

Research Article | DOI: https://doi.org/10.31579/2834-796X/012
Blink and You’ll Miss It: A Rare Case of the Vascular Manifestations of Classic Hodgkin’s Lymphoma
1 Rochester Medical Center, Rochester, Michigan
2 Royal College of Surgeons in Ireland, Bahrain
3 Wayne State University School of Medicine, Detroit, Michigan
*Corresponding Author: Pierre Charbel Atallah, Rochester Medical Center, Rochester, Michigan.
Citation: Pierre Charbel Atallah, Grant Raymor, Parastou Rahimi, Mir Khan, Alessa Atallah (2023). Blink and You’ll Miss It: A Rare Case of the Vascular Manifestations of Classic Hodgkin’s Lymphoma. International Journal of Cardiovascular Medicine, 2(1) DOI:10.31579/2834-796X/012
Copyright: © 2023 Pierre Charbel Atallah, This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 16 December 2022 | Accepted: 29 December 2022 | Published: 03 January 2023
Keywords:
Abstract
Case Report
A 33 year old male with a past medical history significant for obstructive sleep apnea and hyperlipidemia presented with complaints of recurrent facial and neck swelling, syncope, and difficulty swallowing. He was previously referred to Ear Nose and Throat who performed a laryngoscopy that revealed chronic inflammation. He was diagnosed with larygo-pharyngeal reflux and prescribed oxymetazoline. His symptoms were persistent and worsened with physical exertion. He developed chest discomfort and a treadmill stress test was performed and negative. A chest x-ray revealed anterior mediastinal enlargement. Subsequently, he experienced a syncopal episode that occurred while seated. The patient lost consciousness for approximately thirty seconds. Emergency medical services were called. The patient’s vital signs, electrocardiogram, and blood glucose levels were normal.
At the time of evaluation he reported fatigue, shortness of breath, chills, palpitations, and right sided neck and facial swelling with exertion. On review of systems he reported fifteen pounds of unintentional weight loss in the previous six months. Physical examination revealed a blood pressure of 118/86, pulse of 111, respiratory rate of 14 and oxygen saturation of 96% on room air. His cardiovascular exam revealed a mid-systolic click. His right neck was swollen and tender to palpation. No appreciable facial swelling was noted. Blood work revealed an elevated sedimentation rate by modified Wester green of 46 mm/h; a mildly elevated white blood cell count of 11.8 thousand/uL; elevated platelet count of 520 thousand/uL; increased neutrophils of 8531 cells/UL; increased absolute monocytes of 1487; and a markedly elevated C- reactive protein of 231.3.
Stat computed tomography of the neck and chest were obtained to further define the anterior mediastinal enlargement noted on his prior chest x-ray and the neck swelling appreciated on physical examination. CT revealed an extensive heterogeneous non-enhancing mass in the anterior superior mediastinum obstructing multiple veins. Obstruction and thrombi were visualized in the right internal jugular vein (Figure 1), brachiocephalic vein, and the inferior vena cava extending into the superior vena cava with extensive collateral vessel formation (Figure 2). Non-obstructive thrombus was noted in the left internal jugular vein. Numerous small lymph nodes were present. An additional soft tissue mass was seen in the posterior mediastinum adjacent to the distal esophagus with mild diffuse enhancement. A trace pericardial effusion and right sided pleural effusion were also noted.

Figure 1: Computed tomography revealing thrombus and complete obstruction of the right internal jugular vein (white arrow). Non-obstructing thrombus is noted in the left jugular vein (blue arrow).

