

Research Article | DOI: https://doi.org/10.31579/2834-8532/002
Chemical Constituents, Cytotoxicity and Hyperglycemic effect of the Leaves of Solanum Nigrum L.-Black Nightshade
1Department of Biochemistry, Federal University Wukari, Taraba State. Nigeria
2Department of Crop Production and Protection, Federal University Wukari, Taraba State. Nigeria
3Department of Biochemistry, Adamawa State University Mubi (ADSU) Adamawa State Nigeria
*Corresponding Author: Isaac John Umaru, 1Department of Biochemistry, Federal University Wukari, Taraba State. Nigeria.
Citation: Isaac John Umaru, Christopher Emeka Ahuchaogu and Maryam Usman Ahmed, (2022) Chemical Constituents, Cytotoxicity and Hyperglycemic effect of the Leaves of Solanum Nigrum L.-Black Nightshade. Clinical Genetic Research, 1(1); Doi: 10.31579/2834-8532/002
Copyright: © 2022 Isaac John Umaru, This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 12 September 2022 | Accepted: 20 September 2022 | Published: 26 September 2022
Keywords: chemical; constituents; cytotoxicity; leaves; solanum nigrum; diabetics; chromatography; elucidation
Abstract
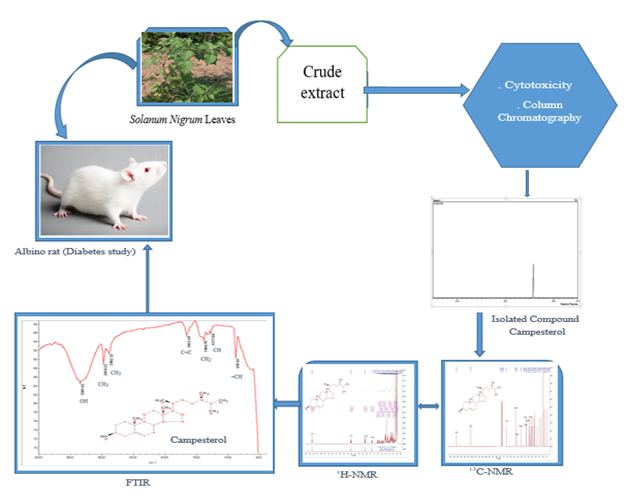
Introduction: The World Health Organization (WHO) defines traditional medicine as practices, knowledge and belief systems which use minerals, plants and animal-based remedies, spiritual therapies and exercises to prevent, treat and maintain wellbeing. Diabetes mellitus is a heterogeneous group of metabolic disorder characterized by high blood glucose level. The pancreatic β-cells and its secretory hormone i.e. insulin are central in the pathophysiology of Diabetes. The aims of this study was to isolate the chemical constituents, test the cytotoxicity of the crude extract and evaluate the hyperglycaemic effects of the isolated compound and crude extract of Solanum Nigrum leaves crude extract
Materials and Methods: The extraction was carried out by conventional extraction by soaking the powdered sample in solvent 1:3 (sample: solvent) in hexane, dichloromethane, chloroform, and ethyl acetate, Cytotoxicity test using Brine shrimp (Artemia salina), and hyperglycaemic evaluation using Alloxan was used intraperitoneally to induce diabetic in albino rats, treatment group including glibenclamide (600 µg/kg) and pioglitazone (429 μg/kg), were considered in the study. The effect of the crude extract on glucose, other biochemical, and the hematological parameters were evaluated. Results: Diabetic control was on the days 7 of the study with 100, 200, 300, 400 and 500 mg/kg of the extract showing a glucose reduction at 500, 338.94±4.14, 184.78±1.12, 129.45±1.23, and 98.11±4 µg/mL as significant. The isolated compound campesterol Indicated significant hyperglycemic reduction in the blood system.
Conclusion: This study showed that Solanum Nigrum L has an anti-hyperglycemic activity and this is also attributed as result of some active chemical constituents like campesterol which play an important role in the management of Diabetes mellitus in the extract. This study was carried out for the first time of Solanum Nigrum L on alloxan-induced diabetic rats.
Introduction
The World Health Organization (WHO) defines traditional medicine as practices, knowledge and belief systems which use minerals, plants and animal-based remedies, spiritual therapies and exercises to prevent, treat and maintain wellbeing (WHO, 2003). The practice is widely accepted and practiced due to some major factors like the poor socio-economic situations of the communities (mostly in sub Saharan regions and third world countries and areas that have suffered insurgences ravaged with hunger as well as the the exorbitant cost of most western drugs and treatments, and its affordability as compared to the availability and accessibility of these medicinal plants (Umaru et al., 2019)
Plants being the most reliable source of food to human have also been used as folk medicine for centuries and as medicinal remedies in health care systems even with the advancement in technology.The medicinal activities of the plants have long been associated with the production of secondary metabolites which includes tannins, terpenoids, coumarins, alkaloids, flavonoids and others. These plant products also help the plants to carry out various activities like defence and pollination. They could also be used as stimulants, poisons or hallucinogenic because these chemical compounds have biological effects on another organism (Ntie-Kang et al., 2013)
Solanum nigrum commonly known as Black night shade belongs to the family solanancae. It is also called garden night shade. The plant is commonly grows as a weed in moist habitats and can be cultivated in tropical and subtropical environment by the seed in the month of April or May. The plant Solanum nigrum has been used traditionally to treat different diseases and ailment such as; Leaves for rheumatic and gouty joints, skin diseases, tuberculosis, nausea and nervous disorder as well as cough and diarrhea. The ethanol extract was reported to have anti-cancerous properties (Jani et al., 2011; Rani, et al., 2017)
Various scientist have also reported of the plant as an anticancer, antifungal, with antioxidant potential (Miraj, 2016). As a hepato-protective activity (Rani et al., 2017), as an antidepressant, antidiabetic, immunostimulant activity, antibacterial and antidiabetes (Dilip, et al., 2012).
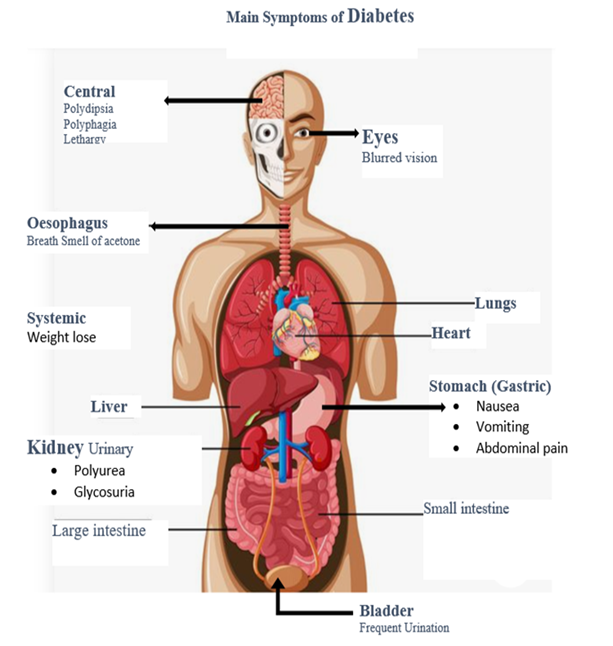
However, diabetes has become one of the most common diseases in the world especially in the less developed countries like Nigeria and Malaysia. Diabetes mellitus (DM) also known as simply diabetes, is a group of metabolic diseases in which there are high blood sugar levels over a prolonged period. This high blood sugar produces the symptoms of frequent urination, increased thirst, and increased hunger. Untreated, diabetes can cause many complications. Acute complications include diabetic ketoacidosis and nonketotic hyperosmolar coma. Serious long-term complications include heart disease, stroke, kidney failure, foot ulcers and damage to the eyes (Umaru et al., 2018).
