

Research Article | DOI: https://doi.org/10.31579/2835-2882/030
Catheter Guided Central Venous Ultrasound in Pediatric Patients: Experience in A Hospital of Second Level in Mexico
- Nayeli Reyes Reyes 1
- Eliazib Natarén Cigarroa 2*
- Edgar Guadarrama Granados 3
- Karina Guadalupe Flores Sánchez 4
- Fernando Ruiz Balbuena 5
1 Medical Specialist Pediatrician, of the Hospital Dr. Gilberto Gomez Jesus Maza.
2 Master Nurse in Public Health, Head of the Intrevenous Therapy Team of the Dr. Jesus Gilberto Gomez Maza Hospital.
3 Medical Specialist in Critical Medicine Pediatrician, Head of the Unit Intensive Care Pediatrics of the Hospital Dr. Gilberto Gomez Jesus Maza.
4 Medical Specialist in pediatric surgery of the Hospital.
5 Doctor of Pharmacology, Head of the teaching and research department of the Hospital.
*Corresponding Author: Eliazib Natarén Cigarroa; Master Nurse in Public Health, Head of the Intrevenous Therapy Team of the Dr. Jesus Gilberto Gomez Maza Hospital, Mexico.
Citation: Nayeli R. Reyes, Eliazib N. Cigarroa, Edgar G. Granados, Flores Sánchez KG, Fernando R. Balbuena, (2023), Catheter guided central venous ultrasound in pediatric patients: experience in a hospital of second level in Mexico, Clinical Research and Studies, 2(4); DOI:10.31579/2835-2882/030
Copyright: © 2023, Eliazib Natarén Cigarroa. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 08 August 2023 | Accepted: 18 August 2023 | Published: 31 August 2023
Keywords: vascular access; ultrasound; pediatrics; catheterization
Abstract
Objective: To compare the number of attempts, procedure time and complications in pediatric patients at the Dr. Jesús Gilberto Gómez Maza hospital in two groups with an indication for the installation of a central venous catheter (CVC).
Methodology: Randomized clinical trial at the Hospital Dr. Jesús Gilberto Gómez Maza, from southeastern Mexico; in the Pediatrics service, which includes pediatric emergency room, pediatric intensive care unit, pediatric hospitalization and operating room for all pediatric patients aged 1 month to 15 years with 11 months hospitalized during the period January 1, 2017 to December 31 of 2018 that required the installation of a CVC with a blind technique versus the ultrasound-guided technique.
Results: A total of 585 patients with indication for CVC installation were included, with distribution of 248 women (42.4%) and 337 men (57.6%), the highest frequency being in the pediatric emergency service, with 388 patients (66.3%), followed by pediatrics with 94 (16.1%). In 471 patients a central and femoral insertion catheter was used (80.5%) and in 114, a peripheral insertion central catheter was used (19.5%). Of the 585 patients, in 448 in cases, the CVC was installed with a blind technique (76.6%) and 137 guided by ultrasound (23.4%) Complications (hematoma, hemorrhage, hemothorax, hydrothorax, catheter material failure, misplacing, multipuncture, arterial puncture, stenosed vein and Venodisection) observed with the blind technique, 107 (23.8%) were recorded and with the ultrasound-guided technique, 9 (6.5%). Of the 137 patients with ultrasound-guided CVC, 92 the procedure time took between 10 to 20 minutes ( 67.1%), and with blind technique, 326 (72.7%) the ti me of hard procedure between 21 and 60 minutes. Regarding the number of punctures, it was observed that the proportions were similar, in the sense that the majority received 1 to 2 punctures for the ultrasound-guided technique (91%), and the blind technique (88.1%).
Conclusions: The insertion of the ultrasound-guided central venous catheter in pediatric patients is an effective and safe technique, with which complications and time during the procedure are significantly reduced.
Introduction
Central venous catheterization is a commonly used technique to gain access to the jugular, subclavian, and femoral veins for hemodynamic monitoring, long-term fluid administration, antibiotics, total parenteral nutrition, and hemodialysis. As a result of this, central venous access has become one of the main forms of treatment in critically ill patients1.
