

Case Report | DOI: https://doi.org/10.31579/2834-5118/031
Calcinosis Cut is Presenting as A Giant Cerebriform Growth Over the Scrotum
Dermatology, Senior Resident, Department of Dermatology, Lady Hardinge Medical College, Connaught place, New Delhi-110001
*Corresponding Author: Amit Kumar Meena, Dermatology, Senior Resident, Department of Dermatology, Lady Hardinge Medical College, Connaught place, New Delhi-110001
Citation: Amit Kumar Meena. (2023). Calcinosis cutis presenting as a giant cerebriform growth over the scrotum. International Journal of Clinical Surgery 2(4); DOI: 10.31579/2834-5118/031
Copyright: © 2023, Amit Kumar Meena. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 06 July 2023 | Accepted: 14 July 2023 | Published: 17 July 2023
Keywords: biomineralization; atherosclerosis; surgical approach
Abstract
Calcinosis cutis is defined as abnormal deposition of calcium in the skin and subcutaneous tissue. Depending on the cause it is classified into 4 types: metastatic, dystrophic, idiopathic and iatrogenic [1].
Introduction
Calcinosis cutis is defined as abnormal deposition of calcium in the skin and subcutaneous tissue. Depending on the cause it is classified into 4 types: metastatic, dystrophic, idiopathic and iatrogenic [1]. Idiopathic scrotal calcinosis cutis (ISCC) is a benign disease of the scrotal skin that presents with multiple nodules over the scrotum [2]. The lesions are mostly asymptomatic and have variation in size and numbers. Surgery is the mainstay of treatment. Various surgical methods include enucleation, wide local excision with direct closure, complex scrotal reconstruction and pinch-punch technique [3,4]. We report herein a case of calcinosis cutis presenting as a giant cerebriform growth over the scrotum.
Case report
A 50-year-old male patient presented with complaint of multiple asymptomatic nodular lesions over the scrotum for the last 1 year. Initially lesions were around the size of pea and gradually increased in size and number to the present size. Patient complaint of difficulty in walking and interference in sexual activity due to large size of the lesion. There was no history of discharge of chalky white material from the lesions. There was no history of scrotal trauma, prior surgery, autoimmune connective tissue disease, endocrinologic, metabolic, neoplastic or any other chronic illness.
General physical examination was within normal limits (WNL). On cutaneous examination, there were multiple yellowish white to brown colored nodules of size ranging from 1 x 1 cm to as large as 6 x 5 cm which were coalescing to form a mass of size 15 x 15 cm. This coalesced mass resembles sulci and gyri of brain and thus giving it a cerebriform appearance (Figure 1). These nodules encircled almost whole of the scrotum. Multiple atrophic scars of variable size were also present. On palpation, these nodules were non tender and firm to hard in consistency. Testis and epididymis were WNL. Rest of the cutaneous and systemic examination was WNL.

On the basis of history and examination, diagnosis of ISCC was kept. Serum calcium, phosphate and parathyroid hormone were within normal limits (WNL). Complete blood count, liver function test, kidney function tests and fasting blood glucose revealed no abnormalities.
