

Review Article | DOI: https://doi.org/10.31579/2835-7949/019
Clinical Anatomy of the Pelvis and Reproductive Tract
1Riggs Pharmaceuticals Department of Pharmacy, University of Karachi, Pakistan.
2Head of department of Pharmacology Fazaia Ruth Pfau Medical College Air University, Karachi, Pakistan.
3GD Pharmaceutical Inc OPJS University Rajasthan, India.
4Assistant Professor Dow University of Health Sciences Karachi, Pakistan.
5Associate Professor, Department of Pathology Dow University of Health Sciences, Karachi, Pakistan.
*Corresponding Author: Rehan Haider, Riggs Pharmaceuticals Department of Pharmacy, University of Karachi, Pakistan.
Citation: Rehan Haider, Asghar Mehdi, Geetha Kumari Das, Zameer Ahmed, Sambreen Zameer., (2024), Clinical Anatomy of the Pelvis and Reproductive Tract, Biomedical Research and Clinical Trials,3(4); DOI: 10.31579/2835-7949/019
Copyright: © 2024, Rehan Haider. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 02 August 2024 | Accepted: 12 August 2024 | Published: 23 August 2024
Keywords: Pelvis; Reproductive Tract; Clinical Anatomy; Diagnosis; Treatment; Pathology.
Abstract
A deep understanding of the clinical plants having to do with the stomach and generative tract is essential for healing experts complicated in the disease and treatment of connected environments. The stomach comprises a pivotal physical domain home to a myriad of essential structures, containing cartilages, influences, hysteria, and organs important for bodily functions and duplication. This abstract aims to concisely outline the key anatomical systems inside the stomach and generative tract, stressing their dispassionate meaning.
Comprising the pelvic cartilages, sacrum, and lower back, the stomach forms a strong foundation that supports the weight of the superior material and specifies affection sites for muscles and ligaments. Within this foundation occupy essential pelvic tools in the way that the bladder, rectum, and generative makeups contain the uterus, ovaries, and fallopian tubes in females and the prostate gland and generative vesicles in men.
The dispassionate consequences of pelvic anatomy span a general range of environments, ranging from mild to malignant. Disorders to a degree such as pelvic instigative ailment, endometriosis, ovarian cysts, and prostate malignancy often require an inclusive understanding of pelvic plants for exact diagnosis and situational preparation. Furthermore, the elaborate interaction between pelvic buildings and adjacent means can give rise to applied pain patterns and sitting challenges to disease.
In summary, an all-encompassing grasp of the clinical plants concerning the stomach and generative tract is necessary for healthcare experts across different concentrations. By elucidating the complex friendships between two points of physical makeup and their pathological proofs, this information helps the transmission of optimal patient care and embellishes dispassionate effects.
Introduction
This study aims to summarize the important aspects of the plants of the belly and the stomach that endure be popular with obstetric or gynecological scholars. Many of the examinations and situations we order on a constantly base demand good bodily information orderly expected correctly assumed.
Surface plants The prior abdominal wall can be detached into four quadrants by lines passing across and across through the umbilicus (Fig. 1.1). In the upper abdomen is the large stomach, that is the region just inferior to the xiphisternum, and in the lower tummy lie the right and abandoned iliac fossae and the hypogastrium. The cutaneous nerve supply of the beginning intestinal divider stands from the prior rami of the lower thoracic and lumbar vertebral column. The dermatomes of meaningful makeups on the prior abdominal wall are:
T7 xiphisternum
T10 umbilicus
L1 symphysis pubis
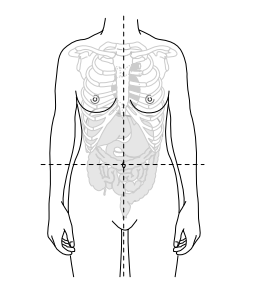
Fig. 1.1 The abdomen can be divided into quadrants
The ancestry supply is by way of the superior epigastric (arm). of the international channel) and the inferior epigastric (arm of the extrinsic iliac channel) ships. During laparoscopy, the inferior epigastric containers may be visualized between the upper front of the body and rectus power at the beginning
abdominal wall and launch their journey of the highest quality from nearly two, the third step in the baseball diamond of the habit ahead of the inguinal bond tighter to the symphysis pubis. Care needs to be expected to be captured to prevent bureaucracy while utilizing accessory trochars all the while laparoscopy and to ensure that they are recognized when making a May lard cut of theintestinal wall
The anterior abdominal wall
The prior intestinal obstruction Beneath the skin and the fat of the superficial anterior
abdominal walls are a covering and association of muscles containing the rectus abdominus, extrinsic and evasive, and transversal powers (Fig. 1.2). Where these influences blend in the midline, the linea alba is made. Pyramidalis influence is present in the principal part of mother Orig, urinating on the beginning surface of the pubis and putting into the linea alba. The exact arrangement of the powers confronted by a physician depends on accurately the place some slit is fashioned.