Diabetes is due to either the pancreas not producing enough insulin, or the cells of the body not responding properly to the insulin produced. There are three main types of diabetes mellitus;
Type 1 DM results from the body's failure to produce enough insulin. This form was previously referred to as "insulin-dependent diabetes mellitus" (IDDM) or "juvenile diabetes". The cause is unknown
Type 2 DM begins with insulin resistance, a condition in which cells fail to respond to insulin properly. As the disease progresses a lack of insulin may also develop. This form was previously referred to as "non-insulin-dependent diabetes mellitus" (NIDDM) or "adult-onset diabetes". The primary cause is excessive body weight and not enough exercise (Govindappa, 2015). Gestational diabetes, is the third main form and occurs when pregnant women without a previous history of diabetes develop a high blood glucose level.
Prevention and treatment
Involves a healthy diet, physical exercise, not using tobacco, and being a normal body weight. Blood pressure control and proper foot care are also important for people with the disease. Type 1 diabetes must be managed with insulin injections. Type 2 diabetes may be treated with medications with or without insulin. Insulin and some oral medications can cause low blood sugar. Weight loss surgery in those with obesity is an effective measure in those with type 2 DM. Gestational diabetes usually resolves after the birth of the baby (Adnette, et al., 2019).
Signs and symptoms are classic symptoms of untreated diabetes are weight loss, polyuria (frequent urination), polydipsia (increased thirst), and polyphagia (increased hunger). Symptoms may develop rapidly (weeks or months) in type usually develop much more slowly and may be subtle or absent in type 2 diabetes. Several other signs and symptoms can mark the onset of diabetes, although they are not specific to the disease. In addition to the known ones above, they include blurry vision, headache, fatigue, slow healing of cuts, and itchy skin. Prolonged high blood glucose can cause glucose absorption in the lens of the eye, which leads to change in shape, resulting in vision changes. A number of skin rashes that can occur in diabetes are collectively known as Diabetic dermatomes. American Diabetes Association. (2009).
People (usually with type 1 diabetes) may also experience episodes of diabetic ketoacidosis, a type of metabolic problems characterized by nausea, vomiting and abdominal pain, the smell of acetone on the breath, deep breathing known as Kussmaul breathing and in severe cases a decreased level of consciousness. A rare but equally severe possibility is common in type 2 diabetes and is mainly the result of dehydration.
All forms of diabetes increase the risk of long term complications. These typically develop after many years about ten to twenty years, but may be the first symptoms in those who have otherwise not received a diagnosis before that time. The major long-term complications relate to damage to blood vessels. Diabetes doubles the risk of cardiovascular disease and about 75% of deaths in diabetics are due to coronary artery disease. Other "macro vascular" diseases are stroke, and peripheral vascular disease. American Diabetes Association. (2009).
The primary micro vascular complications of diabetes include damage to the eyes, kidneys, and nerves. Damage to the eyes, known as diabetic retinopathy, is caused by damage to the blood vessels in the retina of the eye, and can result in gradual vision loss and potentially blindness. Damage to the kidneys, known as diabetic nephropathy, can lead to tissue scarring, urine protein loss, and eventually chronic kidney disease, sometimes requiring dialysis or kidney transplant Damage to the nerves of the body, known as diabetic neuropathy, is the most common complication of diabetes. The symptoms can include numbness, tingling, pain, and altered pain sensation, which can lead to damage to the skin. Diabetes-related foot problems (such as diabetic foot ulcers) may occur, and can be difficult to treat, occasionally requiring amputation. Additionally, proximal diabetic neuropathy causes painful muscle wasting and weakness. There is a link between cognitive deficit and diabetes. Compared to those without diabetes, those with the disease have a 1.2 to 1.5-fold greater rate of decline in cognitive function (Fall, et al., 2016).
Diabetes mellitus is classified into four broad categories: type 1, type 2, gestational diabetes, and "other specific types". The "other specific types" are a collection of a few dozen individual causes. The term "diabetes", without qualification, usually refers to diabetes mellitus. Type 1 diabetes mellitus is characterized by loss of the insulin- producing beta cells of the islets of Langerhans in the pancreas, leading to insulin deficiency. This type can be further classified as immune-mediated or idiopathic. The majority of type 1 diabetes is of the immune-mediated nature, in which a T-cell-mediated autoimmune attack leads to the loss of beta cells and thus insulin. Most people are otherwise healthy and of a healthy weight when onset occurs. Sensitivity and responsiveness to insulin are usually normal, especially in the early stages. Type 1 diabetes can affect children or adults, but was traditionally termed juvenile diabetes because a majority of these diabetes cases were in children (WHO, 2019)
"Brittle" diabetes, also known as unstable diabetes or labile diabetes, is a term that was traditionally used to describe the dramatic and recurrent swings in glucose levels often occurring for no apparent reason in insulin-dependent diabetes. This term however, has no biologic basis and should not be used. Still type 1 diabetes can be accompanied by irregular and unpredictable hyperglycaemia, frequently with ketosis and some with serious hypoglyemia. Other complication include an impaired counter regulatory response to hypoglycaemia, infection, gastroparesis which leads to erratic absorption of dietary carbohydrates), and endocrinopathies (e.g., Addison’s disease). These phenomena are believed to occur no more frequently than in 1% to 2% of persons with type 1 diabetes. (WHO, 2019)
Type 1 diabetes is partly inherited, with multiple genes, including certain HLA genotypes, known to influence the risk of diabetes. In genetically susceptible people, the onset of diabetes can be triggered by one or more environmental factors, such as a viral infection or diet. There are some evidence that suggests an association between type 1 diabetes and Coxsackie B4 virus. Unlike type 2 diabetes. The onset of type 1diabetes is unrelated to lifestyle (Bai, et al., 2019)
Type 2 diabetes mellitus is characterized by insulin resistance, which may be combined with relatively reduced insulin secretion. The defective responsiveness of body tissues to insulin is believed to involve the insulin receptor. However, the specific defects are not known. Diabetes mellitus cases due to a known defect are classified separately. Type 2 diabetes is the most common type. In the early stage of type 2, the predominant abnormality is reduced insulin sensitivity. At this stage, hyperglycaemia can be reversed by a variety of measures and medications that improve insulin sensitivity or reduce glucose production by the liver (Durruty, et al., 2019)
Type 2 diabetes is due primarily to lifestyle factors and genetics. A number of lifestyle factors are known to be important to the development of type 2 diabetes, including obesity (defined by a body mass index of greater than thirty), lack of physical activity, poor diet, stress, and urbanization. Excess body fat is associated with 30% of cases in those of Chinese and Japanese descent, 60-80% of cases in those of European and African descent, and 100% of Pima Indians and Pacific Islanders. Those who are not obese often have a high waist–hip ratio. (Durruty, et al., 2019)
Dietary factors also influence the risk of developing type 2 diabetes. Consumption of sugar-sweetened drinks in excess is associated with an increased risk. The type of fats in the diet is also important, with saturated fats and trans fatty acids increasing the risk and polyunsaturated and monounsaturated fat decreasing the risk. Eating lots of white rice appears to also play a role in increasing risk. A lack of exercise is believed to cause 7% of cases. (Sam, et al., 2017)
Gestational diabetes mellitus (GDM) resembles type 2 diabetes in several respects, involving a combination of relatively inadequate insulin secretion and responsiveness. It occurs in about 2-10% of all pregnancies and may improve or disappear after delivery. However, after pregnancy approximately 5-10% of women with gestational diabetes are found to have diabetes mellitus, most commonly type. Gestational diabetes is fully treatable, but requires careful medical supervision throughout the pregnancy. Management may include dietary changes, blood glucose monitoring, and in some cases insulin may be required (Herath, et al., 2017).
