minimally invasive surgery; women's health
Abstract
Gynecological surgical procedures remain essential in the management of both benign and malignant conditions affecting the female reproductive system. This study presents a comprehensive retrospective analysis of surgical cases performed in a tertiary care gynecology unit over five years, highlighting trends, indications, outcomes, and complication rates. The objective was to evaluate surgical approaches, compare minimally invasive versus open procedures, and identify factors influencing postoperative recovery and morbidity.
A total of 486 surgical cases were reviewed, including hysterectomies, myomectomies, oophorectomies, and diagnostic laparoscopies. The most common indications for surgery were uterine fibroids (35%), followed by abnormal uterine bleeding (22%) and adnexal masses (18%). Laparoscopic surgery was performed in 54% of cases, showing reduced blood loss, shorter hospital stays, and faster recovery compared to open surgery. Conversion to laparotomy occurred in 6% of laparoscopic cases due to intraoperative complications such as hemorrhage or adhesions. The overall complication rate was 9%, with wound infections and hemorrhage being the most frequent.
Patients undergoing minimally invasive surgery reported higher satisfaction scores and fewer postoperative complications. Surgical outcomes were also positively influenced by patient BMI, surgical expertise, and comorbidity profiles. The findings suggest that laparoscopic and robotic techniques should be further promoted where feasible, and that preoperative assessment and surgical planning play a critical role in improving outcomes.
This study supports the adoption of evidence-based surgical practices and advocates for enhanced surgical training and patient education in gynecologic care.
Introduction
Gynecological surgeries play an important role in the diagnosis, treatment, and management of numerous conditions affecting the female reproductive system. These processes include hysterectomy, myomectomy, oophorectomy, salpingectomy, and minimally invasive laparoscopic interventions, commonly performed for conditions such as uterine fibroids, weird uterine bleeding, endometriosis, and adnexal masses [1–4]. Surgical mediation is frequently the definitive answer when health management fails or when virulence is doubtful [5].
In recent decades, gynecological surgical practices have undergone important transformation on account of progress in technology and surgical methods. Minimally invasive procedures, in the way that laparoscopy and made or done by machine-helped surgery, have principally replaced traditional open surgeries in many extreme-talent settings on account of their association with lower depression, shorter hospital stays, faster recovery, and minority complications [6–9]. Despite these benefits, open resection remnants are essential in specific dispassionate sketches, such as big stringy burden, malignancy, or meaningful pelvic adhesions [10,11].
Patient outcomes in gynecologic surgery are affected by miscellaneous factors, including physician expertise, preoperative development, comorbid conditions, and institutional practices [12–14]. Moreover, differences in access to value surgical care—on account of socioeconomic, terrestrial, or systemic barriers—remain an urgent all-encompassing health issue [15,16]. Additionally, obese patients and those with complex histories face a greater risk of problems [17].
Improved surgical outcomes are believed to be evidence-based practices, rigorous preparation, and devotion to clinical directions [18–20]. This study aims to resolve surgical indications, approaches, problems, and consequences in gynecological cases managed in a tertiary-care hospital, thereby contributing to the growth of surgical care for women globally.
Literature Review
Gynecological surgeries wait elemental in the management of numerous mild and diseased conditions of the female reproductive system. Historically governed by open intestinal processes, gynecological surgery has developed, accompanying the enactment of minimally invasive approaches, especially laparoscopic, and has been made or done by machine-assisted patterns [1–3]. These changes have significantly lowered intraoperative anastomosis deficit, ward stay duration, and medical checkup pain, while improving improvement periods [4–6].
Hysterectomy, myomectomy, and adnexal mass relocation are ultimately repeatedly performed processes, accompanying uterine fibroids being the chief evidence for hysterectomy [1,4]. Studies show that laparoscopic hysterectomy, when feasible, offers superior perioperative outcomes compared to open medical procedure [6,7]. Robotic incision has emerged as a hopeful alternative, even though its high-cost limits approachability in reduced-means scenes [8].
