

Review Article | DOI: https://doi.org/10.31579/2835-785X/045
Burden of Non-Communicable Diseases Risk Factors in Libya and other Arabic Countries: Step Wise Survey Comparative Analysis
1 Department of Community and Family Medicine, Faculty of Medicine, Sabratha Universit, Libya.
2 Pharmacology Department, Faculty of Medicine, Sabratha University, Libya.
3 Department of Physiology, Faculty of Medicine, Sabratha University, Libya.
*Corresponding Author: Azab Elsayed Azab, Department of Physiology, Faculty of Medicine, Sabratha University, Libya.
Citation: Mohamed A. Alsla, Rabia AM Yahya, Azab Elsayed Azab (2024 Burden of Non- Communicable Diseases Risk Factors in Libya and other Arabic Countries: Step Wise Survey Comparative Analysis, International Journal of Clinical Research and Reports. 3(2); DOI:10.31579/2835-785X/045
Copyright: © 2024, Azab Elsayed Azab. This is an open-access artic le distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 15 March 2024 | Accepted: 21 March 2024 | Published: 05 April 2024
Keywords: non-communicable diseases, NCDs risk factors, step wise survey comparative analysis, Libya, Arabic countries
Abstract
Background: Non- Communicable Diseases (NCDs), such as cardiovascular diseases, diabetes, cancer, and respiratory diseases, are a growing public health concern globally. The risk of NCDs is boost due to modifiable behaviours, such as tobacco use, physical inactivity, unhealthy diet and the harmful use of alcohol. Metabolic risk factors in the form of raised blood pressure, obesity, high blood glucose levels, and high levels of lipids in the blood all are connected with increased risk of NCDs. Objectives: The current study aims to investigate the burden of NCDs risk factors in Libya and compare it with other Arabic countries using a step survey comparative analysis. Methodology: The study population was drawn from WHO STEP wise approach to Surveillance which is an Observational, cross-sectional community-based survey conducted in Libya in 2023 as well as in different other nine Arabic countries. Multistage cluster sampling strategies were used in all countries included in this analysis. The survey used demographic and behavioural information questionnaires as well as physical and biochemical measurements among adults aged 18 years and above. Results: A total of 49000 individuals aged 18-69 years participated in the step wise survey in Libya as well as other 9 Arabic countries. The survey conducted over the last 12 years in different 10 countries included in the analysis. Oman has the largest sample (N= 9053) and Lebanon (N=1899) has the smallest sample. Over all prevalence of current smoking among Libyan was 21.5%. 19% of Libyan currently smoke tobacco daily. In all Arabic countries, men were much likely than women to smoke. Alcohol consumption was observed in 0.7% of Libyans. Lebanon males had the highest prevalence of alcohol abuse (14.7%) among males also Lebanon females had the highest prevalence among women (4.4%). Prevalence of inadequate fruit and vegetable intake among Libyans were about 93% which is relatively higher than any other Arabic country. The overall prevalence of insufficient physical activity among Libyans was 45%. Algerian men had the lowest prevalence of physical inactivity (13.7%) whereas Moroccan women had the lowest prevalence among women (26%). Libyans spent around 25.7 minutes on average per day in physical activity (51min males vs. 11 min females). .Morocco had the highest prevalence of the median time spent on physical activity on average per day (137minutes by Morocco men and 90 minutes by Morocco women). The overall prevalence of overweight (body Mass index BMI> 25) in Libyans was 56.8%. Libyan women were tend to be overweigh compared to Libyan men (62% in women Vs to 51.9% in men ). Kuwait had the highest prevalence of overweight 77.2% while Morocco had the lowest prevalence 53%. In regard to obesity (BMI >30) , 29% of Libyans were obese and Kuwait had the highest overall prevalence of obesity (40%). The overall prevalence of raised blood pressure (SBP>140 and or DBP >90 mmHg not on medication) was 25.3% among Libyans . A higher was observed among Libyan men (26.6%) than women (24%). Among countries included in the analysis, the highest prevalence was among Algerian men (80.8%) and Algerian as well as Egyptian women( 63.2%). Overall occurrence of raised fasting blood glucose was 14.9% among Libyans. the prevalence was slightly higher among women (15%). Qatar found to have the highest occurrence of raised blood glucose (16.7%) while Jordan found to have the lowest occurrence of raised blood glucose (8.2%). Raised total cholesterol was found in 14.6% of Libyans with slightly higher in women (16.2%) . among different countries included in the analysis, Lebanon had the highest overall prevalence (65.4%) .Moreover, Lebanon men and women had the highest prevalence. Conclusion: NCDs pose a significant threat to human health and economic stability in Libya and across the Arab world. The rising prevalence of these diseases, including cardiovascular disease, cancer, chronic respiratory illness, and diabetes, is largely driven by modifiable risk factors like tobacco use, unhealthy diets, and physical inactivity. Despite the alarming statistics, effective interventions already exist. Implementing these strategies, with a focus on salt reduction, stricter tobacco control, and health promotion initiatives, requires strong political commitment and a multi-sectoral approach. Strengthening healthcare systems and establishing robust monitoring programs are crucial for tracking progress and ensuring accountability. By prioritizing NCD prevention and control, Arab nations, including Libya, can improve their citizens health and well-being while reducing the economic burden associated with these chronic illnesses. Taking decisive action now will pave the way for a healthier future for generations to come.
Introduction
Non-infectious diseases, such as cardiovascular diseases, diabetes, cancer, and respiratory diseases, are a growing public health concern globally. Annually, these diseases are accounted for 42 million deaths and the numbers are projected to increase by 17% by 2025 [1]. The burden of these diseases is particularly high in low- and middle-income countries. The World Health Organization (WHO) estimated that there will be around 2.4 million deaths from Non- Communicable Diseases (NCDs) in Eastern Mediterranean Region which included Arabic countries [1, 2].
The risk of NCDs is boost due to modifiable behaviours, such as tobacco use, physical inactivity, unhealthy diet and the harmful use of alcohol. Annually, tobacco kills over 8 million, 1.8 million deaths due to excess salt/ sodium intake, and 830 000 deaths can be attributed to insufficient physical activity [2&3]. Metabolic risk factors in form of raised blood pressure, overweight/obesity; high blood glucose levels; and high levels of fat in the blood all are connected with increased risk of NCDs.
In terms of attributable deaths, the leading metabolic risk factor globally is elevated blood pressure (to which 19% of global deaths are attributed) followed by raised blood glucose and overweight and obesity. Several environmental risk factors contribute to NCDs. Air pollution is the largest of these, accounting for 6.7 million deaths globally, of which about 5.7 million are due to NCDs, including stroke, ischaemic heart disease, chronic obstructive pulmonary disease, and lung cancer [3].
In Libya, NCDs cause 186.11 deaths per 100000 population and they are accounted for the mainstream of loss of years of productive life and diminution of life expectancy [4].
Objectives
Step surveys are a widely used method for assessing the prevalence and risk factors of non-infectious diseases. However, there is limited research comparing step survey data between Arabic countries. The current study aims to fill this gap by conducting a comparative analysis of step survey data for non-infectious diseases between Libya and other Arabic countries.
Methods
Study design:
The study population was drawn WHO STEP wise approach to Surveillance (WHO STEPS, WHO 2005) which is a Observational, cross-sectional community-based survey conducted in Libya in 2023 as well as in different Arabic countries. Multistage cluster sampling strategies were used in all Arabic countries included in this comparison to conduct STEP wise survey. The population surveyed adults aged 18 years or older, men and women [5-7].
Data collection:
The WHO NCD STEPS instrument (Version 3.1) [5-7] consisted of three steps. Step 1 consisted of face-to-face interviews using an advanced standardized country-specific version of the STEPS questionnaire and locally-adapted show cards. These included socio-demographic characteristics, key behavioural risk factors, lifestyles, and history of chronic diseases. Due to the. The data collection was conducted by Arabic language . The tool was validated by a well-established method of translation from the original English version into Arabic by an expert panel and adapted to the local environment and needs, and tested in terms of wording and understanding, in order for the final version to be conceptually equivalent in both versions.
