

Case report | DOI: https://doi.org/10.31579/2834-796X/085
Chronic headaches with aura as a neurologic manifestation of Carney Complex- A case report
1Asistant professor, Istanbul Atlas University- Faculty of Medicine, Istanbul- Turkey.
2Medical student, 5.class. Istanbul Atlas University- Faculty of Medicine, Istanbul- Turkey.
*Corresponding Author: Asuda Nur Say, Asistant Professor, Istanbul Atlas University- Faculty of Medicine, Istanbul- Turkey.
Citation: Asuda Nur Say, Mohammed Habib, Zeki Dogan, M. Rifat Yıldırım, Gokhan Bektasoglu, (2024), Chronic headaches with aura as a neurologic manifestation of Carney Complex- A case report, International Journal of Cardiovascular Medicine, 3(6); DOI:10.31579/2834-796X/085
Copyright: © 2024, Asuda Nur Say. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 01 November 2024 | Accepted: 20 November 2024 | Published: 09 December 2024
Keywords: Cardiac myxomas; headaches; cardiac surgery
Abstract
The primary cardiac tumors are extremely rare and atrial myxomas are representing approximately 50% of all cardiac tumors, left atrial myxomas are the most common, the symptoms are many included being migraines, dyspnea, and chest pain. In this report, we present a 45-year-old male presented with chronic headaches with aura was triggered by physical exertion. Taking Ibuprofen 600 mg three times daily provided relief to the patient. Braim MRI showing extension from the right pontocerebellar sibling to the internal acoustic canal 16.5x8 mm sized mass lesions with intense homogeneous contrast enhancement (primarily the acoustic schwannoma list was evaluated). Chronic lacunar infarct area at the level of the right centrum semiovale and Gamma Knife Radiosurgery was done but the chronic headaches still continuous with palpitations then Echocardiography suggested left atrial myxoma with freely moving with diastolic and prolapse into the left ventricle successful removal by cardiac surgery.
Introduction
Cardiac myxomas are oval shaped, mobile, pedunculated intra-cardiac primary cardiac tumors [1]. Cardiac myxomas are rare in the general population, with an overall estimated incidence of 0.5–1 per million population per year. [2].
Carney complex is a rare disease with only about 750 cases reported in the scientific and medical literature. In more than 70% of cases, Carney complex is related to mutations of the PRKAR1A gene coding for regulatory subunit
R1alpha of protein kinase. The mutation c.709-7del6 is mostly associated with isolated PPNAD, and the mutation c.491-492del is associated with more frequent cardiac myxomas, lentigines and thyroid tumors.
Carney complex. It is characterized by cardiac myxoma, nonendocrine tumors, abnormal skin pigmentation and melanotic schwannoma [3]. Cardiac myxoma are found in 20–40% of CNC patients. [4].
Case Report
A 45-year-old male patient presented with intermittent headaches lasting 30 minutes to 2 hours in duration. Initially, the headaches were of a low frequency (about 4 times monthly), described as throbbing, associated with an aura triggered by physical exertion since 2018. He elaborated this psychedelic pattern aura as “zig zag squiggly lines” highlighted. At the onset of the aura, the patient would lie down in a room and take ibuprofen 600 mg for relief of symptoms. The aura typically lasted about 30 minutes with intermittent headaches. Headaches were associated with nausea. On physical examination, the patient was heart rate of 72 beats per minute, blood pressure of 125/70 mmHg, and oxygen saturation of 98% on room air. He was a well-appearing man without respiratory distress. A cardiac exam revealed normal heart rate and regular rhythm, normal S1 and S2 heart sounds without tumor plop. No jugular venous distension or peripheral edema was noted. A lung exam revealed good inspiratory effort and no crackles or rales to posterior auscultation. The skin exam was not notable any pigmented and non-pigmented rubbery nodules,
At 2023; the brain MRI suggested extension from the right pontocerebellar sibling to the internal acoustic canal 16.5x8 mm sized mass lesions with intense homogeneous contrast enhancement (primarily the acoustic schwannoma list was evaluated). Chronic lacunar infarct area at the level of the right centrum semiovale and Gamma Knife Radiosurgery was done. figure 1
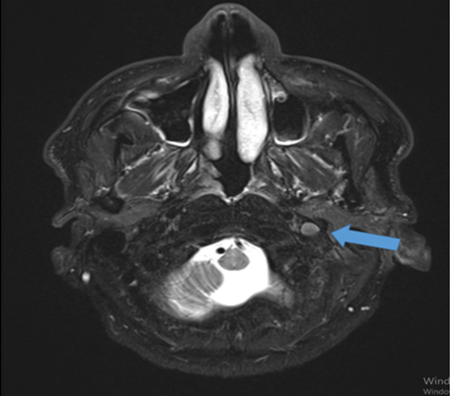
Figure1. brain MRI right cerebellopontine angle tumors (acoustic Schwannomas)
At 2024: Trans-esophageal echocardiogram showed the presence of a 2.3x2 cm myxoma in the left atrium, with good left ventricular ejection fraction (LVEF; 64%), freely moving with diastolic and prolapse into the left ventricle (Figure 2).