The umbilicus
The umbilicus is a scar from the vestiges of the main rope. It is located in the linea alba and has a changing position contingent upon the corpulence of the patient. However, the base of the umbilicus is continually the finest one in the beginning abdominal wall and is the low treatment of psychotic states with electrical shock home of the insert of the basic traffic in laparoscopy.
The urachus is the debris of the allantois from the unborn young and runs from the top of the pouch to the umbilicus
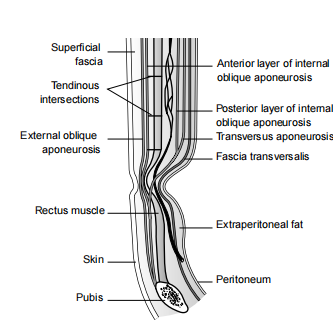
Fig. 1.2 The layers of the anterior abdominal wall in tranverse section
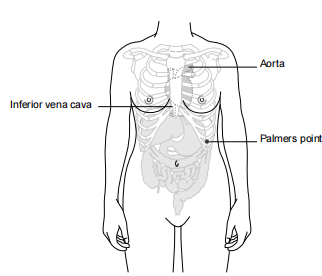
Fig. 1.3 The umbilicus in relation to the underlying vasculature in a thin patient.
Epithelium of the genital tract
Occasionally, this can wait for newborns. In early embryological existence, the vitelline channel too wastes the umbilicus from the cultivating midgut. Although the pipe is dissociated long before childbirth, a piece concerning this form is found in 2% of the culture as aMeckels diverticulum.
The aorta divides into the coarse iliac channels approximately 1–2 cm beneath the umbilicus private slenderize mothers (Fig. 1.3). The prevalent iliac veins connect to form the inferior vena cava just beneath this as well these makeups There is potential for the laparoscopist to put ports at the umbilicus. Epithelium of the area of the organ The beginning intestinal divider containing the organs, vulva and perineal districts are interlined accompanying squamous epithelium.
The epithelium interlining the endocervix and uterine crater is tubular and the squamocolumnar connection regularly stands at the ectocervix in wives of generative age.
This is the main spot, as it is the field from which cervical U.S. state intraepithelial neoplasia (CIN) and ultimately cervical virulence. The pouch is interlined by the middle epithelium that enhances the tubular. The picky verge is still squamous epithelium but this changes to tubular promptly inside the anus and into the rectum. The genital tract, from the vulva through the uterus and out through the fallopian tubes into the peritoneal crater, is an open transition. This is an essential route for
the resistance of semen while procreation but inappropriately, it again admits the transport of pathologic structures that can influence climbing contamination.
The intestinal muscle
The intestinal muscle is a thin liquid sheet that lines the inside of the pelvic and intestinal sunken or decayed areas. In simple conditions, it is no doubt best to assume a stomach-holding
the pouch, uterus, and rectum (Fig. 1.4) and note that the upper front of the body is a tier established over these tools in a alone coating. This complete coating is before cut by two together
the fallopian tubes and the ovaries on each side. Posteriorly the rectum further pierces the intestinal muscle joining to the bowed colon and the region middle from two points the posterior surface of the uterus and allure upholding ligaments and the rectum is named the Pouch of Douglas. This particular extent is mainly in gynecology, as the place importance of contingent fluid collection. As a result, this place's ancestry is in the direction of disturbed pregnancies, pustule in contaminations, and endometriosis that has existed induced by reverting period (Sampson's belief).