Step 2 consisted of physical measurements (weight, height, waist and hip circumference), and blood pressure to investigate biological risk factors such as raised blood pressure, and overweight and obesity. Weight was recorded using a portable digital weighing scale with light clothing on and without shoes, with a precision of 0.1 kg. Similarly, adult portable stadiometers were used to measure height (in centimetres up to 0.1 cm) after removing shoes, socks, slippers and any head gear. Blood pressure measurements were done thrice at three-minute intervals, and the mean of the second and third readings were taken according to the STEPS protocol. Calibrated measuring instruments were used throughout the survey for height (SECA1 213 portable stadiometer), weight (SECA1 813 digital floor scale), and blood pressure (Omron digital blood pressure device).
Step 3 consisted of biochemical markers levels (fasting capillary blood for glucose and lipid profile, and non-fasting urinary samples for sodium) to identify raised blood glucose, raised blood cholesterol, and sodium intake. Appointments were given on consent with the respondents for collection of biochemical markers. Trained nurses collected the blood samples using fingertip puncture which were analysed using a standard portable dry chemistry device. Calibrated and validated measuring instruments were used throughout the survey for blood parameters (CardioChek1 Plus analyser) as provided by WHO. Spot urine samples were collected from the participants who were asked to collect a sample in the evening before fasting, which was brought to the appointment for blood testing the next morning. Sodium levels in the urine samples were determined using an ion-selective electrode with Abbott Architect c8000 & Roche Cobas 6000 analysers [6&7]. Quality control measures were taken by each of the health centre laboratories’ analysers to ensure accurate results
Results
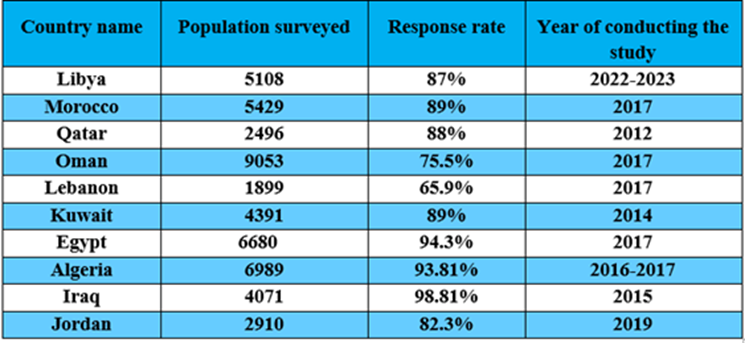
A total of 49000 individuals aged 18-69 years participated in the stepwise survey in Libya as well as other 9 Arabic countries. The survey conducted over the last 12 years in 10 different countries included in the analysis. Oman has the largest sample (N= 9053) and Lebanon (N=1899) has the smallest sample. Table 1 shows the population surveyed in each country, response rate, and year of conducting the study.
Table 1: The stepwise survey in 10 different countries included in the analysis.
1-Tobacco abuse:
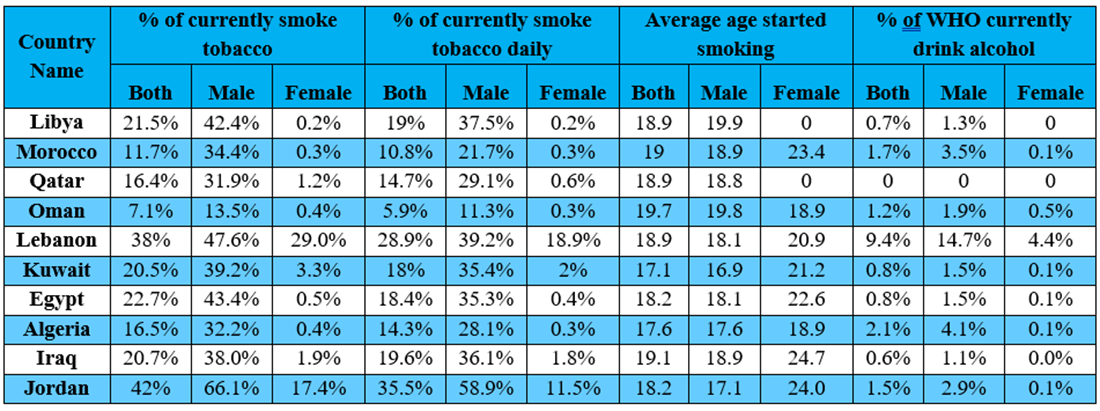
As shown in table 2, Over all prevalence of current smoking among Libyan was 21.5%. 19% of Libyan currently smoke tobacco daily. Comparing between Arabic countries, Men were much likely than women to smoke in all countries, the frequency of currently smoking ranged from 7.1 (Oman) to 42% (Jordan) the highest prevalence of current smoking daily was observed among Jordanian men (58.9%) while Lebanon women had the highest prevalence of currently smoke daily (7%) among women. the Kuwaiti boys had the lowest average age of start smoking (16.9 years).
