

Case Report | DOI: https://doi.org/10.31579/2835-2882/024
Castleman Disease Versus Generalized Tuberculosis: a Case of Fever of Unknown Origin
Assistant in Internal Medicine in Alberto Sabogal National Hospital in Callao-Peru.
*Corresponding Author: Edgard Niño-Morin, Assistant in Internal Medicine in Alberto Sabogal National Hospital in Callao-Peru.
Citation: Edgard N. Morin, Daniel S. Morillos, Rafael B. Celis, (2023), Castleman Disease Versus Generalized Tuberculosis: a Case of Fever of Unknown Origin, Clinical Research and Studies, 2(4); DOI:10.31579/2835-2882/024
Copyright: 2023, Edgard Niño-Morin. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 04 July 2023 | Accepted: 18 July 2023 | Published: 28 July 2023
Keywords: castleman disease; tuberculosis; fever of unknown origin
Abstract
We present the case of a 25-year-old woman with fever of unknown origin, whose cervical node biopsy study was reported as Castleman disease, but who at follow-up turned out to be multisystem tuberculosis. I received antituberculous treatment with good clinical and laboratory evolution at follow-up. It is emphasized that, in the face of diseases of low prevalence, such as Castleman disease, tuberculosis should be ruled out in countries like ours.
Introduction
The tuberculosis was described from the antiquity by Sylvius (1695), giving it such a tuber nomination for the relationship of this disease with the presence of lymph nodes in the lungs found in individuals deceased, until he discovery of the bacillus by Robert Koch in 1882. In he
Peru reported that 119 out of 100,000 inhabitants can have tuberculosis and in 2019 there have been 31 764 new cases. It commonly manifests with fever, persistent cough, weight loss, and as more presentations atypical, such as pleural effusion, aseptic pyuria, scrofula, besides of conditions in different organs present in the tuberculosis systemic [1].
His diagnosis HE bases in evidence as the tuberculin that present 99% sensitivity and 95% specificity. Serum gamma interferon such as QuantiFERON -TB golden and he T-SPOT-TB are tools with sensitivity of the 70 and 90% and specificity of the 90 and 93%, respectively. smear microscopy by sputum has a sensitivity of the 90% He PCR has a sensitivity of the 85% and specificity of the 97% The gold standard test continues to be the crop with an 80% sensitivity and 90% specificity, with difficulty of the delay in the result that they can be weeks, in the case of the media solid [2]. He studies pathology of the injuries tubercular HE characterizes by the training of granulomas that are product of the inflammation chronicle, aggregation of macrophages, surrounded mainly by lymphocytes, plasma cells, alternately form necrosis, giant cell formation, and neoformations capillaries, the which they can see each other affected in view of disturbance of the immunity, by it which can simulate multiple diseases Chronicles, as brucellosis, abscesses and, inclusive, neoformations [3].
The disease of Castleman is a disorder lymphoproliferative of very low prevalence, described in the year 1956 by Castleman and Towne [4]. The hypothesis of his pathology HE bases in polymorphisms of the receiver of the interleukin 6, caused by various pathogens, among these the most studied we have HIV, HHV-8, generating a chronic inflammatory process with main protagonist to the overexpression of IL-6 and causing his varied symptoms and pathological changes [5]. It occasionally presents with manifestations similar to the tuberculosis, introducing yourself fever, sweating nocturnal, weight loss, related to symptoms B, in addition to symptoms systemic, failure liverwort, renal, alterations hematological, etc., which can occur in the tuberculosis systemic [6].
Presentation of the Case
Women of 25 years of age, coming from of Lime, of occupation supervisor of store, with background relatives of father and grandmother who had tuberculosis and received complete treatment, without harmful habits or allergies of importance.
He mentioned that two weeks before his admission he presented pain lumbar, nausea, vomiting and dehydration, reason for which he repeatedly went to the emergency service. She was admitted due to malaise, paleness, and drowsiness and was hospitalized for a complicated urinary tract infection. Six days later, she presented respiratory failure, anasarca, jaundice, anemia, and thrombocytopenia, for which she was referred to a hospital for more complex cases.