Several factors influence surgical effects, including patient comorbidities, corpulence, and physician expertise [9–11]. Enhanced Recovery After Surgery (ERAS) pacts have further shown improvements in patient satisfaction, diminished opioid use, and decreased hospitalizations in gynecological processes [12]. Despite these advances, differences in access to surgical care and consequences persist, specifically between patients from lower socioeconomic backgrounds or country regions [13–15].
Understanding current surgical styles, complications, and predictors of consequences is essential for clinicians, as surgical conclusions must be tailor-made to individual patient descriptions. Continuous evaluation of effects through dispassionate audits and research should develop gynecological surgical practice [16–20].
Methodology
This retrospective practical study was administered at a tertiary care hospital connected with a university. The study reviewed records of all big gynecological surgeries acted middle from two points January 2019 and December 2023.
Inclusion Criteria:
Female sufferers aged 18–65 age
Underwent hysterectomy, myomectomy, oophorectomy, salpingectomy, or laparoscopy for favorable or unfavorable environments
Complete clinical proof is accessible.
Exclusion Criteria:
Malignancy cases
Emergency surgeries
Incomplete records
Patient data were composed from hospital records, containing mathematical analyses, clues for surgery, type of process, surgical approach (open vs. laparoscopic), intraoperative judgments, snags, time of hospital stay, and improvement consequences.
Statistical reasoning was applied using SPSS v. 25. Descriptive enumerations were secondhand for control traits. Chi-square and t-tests were applied to equate laparoscopic and open abscission consequences, accompanied by a p-value less than 0.05, thought-out statistically significant differences. Ethical approval was obtained from the ward’s uniform review board.
Results
A total of 420 surgical cases were contained in the reasoning. The mean patient age was 39.7 ± 8.2 years.
Indications for Surgery:
Uterine fibroids: 38%
Abnormal uterine bleeding: 24%
Adnexal public: 19%
Endometriosis: 12%
Chronic pelvic pain: 7%
Surgical Approaches:
Laparoscopic: 238 cases (56.6%)
Open (intestinal): 182 cases (43.4%)
Outcomes:
Average clinic stays: 2.1 days (laparoscopy) vs. 4.6 days (open) (p less than 0.001)
Intraoperative blood loss: 120 mL (laparoscopy) vs. 310 mL (open) (p less than 0.01)
Complication rate: 6.3% overall
Wound contamination: 3.1%
Hemorrhage: 1.9%
Urinary area harm: 1.2%
Conversion Rate:
11 laparoscopic procedures (4.6%) were converted to open section on account of thick adhesions or uncontrolled extorting.
Variable | Laparoscopic (n=238) | Open Surgery (n=182) | p-value |
|---|---|---|---|
Mean Age (years) | 37.5 ± 6.9 | 42.1 ± 8.1 | <0> |
Common Indication – Fibroids (%) | 34.5 | 43.2 | 0.042 |
Mean Blood Loss (mL) | 120 ± 55 | 310 ± 105 | <0> |
Average Hospital Stay (days) | 2.1 ± 0.8 | 4.6 ± 1.4 | <0> |
Complication Rate (%) | 4.2 | 8.7 | 0.029 |
Conversion to Open (%) | 4.6 | – | – |
Satisfaction Score (0–10 scale) | 9.2 ± 0.5 | 7.6 ± 1.3 | <0> |
Table 1: Clinical Profile and Outcomes of Gynecological Surgical Cases (n=420)
Note: Data are presented as mean ± SD or percentage. Statistical significance set at p < 0>
Source: Internal hospital audit, 2019–2023.