The first ultrasound-guided venous catheterization was performed almost 40 years ago, and over the past 10 years, the development of portable ultrasound devices has made this technique more affordable2.
In a study carried out in London, a group of participants in relation to ultrasound-guided insertion, who had no previous experience, was compared to evaluate learning curves regarding placement of vascular accesses with blind technique and that assisted by ultrasound guidance, finding how The result was a lower rate of punctures in the last group, as well as improvement when overcoming learning curves with fewer punctures, which allowed establishing the method as a more competent path with a greater degree of safety3.
In another study carried out in Paraguay, 149 patients over 18 years of age were evaluated, with an indication for programmed placement of a central venous catheter in the internal jugular vein, performing 90 approaches with ultrasound guidance and 59 by blind technique, with a finding of time of completion and number The number of punctures was lower in the group with ultrasound guidance, as well as a lower proportion of complications4.
Another study carried out in the Intensive Care Unit of Hospital Ángeles Pedregal, Mexico, evaluated a group of 35 patients, in which it was sought to identify the efficacy of central venous catheter placement with the use of ultrasound and complications attributable to the procedure , finding a successful placement of 33 of the 35 catheters, with a success rate of 94.28%, scoring the use of ultrasound for the placement of a central vascular access as an effective procedure with a low rate of complications5.
The use of ultrasound to guide the catheterization of vascular structures offers theoretical advantages and promises to make the installation of vascular accesses a precise and safe technique, reducing complications and decreasing the insertion time of catheters. found focused on adult patients.
In our unit, catheterization of ultrasound-guided vascular accesses is frequent in the pediatric population, which is why this research showed that the advantages obtained through this procedure exceed the results obtained in comparison to the placement of vascular accesses performed using anatomical landmarks.
4. Objectives
4.1.- General objective
To compare the insertion of an ultrasound-guided central venous catheter in two groups versus the blind technique in pediatric patients, from the Dr. Jesús Gilberto Gómez Maza second-level care hospital in the period from January 1, 2017 to December 31, 2018.
4.2.- Specific objectives
4.2.1. Demonstrate that the ultrasound-guided placement of a central venous catheter has fewer complications compared to the blind technique.
4.2.2. Determine the number of punctures performed with each technique.
4.2.3. Know the average time of central venous catheter placement with ultrasound guidance and blind technique.
4.2.4. Identify the least traumatic technique with the fewest associated immediate complications.
5. Methodology
5.1 Study design
Randomized clinical trial
5 .2 Description of the study area
The present investigation was carried out at the Chiapas Hospital unites us Dr. Gilberto Gómez Maza located in the city of Tuxtla Gutiérrez, Chiapas; in the Pediatric service, which includes the areas of pediatric emergencies, pediatric intensive therapy, pediatric hospitalization and operating rooms. The CVCs were installed by pediatric doctors, pediatric residents, a PICC Team and the Hospital's Intravenous Therapy Team (ETI); Variables such as time, number of punctures, and complications were measured through a CVC installation check list, protocolized and standardized by the Hospital ETI regulated by the Mexican government, applied by trained nursing personnel during the insertion of a CVC.
5 .3 Population
Pediatric patients from 1 month to 15 years with 11 months of age who were hospitalized in the medical unit during the period January 1, 2017 to December 31, 2018 that required the installation of a central venous access, independent of the underlying pathology.
5.4. Definition of study units
5.4.1. Inclusion criteria
5.4.1.1. Pediatric patients
5.4.1.2. Male and female gender
5.4.1.3. Patients requiring central vascular access placement
5.4.1.4. Patients who enter the service in the aforementioned period of time.
5.4.1.5. Patients who have an informed consent signed by a parent or guardian.
5.4.2. Exclusion criteria
5.4.2.1. Patients undergoing emergency surgery.
5.4.2.2. Patients with a history of coagulopathies.
5.4.2.3. Patients with incomplete information (incorrect / incomplete data collection format).
Ethical aspects and patient consent
The preliminary draft was submitted to the hospital's research committee, for its registration and its corresponding approval. An informed consent form was structured and signed by the children's parents when they agreed to participate in the study. The data and identity of each patient were protected according to the Helsinki convention, maintaining anonymity and in compliance with the law on data protection and human rights of minors of the State of Chiapas, Mexico.