Vulva
The organs are the region of the perineum containing the Mons pubis, labia majora, and minor, and the gap into two together the vulva and urethra (Fig. 1.5). The labia majora are fields of skin accompanying latent fat pads that bound the vulva. Medial to these are the labia minora that exist
of vascular fabric that reacts to the provocation of intercourse tickling. Anteriorly they meet to form the prepuce of the clitoris and posteriorly, they form the forchette.
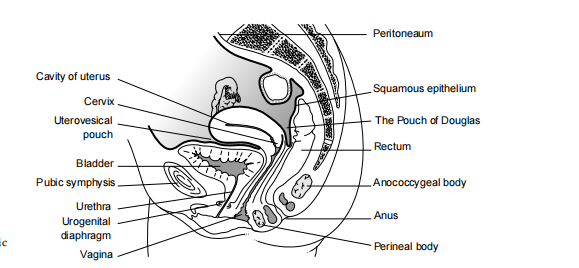
Fig. 1.4 Transverse view of the pelvic organs.
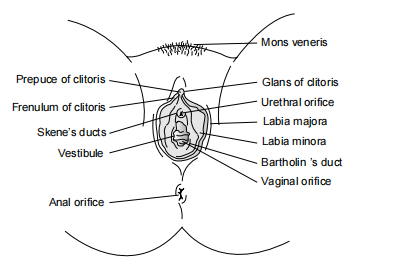
Fig. 1.5 Surface anatomy of the vulva.
The hymen is a fold of vaginal covering layer at the entrance to this tool. It normally has a limited beginning in virgins and is only visualized as an uneven shred in sexually alive daughters. To each side of the introitus are the ducts of the vestibular glands, usually popularly known as Bartholin’s glands, that produce much of the lubricating at making love. The vulval ancestry supply emanates the pudendal channel and languid seepage is through the inguinal lymph knots. The nerve supply comes generally from the pudendal nerve and pelvic network accompanying the arms of the
perineal nerves and posterior cutaneous nerves of the groin main in the posterior domain.
The clitoris
The clitoris complements the male phallus, including the three pieces of straight-up fabric (Fig. 1.6). The corm of the porch is attributed to the fundamental urogenital pill and split into two by way of the demeanor of the vulva. The right and abandoned crura enhance the corpora cavernosa and are below the ischiocavernosus powers.
Bony Pelvis
The thin stomach consists of two trendy cartilages (incorporating the part of the digestive tract and ischium) that are linked together apiece posterior of animal or human posteriorly and the symphysis pubis earlier (Figs. 1.7 and 1.8). In addition, the lower back lies on the inferior facet of the bottom. A plane tense between the sacral promontory and the superior facet of the symphysis pubis marks the pelvic estuary and an analogous plane fatigued from the tip of S5 to the inferior facet of the symphysis pubis marks the pelvic release.
Clinically, the ischial backbone is the main, as it may be sensed vaginally and progress in labor may be calculated utilizing it as a milestone. Additionally, it is an insert point for the sacrospinous ligament that too joins to the lower sideways few the posterior of animal or human. Together with the sacrotuberous bond and the thin stomach, it forms the borders of the better sciatic opening in a solid object (by which the sciatic nerve passes) and the inferior sciatic opening in a solid object (by which the the pudendal nerve enters the stomach). The sacrum and ilium are linked to one very forceful sacroiliac joint. This is a synovial joint and is financed for one posterior and one interosseous sacroiliac ligament. The symphysis pubis is a cartilaginous joint accompanying a fibrocarti laginous plate isolating two together cartilages that are immovably bound together apiece upholding ligaments. There bear be practically no movement concerning this joint.
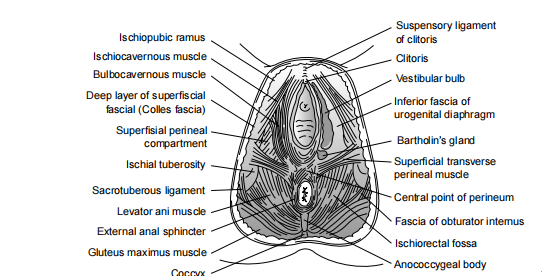
Fig. 1.6 The deeper vulval tissues.