2-Alcohol consumption:
Alcohol consumption was observed in 0.7% of Libyan. The overall prevalence ranged from 0.6 to 9.4%. Lebanon males had the highest prevalence of alcohol abuse (14.7%) among males also Lebanon females had the highest prevalence among women (4.4%) (Table 2)
Table 2: Shows the percentage of currently smoking tobacco, % of currently smoking tobacco daily, average age started smoking, and % of WHO currently drink alcohol in 10 different countries included in the analysis.
3-Unhealthy diet:
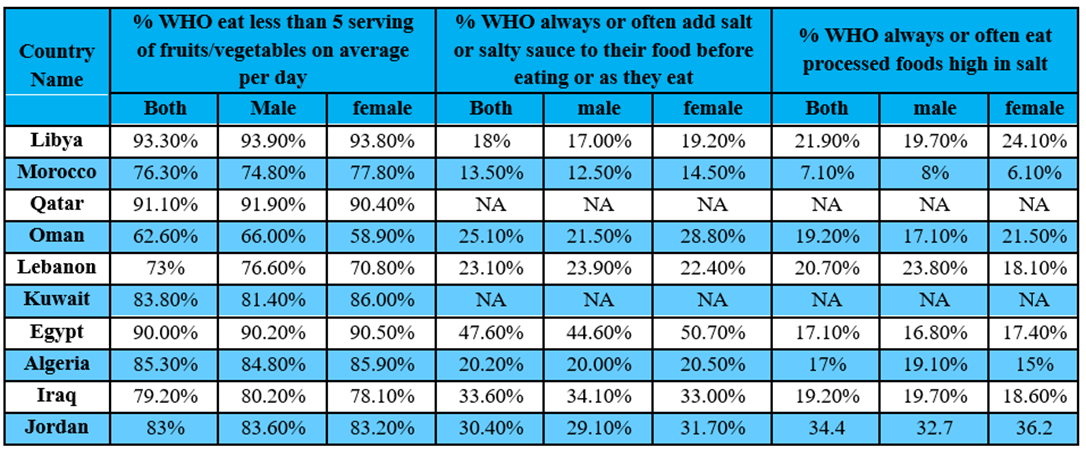
As shown in Table 3, Prevalence of inadequate fruit and vegetable intake (less than 5 serving of fruits and vegetables on average per day ) among Libyans were about 93% which is relatively higher than any other Arabic country included in this comparison; on the other hand, Oman had the lowest prevalence at 62.6%. Regarding, people who always or often add salt or salty sauce to their food, Egyptian women had the highest prevalence (50.70%) among women as well as Egyptian men had the highest prevalence among men (47.60%).
Table 3: Shows the percentage of WHO eat less than 5 serving of fruits/vegetables on average per day, % WHO always or often add salt or salty sauce to their food before eating or as they eat, and % WHO always or often eat processed foods high in salt in different 10 countries included in the analysis.