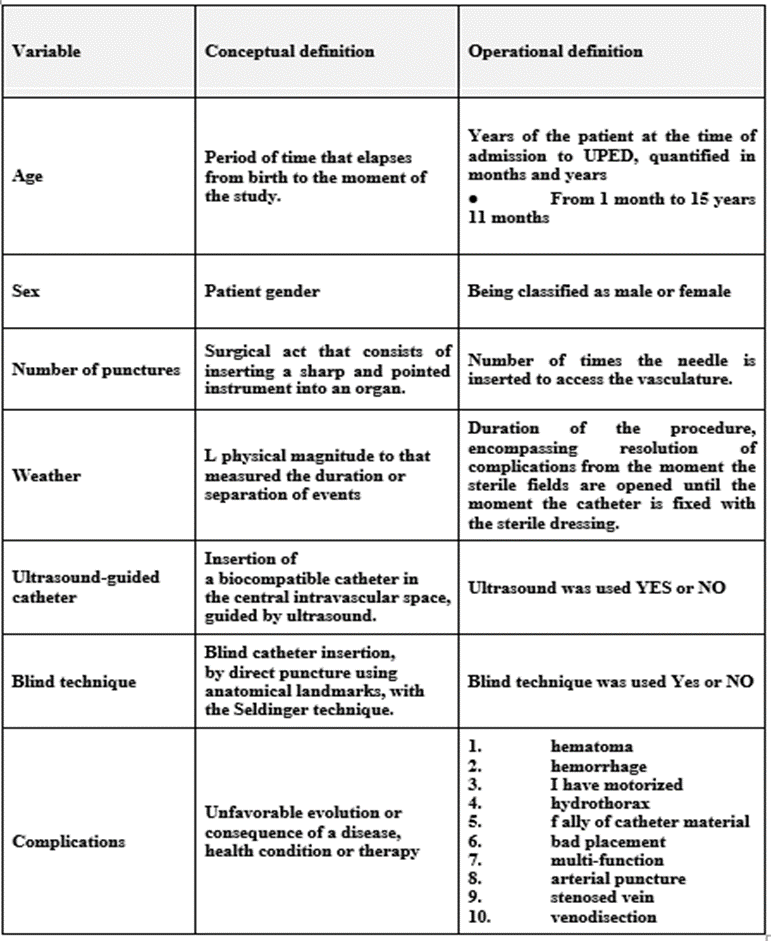
Table 5 .5. Conceptual and operational definition of variables
5.6 Instrument and data collection method
A data collection sheet was prepared that included all the variables already described in table 6.5 and later a form was created in the statistical program EPI-INFO version 3.4.
5 .7 Data Analysis Plan
The information collected was emptied into a database in the aforementioned statistical program, percentages, averages and standard deviations were calculated, statistical tests were used to cross variables. Subsequently, a bivariate analysis was performed; Using the X2 statistic, a p value less than 0.05 was considered a statistically significant value.
6. Results
In the present investigation, a total of 585 patients cared for in the Pediatric service at the Hospital “Dr. Jesús Gilberto Gómez Maza”, 248 were women (42.4%) and 337 were men (57.6%); see table 6.1.
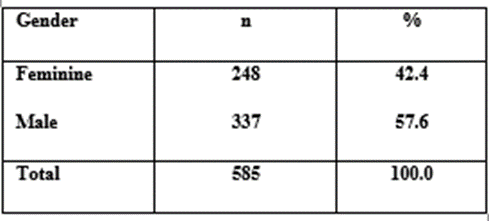
Table 6.1: Population distribution according to gender
Of the 585 patients included in the study, according to the care service, the largest number of patients corresponded to the pediatric emergency service, with 388 patients (66.3%), followed by patients from the pediatric service with 94 (16.1%), in pediatric intensive care with 89 (15.2%), and finally 14 patients in the operating room (2.4%); see table 6.2.