He was admitted with the diagnoses of multiorgan dysfunction syndrome due to respiratory failure, bicytopenia, and cholestatic hyperbilirubinemia; in addition, urinary tract infection, wasting syndrome, edema and fever. Imaging study revealed bilateral pleuroparenchymal involvement (Figures 1-3). Supportive measures, antibiotics against germs resistant to beta-lactamases were indicated, and imaging and laboratory tests were requested (pancultures, agglutinations, BK, quantiferon, ANA, ENA profile).
Three weeks later, due to poor evolution, she was transferred to the Intensive Care Unit with suspicion of septic shock. He returned to service after a week, persisting febrile despite having received broad-spectrum antibiotics, plus non-contributory auxiliary test results, which led to considering a case of fever of unknown origin (FOD). Liver biopsy, aspirate, and bone marrow biopsy studies were delayed due to thrombocytopenia and severe anemia. Two weeks later, two small cervical adenopathies were evidenced, which were taken for biopsy, finding lymph node inflammatory tissue (Figure 4). After a week, under more stable conditions, it was possible to take the lymph node samples, but with unsatisfactory results. Continuing with the FOD study plan, it was decided to perform positron emission tomography, finding multiple reactive adenopathies at the cervical, thoracic, abdominal, and inguinal level. Four weeks later, a cervical lymph node excision biopsy was performed, which revealed onion-shaped ganglion follicles plus vascular infiltration at the germinal center level, consistent with Castleman disease (Figures 5-6). Subsequently, antibodies to human herpes virus type 8 were negative, classifying idiopathic multicentric Castleman disease.
Four days later, being afebrile, stable, and due to the arrival of the second wave of the SARS CoV-2 pandemic, it was decided to discharge the patient with controls by an external office of the hematology service to continue with the study and treatment of the disease.
After discharge, the hematology service held a medical meeting regarding the possibility of chemotherapy, in which they decided to start it according to the patient's evolution. Despite this, the patient reports that she continued to have night sweats, tiredness, anemia, weakness, and a sensation of intermittent temperature rise. Twelve days after discharge, a report of a positive gastric aspirate culture for Mycobacterium tuberculosis was received, for which reason the diagnosis of idiopathic multicentric Castleman disease was flatly rejected because active tuberculosis infection was within the criteria. of exclusion, according to the 2016 International Consensus on Castleman Disease.
In conclusion, we determined that the final diagnosis of the case was multisystemic tuberculosis, which histologically presents similar characteristics with Castleman's disease. Anti-tuberculosis treatment was started for six months, presenting a favorable evolution with total resolution of symptoms and with normal control tests, thus avoiding the inappropriate use of chemotherapy.
Discussion
The case raises the search for a relationship between tuberculosis and Castleman's disease. Reviewing various literatures and clinical practice guidelines, we found that, within the criteria, other entities must be ruled out before determining multicentric Castleman disease, one of which can simulate this is active tuberculosis [7]. According to Berit Carrol, it is hypothesized that the cause of this peculiarity is due to the role of the SOCS-3 protein that binds to the JAK kinase and cytokine receptor, inhibiting SAT3 that regulates the expression of IL-6 and IL-
10 [8]. In the same way, part of the population has genetic defects of this protein, which makes it prone to poor control of chronic infections, such as Mycobacterium tuberculosis or Toxoplasma gondii, because they have an alteration of the gene that expresses this protein. protein which would lead to the activation and chronic inflammation caused by IL-6 overexpression with the subsequent presentation of clinical manifestations and anatomopathological changes -such as production of blood vessels, migration of lymphocytes-, which can simulate the hyaline vascular image and increase in lymphatic follicles similar to Castleman's disease [9]. We mention the case presented by the Japanese Hematology Society, in 2019, of a 65-year-old man who was hospitalized for suspected nephrotic syndrome due to hypoalbuminemia and edema, and who Performing an abdominal tomography revealed mediastinal lymphadenopathy, of which five lymph nodes were taken, one of them revealed granulomas with necrosis and the rest showed lymphatic follicles in onion skin with vessels penetrating the germinal center, compatible with Castleman's disease. Faced with these two entities, PCR was performed on all biopsies, finding Mycobacterium tuberculosis DNA positive even in those diagnosed with Castleman's disease [10].