Though it may be transient, untreated gestational diabetes can damage the health of the fetus or mother. Risks to the baby include macrosomia (high birth weight), congenital cardiac and central nervous system anomalies, and skeletal muscle malformations. Increased fetal insulin may inhibit fetal surfactant production and cause respiratory distress syndrome. Hyperbilirubinemia may result from red blood cell destruction. In severe cases, perinatal death may occur, most commonly as a result of poor placental perfusion due to vascular impairment. Labour induction may be indicated with decreased placental function. A Caesarean section may be performed if there is marked fetal distress or an increased risk of injury associated with macrosomia, such as shoulder dystocia (Salma, et al., 2018).
This study was conducted to isolate a chemical constituent, evaluate Cytotoxicity and antidiabetic potentials of the Leaves of Solanum Nigrum L.-Black Nightshade, and in ascertain the compound responsible for the activities as acclaimed by the traditional medical practitioners.

Materials and Methods
Sample collection
Samples of leaves of Solanum Nigrum L.-Black Nightshade, were collected from the Universiti Malaysia Sarawak in March 2019. The samples were authenticated and deposited at the Universiti Herbarium with Voucher specimen No IJU15010238.
Chemical reagents
Chemical reagents used to induce Diabetes in albino rats; streptozotocin and standard for anti-diabetes drug glibenclamide and pioglitazone were purchased from Sigma-Aldrich Co, Selangor Malaysia.
Preparation of crude extract
The Solanum Nigrum L.-Black Nightshade, leaves were air dried, ground in an electric blender, soaked in methanol for 7 days, then filtered. The residue was re-extracted with fresh methanol for 72 hrs. All the solvent were combined and evaporated in rotary evaporator (Rato-vap). The extract was stored in a sample bottle prior to use.
Cytotoxicity test
The test was conducted using larvae of Artemia salina. A One spatula full of brine eggs was placed into a 250 mL beaker containing 150 mL of sea water placed under light environment. A source of O2 supply was connected to the beaker using water pump at reduced pressure and allowed for 72 hrs to hatch. The brine shrimp (nauplii) were then used for the test.
4 mg of the extract was dissolved in 200 µL of DMSO, 5 mL of filtered seawater containing chosen concentration was prepared by serial dilution with DMSO. The assay system was prepared with 5 mL of filtered seawater containing chosen concentration of extract and 1% yeast extract (for feeding) in a pre-marked 6-well microplate and 10 brine shrimps were carefully taken with micropipette and introduced into each microplate.
Filtered seawater was added to DMSO and 10 brine shrimps in triplicates and this was used as the control groups. If the brine shrimp in these microplates shows a rapid mortality rate, then the test is considered invalid as the nauplii might have died due to some reasons other than the cytotoxicity of the extracts. The setup was allowed to remain for 24 hrs under constant illumination of fluorescent and number of survived nauplii were counted with a hand lens. Based on the data obtained, the average death of the brine shrimp at different concentrations of the extract. These was done in triplicate.
Isolation of the chemical constituent of Methanol crude Leaves extract
A glass column of size 40/34 (large) was used for chromatography, and the sorbent used was silica gel 60. Silica gel slurry was prepared by dissolving silica gel (150 g) with suitable of hexane. Using increasing proportion pattern of polar and non-polar solvent (hexane, dichloromethane, chloroform, ethyl acetate and methanol). One hundred milliliter fractions were collected. All fractions were monitored by thin layer chromatography. Fractions with the spots of same Rf value were combined and re-Colum in appropriate columns (24/29 and 14/23) and solvent system until TLC of one spot presumable to be pure isolates were obtained as confirmed in UV and vanillin stain (Umaru et al., 2019)
Fraction with single component (one spot) that appeared in TLC plate was treated as possible pure secondary metabolite. The combined fractions which contained the same single component was then allowed to air-dried or evaporated to dryness to obtain a pure secondary metabolite.
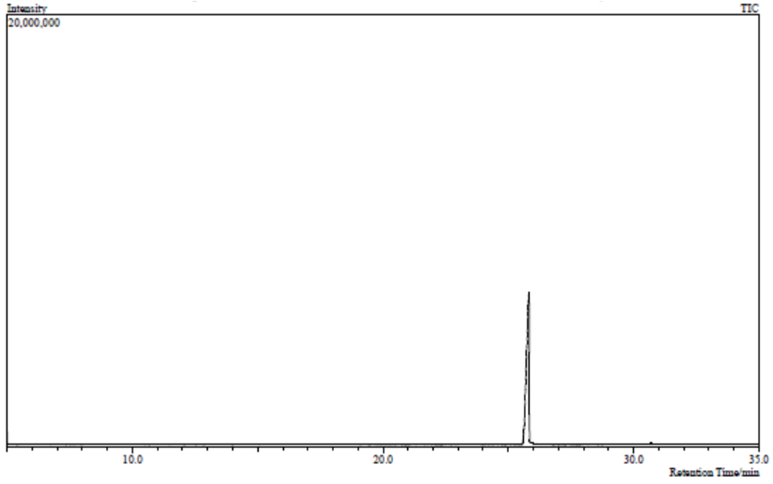
Gas Chromatography – Mass spectrometry (GC-MS)
The presumed one spot fraction was subjected to GC-MS Spectrometry model QP2010. Compound identification was obtained by matching the retention times of the compounds and the mass spectral obtained from the library data of the corresponding compound (Umaru et al., 2020)
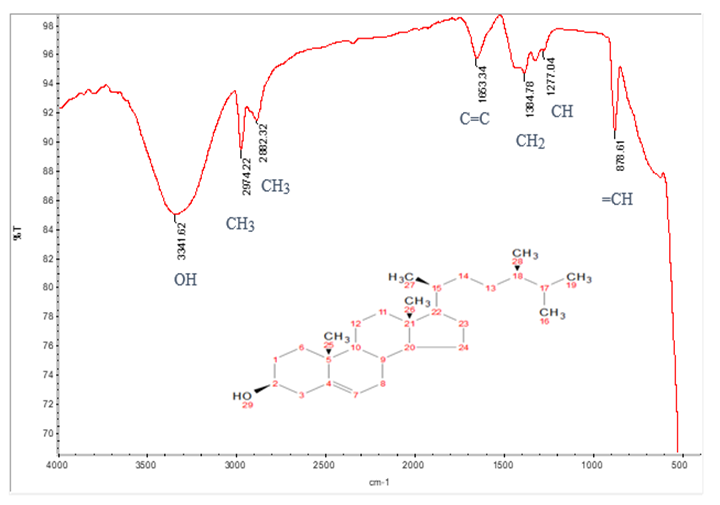
Fourier Transform Infra-Red Spectrometry (FT-IR)
Fourier Transform Infra-Red (FT-IR) was performed using FTIR spectroscopy Thermos Scientific, Nicolet iS10 SMART iTR model, to detect the chemical bonds and functional groups of the compounds isolated. The characteristic of the chemical bonds was read by spectrum produced through transmittance of wavelength of light. The chemical bond in a molecule were detected by interpreting the infra-red transmittance spectrum and the functional groups of the compounds were identified based on the Table of Characteristic IR absorptions published in Organic Chemistry (Janice, 2008).
Nuclear Magnetic Resonance (NMR)
Nuclear Magnetic Resonance (NMR) spectrometry was performed using JEOL JNM-ECA 500 Spectrometer. Sample was dissolved in 0.8 mL chloroform D1 (CDCl3) and placed into the NMR machine for the 1H (500 MHz) and 13C (125 MHz) spectra, which was detected based on the guide of the possible proposed structure given by NIST library.
Melting Point of the compounds
The melting point was tested using melting point apparatus Stuat model SMP3. With small amount inserted the heating process was monitored and the temperature at which the sample begins to melt and completely melted was recorded.