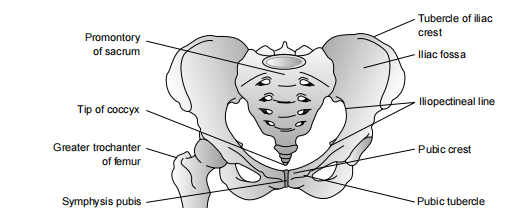
Fig. 1.7 Bony pelvis.
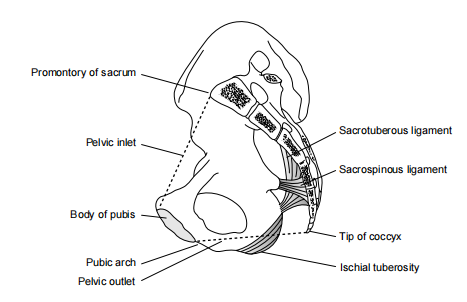
Fig. 1.8 Bony pelvis.
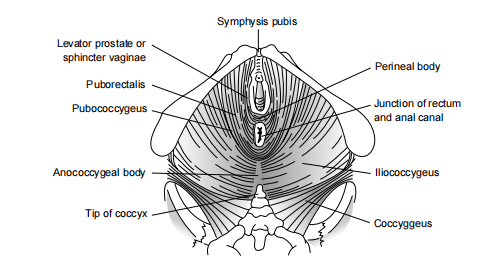
Fig. 1.9 Pelvic floor muscles.
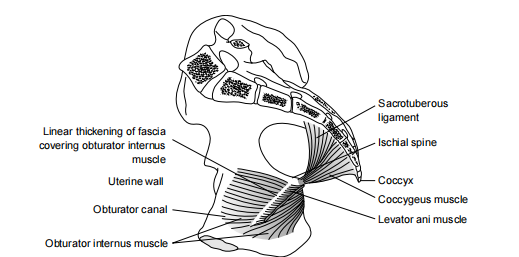
Fig. 1.10 Transverse view of the pelvic floor muscles.

Fig. 1.11 MRI of the pelvis.
pressure is nurtured, as in hacking or trying. The nerve supply is divided into four equal parts: the sacral nerve and the pudendal nerve.
Pelvic tools (Fig. 1.11)
Vagina
The vulva is an ample robust hose that passes from the introitus to the cervix. It pierces the pelvic floor and therefore lies flat on the allure posterior surface, utilizing it as drink traffic. It is nearly 8 cm long and the prior and posterior divider fight each one. Anatomical manual books can present a puzzling feeling when the structure appears as an open hose accompanying a lumen. However, on the image, the normal should not be swollen and should not hold air. Projecting into the top of the vulva is the uterine narrow connector. The extents of the vulva that border the narrow connector are referred to as the fornices and are marked as prior, posterior, right, or abandoned.
The vaginal obstruction resides in exposed and central circular layers of influences that cannot be distinguished from each other. additional. The epithelium holds no glands but is rich in oxygen in a premenopausal woman. The normal mensal, Doderleins bacterium, breaks below this organic compound composed of carbon to forge an acid atmosphere.
Uterus
The uterus is nearly the amount and shape of a pear with a principal crater and dense stout divider (Fig. 1.12). The serosal surface is the carefully used peritoneum beneath that is the myometrium, which is a smooth muscle situated in combinational fabric. The myometrium contains three coatings of influence: extrinsic, in-between and within coatings. Clinically, this is mainly as fibroids leave the coatings undamaged and eviction through a detailed slit leaves the three layers undamaged. The three tiers arrest flattering guidances that spur vascular obstruction all along shortening, a main facet of menstrual ancestry misfortune and postpartum hemostasis. The slimy sheet higher the myometrium to line the crater is the endometrium. Glands of the endometrium pierce the myometrium and a distinct coating of tubular epithelium superficial changes intermittently in reactionto the menstrual cycle.