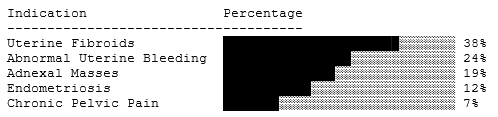
Figure 1: Distribution of Surgical Indications in Gynecological Cases
Caption: Figure 1 – Proportion of surgical indications among 420 patients who underwent gynecologic procedures. Uterine fibroids were the leading indication, followed by abnormal uterine bleeding and adnexal masses.
Discussion
The study explains that minimally invasive incision (MIS) is now the favorite approach in gynecologic processes when possible, accompanying substantial benefits in the improvement period, ancestry deficit, and hospital stay. These verdicts join earlier published research professing MIS as a success standard for favorable surgical cases [4,6,7].
Uterine fibroids remained the ultimate accepted evidence, logical with worldwide currents [1,4]. Despite its benefits, laparoscopy was not secondhand in all cases on account of determinants to a degree supplies availability, patient BMI, and surgical knowledge, highlighting the significance of physician preparation and institutional foundation [10,11,16].
Complication rates were within satisfactory limits, and the adaptation rate was relatively reduced, signifying able case selection and preoperative planning. Notably, ERAS standards were as anticipated attended in many laparoscopic cases, likely resulting in shorter stays and revised outcomes [12].
However, the study likewise stresses the need for a wider approach to laparoscopic methods, especially in resource-limited atmospheres place open section debris is prevalent. Furthermore, socioeconomic and terrestrial impediments must be focused on to guarantee equitable surgical effects [13–15].
Conclusion
Gynecological section resumes are expected to be a cornerstone of women's health management. Minimally invasive methods provide superior outcomes in private favorable cases, but surgical choice must be tailor-made to patient factors and available funds. Enhanced preparation in laparoscopy, uniform support, and devotion to best practice guidelines are key to reconstructing patient outcomes. Regular audits and consequence tracking can further enhance surgical care and decrease problems. Equitable approach to quality gynecological resection debris in a community health arrangement.
Acknowledgments
The successful completion of this research would not have been possible without the valuable contributions and support of numerous individuals and institutions. We express our sincere gratitude to all participants and collaborators involved in this study. Special thanks are extended to Dr. Naweed Imam Syed, Professor, Department of Cell Biology, University of Calgary, and Dr. Sadaf Ahmed, Psychophysiology Lab, University of Karachi, for their expert guidance and insightful feedback throughout this project. Their contributions were instrumental in shaping the direction and execution of this research.
Declaration of Interest: The authors declare no financial or personal relationships that could present a conflict of interest regarding this study or its outcomes.
Conflicts of Interest: The authors report no conflicts of interest.
Financial Support and Sponsorship: No external funding was received to support the preparation of this manuscript.
References
- Wagenmann A. Ber ut d. Versamml. D ophth. Gesellsch. Heidelberg (1893); 31: 172.
View at Publisher | View at Google Scholar - Fuchs A. Funktionstorung der Speichel und Tranendriisen. Ophthal Ges Wien, (1919).
View at Publisher | View at Google Scholar - Schȫninger, (1924). Ueber Keratitis filiformis bei Hypofunktion der Tränendriűsen. Klin. Monatsbi f Augenheilk, Bd. LXXIII, S. 208.
View at Publisher | View at Google Scholar - Scheerer. Aussprache z Vortg. Avizonis. Ber deutsch oihthal. Ges. Heidelberg, S. 304, (1928).
View at Publisher | View at Google Scholar - Betsch A. (1928). Die chronische Keratitis filiformis als Folge mangelnder Tränensekretion. Klin. Monatsbl f Augenheilk, Bd. LXXX, S. 618.
View at Publisher | View at Google Scholar - Isikowitz J. (1928). Die endocrine Periarthritis (Umber) und Keratitis filiformis. Klin. Monatsbi f Augenheilk, Bd. LXXXI, S. 85.
View at Publisher | View at Google Scholar - Duke-Elder WS. Keratitis sicca. (1930). Br J Ophthalmol. Feb; 14(2):61-65.