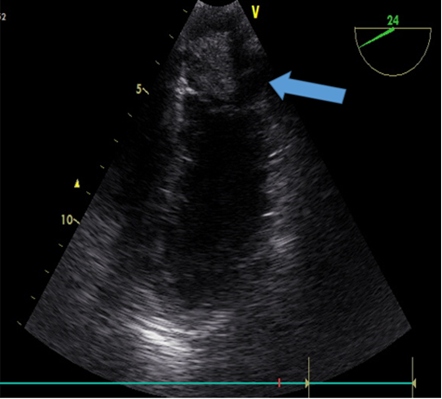
Figure 2. Trans-esophageal echocardiogram showed the presence of a 2.3x2 cm myxoma in the left atrium
The surgical approach was performed by left axillary thoracotomy, aorto-bicaval cardiopulmonary bypass, and normothermic anterograde blood cardioplegia. After the hockey stick aortotomy, a translucent fragile jellylike tumor was visualized in the left atrium and the tumor was removed (Figure 3) the patient was discharged from hospital at 3rd day without complications.
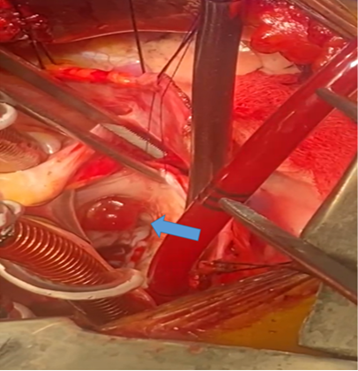
Figure 3. Left atrial myxoma
Discussion
The incidence of a cardiac myxoma in Carney complex patients was (42.6%). The overall risk of developing the psammomata’s melanotic schwannoma coincidence with cardiac myxoma only in the 11.7% of patients with carney complex [5].
Cardiac myxomas in patients with Carney complex are of great concern because they can cause intracardiac obstruction and systemic embolism the formation of emboli, and sudden death [6].
When cardiac myxomas recur frequently, they may require Cardiac auto transplantation and radical bi-atrial resection [7].
In conclusion
our case report provides risk estimates for cardiac myxomas in patients with long standing migraine with aura despite diagnosis of brain schwannoma. Early diagnosis by echocardiography is recommended annually for early detection of primary or recurrent tumor.
Ethical approval Yes. Written consent received.
Funding: None.
Conflicts of interest
The authors state that there are no conflicts of interest
References
- Mahavar RK, Arora D, Singh A, Mishra M, (2021). Recurrent cardiac myxoma: a case report. Ann Card Anaesth. 24:490-2.
View at Publisher | View at Google Scholar - Briassoulis G, Kuburovic V, Xekouki P, et al. Recurrent left atrial myxomas in Carney complex: a genetic cause of multiple strokes that can be prevented. J Stroke Cerebrovasc Dis. 2012;21:914 e911–918
View at Publisher | View at Google Scholar - Bain J. “Carney’s complex”. Mayo Clin Proc. 1986;61:5083.
View at Publisher | View at Google Scholar - spiard S, Bertherat J. Carney complex. Front Horm Res. 2013;41:50–62.
View at Publisher | View at Google Scholar - Georgia Pitsava, et al. (2021). Predicting the risk of cardiac myxoma in Carney complex . Genetics in Medicine 23:80–85.
View at Publisher | View at Google Scholar - Bandettini WP, Karageorgiadis AS, Sinaii N, et al. (2016). Growth hormone and risk for cardiac tumors in Carney complex. Endocr Relat Cancer. 23: 739–746
View at Publisher | View at Google Scholar - Gammie JS, Abrishamchian AR, Griffith BP. (2007). Cardiac autotransplantation and radical bi-atrial resection for recurrent atrial myxoma. Ann Thorac Surg. 83:1545–1547.
View at Publisher | View at Google Scholar