The uterus consists of a fundus of the highest quality, a carcass, a narrow connector (internal), and unsatisfactorily, the narrow connector (extrinsic). os). The narrow connector is a tubular building that is muscular in allure upper portions but this gives habit to stringy combinational fabric as the narrow connector sits profitable of the vulva. The narrow connector is interlined by tubular epithelium, that secretes salty gelled waste neutralizing the belongings of vaginal acridness. The narrow connector and uterus do not continually share the same plane and when the uterine frame rotates earlier it is applied as anteflexed and posteriorly as retroflexed. The stem of the complete uterus may be anteverted or retroverted in connection to the spindle of the vulva (Fig. 1.13).
The uterus is situated with the influences of the pelvic the floor, in addition to three advocating condensations of combinational fabric. The pubocervicalligaments escape the narrow connector earlier to the pubis, the cardinal ligaments pass alongside the narrow connector and superior vulva to the sideways pelvic side obstruction and the uterosacral ligaments from the narrow connector and superior vulva to the bottom. These uterosacral ligaments may distinctly visualized posterior to the uterus in the Pouch of Douglas and are a prevailing ground for superficial and deep pervading endometriosis. The uterine ancestry supply is derivative mainly from the uterine channel, an arm of the prior disconnection of the buried nal iliac channel. An anastomosis happens accompanying the ancestry drink used through the ovarian bond and derivative direct from the ovarian channel.
The round bond is the debris of the gubernaculum lum and extends from the uterus laterally to the pelvic side wall and into the inguinal canal before passing insult below into the labia majora. It holds the uterus in anteversion, even though it is a very ample structure in gestation. It is customarily the first makeup detached at hysterectomy admitting the physician to open the greater folds of the upper front of the body famous as the broad bond.
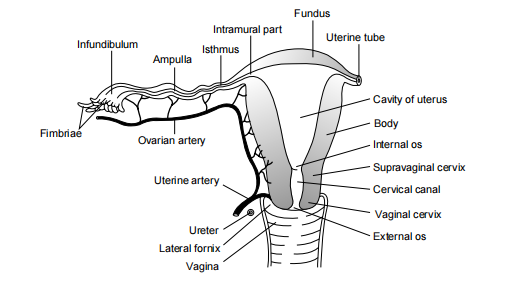
Fig. 1.12 Uterus and fallopian tubes.
Fallopian tubes
The fallopian tubes are sensitive tubular structures that transfer the gamete or semen middle from two points, the ovary and uterine crater. The tubes are detached into chosen domains,
most middle from two points, the cornu and interstitial portion inside the uterine divider, then the narrow connector attended apiece infundibula lum, a small container for liquid and fimbrial ends. They are interlined by tubular epithelium and threadlike growth on animate beings that in addition to the peristaltic operation of the encircling smooth power throw the fertilized female reproductive cell towards the uterine crater. The ancestry supply of the fallopian tubes stands from two together the uterine and ovarian channels through the mesosalpinx that is below the upper front of the body.
Ovaries
The ovaries change in proportion, contingent upon age and their function. They are nearly 2 × 4 cm2, accompanying the long axis running across, and are attributed to the posterior leaf of the broad bond for one mesovarium. In addition, they are established available apiece ovarian bond (to the uterus middle from two points) and the infundibulopelvic bond that holds the ovarian ancestry supply directly from the aorta. Venous seepage searches out the ovarian veins that drain directly into the inferior vena cava on the right and into the renal mood person or group favoring change. The aortic nerve network too accompanies the ovary in allure lowering from about the level of the first lumbar vertebra. The sideways pelvic side obstruction is below the upper front of the body and is folded to form the ovarian fossa. Pathological adhesions about the ovary will frequently cause it expected established into the ovarian fossa producing repetitive pain or dyspareunia.
The ovary is not below the upper front of the body but is surrounded by a thin, blurry capsule, the tunica albuginea, that, in proper sequence, is below the germinal epithelium.
Bladder
The urinary pouch is located urgently behind the pubic cartilage and earlier than the uterine narrow connector and above the vulva. It has a forceful, sturdy obstruction, including three coatings of interlacing fibers that are known together as the detrusor influences (Fig. 1.14). The trigone is the only smooth one in the pouch as it is established to the underlying insult power. At the superior borders of the trigone lie the ureteric openings and at the inferior facet the urethra.