It is because of these false positives that the 2017 Clinical Practice Guideline on Castleman Disease currently emphasizes the exclusion of this diagnosis in the presence of other diseases due to their great similarity, including histological, as is the case with tuberculosis.7 Finally, we recommend that in the case of low-prevalence diseases, it should be considered a priority to rule out tuberculosis before starting any treatment, avoiding unnecessary adverse effects.
Annexes
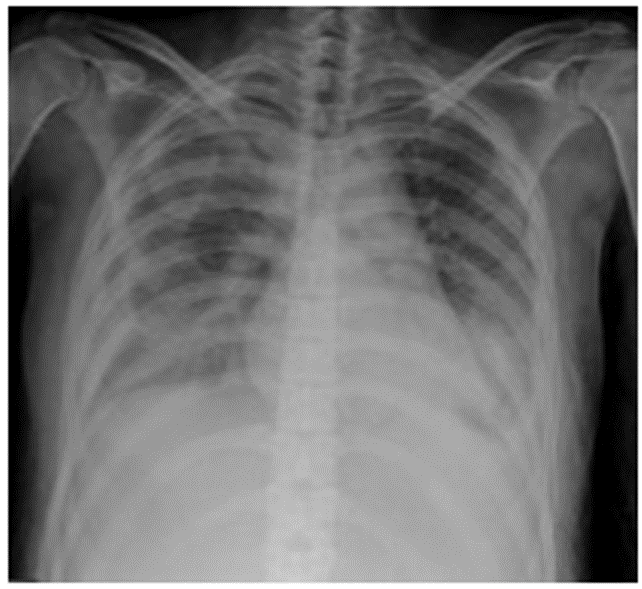
Figure 1
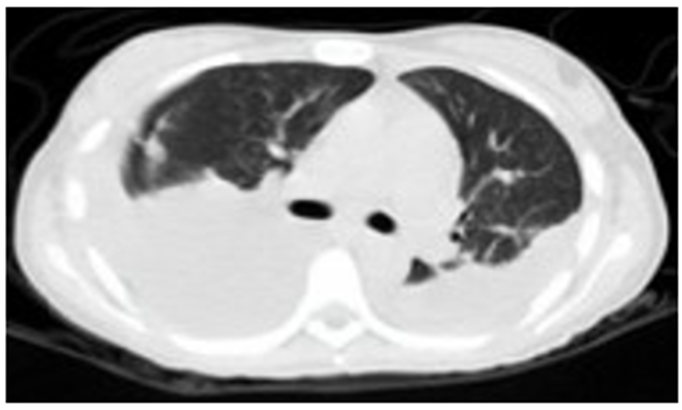
Figure 2
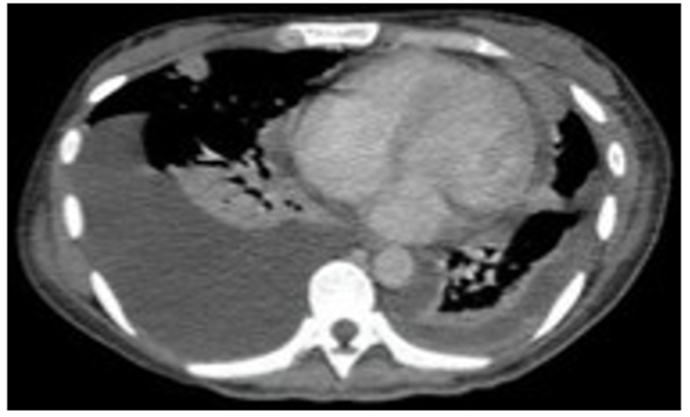
Figure 3
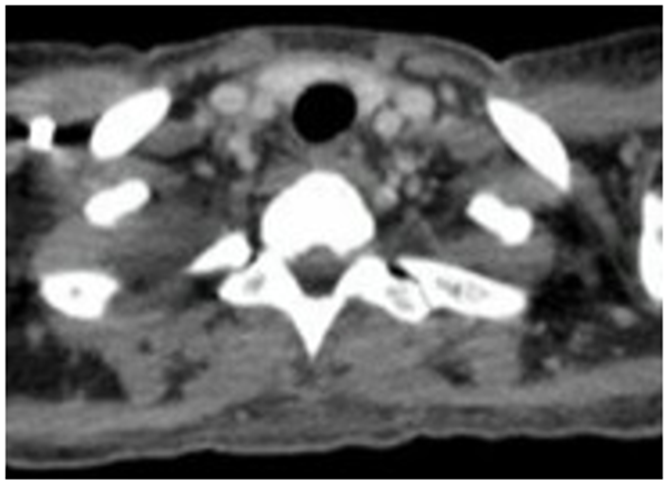
Figure 4

Figure 5
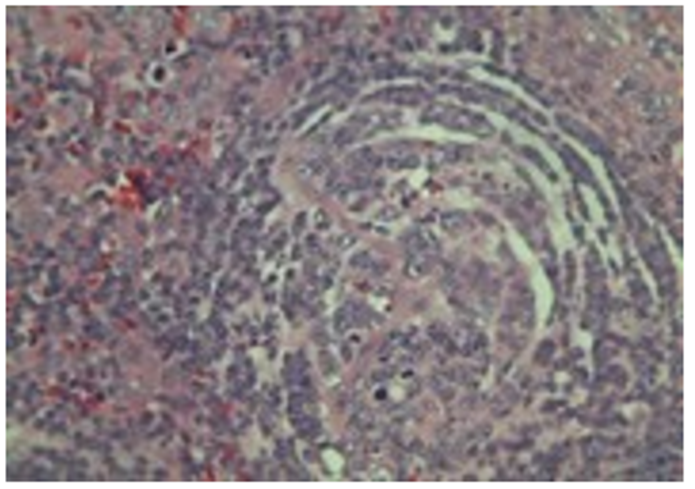
Figure 6
References
- Khan FMA, Kazmi Z, Hasan MM, dos Santos Costa AC, Ahmad S, et al. (2021), Resurgence of tuberculosis amid COVID-19 in Peru: Associated risk factors and recommendations. Int J Health Plann Manage;36(6):2441-2445. URL
View at Publisher | View at Google Scholar - Flores-Ibarra AA, Dolores Ochoa-Vázquez M, Alejandra G, Tec S. (2016), Diagnostic strategies applied in the Tuberculosis Clinic of the General Hospital Centro Médico Nacional la Raza. Rev Med Inst Mex Seguro Soc;54(1):122-127.