4-Physical Inactivity:
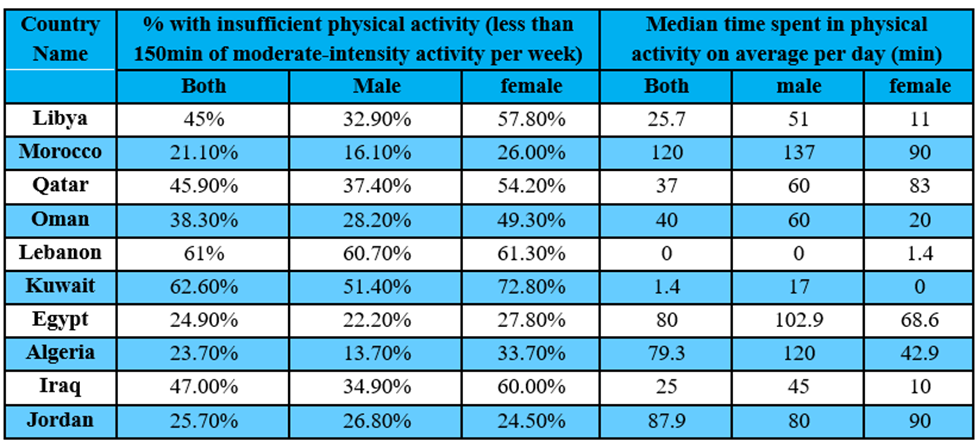
Physical inactivity is defined as (less than 150min of moderate-intensity activity per week), the overall prevalence of insufficient physical activity among Libyans was 45%. Algerian men had the lowest prevalence of physical inactivity (13.7%) whereas Moroccan women had the lowest prevalence among women (26%). (Table 4). Concerning the median time spent in physical activity on average per day, Libyans spent around 25.7 minutes on average per day in physical activity (51min males vs. 11 min females). Morocco had the highest prevalence of the median time spent on physical activity on average per day (137minutes by Morocco men and 90 minutes by Morocco women).
Table 4: Show the percentage with insufficient physical activity and median time spent in physical activity on average per day in different 10 countries included in the analysis.
Biological risk factors:
1-overweight and obesity:
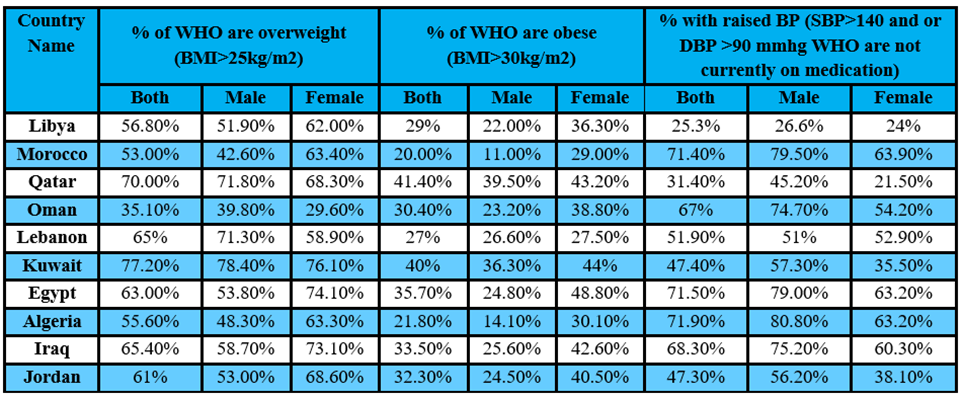
The overall prevalence of overweight (body Mass index BMI> 25) in Libyans was 56.8%. Libyan women were tending to be overweigh compared to Libyan men (62% in women Vs to 51.9% in men). About other Arabic countries, Kuwait had the highest prevalence of overweight 77.2% while Morocco had the lowest prevalence 53%. in regard to obesity (BMI >30), 29% of Libyans were obese a and Kuwait had the highest overall prevalence of obesity (40%). the most noticed difference is the much higher obesity prevalent among Egyptian women (48.8%) as well as Qatar men (41.4) (Table 5).
2-Raised blood pressure:
The overall prevalence of raised blood pressure (SBP>140 and or DBP >90 mmHg not on medication) was 25.3% among Libyans. A higher was observed among Libyan men (26.6%) than women (24%). Among countries included in the analysis, the highest prevalence was among Algerian men (80.8%) and Algerian as well as Egyptian women (63.2%) (Table 5).
Table 5: Show the percentage of WHO are overweight, % of WHO are obese, and % with raised BP in different 10 countries included in the analysis.