Diabetic Study
Animal used in the study
Seventy-two male albino rats weighing about 180 to 200 g were purchased from the animal farm, they were housed in clean smaller animal cages, and nine rats’ cages were used and maintained at room temperature 25oc with relative humidity of 46-55% under 12:12 hrs. light and dark cycle for one week with food access and water at libitum. The experiment procedure was carried out based on the approval of the institutional Animal ethical committee, and the experiment was carried out in compliance with the ethical committee.
Methodology
Preparation of crude extract and isolated compound were used to evaluate the diabetic potential of Solanum Nigrum leaves. The induction of diabetes was carried out using streptozotocin. The drug was (streptozotocin) was dissolved in freshly prepared 0.1 M citrate buffer having pH 4.5. A dose of 50 mg of streptozotocin per kg body weight was injected intraperitoneal which eventually produce a sign of diabetes such as increase in food intake, frequent urination, and increase in the blood glucose concentration similar human as indicated in Figure 1. Streptozotocin was selected for this study because of its greater selectivity of β-cell, lower mortality and relatively longer half-life to about 15 min in the body. The effect of streptozotocin (diabetes) was confirmed 48hrs after administration of the streptozotocin using glucometer. From the test all animals with plasma level greater than 200 mg/dl were considered to be used in the study because they are considered to be diabetes (Gupta, et al., 2017). Daily test reading using glucometer was carried out and the weight of the rats during the course of the treatment were recorded. A drop of blood from the tail vein were collected on the strip device gives the reading with two to five second. Ethanol was used to clean the tail of the study animal.
Dosage preparation and treatment protocol
The dosage of the sample for the study were prepared and fusion of the extracts were given to the rats orally by cannula. However, rats that died in the course of the induction of streptozotocin administration were disposed of and cages were changed within three to four days of the start experiment. In the treatment protocol, the rats were divided into nine groups each containing eight animals;
- Group 1 Normal non-diabetes rats
- Group 2 Diabetic rats as control
- Group 3 Diabetic rats with gilbenclamide (600 µg/kg)
- Group 4 Diabetic rats with pioglitazone (429 μg/kg)
- Group 5 Diabetic rats treated with 100 mg/kg crude and Campesterol respectively
- Group 6 Diabetic rats treated with 200 mg/kg crude and Campesterol respectively
- Group 7 Diabetic rats treated with 300 mg/kg crude and Campesterol respectively
- Group 8 Diabetic rats treated with 400 mg/kg crude and Campesterol respectively
- Group 9 Diabetic rats treated with 500 mg/kg crude and Campesterol respectively
The antidiabetic activity of the crude extract and the isolated compound were evaluated by the estimation of the blood glucose levels and the body weight measurement on the day 0, day 7, day 14 and day 21 of the study by using a commercial kits ( Accu-chek active test meter). This study will be based on two parameters on which diabetes affected first one on weight and the second is blood glucose level i.e. body weight and blood glucose test level of the animals before and after streptozotocin injection.
Results and Discussion
Results
The 1H-NMR and 13C-NMR data on the isolated compound, crude extract, cytotoxicity and anti-diabetes potential are as recorded below
Solvent system | Average death of Artemia salina Concentration (µg/mL) | LC50 (µg/mL) | |||||
1 | 10 | 25 | 50 | 100 | 500 | ||
Control | 0 | 0 | 0 | 0 | 0 | 0 |
|
Thymol | 5.00±0.57 | 7.00±0.58 | 10.00±0.00 | 10.00±0.00 | 10.00±0.00 | 10.00±0.00 | 1.16 |
Hexane | 4.80±0.58 | 5.70±0.58 | 5.33±1.16 | 7.33±1.16 | 9.33±1.16 | 10.00±0.00 | 24.09 |
Dichloromethane | 4.00±0.00 | 4.70±0.58 | 5.70±0.58 | 8.44±0.00 | 8.67±0.58 | 10.00±0.00 | 27.59 |
Chloroform | 4.00±1.00 | 5.70±0.58 | 7.70±0.58 | 8.00±0.00 | 8.67±0.58 | 9.700±0.58 | 10.54 |
Ethyl acetate | 4.00±0.00 | 4.70±0.58 | 5.70±0.58 | 8.00±0.00 | 8.67±0.58 | 10.00±0.00 | 27.41 |
Campesterol | 4.33±1.15 | 4.77±0.58 | 8.70±2.31 | 9.33±1.15 | 10.0±0.00 | 10.00±0.00 | 18.46 |
The result is Mean±SD. N = 10
Table 2: Average death of brine shrimp (Artimia salina) at different concentration of leaf extract of Solanum Nigrum