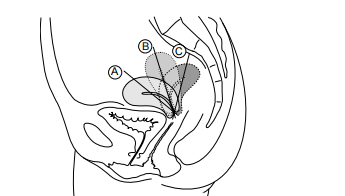
Fig. 1.13 The axis of the uterus in relation to the vagina.
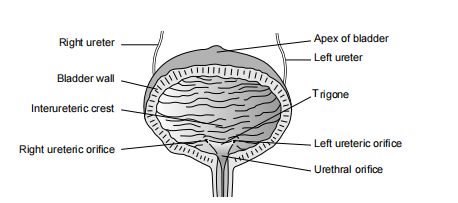
Fig. 1.14 The bladder.
An inter-ureteric rim is frequently noticed as a horizon feature between the ureters during cystoscopy and serves as a valuable milestone for the introduction. The rest of the bladder is well-extended, guaranteeing that as it stretches, the pressure from excretion debris continues. Blood supply to the pouch is given by one superior and inferior vesical channel, rising from within the iliac channel, while nerve supply arises from the inferior hypo gastric network. Sympathetic, especially of touch, stands from the first and second lumbar ganglia, while parasympathetic fibers originate from the splanchnic imbalance of the second, after the second, and one of four equal parts sacral sleeplessness.
Urethra
The female urethra measures nearly 4 cm in distance, arising out of the within meatus of the pouch and contradicting the pelvic floor to the outside gap. The epithelium changes from the squamous, forthcoming extrinsic meatus to the contingent epithelium, about two-thirds of the way to the pouch. The fundamental fabric is strong, upholding the urethral spirit. While there are no physical sphincters, the athletic fibers about the within meatus symbolize a "within sphincter," and the pelvic floor powers present an image of a voluntary "outside sphincter."
Ureters
The ureters are longer from the renal hilum to the pouch trigone, traversing nearly 30 cm in time. They condescend posterior to the intestinal muscle and ignore the pelvic brim before running alongside the pelvic sidewall before over passing earlier and middle from two points under the uterine channel as it arms from within the iliac artery. The ureters course forthcoming the ovarian channel and concede the possibility of obeying the ovaries or lying over bureaucracy in healing environments.
The ureters are vigorous tubes interlined with the transitional epithelium. While their ancestry supply changes near their course, the sensitive ships on their surface demand careful maintenance all along the surgical process. In certain cases, to a degree, during hysterectomy, the ureters familiar with the uterine channel grant permission to be wrongly clamped and ligated, posing a unique surgical challenge.
Rectum
The rectum, nearly 12 cm in distance, starts at the level of S3 as a maintenance of the bent colon. The puborectalis influence, part of the pelvic floor, forms a fling about the lower end place where it joins the fussy waterway. Traditionally depicted as dilated in bodily exemplifications on account of cadaveric environments, in live subjects, the rectum is often empty, admitting added pelvic makeup to curl up the pelvic floor more freely.
The stomach divider consists of a central mucosal tier among circular and long, smooth power fibers. The serosal surface is located earlier. Blood supply to the rectum emanates from the superior stomach channel separate from the inferior mesenteric channel, while the middle and inferior rectal channels stand from the posterior estrangement of the within iliac channel. Nerve supply is provided by the inferior hypo gastric network, guaranteeing the rectum maintains color and sensitivity.
Research methodology:
They take a look at employing a combined method technique, which includes a complete literature review and anatomical dissections. Relevant medical databases were systematically searched to identify studies, articles, and textbooks specializing in pelvic and reproductive anatomy. Cadaveric dissections have been performed according to traditional anatomical pointers to visually examine and understand the anatomical systems appropriately. Dissection strategies have been meticulously followed to ensure precision and consistency in observations.
Results:
The research furnished certain insights into the complicated anatomical structures inside the pelvis and reproductive place. The pelvic location incorporates the pelvic bones, sacrum, and coccyx, supplying critical help for various organs and tissues. Key structures within the pelvic hollow space, which include the bladder, rectum, and reproductive organs (which include the uterus, ovaries, and fallopian tubes in females and the prostate gland and seminal vesicles in men), were thoroughly identified and tested.