3-Rasied Blood glucose and raised total cholesterol:
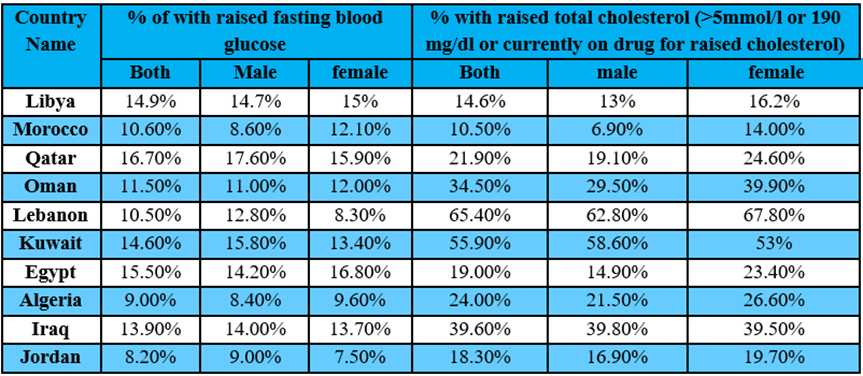
As shown in (Table 6), overall occurrence of raised fasting blood glucose was 14.9% among Libyans. the prevalence was slightly higher among women (15%). Qatar found to have the highest occurrence of raised blood glucose (16.7%) while Jordan found to have the lowest occurrence of raised blood glucose (8.2%). Raised total cholesterol was found in 14.6% of Libyans with slightly higher in women (16.2%). among different countries included in the analysis, Lebanon had the highest overall prevalence (65.4%) Moreover, Lebanon men and women had the highest prevalence (62.8% and 67.8% respectively).
Table 6: Show the percentage of with raised fasting blood glucose, and % with raised total cholesterol in 10 different countries included in the analysis.
Discussion
Non-Communicable Diseases are a major public health concern globally, with a significant burden on healthcare systems and economies. In the Arab region, including Libya, NCDs are a leading cause of morbidity and mortality. This study aims to investigate the burden of NCD risk factors in Libya and compare it with other Arabic countries using a step survey comparative analysis.
In this comparative analysis, smoking was found prevalent among men in all Arabic countries Libyans men ranked almost six (42.2%) whereas Jordanian men ranked number one with the highest prevalence (66.1%) and Omani men ranked number ten with lowest prevalence (13.4%).
Increased trend of smoking in Arabic countries is due to many factors urbanization is considered one of main factors. Also, cultural attitude toward smoking is differ among Arabic countries. Some countries like Lebanon consider smoking socially accepted while others like Oman Not. Some communities even encourage smoking in social settings such as cafes and gatherings. Furthermore, tobacco control policies also vary among Arabic countries. Some countries have implemented comprehensive tobacco control measures, such as bans on smoking in public places and advertising restrictions. For example, Oman has implemented strict anti-smoking laws since 2010 and has seen a decrease in smoking rates as a result [8]. In contrast, other countries have less stringent tobacco control policies and continue to struggle with high rates of smoking. For combating smoking, Libya as well as other countries needs to adopt policies recommended by WHO’s MPOWER package in order to reduce prevalence of tobacco consumption.
Alcohol consumption was among the least frequent risk factors in all Arabic countries. among Libyans only 0.7% report Alcohol use and Lebanon has the highest prevalence. results of alcohol consumption should be interpreted with some caution because there might be underestimation due to stigma associated with alcohol use in most Arabic countries.
Inadequate intake of fruit and vegetables per day was found very prevalent among all countries included in this comparison. Libya has the highest prevalence (93%) followed by Qatar (91%) while Oman has the lowest prevalence (62%). Despite the abundance of fresh produce in the region, many people do not consume enough fruits and vegetables on a daily basis. The 2002 joint FAO/WHO expert consultation on Diet, Nutrition, and prevention of NCD recommends a minimum of 400 g per day of fruits and vegetables. There are several factors that contribute to the prevalence of inadequate fruit and vegetable intake in Arabic countries. One of the main reasons is the traditional diet in many Arab countries, which tends to be high in carbohydrates, fats, and sugars, and low in fruits and vegetables. This dietary pattern is often influenced by cultural norms and preferences, as well as economic factors that make unhealthy processed foods more affordable and accessible than fresh produce. Furthermore, there may be a lack of awareness about the importance of consuming adequate amounts of fruits and vegetables for overall health. Many people may not realize the benefits of a diet rich in fruits and vegetables, such as reduced risk of chronic diseases like heart disease, diabetes, and certain types of cancer.