View at Publisher | View at Google Scholar - Fernandez GP. (2009), Head and neck tuberculosis. Acta Otolaryngol Esp;60(1):59-66.
View at Publisher | View at Google Scholar - Siltuximab (2016), (Sylvant ®) Therapeutic Positioning Report in multicentric Castleman's disease.1-6.
View at Publisher | View at Google Scholar - González García A, Moreno Cobo M, Patier de la Peña JL. (2016), Diagnosis and current treatment of Castleman's disease. Rev Clin Esp;216(3):146-156.
View at Publisher | View at Google Scholar - Fajgenbaum DC, Uldrick TS, Bagg A, Frank D, Wu D, et al. (2017), International, evidence-based consensus diagnose criteria for HHV-8-negative/ idiopathic multicentric Castleman disease. Blood;129(12):1646-1657.
View at Publisher | View at Google Scholar - Carow B, Rottenberg ME. (2014), SOCS3, a major regulator of infection and inflammation. Front Immunol;5(Feb):1-13.
View at Publisher | View at Google Scholar - Yoshizaki K, Murayama S, Ito H, Koga T. (2018), The Role of Interleukin-6 in Castleman Disease. Hematol Oncol Clin North Am.
View at Publisher | View at Google Scholar - Ide M, Yokoyama T, Ogino T. (2019), Tuberculous lymphadenitis mimicking Castleman disease-like histological features. Int J Hematol;109(3):245-246.
View at Publisher | View at Google Scholar