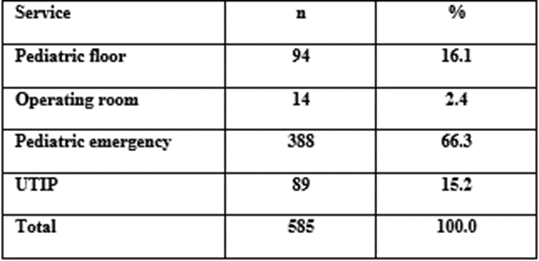
Table 6.2: Care service according to placement of vascular access
Of the 585 patients undergoing catheterization, 471 patients underwent central venous and femoral insertion catheterization (CICC and FICC) (80.5%) and in 114, placement of the peripherally inserted central catheter (PICC) was performed (19.5 %); see table 6.3.
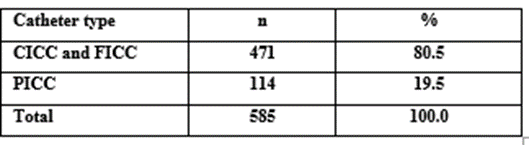
Table 6.3: Type of venous access approach
Regarding the installation technique, of the 585 patients, in 448 cases the vascular access was approached using a blind technique due to anatomical repairs (76.6%) and 137 guided with ultrasound (23.4%), see table 6.4.
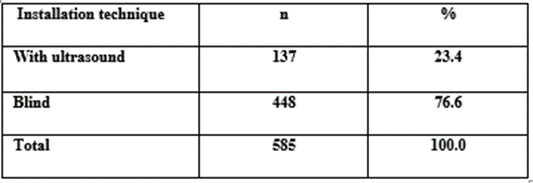
Table 6.4: Distribution of number of approaches according to installation technique
Regarding complications such as (hematoma, hemorrhage, hemothorax, hydrothorax, catheter material failures, misplacement, multi-function, arterial puncture, stenosed vein and venodisection), observed with the blind technique, 107 (23.8%) and with the technique guided by ultrasound, 9 (6.5%). This difference was statistically significant (X2 = 19.80; p-value = 0.0000); see Figure 6.1.
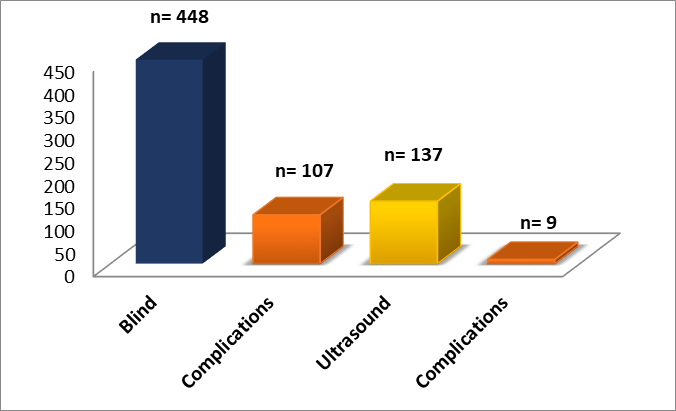
Figure 6.1: Frequency of complications associated with the installation technique
Of the 137 patients who underwent catheterization guided by ultrasound, 92 the procedure time took between 10 to 20 minutes (67.1%), and 326 (72.7%) who were approached with a blind technique, the procedure time lasted between 21 and 60 minutes. That is, the procedure time was significantly shorter with the first technique than with the second (X2 = 129.45; p-value = 0.0000). See table 6.5.