|
| Induced Diabetics | |||||||
Parameters | Control | Diabetic control | glibenclamide | pioglitazone | Treatment Groups with Solanum Nigrum crude | ||||
|
|
|
|
| 100 | 200 | 300 | 400 | 500 |
Day 0 Pre-T | 89.7±5.12 | 258.72±2.44 | 258.50±0.93 | 315.13±5.51 | 317.56±1.22 | 326.17±1.33 | 337.87±3.32 | 338.89±3.88 | 338.94±4.14 |
Day 7 PT | 91.8±1.11 | 316.63±1.00 | 215.89±0.71 | 208.19±22.2 | 316.46±0.15 | 216.32±0.45 | 204.44±0.34 | 196.78±1.00 | 184.78±1.12 |
Day 14 PT | 92.3±0.42 | 338.00±0.45 | 162.79±0.21 | 146.26±25.1 | 229.66±0.35 | 209.13±0.24 | 170.08±0.12 | 149.45±0.99 | 129.45±1.23 |
Day 21 PT | 91.7±1.27 | 463.00±1.17 | 96.84±0.62 | 111.13±12.2 | 196.11±7.52 | 126.20±1.23 | 119.11±18.16 | 103.08±15.67 | 98.11.08±4.67 |
Pre-T = Pre-treatment, PT = Post treatment
Table 3: Change on blood glucose level (mean±SD, mg/dl) in groups of normal and Streptozotocin (STZ) induced diabetic Rats (n=8)
|
| Induced Diabetics | |||||||
Parameters | Control | Diabetic control | glibenclamide | pioglitazone | Treatment Groups with Solanum Nigrum crude | ||||
|
|
|
|
| 100 | 200 | 300 | 400 | 500 |
Day 0 Pre-T | 180.11±0.33 | 209.34±0.51 | 188.00±0.15 | 191.02±1.15 | 186.30±0.27 | 201.42±0.18 | 206.11±0.22 | 205.9±0.77 | 211.9±0.45 |
Day 7 PT | 200.01±0.43 | 198.01±0.16 | 206.01±0.27 | 211.23±0.17 | 194.00±0.37 | 189.00±0.27 | 204.22±0.18 | 210.00±0.47 | 215.00±0.65 |
Day 14 PT | 189.00±0.45 | 178.33±1.22 | 219.00±0.15 | 221.12±0.13 | 197.33±1.64 | 177.40±0.55 | 217.42±0.17 | 213.12±0.56 | 217.12±0.77 |
Day 21 PT | 203.67±2.78 | 159.45±3.13 | 238.03±0.19 | 247.45±1.39 | 200.23±4.39 | 165.00±1.33 | 208.19±0.34 | 217.14±1123 | 223.14±1.28 |
Pre-T = Pre-treatment, PT = Post treatment
Table 4: Changes on body weight (mean ±SD, mg/dl) in groups of normal and Streptozotocin (STZ) induced diabetic Rats (n=8)
|
| Induced Diabetics | |||||||
Parameters | Control | Diabetic control | glibenclamide | pioglitazone | Treatment Groups with isolated Campesterol (µg/dl) | ||||
|
|
|
|
| 100 | 200 | 300 | 400 | 500 |
Day 0 Pre-T | 89.7±5.12 | 258.72±2.44 | 258.50±0.93 | 315.13±1.51 | 306.56±1.37 | 323.17±1.26 | 342.87±1.67 | 329.89±1.17 | 336.14±4.22 |
Day 7 PT | 91.8±1.11 | 316.63±1.00 | 215.89±0.71 | 208.19±1.26 | 296.46±0.43 | 212.32±0.29 | 199.44±0.14 | 146.78±1.23 | 124.45±1.43 |
Day 14 PT | 92.3±0.42 | 338.00±0.45 | 162.79±0.21 | 146.26±2.12 | 218.66±0.39 | 198.13±0.21 | 157.08±0.17 | 120.45±0.16 | 100.11±1.22 |
Day 21 PT | 91.7±1.27 | 463.00±1.17 | 96.84±0.62 | 111.13±1.25 | 169.11±1.64 | 154.20±1.22 | 108.11±1.13 | 98.08±11.65 | 73.09±0.13 |
Pre-T = Pre-treatment, PT = Post treatment
Table 5: Change on blood glucose level (mean±SD, µg/dl) in groups of normal and Streptozotocin (STZ) induced diabetic Rats (n=8)
|
| Induced Diabetics | |||||||
Parameters | Control | Diabetic control | glibenclamide | pioglitazone | Treatment Groups with isolated Campesterol (µg/dl) | ||||
|
|
|
|
| 100 | 200 | 300 | 400 | 500 |
Day 0 Pre-T | 180.11±0.33 | 209.34±0.57 | 188.00±0.16 | 191.02±1.19 | 184.30±0.22 | 203.42±0.19 | 205.11±0.23 | 208.9±0.18 | 209.9±0.36 |
Day 7 PT | 200.01±0.43 | 198.01±0.19 | 206.01±0.29 | 211.23±0.18 | 188.46±0.28 | 210±1.66 | 216.44±2.11 | 216.78±1.22 | 236.12±1.34 |
Day 14 PT | 189.00±0.45 | 178.33±1.25 | 219.00±0.17 | 221.12±0.16 | 190.26±0.39 | 221.13±0.48 | 230.08±1.33 | 229.45±1.57 | 239.16±0.67 |
Day 21 PT | 203.67±2.78 | 159.45±3.14 | 238.03±0.24 | 247.45±1.38 | 192.11±3.57 | 199.20±2.29 | 238.11±4.12 | 241.08±1.87 | 249.34±1.64 |
Table 6: Changes on body weight (mean ±SD, µg /dl) in groups of normal and Streptozotocin (STZ) induced diabetic Rats (n=8)
Solvent system | Average death of Artemia salina Concentration (µg/mL) | LC50 (µg/mL) | |||||
1 | 10 | 25 | 50 | 100 | 500 | ||
Control | 0 | 0 | 0 | 0 | 0 | 0 |
|
Thymol | 5.00±0.57 | 7.00±0.58 | 10.00±0.00 | 10.00±0.00 | 10.00±0.00 | 10.00±0.00 | 1.16 |
Hexane | 4.80±0.58 | 5.70±0.58 | 5.33±1.16 | 7.33±1.16 | 9.33±1.16 | 10.00±0.00 | 24.09 |
Dichloromethane | 4.00±0.00 | 4.70±0.58 | 5.70±0.58 | 8.44±0.00 | 8.67±0.58 | 10.00±0.00 | 27.59 |
Chloroform | 4.00±1.00 | 5.70±0.58 | 7.70±0.58 | 8.00±0.00 | 8.67±0.58 | 9.700±0.58 | 10.54 |
Ethyl acetate | 4.00±0.00 | 4.70±0.58 | 5.70±0.58 | 8.00±0.00 | 8.67±0.58 | 10.00±0.00 | 27.41 |
Campesterol | 4.33±1.15 | 4.77±0.58 | 8.70±2.31 | 9.33±1.15 | 10.0±0.00 | 10.00±0.00 | 18.46 |
The result is Mean±SD. N = 10