Inadequate physical activity which is defined as less than 150minutes of moderate or vigorous physical activity weekly was found very prevalent among Libyans as well as other countries. Libyans for example spent only 25 minutes on average weekly in physical activity. on the other hand, only Moroccans spent about 120mintues followed by Jordanians(87mintues). several factors contribute to such low rate of physical activity among Arab countries such as rapid urbanization has led to an increase in sedentary jobs and reliance on cars for transportation. Also, lack of awareness about the importance of regular physical activity plays a role.
in 2019, obesity was responsible for 160 million of Disability-adjusted life years (DALYs) and 5.02 million deaths. the global prevalence of obesity is nearly 13% and countries of EMR is ranked the third highest across the all-global regions. The current prevalence of obesity in Libya is estimated at29% while the prevalence of overweight is about 56.8%. Among countries in the comparison, Qatar revealed the highest rate of obesity (40%) and Kuwait revealed the highest rate of overweight around (77%). women in all Arabic counties were found to be obese and overweighed compared to men .in cross-sectional survey conducted by Lemamsha et al., in 2019, revealed that the prevalence of obesity, overweight, and normal weight among Libyan adults was 42.4%, 32.9%, and 24.7%, respectively. Women were more likely than men to be overweight or obese (the prevalence of overweight was 33.2% in women vs. 32.4% in men, and the prevalence of obesity was 47.4% in women versus 33.8% in men) [9,10]. In a study conducted in Libya that explored the key risk and protective factors beyond the high rate of obesity and overweight is due to changing dietary habits with a shift toward a more Westernized diet that is high in processed foods, sugar, and unhealthy fat. Additionally, sedentary lifestyles and lack of physical activity [9,10]. Finding of this comparison is consistent with study by Al-Jawaldeh and Abbass which indicated that obesity is first risk factor resulted in the total number of DALYs in 2019 in eight Arabic countries (Bahrain, Jordan, Kuwait, Libya, Oman, Qatar) and second reported risk factor in other centuries (Egypt, Iraq, Morocco) [11].
The prevalence of raised blood pressure or hypertension was reported in 25% of Libyans and Libya has the lowest prevalence while Morocco has the highest prevalence. Hypertension is a leading cause of heart failure, ischemic heart disease, peripheral vascular disease, renal failure, stroke, and dementia.
Hypertension was responsible for 235 million DALYs and 1.8million deaths in 2019. Among all the WHO regions, EMR including Arabic countries has the second – highest incidence of hypertension after Africa. Furthermore, raised blood pressure is the first reported risk factor resulted in DALYs in (Egypt, Iraq, and Morocoo) and second reported factor in other countries (Jordan, Libya, and Oman) [11].
High fasting blood glucose is reported in 14% of Libyans. the global prevalence of raised fasting blood glucose was about 9% in 2014.the fasting blood glucose was ranked as the sixth most common cause of DAYs in 2019. Prevalence of raised blood glucose in Libya is not differ from other EMR (around 14%). Libya as well as other upper –middle-income group tend to have higher level (Qatar followed by Kuwait then Egypt) [11].
High blood cholesterol is leading cause of ischemic heart disease as well as ischemic stroke. Among adults aged >25 years, the global prevalence of raised blood cholesterol (>5mmol/l) is 38.9% (37.3% for men and 40.2% for women). in 2018, the highest recorded raised blood cholesterol was in Lebanon followed by Kuwait, and Jordon which is consistent of findings of this analysis.