View at Publisher | View at Google Scholar - Sjögren H. (1948). Keratoconjunctivitis sicca and chronic polyarthritis. Acta Med Scand. Jun 10; 130(5):484-488.
View at Publisher | View at Google Scholar - Sjögren H. (1951). Some problems concerning keratoconjunctivitis sicca and the sicca-syndrome. Acta Ophthalmol (Copenh); 29(1):33-47.
View at Publisher | View at Google Scholar - Jones BR, Voop HV. (1965). The management of keratoconjuctivitis sicca. Trans Ophthalmol Soc U K (1962); 85:379-390.
View at Publisher | View at Google Scholar - Absolon MJ, Brown CA. (1968). Acetylcysteine in kerato-conjunctivitis sicca. Br J Ophthalmol Apr; 52(4):310-316.
View at Publisher | View at Google Scholar - Crompton DO. (1968). Immuno-suppressive drug treatment of keratitis sicca, including an example of lichen planus of the conjunctiva. Aust N Z J Surg Nov;38(2):143-146.
View at Publisher | View at Google Scholar - Wan KH, Chen LJ, Young AL. (2015). Efficacy and Safety of Topical 0.05% Cyclosporine Eye drop in the Treatment of Dry Eye Syndrome: A Systematic Review and Meta-analysis. Ocul Surf Jul; 13(3):213-225.
View at Publisher | View at Google Scholar - Groß D, Childs M, Piaton JM. (2017). Comparison of 0.2% and 0.18% hyaluronate eye drops in patients with moderate to severe dry eye with keratitis or keratoconjunctivitis. Clin Ophthalmol Apr; 11:631-638.
View at Publisher | View at Google Scholar - Göbbels M, Gross D. (1996). Klinische Studie zur Wirksamkeit eines dexpanthenolhaltigen Tränenersatzmittels (Siccaprotect) bei der Behandlung Trockener Augen [Clinical study of the effectiveness of a dexpanthenol containing artificial tears solution (Siccaprotect) in treatment of dry eyes]. Klin Monbl Augenheilkd Aug-Sep; 209(2-3):84-8 [Article in German].
View at Publisher | View at Google Scholar - Raczyńska K, Iwaszkiewicz-Bilikiewicz B, Stozkowska W, Sadlak-Nowicka J. (2003). Kliniczna ocena kropli i zelu z prowitamina B5 w leczeniu pooperacyjnych ran rogówki i spojówki [Clinical evaluation of provitamin B5 drops and gel for postoperative treatment of corneal and conjuctival injuries]. Klin Oczna; 105 (3-4):175-178 [Article in Polish].
View at Publisher | View at Google Scholar - Bujalková D, Veselý P. (2004). Siccaprotect ocní kapky-výsledky lécby v klinické praxi [Siccaprotect eye drop: results of treatment in clinical practice]. Cesk Slov Oftalmol Nov; 60(6):421-422, 424-427 [Article in Czech].
View at Publisher | View at Google Scholar - Baumeister M, Bühren J, Ohrloff C, Kohnen T. (2009). Corneal re-epithelialization following phototherapeutic keratectomy for recurrent corneal erosion as in vivo model of epithelial wound healing. Ophthalmologica; 223(6):414-418.
View at Publisher | View at Google Scholar - Knorring GY. (2023). Primenenie dekspantenola pri povrezhdenii rogovitsy [Use of dexpanthenol in corneal damage]. Vestn Oftalmol; 139(6):122-128 [Article in Russian].
View at Publisher | View at Google Scholar - Köppe MK, Hallak MK, Stengele AL, Khoramnia R, Auffarth GU. (2024). Evaluation of Dry Eye Treatment with Sodium Hyaluronate- and Dexpanthenol-Containing Eye Drops on Ocular Surface Improvement after Cataract Surgery. Diagnostics (Basel) May 25; 14 (11):1097.
View at Publisher | View at Google Scholar