Table 2: Average death of brine shrimp (Artimia salina) at different concentration of leaf extract of Solanum Nigrum
|
| Induced Diabetics | |||||||
Parameters | Control | Diabetic control | glibenclamide | pioglitazone | Treatment Groups with Solanum Nigrum crude | ||||
|
|
|
|
| 100 | 200 | 300 | 400 | 500 |
Day 0 Pre-T | 89.7±5.12 | 258.72±2.44 | 258.50±0.93 | 315.13±5.51 | 317.56±1.22 | 326.17±1.33 | 337.87±3.32 | 338.89±3.88 | 338.94±4.14 |
Day 7 PT | 91.8±1.11 | 316.63±1.00 | 215.89±0.71 | 208.19±22.2 | 316.46±0.15 | 216.32±0.45 | 204.44±0.34 | 196.78±1.00 | 184.78±1.12 |
Day 14 PT | 92.3±0.42 | 338.00±0.45 | 162.79±0.21 | 146.26±25.1 | 229.66±0.35 | 209.13±0.24 | 170.08±0.12 | 149.45±0.99 | 129.45±1.23 |
Day 21 PT | 91.7±1.27 | 463.00±1.17 | 96.84±0.62 | 111.13±12.2 | 196.11±7.52 | 126.20±1.23 | 119.11±18.16 | 103.08±15.67 | 98.11.08±4.67 |
Pre-T = Pre-treatment, PT = Post treatment
Table 3: Change on blood glucose level (mean±SD, mg/dl) in groups of normal and Streptozotocin (STZ) induced diabetic Rats (n=8)
|
| Induced Diabetics | |||||||
Parameters | Control | Diabetic control | glibenclamide | pioglitazone | Treatment Groups with Solanum Nigrum crude | ||||
|
|
|
|
| 100 | 200 | 300 | 400 | 500 |
Day 0 Pre-T | 180.11±0.33 | 209.34±0.51 | 188.00±0.15 | 191.02±1.15 | 186.30±0.27 | 201.42±0.18 | 206.11±0.22 | 205.9±0.77 | 211.9±0.45 |
Day 7 PT | 200.01±0.43 | 198.01±0.16 | 206.01±0.27 | 211.23±0.17 | 194.00±0.37 | 189.00±0.27 | 204.22±0.18 | 210.00±0.47 | 215.00±0.65 |
Day 14 PT | 189.00±0.45 | 178.33±1.22 | 219.00±0.15 | 221.12±0.13 | 197.33±1.64 | 177.40±0.55 | 217.42±0.17 | 213.12±0.56 | 217.12±0.77 |
Day 21 PT | 203.67±2.78 | 159.45±3.13 | 238.03±0.19 | 247.45±1.39 | 200.23±4.39 | 165.00±1.33 | 208.19±0.34 | 217.14±1123 | 223.14±1.28 |
Pre-T = Pre-treatment, PT = Post treatment
Table 4: Changes on body weight (mean ±SD, mg/dl) in groups of normal and Streptozotocin (STZ) induced diabetic Rats (n=8)
|
| Induced Diabetics | |||||||
Parameters | Control | Diabetic control | glibenclamide | pioglitazone | Treatment Groups with isolated Campesterol (µg/dl) | ||||
|
|
|
|
| 100 | 200 | 300 | 400 | 500 |
Day 0 Pre-T | 89.7±5.12 | 258.72±2.44 | 258.50±0.93 | 315.13±1.51 | 306.56±1.37 | 323.17±1.26 | 342.87±1.67 | 329.89±1.17 | 336.14±4.22 |
Day 7 PT | 91.8±1.11 | 316.63±1.00 | 215.89±0.71 | 208.19±1.26 | 296.46±0.43 | 212.32±0.29 | 199.44±0.14 | 146.78±1.23 | 124.45±1.43 |
Day 14 PT | 92.3±0.42 | 338.00±0.45 | 162.79±0.21 | 146.26±2.12 | 218.66±0.39 | 198.13±0.21 | 157.08±0.17 | 120.45±0.16 | 100.11±1.22 |
Day 21 PT | 91.7±1.27 | 463.00±1.17 | 96.84±0.62 | 111.13±1.25 | 169.11±1.64 | 154.20±1.22 | 108.11±1.13 | 98.08±11.65 | 73.09±0.13 |
Pre-T = Pre-treatment, PT = Post treatment
Table 5: Change on blood glucose level (mean±SD, µg/dl) in groups of normal and Streptozotocin (STZ) induced diabetic Rats (n=8)
|
| Induced Diabetics | |||||||
Parameters | Control | Diabetic control | glibenclamide | pioglitazone | Treatment Groups with isolated Campesterol (µg/dl) | ||||
|
|
|
|
| 100 | 200 | 300 | 400 | 500 |
Day 0 Pre-T | 180.11±0.33 | 209.34±0.57 | 188.00±0.16 | 191.02±1.19 | 184.30±0.22 | 203.42±0.19 | 205.11±0.23 | 208.9±0.18 | 209.9±0.36 |
Day 7 PT | 200.01±0.43 | 198.01±0.19 | 206.01±0.29 | 211.23±0.18 | 188.46±0.28 | 210±1.66 | 216.44±2.11 | 216.78±1.22 | 236.12±1.34 |
Day 14 PT | 189.00±0.45 | 178.33±1.25 | 219.00±0.17 | 221.12±0.16 | 190.26±0.39 | 221.13±0.48 | 230.08±1.33 | 229.45±1.57 | 239.16±0.67 |
Day 21 PT | 203.67±2.78 | 159.45±3.14 | 238.03±0.24 | 247.45±1.38 | 192.11±3.57 | 199.20±2.29 | 238.11±4.12 | 241.08±1.87 | 249.34±1.64 |
Table 6: Changes on body weight (mean ±SD, µg /dl) in groups of normal and Streptozotocin (STZ) induced diabetic Rats (n=8)
Discussion
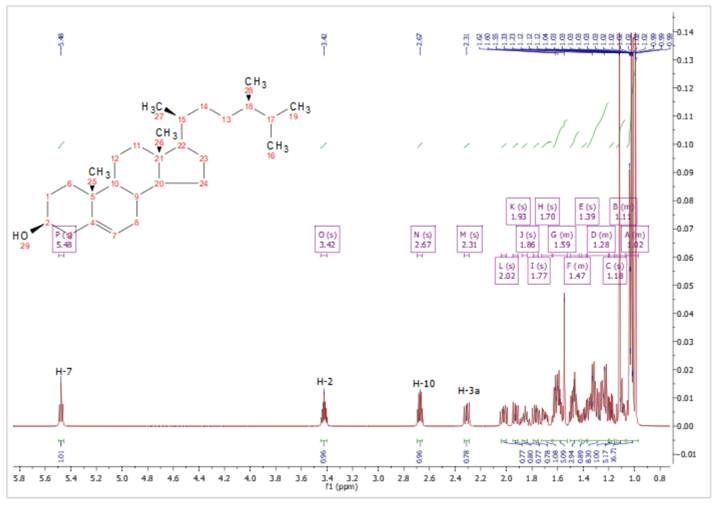
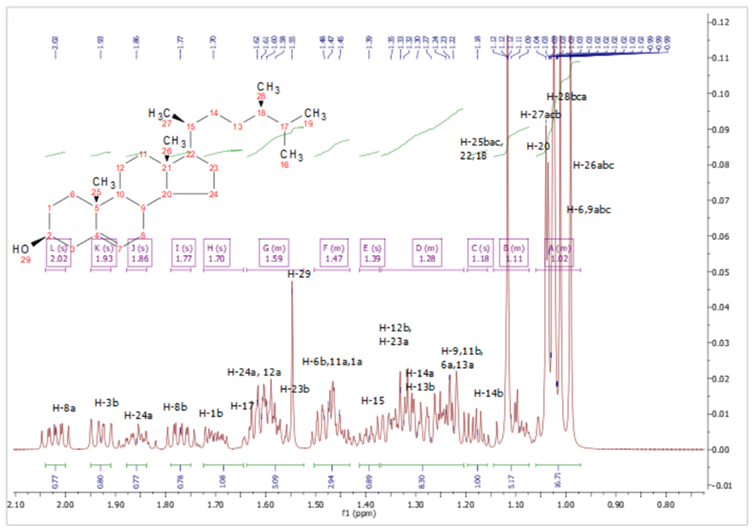
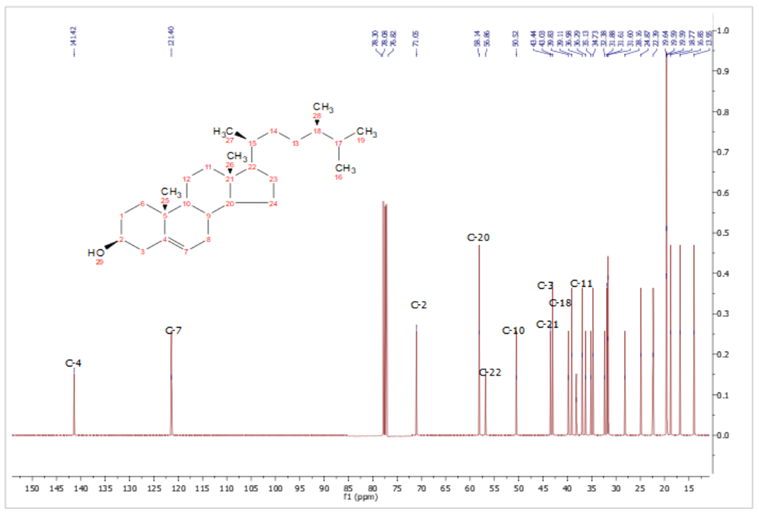
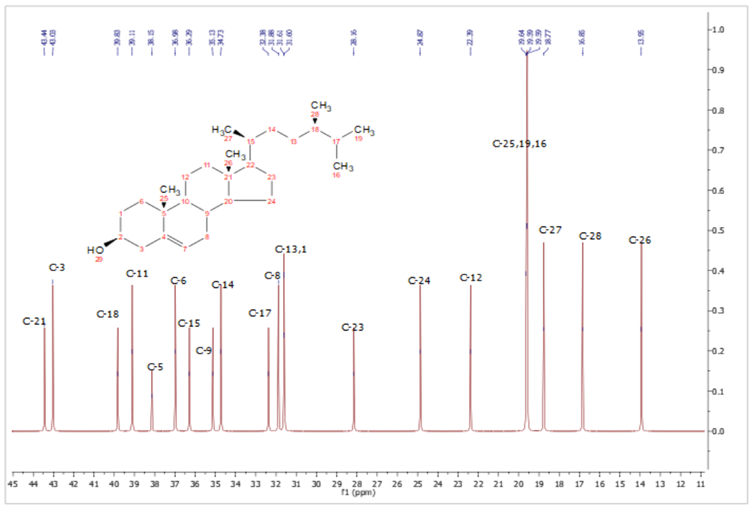
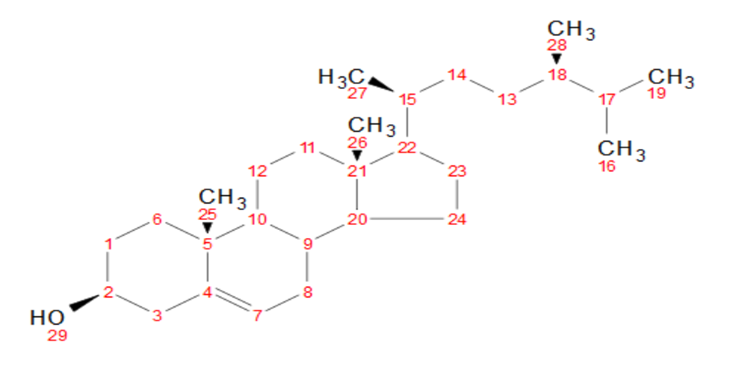
Data from the isolated compound gives a formulas C29H48O, which was supported by the 13C-NMR and 1H-NMR spectrum. The isolated compound showed characteristic absorption frequency. IR spectrum (KBr) at 3341.62 (O-H stretching) and C=C vibration was shown at 1653.34 cm-1. Other absorption peaks includes 1384.78 (CH2), 1277 cm-1 (C-H) and cycloalkane at 878.61 cm-1. The Physical characteristics of the isolated compound a pale yellow powder, m.p. 157-158oC.