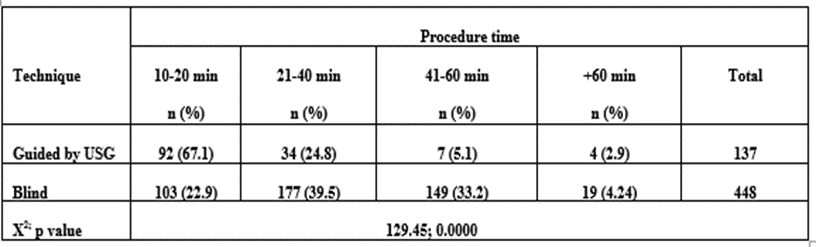
Table 6.5: Procedure time according to approach technique
When the number of punctures was evaluated, it was observed that the proportions were similar, in the sense that the majority received 1 to 2 punctures for the ultrasound-guided technique (91%), such as the blind (88.1%); X2 = 1, p-value = 0.3168. See table 6.6.
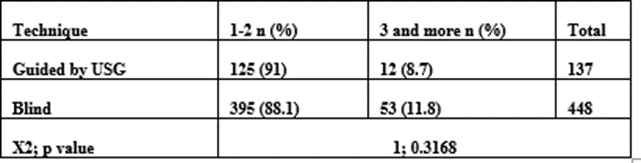
Table 6.6: Distribution of number of punctures by approach technique
7. Discussion
With current technological advances, it is possible to place ultrasound within the reach of hospital units with its implementation in the insertion of central accesses, thus reducing the risk of complications. For the application of catheters, it has been verified in several studies, when a procedure is performed with an ultrasound-guided technique, it represents advantages, versus conventional technique. However, reports of the application of this procedure in critical patients in pediatric units are still limited worldwide36.
In the present investigation, it has been corroborated in the first instance that complications are significantly lower when the procedure was performed with the ultrasound-guided technique (6.5%), than with the blind technique (23.8%). This result is very similar to a study carried out by Uruguayan researchers, who registered a lower proportion of complications, with the use of an ultrasound-guided technique4.
Likewise, in another study carried out in Mexico City, where the installation of a central venous catheter is evaluated by ultrasound, a success rate of 94.2% was reported; Regarding complications, they only reported two cases associated with immediate complications, being arterial puncture and hemothorax5.
On the other hand, in a meta-analysis carried out in Germany, with a sample of 5,108 patients, where the cannulation of the internal jugular vein was assessed using an ultrasound-guided technique, a reduction in the total rate of complications was found, compared to the blind technique37.
Regarding the time involved in performing the procedure, it was also observed that the ultrasound-guided technique was performed in a significantly shorter time, since most of it was performed between 10 and 20 minutes (%), while with the blind technique, The vast majority were carried out between 20 and 60 minutes, these data are similar in research carried out by Venezuelan doctors, where they confirm a lower access time in the group evaluated by means of an ultrasound-guided technique with 27 minutes, while in the group with approach by blind technique was 48 minutes on average1.
Regarding the number of punctures, no significant differences were found, however, in a study carried out in a hospital in Venezuela, it was found that the number of punctures was lower using an ultrasound-guided approach technique1.
8. Conclusions
The present work concludes that central venous catheterization using an ultrasound-guided technique in pediatric patients is an effective and safe technique, with which complications and installation time are significantly reduced. However, we believe that to achieve the best skill level for central venous catheter placement, knowledge of the blind technique and knowledge of ultrasound-guided catheter placement must be combined and integrated.
The duration of the ultrasound procedure was performed in a shorter time, from 10 to 20 minutes, which makes it a very useful technique in the management of pediatric patients who require rapid central venous cannulation for timely care.
The immediate complications that occur with the use of ultrasound are minor and in our case they occurred in only 9 children, and they did not represent a high risk for the patients and did not prevent the success of the procedure.
The results obtained in this study can be taken to implement strategies that involve the integration of an ultrasound equipment available in critical areas, as well as training for medical and nursing personnel, who at a certain moment can carry out the procedure, whose priority objective is to improve the survival of our patients, thus improving the quality of care offered.
10. Annexes
References
- Marin RS, Salazar W, Reyna VE, Mejia MJ, Reyna VN, et al. (2014). Central venous catheterization guided by ultrasound or by anatomical points, MedULA Revista de Facultad de Medicina, Universidad de Los Andes, Vol. 23. No. 2, 24: 41-46.