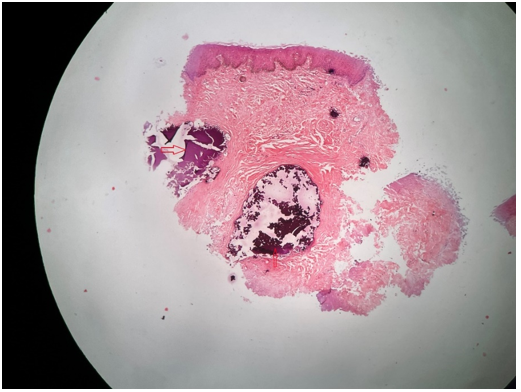
Histopathology from the nodule revealed normal epidermis with focal dermal collections of deeply basophilic material consistent with calcinosis cutis (Figure 2). On the basis of history, examination and investigations patient was diagnosed as ISCC. He was referred to surgery department for further management
Discussion
ISCC is a benign disease of unknown etiology. It commonly occurs between third to fourth decade of life [5]. It presents with multiple, calcified nodules without any systemic disorder of calcium phosphate metabolism. It is usually asymptomatic. However, patient may complain of itching, pain and
discharge of chalky white material from the lesions. The lesions are usually skin colored to white-yellow and vary from 1 mm to 2 cm in diameter. However, nodules were much larger in our patient. Pathogenesis still remains elusive and continues to be debated. Controversy still exist whether it is idiopathic or the result of dystrophic calcification of pre-existing lesions like epidermal cyst, eccrine duct milia and degenerated dartos muscle [6]. Differential diagnosis of nodular lesions over the scrotum includes lipoma, steatocystoma multiplex, fibroma, lymphagioma circumscriptum, cutaneous horn and angiokeratoma [7]. Definitive diagnosis requires histopathological examination which shows focal dermal collections of deeply basophilic material on hematoxylin and eosin stain and stains black with Von Kossa stain [8] Our case also shows histopathological features consistent with calcinosis cutis. Treatment is largely cosmetic. Surgical excision is the treatment of choice and provides a good clinical outcome. However, recurrence may occur after surgery due to left over microscopic foci of calcification. Concomitant use of local steroids and vitamin A after surgical excision may help in preventing recurrence [9]. Calcified masses are usually located in the dermis, therefore surgical resection should be limited to the scrotal wall [9]. A novel pinch-punch technique has been described by Chang et al [10]. for less extensive scrotal calcinosis. It is an easy and convenient method associated with minimal scarring [10].
Conclusions
ISCC is a benign condition, which mostly remains asymptomatic. However, larger lesions may cause difficulty in walking and interfere with sexual activity as seen in our patient. Such larger lesions may be a cause of unnecessary worry to patient. Interesting feature in our patient was rapid progression and cerebriform appearance of the lesions. To the best of our knowledge, such giant cerebriform presentation of ISCC have never been reported till date.
References
- Valenzuela A, Chung L. (2015). Calcinosis: pathophysiology and management. Curr Opin Rheumatol. 27(6):542-528.
View at Publisher | View at Google Scholar - Karaca M, Taylan G, Akan M, Eker G, s K, Gul ss. (2011). Idiopathic scrotal calcinosis: surgical treatment and histopathologic evaluation of etiology. Urology.76(6):1493-1495.
View at Publisher | View at Google Scholar - Khallouk A, Yazami OE, Mellas S, Tazi MF, El Fassi J, Farih MH. (2010). Idiopathic scrotal calcinosis: a non-elucidated pathogenesis and its surgical treatment. Rev Urol. 13(2):95-97.
View at Publisher | View at Google Scholar - Rout AN, Pradhan S, Sirka CS. (2021). Pinch-punch technique for scrotal calcinosis cutis. Indian J Dermatol Venereol Leprol. 87(6):858-460.
View at Publisher | View at Google Scholar - Saad AG, Zaatari GS. . (2001). Scrotal calcinosis: is it idiopathic? Urology. 2001;57(2):365.
View at Publisher | View at Google Scholar - Tela UM, Ibrahim MB. (2012). Scrotal calcinosis: a case report and review of pathogenesis and surgical management. Case Rep Urol.475246.
View at Publisher | View at Google Scholar - Gormally S, Dorman T, Powell FC. (1992). Calcinosis of the scrotum. Int J Dermatol. 31(2):75-79.
View at Publisher | View at Google Scholar - Yusuf SM, Uloko AE, Sani MU, Mijinyawa SM, Mohammed AZ. (2010). Idiopathic scrotal calcinosis; a rare scrotal tumour: a case report and review of literature. Niger J Med. 19(4):482-484.
View at Publisher | View at Google Scholar - Ruiz-Genao DP, Ríos-Buceta L, Herrero L, Fraga J, Aragüés M, García-Díez A. (2002). Massive scrotal calcinosis. Dermatol Surg. 28(8):745-747.
View at Publisher | View at Google Scholar - Chang CH, Yang CH, Hong HS. (2004). Surgical Pearl: Pinch-punch excisions for scrotal calcinosis. J Am Acad Dermatol. 50(5):780-781.
View at Publisher | View at Google Scholar