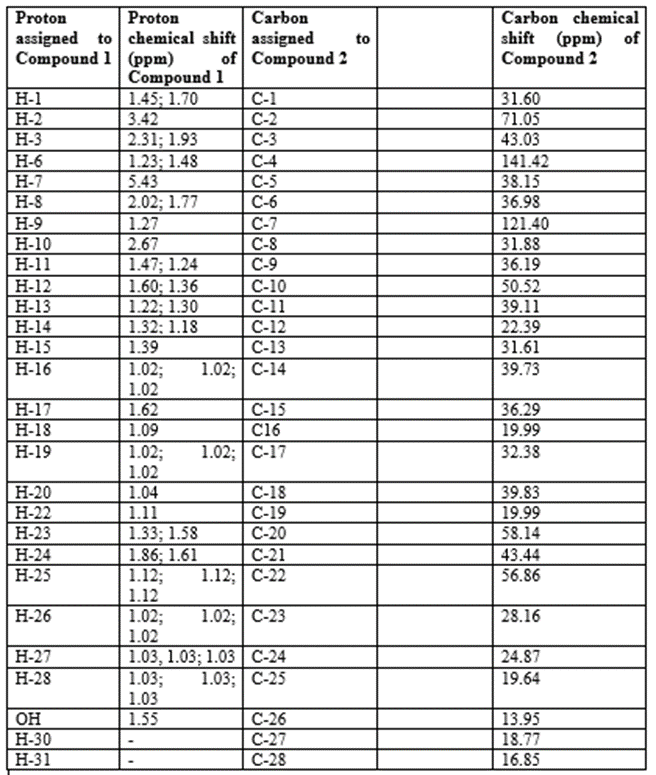
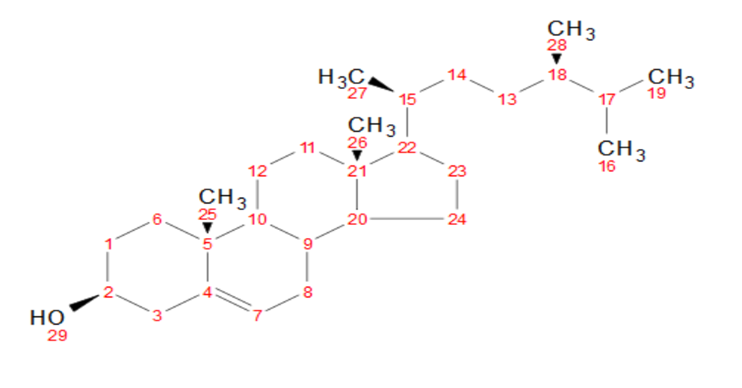
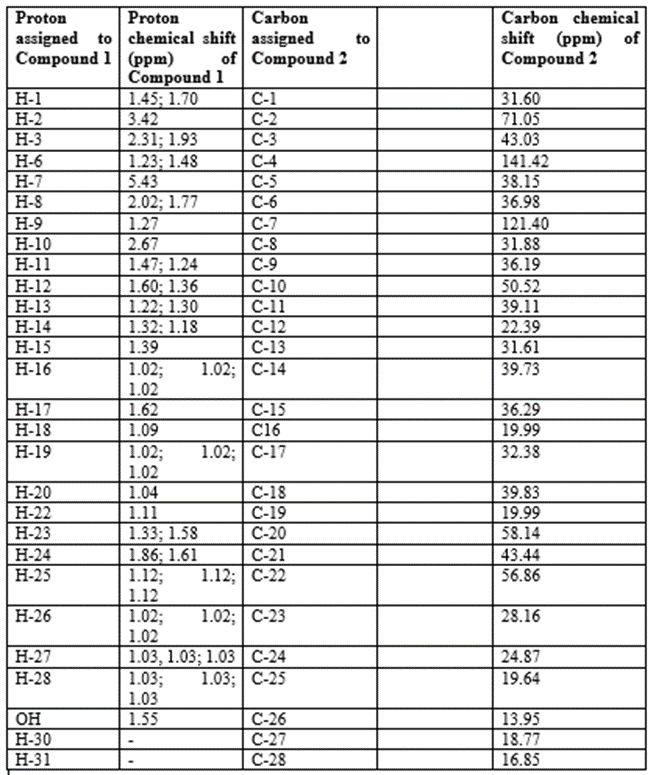
The 1H-NMR (ppm) spectrum showed 43 resonance, six methyl (CH3) groups and one olefenic group at δ 1.02, δ 1.02, δ 1.12, δ 1.02, δ 1.03, δ 1.03 and δ 1.03, respectively, they were assigned to H-16, H-19, H-25, H-26, H-27 and H-28. A hydroxyl group was observed at δ 1.55 an assigned to OH group. As shown in Table 1 the 13C-NMR showed 28 carbon resonance, the structure of the isolated compound was assigned as shown in Table 1 which correspond to the proposed campesterol with chemical structure of C28H43O as shown in Figure 10.
The cytotoxicity of the Crude extracts and pure substances into toxic were classified into toxic (LC50 value < 1000> 1000μg/ml) according to reports of Meyer et al. (1982). In this test majority of the extracts (four out of five) showed good brine shrimp larvicidal activity. Chloroform extract of Solanum Nigrum and the isolated compound (campesterol) was found to be highly effective (LC50 =10.54 μg/ml and 18.46 μg/ml) whereas Hexane, dichloromethane and ethyl acetate showed considerable action and their LC50 values were 24.09 μg/ml, 27.59 μg/ml, and 27.41 μg/ml, respectively. Natural products play an important role in and they offer valuable source of compounds with a wide variety of biological activities and chemical structures which provide important prototypes for the development of novel drugs (Schwartsmann, 2000; Vuorela et al., 2004). This is also true for anti-diabetes, anti-cancer agents, most of which have been derived from natural sources; directly as pure native compounds, or as semi-synthetic analogs, or as models for synthetic compounds (Lindholm, 2005). The correlation between the brine shrimp lethality assay and in vitrogrowth inhibition of human solid tumour cell lines shows the value of this bioassay as a pre-screening tool for anti-tumour drug research (Anderson et al., 1991).
Qualitative phytochemical analysis results (Table II) shows that all the plant extracts in this investigation possess one or different types of secondary metabolites. The isolation of campesterol is another novel in the study of Solanum Nigrum leaves crude extract.
The evolution of the anti-diabetes potentials of the crude and campesterol, after the blood sugar level was increased as compared to the rats with normal blood sugar level. Group 1 rats had normal blood glucose level and they were considered as the non-diabetes group whereas group 2-9 were considered as diabetic animals. It was shown that the blood glucose level >200 mg/dl were considered as diabetic. Rate of motility is high as in case of STZ used to induce the diabetes in rats.
In this study, diabetes was induced in rats by single intraperitoneal injection of streptozotocin (50 mg/kg b.wt.). However, at the end of 21 days of treatment, there was a decrease of blood glucose levels with the glibenclamide, the isolated compound and total crude extract of plant (500 mg/kg) respectively when compared with diabetic control group as shown in Table 1. Streptozotocin induced diabetic rats showed significant reduction in body weight as compared to normal group. At the end of 21 days treatment, the body weight of normal rats, treated with aqueous combined plant extract and standard drug treated group increased significantly, whereas body weight of diabetic control group rats decreased as shown in Table 2.