View at Publisher | View at Google Scholar - Reusz G. Csomos A. (2015). The role of ultrasound guidance for vascular access, Current Opinion in Anesthesiology Volume 28- Issue 6- p710-716.
View at Publisher | View at Google Scholar - Jaffer U, Normahani P, Singh P, Aslam M, Standfield NJ;(2015). Randomized study of teaching ultrasound-guided vascular cannulation using a phantom and the freehand versus needle guide-assisted puncture techniques, Journal of Clinical Ultrasound, Vol. 43, No. 8, p469-477.
View at Publisher | View at Google Scholar - Acosta CDD; (2017). Ultrasound-guided catheterization of the internal jugular vein: comparative study with the conventional technique for anatomical landmarks, Rev. virtual Soc. Parag. Med. Int. 4 (1): 57-65.
View at Publisher | View at Google Scholar - Vidal AE, Hernández CC, Carrillo SCR, Esponda JGP; Central venous catheter installation by ultrasound. Experience of the Intensive Therapy Unit of Hospital Ángeles Pedregal, Acta Medica Grupo Ángeles, Volume 15.
View at Publisher | View at Google Scholar - Duran BG;(2010). High-resolution ultrasound-guided angioacces in cancer patients, Revista Mexicana de Oncologia Vol. 33 Suppl. 1, p S510-S15.
View at Publisher | View at Google Scholar - Soni NJ, Arntfield R, Kory P; (2016). Bedside ultrasound. Fundamentals of Clinical Ultrasound Elsevier Spain.
View at Publisher | View at Google Scholar - McLario DJ, Sivitz AB (2015). Point-of-Care Ultrasound in Pediatric Clinical Care. JAMA Pediatr. 169 (6): 594-600.
View at Publisher | View at Google Scholar - Menéndez SJJ (2018). Ultrasound-guided vascular canalization: option or obligation. Evid Pediatr. 2018; 14: 1.
View at Publisher | View at Google Scholar - Lau CSM, Chamberlain RS (2016). Ultrasound-guided central venous catheter placement increases success rates in pediatric patients: a meta-analysis. Pediatr Res, 8; 80 (2): 178–84.
View at Publisher | View at Google Scholar - Vargas JF, Mejía JA, Gómez CM, Restrepo CE; (2013). Ultrasound-guided vascular accesses in children, Revista de Cirugía Pediátrica Vol. 3, No. 1.
View at Publisher | View at Google Scholar - Enriquez JL, Wu TS; (2014).an Introduction to Ultrasound Equipment and Knobology. Crit Care Clin. 30 (1): 25–45.
View at Publisher | View at Google Scholar - Baique SPM; (2016). Basic aspects of central venous access with ultrasound guidance; Rev Hisp Cienc Salud, 2 (1): 62-70.
View at Publisher | View at Google Scholar - Bakhru RN, Schweickert WD;(2013). Intensive Care Ultrasound: I. Physics, Equipment, and Image Quality. Ann Am Thorac Soc, 10 (5): 540–548.
View at Publisher | View at Google Scholar - Urías E, Ortega J, Valenzuela H;(2017). Head to toe ultrasound in critical areas. First. Mexico: Editorial Prado;
View at Publisher | View at Google Scholar - Llorente FA;(2012). Sonographic canalization of central lines. An Pediatr Contin, 10 (6): 348–52.
View at Publisher | View at Google Scholar - Reusz G, Sarkany P, Gal J, Csomos A; (2014). Needle-related ultrasound artifacts and their importance in anesthetic practice. Br J Anaesth, 112 (5): 794–802.
View at Publisher | View at Google Scholar - White P;(2016). Ultrasound in the critically ill, Barcelona: Elsevier;
View at Publisher | View at Google Scholar - Amaya ZWF, Raffán SF, Niño de Mejía C, Hermida E, Alvarado SJ, (2015). Internal jugular venous cannulation: how much security can we offer? Rev Colomb Anestesiol, 43 (1): 76–86.
View at Publisher | View at Google Scholar - Smith RN, Nolan JP; (2013). Central venous catheters. BMJ, Nov 11; 347.