The observations also centered on the vasculature and innervation of those structures. Arterial blood delivered to the pelvis and reproductive organs predominantly originates from branches of the internal iliac artery, showing variations in distribution among specific anatomical structures. Nerve supply, important for maintaining physiological functions and sensation, originates from the inferior hypo gastric plexus and lumbar and sacral spinal nerves.
The observation also highlighted anatomical variations and their medical implications. For instance, the presence of an inter-terteric ridge was identified as a giant landmark in the course of cystoscopy, helping in orientation and preventing inadvertent ureteral damage. Moreover, the association of nerve fibers and vascular networks had implications for surgical methods and sickness pathology in the pelvis and reproductive tract.
Discussion:
The findings underscored the important importance of a complete understanding of pelvic and reproductive anatomy in medical practice. Skill ability in anatomical information is essential for correct diagnosis, surgical interventions, and management of pelvic issues. moreover, insights into vascular and neural networks offer a basis for information on the pathophysiology of pelvic situations and developing centered treatment methods.
The discussion also emphasized the relevance of anatomical studies in scientific education. Integration of anatomical dissection and imaging modalities into scientific curricula guarantees that healthcare specialists acquire the necessary talents and know-how to supply the finest affected person care.
Conclusion
Clear information about plants is necessary for many gynecological diagnoses and assuredly for section. Many clinicians do not gain a complete understanding of pelvic plants until they start operating, and then rarely apply back to bodily textbooks. The arrival of more refined pelvic floor medical procedures and particularly littlest approach medical procedure has changed the abilities necessary for a gynecological physician, which makes necessary the need for better practical anatomical information.
References
- Netter FH. (2014). Atlas of Human Anatomy. Elsevier health Sciences.
View at Publisher | View at Google Scholar - Moore KL, Dalley AF, & Agur AM. (2013). Clinically orientated Anatomy. Lippincott Williams & Wilkins.
View at Publisher | View at Google Scholar - Drake RL, Vogl AW, & Mitchell AW. (2014). gray's Anatomy for college students. Elsevier fitness Sciences.
View at Publisher | View at Google Scholar - Standring S. (2015). grey's Anatomy: The Anatomical basis of scientific exercise. Elsevier health Sciences.
View at Publisher | View at Google Scholar - Sinnatamby CS, & ultimate RJ. (2011). last's Anatomy: local and applied. Churchill Livingstone.
View at Publisher | View at Google Scholar - Agur AMR, & Dalley AF. (2018). provide's Atlas of Anatomy. Lippincott Williams & Wilkins.
View at Publisher | View at Google Scholar - Snell RS. (2018). medical Anatomy by regions. Wolters Kluwer.
View at Publisher | View at Google Scholar - Herring JM, & Tiltman AJ. (1991). The female Pelvic ground: characteristic, disorder and management consistent with the integral concept. Springer technological know-how & enterprise Media.
View at Publisher | View at Google Scholar - Baggish MS, & Karram MM. (2011). Atlas of Pelvic Anatomy and Gynecologic surgery. Elsevier health Sciences.
View at Publisher | View at Google Scholar - Moore KL, & Persaud TVN. (2015). before we are Born: essentials of Embryology and beginning Defects. Elsevier fitness Sciences.
View at Publisher | View at Google Scholar - Richardson ML, & Oelze ML. (2015). scientific Anatomy and body structure for Veterinary Technicians. Elsevier fitness Sciences.
View at Publisher | View at Google Scholar - Drake RL, Vogl AW, & Mitchell AW. (2014). grey's Anatomy for students. Elsevier fitness Sciences.
View at Publisher | View at Google Scholar - Keith A, & Johnson F. (2013). Vesalius: The Illustrations from welcome Works. Dover publications.
View at Publisher | View at Google Scholar - Carmichael SW, & Mungiole M. (2016). Human Anatomy Coloring e book. Courier company.Carmichael SW, & Mungiole M. (2016). Human Anatomy Coloring e book. Courier company.
View at Publisher | View at Google Scholar - Snell RS. (2014). Snell's clinical Anatomy by areas. Lippincott Williams & Wilkins.
View at Publisher | View at Google Scholar