We are made to understand that diabetes mellitus is a heterogeneous group of metabolic disorders characterized by high blood glucose level. Since ancient times plants have been extemporary source of medicine. Since ancient times, plants and plant extracts were used cost-effectively worldwide to treat diabetes. In fact, in many parts of the world, especially poor countries, this may be the only form of therapy available to treat diabetes patients. Therefore, traditional medicine offers promising solutions to face the global increasing demands for new therapeutic agents. Insufficient data exist for most plants to guarantee their quality, efficacy and safety (Farnsworth, 1988).
Akilmoludun et al. (2007) described medicinal effects of plants which are often attributed to the antioxidant activity of the phytochemical constituents, mainly the phenolic. He also explained the synergistic relationship amongst phytochemicals is responsible for the overall beneficial effect derivable from plants (
Treatment of these compound campesterol and the total crude extract showed significant blood glucose lowering effect in diabetic rats which was comparable showed significant blood glucose lowering effect in diabetic rats which was comparable to the blood glucose lowering effect of known standard anti-diabetic drug. The fusion of phytomedicinal plants (Solanum Nigrum) and its isolates (campesterol) was found to be very effective in the treatment of diabetes. They inhibit the postprandial rise in hyperglycaemia in STZ-induced diabetes comparable to that of standard anti-diabetic drug (glibenclamide, pioglitazone).
Conclusion
In conclusion, campesterol isolated from leaves crude extract of Solanum Nigrum has proven itself to be nature’s extraordinary therapeutic agent and it has also been proved during the course of this work. It has also been proved that, Solanum Nigrum is a potent medicinal plant and attention should be spent on developing it as a sustainable drug for prophylaxis and treatment of complications such as diabetes and other diseases.
Acknowledgements
The authors wish to express their appreciation to all the technical staffs of the laboratory unit of Natural product, the Department of Microbiology, Biochemistry, Faculty of Resource Science and Technology Universiti Malaysia Sarawak for their support and all the technical assistance rendered during the course of this research work.
Conflict of Interest
The authors declare no conflict of interest.
References
- World Health Organization. (2003). Diet, nutrition, and the prevention of chronic diseases: report of a joint WHO/FAO expert consultation (Vol. 916). World Health Organization.
View at Publisher | View at Google Scholar - Umaru, I. J., Badruddin, F. A., & Umaru, H. A. (2019). Phytochemical screening of essential oils and antibacterial activity and antioxidant properties of Barringtonia asiatica (L) leaf extract. Biochemistry Research International, 2019.
View at Publisher | View at Google Scholar - Ntie-Kang, F., Mbah, J. A., Mbaze, L. M., Lifongo, L. L., Scharfe, M., Ngo Hannam J., Cho-Ngwa, F., Onguéné, P. A., Owono, L. C. O., Megnassan, E., Sippl, W. & Efange, S. M. N. (2013). CamMedNP: Building the Cameroonian 3D structural natural products database for virtual screening. BMC Complementary Alternative Medicine, 13, 88-96.
View at Publisher | View at Google Scholar - Jain, R., Sharma, A., Gupta, S., Sarethy, I. P., & Gabrani, R. (2011). Solanum nigrum: current perspectives on therapeutic properties. Altern Med Rev, 16(1), 78-85.
View at Publisher | View at Google Scholar - Rani, Y. S., Reddy, V. J., Basha, S. J., Koshma, M., Hanumanthu, G., & Swaroopa, P. (2017). A review on Solanum nigrum. World J. Pharm. Pharm. Sci, 6, 293-303.
View at Publisher | View at Google Scholar - Miraj, S. (2016). Solanum nigrum: A review study with anti-cancer and antitumor perspective. Der Pharma Chemica, 8(17), 62-68.
View at Publisher | View at Google Scholar - Dilip, K. J., Saroja, K., & Murthy, A. R. V. (2012). Pharmacognostic study of Kakamachi (Solanum nigrum Linn). Journal of Pharmaceutical and Scientific Innovation (JPSI), 1(4), 42-48.
View at Publisher | View at Google Scholar - Umaru, I. J., Boyi, R. H., Miyel, M. H., Kukoyi, A. J., & Umaru, K. I. (2018). Antidiabetic Potentials of Leaves Extract of Barringtonia racemosa (L) in Alloxan-Induced Albino Rats. American Journal of Pharmacology and Pharmacotheraphy, 5(2), 5.
View at Publisher | View at Google Scholar - Govindappa, M. (2015). A review on role of plant (s) extracts and its phytochemicals for the management of diabetes. J Diabetes Metab, 6(7), 1-38.
View at Publisher | View at Google Scholar - Adnette, F.N., Ulbad, T. P., Magloire, N., Ruffine, F., Koutinhouin, G. B., & Akadiri, y. (2019). Diabetes mellitus: classification, epidemiology, physiopathology, immunology, risk factors, prevention and nutrition. International Journal of Advanced Research (IJAR), 7(7), 855-865.
View at Publisher | View at Google Scholar - American Diabetes Association. (2009). Diagnosis and classification of diabetes mellitus. Diabetes care, 32(Supplement 1), S62-S67.
View at Publisher | View at Google Scholar - Fall, C. H., Osmond, C., Haazen, D. S., Sachdev, H. S., Victora, C., Martorell, R., ... & Richter, L. M. (2016). Disadvantages of having an adolescent mother. The Lancet Global Health, 4(11), 787-788.
View at Publisher | View at Google Scholar - World Health Organization. (2019). Classification of diabetes mellitus.
View at Publisher | View at Google Scholar - Bai, J., Gao, Q., Wang, C., & Dai, J. (2019). Diabetes mellitus and risk of low-energy fracture: a meta-analysis. Aging clinical and experimental research, 1-14.
View at Publisher | View at Google Scholar - Durruty, P., Sanzana, M., & Sanhueza, L. (2019). Pathogenesis of type 2 diabetes mellitus. In Type 2 Diabetes-From Pathophysiology to Modern Management. IntechOpen.
View at Publisher | View at Google Scholar - Sami, W., Ansari, T., Butt, N. S., & Ab Hamid, M. R. (2017). Effect of diet on type 2 diabetes mellitus: A review. International journal of health sciences, 11(2), 65.
View at Publisher | View at Google Scholar - Herath, H., Herath, R., & Wickremasinghe, R. (2017). Gestational diabetes mellitus and risk of type 2 diabetes 10 years after the index pregnancy in Sri Lankan women-A community based retrospective cohort study. PloS one, 12(6), e0179647.
View at Publisher | View at Google Scholar - Salman, Y. J., Ahmed, E. S., & Taqi, R. H. (2018). International journal of current research and academic review. Int. J. Curr. Res. Aca. Rev, 6(10), 39-50.
View at Publisher | View at Google Scholar - Gupta, R., & Sharma, A. K. (2017). Anti-hyperglycemic activity of aqueous extracts of some medicinal plants on wistar rats. J Diabetes Metab, 8(752), 2.
View at Publisher | View at Google Scholar - Jain, P. S., & Bari, S. B. (2010). Isolation of lupeol, stigmasterol and campesterol from petroleum ether extract of woody stem of Wrightia tinctoria. Asian Journal of Plant Sciences, 9(3), 163.
View at Publisher | View at Google Scholar - Farnsworth, N. R. (1988). Screening plants for new medicines. Biodiversity, 15(3), 81-99.
View at Publisher | View at Google Scholar - Akinmoladun AC, Ibukun EO, Afor E, Obuotor EM, Farombi EO (2007). Phytochemical constituent and antioxidant activity of extract from the leaves of Ocimum gratissimum. Science Research Essay 2: 163-166.
View at Publisher | View at Google Scholar