Figure 2: 3D volume rendered computed tomography image revealing extensive venous collateralization distal to the right internal jugular artery obstruction (white arrow).
The patient was sent to the emergency center for intravenous heparin therapy and further evaluation. In the hospital, a successful CT fluoroscopic guided percutaneous core mediastinal mass biopsy was performed.
Pathology was consistent with classic Hodgkin lymphoma (Figure 3). The patient was diagnosed with stage IIb unfavorable
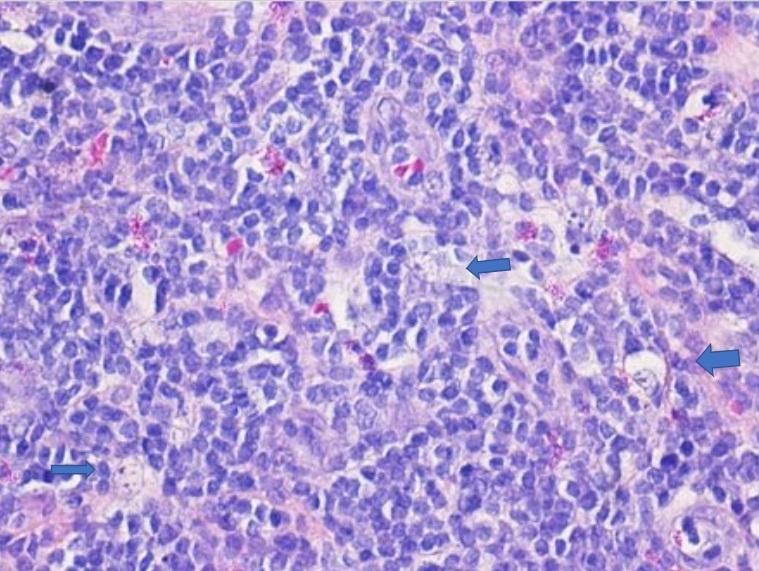
Figure 3: H&E (40x). High power view of the biopsy specimen shows numerous large, neoplastic cells with abundant cytoplasm, known as lacunar or Hodgkin cells (arrow) consistent with a diagnosis of Hodgkin lymphoma.
Classical Hodgkin lymphoma nodular sclerosis subtype (CD 30 positive, CD 15 partially positive, CD 20 negative with bulky disease and B symptoms). An EGD with endoscopic ultrasound was performed to biopsy the mass previously visualized at the level of the distal esophagus. This revealed inflammatory cells suspicious for Hodgkin lymphoma. The patient transitioned from IV heparin to Eliquis 5 mg bid po while in the hospital. A PICC line was placed and he successfully completed six cycles of ABVD chemotherapy. Eliquis was discontinued. A six month follow-up ultrasound of the bilateral internal jugular veins revealed chronic thrombus with extensive collateralization.
Venous thrombotic disease, although common in malignancy, is not often associated with Classic Hodgkin’s lymphoma. This patient’s presentation, with clinical manifestations of thrombotic superior vena cava syndrome, is very rare - with only several cases reported in the literature. A rapid and accurate diagnosis of superior vena cava syndrome is imperative to decrease morbidity and mortality. Approximately 15,000 cases of SVC syndrome occur each year in the United States. The incidence of SVC syndrome reported in the literature ranges from 1 in 650 to 1 in 3100 patients [1].
Superior vena cava syndrome is a condition caused by any compression or obstruction of the SVC, including direct invasion by a malignancy; external compression by tumors, as seen in this case; aortic aneurysm; or fibrosis. Thrombosis secondary to indwelling central venous catheters and pacemaker/ICD leads is also increasingly common [2].
The signs and symptoms of superior vena cava syndrome may have an insidious onset due to the formation of an extensive network of collateral vessels that redirect venous return distal to the site of venous obstruction. The most common presenting symptoms of SVC syndrome are face/neck swelling, distended neck veins, cough, dyspnea, orthopnea, upper extremity swelling, distended chest vein collaterals, and conjunctival suffusion [1].
The management of SVC syndrome is guided by clinical presentation. For patients with thrombus related to an indwelling intravascular device, device removal, anticoagulation therapy, and catheter-directed thrombolysis should be considered. Multidisciplinary treatment for obstruction due to malignancy is critical. Appropriate chemotherapy or radiation therapy, as indicated, can alleviate the symptoms of superior vena cava syndrome by reducing the amount of venous obstruction. In severe cases, open surgical repair may be indicated to overcome SVC obstruction, however, endovascular therapy is now the first-line treatment for SVC syndrome. Acute or subacute thrombus can be managed with catheter-based thrombolysis or thrombectomy prior to venoplasty and stent placement. [1] Despite the prevalence of superior vena cava syndrome due to thrombus, there are no clear guidelines for anticoagulation management and further research is needed to better understand the appropriate choice of anticoagulant and the duration of treatment.
References
- Seligson MT, Surowiec SM. Superior Vena Cava Syndrome. [Updated 2021 Jul 13]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2022 Jan. https://www.ncbi.nlm.nih.gov/books/NBK441981/
View at Publisher | View at Google Scholar - Ni R, Amr M, Kalla A. Hodgkin Lymphoma-Associated Superior Vena Cava Syndrome: A Case Report and Review of the Literature. Am J Case Rep. 2021;22:e929437. Published 2021 Apr 10.
View at Publisher | View at Google Scholar