Conclusion
Non-communicable diseases (NCDs) pose a significant threat to human health and economic stability in Libya and across the Arab world. The rising prevalence of these diseases, including cardiovascular disease, cancer, chronic respiratory illness, and diabetes, is largely driven by modifiable risk factors like tobacco use, unhealthy diets, and physical inactivity. Despite the alarming statistics, effective interventions already exist. Implementing these strategies, with a focus on salt reduction, stricter tobacco control, and health promotion initiatives, requires strong political commitment and a multi-sectoral approach. Strengthening healthcare systems and establishing robust monitoring programs are crucial for tracking progress and ensuring accountability. By prioritizing NCD prevention and control, Arab nations, including Libya, can improve their citizens health and well-being while reducing the economic burden associated with these chronic illnesses. Taking decisive action now will pave the way for a healthier future for generations to come.
Strengths and limitations
One of the key strengths of this study is its comparative approach, which allows for a better understanding of the similarities and differences in NCD risk factors across different Arabic countries. The data were collected using a standard protocol to ensure the comparability of data, STEPS survey is the largest survey conducted in Libya as well as other Arabic countries which focused on collecting comprehensive information on both modifiable behavioural risk factors (smoking, alcohol consumption, physical inactivity, and unhealthy diet) and biological risk factors (overweight and obesity, raised blood pressure, raised blood glucose, and raised total cholesterol
An important limitation of this study is accuracy of data since they are collected at different countries, and also potential bias on self-reporting tobacco and alcohol use due to social customs, Islamic values, and stigmatization. Also, because this analysis depends on cross-sectional design, causal inferences will be of limited value.
References
- World Health Organization. Global Status Report on Non-communicable Diseases 2014 (2014).
View at Publisher | View at Google Scholar - World Health Organization. Non-communicable Diseases: Progress Monitor (2020).
View at Publisher | View at Google Scholar - World Health Organization. Global Health Observatory. Indicators. www.who.int. Available online at: https://www.who.int/data/gho/data/ indicators (accessed August 31, 2021).
View at Publisher | View at Google Scholar - World Health Organization. Non-communicable Diseases Country Profiles (2018).
View at Publisher | View at Google Scholar - NCDs | STEPwise approach to surveillance (STEPS). In: WHO [Internet]. [cited 3 Nov 2019]. http:// www.who.int/ncds/surveillance/steps/en/
View at Publisher | View at Google Scholar - World Health Organization. WHO STEPS Surveillance Manual. The WHO STEPwise approach to non-communicable disease risk factor surveillance. https://cdn.who.int/media/docs/default-source/ncds/ ncd-surveillance/steps/steps-manual_f0075411-1e6d-46ef-85be-fe826d2b9c47.pdf?sfvrsn= c281673d_5
View at Publisher | View at Google Scholar - World Health Organization. WHO STEPS Instrument. https://www.who.int/ncds/surveillance/steps/ instrument/STEPS_Instrument_V3.1.pdf
View at Publisher | View at Google Scholar - Al-Mawali A, Jayapal SK, Morsi M, Al-Shekaili W, Pinto AD, Al-Kharusi H, Al-Harrasi A, Al-Balushi Z, Idikula J. Prevalence of risk factors of non-communicable diseases in the Sultanate of Oman: STEPS survey 2017. PLoS One. 2021 Oct 28;16(10):e0259239. doi: 10.1371/journal.pone.0259239. PMID: 34710161; PMCID: PMC8553065.
View at Publisher | View at Google Scholar - Lemamsha H, Papadopoulos C, Randhawa G. Understanding the risk and protective factors associated with obesity amongst Libyan adults - a qualitative study. BMC Public Health. (2018) 18:493. doi: 10.1186/s12889-018-5411-z
View at Publisher | View at Google Scholar - Lemamsha H, Randhawa G, Papadopoulos C. Prevalence of overweight and obesity among Libyan men and women. Biomed Res Int. (2019) 2019:8531360. doi: 10.1155/2019/8531360
View at Publisher | View at Google Scholar - Al-Jawaldeh A, Abbass MMS. Unhealthy Dietary Habits and Obesity: The Major Risk Factors Beyond Non-Communicable Diseases in the Eastern Mediterranean Region. Front Nutr. 2022 Mar 16;9:817808. doi: 10.3389/fnut.2022.817808. PMID: 35369054; PMCID: PMC8970016.
View at Publisher | View at Google Scholar