View at Publisher | View at Google Scholar - Married F J, García T; (2015). Central venous lines. Direct percutaneous cannulation. And emergency treatment of severe child. Third Ed. Madrid: Ergon;
View at Publisher | View at Google Scholar - Bodenham A,(2017). Vascular Acces; Rev. Med. Clin. Condes, 28 (5) 713-726.
View at Publisher | View at Google Scholar - Rivas TR;(2011). Mechanical complications of central venous accesses, Rev. Med. Clin. Counts, 22 (3) 350-360.
View at Publisher | View at Google Scholar - Parienti JJ, Mongardon N, Mégarbane B, Mira JP, Kalfon P, et al. (2015). Intravascular Complications of Central Venous Catheterization by Insertion Site. N Engl J Med, 24; 373 (13): 1220–9.
View at Publisher | View at Google Scholar - Lona RJC, López BB, Celis RA J, Pérez MJJ, Ascencio EEP;(2016). Central venous catheter-related bacteremia: incidence and risk factors in a hospital in western Mexico. Bol Med Hosp Infant Mex, 73 (2): 105-10.
View at Publisher | View at Google Scholar - Moureau N, Lamperti M, Kelly LJ, Dawson R, Elbarbary M, et al. (2013). Evidence-based consensus on the insertion of central venous access devices: definition of minimal requirements for training. 110: 347–356.
View at Publisher | View at Google Scholar - Subert M, Vailati D, Lamperti M, Caldiroli D;(2011). Advantages of using ultrasound as a guide for the placement of vascular accesses in pediatrics. Health and Science, 18 (6): 516–520.
View at Publisher | View at Google Scholar - Barr L, Hatch N, Roque PJ, Wu TS;(2014). Basic Ultrasound-guided Procedures. Crit Care Clin, 30 (2): 275–304.
View at Publisher | View at Google Scholar - Kim H, Jeong CH, Byon HJ, Shin HK, Yun TJ, et al. (2013). Predicting the optimal depth of left-sided central venous catheters in children. Anesthesia. 68 (10): 1033–1037.
View at Publisher | View at Google Scholar - Perin G, Scarpa MG;(2015). Defining central venous line position in children: tips for the tip. J Vasc Access, 16 (2): 77–86.
View at Publisher | View at Google Scholar - Souza NE, Grousson S, Duflo F, Tahon F, Mottolese C, et al. (2014). Ultrasonographic anatomic variations of the major veins in pediatric patients. Br J Anaesth, 1; 112 (5): 879–84.
View at Publisher | View at Google Scholar - Schindler E, Schears GJ, Hall SR, Yamamoto T (2012). Ultrasound for vascular access in pediatric patients. Pediatric Anesthesia. Vol. 22.
View at Publisher | View at Google Scholar - Hoffman T, Du Plessis M, Prekupec MP, Gielecki J, Zurada A, et al. (2017). Ultrasound guided central venous catheterization: A review of the relevant anatomy, technique, complications, and anatomical variations. Clin Anat, 30 (2): 23750.
View at Publisher | View at Google Scholar - Jöhr M, Berger TM; (2015). Venous access in children. Curr Opin Anesthesiology. 28 (3): 314–20.
View at Publisher | View at Google Scholar - Breschan C, Graf G, Jost R, Stettner H, Feigl G, et al. (2015).; Ultrasound-guided supraclavicular cannulation of the right brachiocephalic vein in small infants: a consecutive, prospective case series. Anderson B, editor. Pediatr Anesth. 25 (9): 943–949.
View at Publisher | View at Google Scholar - Oulego EI, Muñoz LA, Alonso QP, Rodríguez NA, (2016). Comparison of ultrasound guided brachiocephalic and internal jugular vein cannulation in critically ill children. Journal Critical Care, 35: 133–137.
View at Publisher | View at Google Scholar - Brass P, Hellmich M, Kolodziej L, Schick G, Smith AF, et al. (2015). Ultrasound guidance versus anatomical landmarks for internal jugular vein catheterization. Cochrane Database Syst Rev, 1: Cd006962
View at Publisher | View at Google Scholar
