

Case Report | DOI: https://doi.org/10.31579/2835-7957/133
Balanitis a Public Health Challenge for Men
*Corresponding Author: Ali M, Department of Microbiology, Federal University Gusau.
Citation: Suresh Kishanrao, (2025), Balanitis a Public Health Challenge for Men, Clinical Reviews and Case Reports, 4(4); DOI:10.31579/2835-7957/133
Copyright: © 2025, Suresh Kishanrao. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 16 July 2025 | Accepted: 31 July 2025 | Published: 11 August 2025
Keywords: balanitis, balanoposthitis; circumcision; penile hygiene; sexually transmitted infection (sti); candida infection; penile cancer
Abstract
Balanitis is inflammation of the glans penis and is a common condition that affects an estimated 3-11% of males commonly in uncircumcised males. Balanoposthitis is inflammation of the mucosa of the glans and prepuce of the penis. Phimosis refers to the inability to retract the foreskin, while paraphimosis refers to foreskin trapped in the retracted position. Both these conditions are clinical diagnoses, they often occur secondary to Balanitis & Balanoposthitis & are considered are urologic emergencies warranting urgent surgical intervention. Balanitis in children and adolescents is mainly due to lack of personal or genital hygiene. Among sexually active adults Health care providers usually suspect a sexually transmitted infection (STI) as some STIs do cause balanitis. Balanitis is neither a STI nor it is contagious. The main symptoms of balanitis include inflammation and pain on the head of the penis. It might lead to complications of phimosis if not treated early. Patients with balanitis present with i) Penile discharge ii) Pain or difficulty with retraction of foreskin, iii) Erectile dysfunction, iv) Difficulty urinating /controlling urine stream v) Inability to insert a Foley catheter, vi) Tenderness and erythema of the glans penis, and vii) Itching. On Physical examination one can find i) Erythema and oedema of glans penis or foreskin ii) Foul odour iii) Discharge iv) Ulceration and/or plaque. In delayed care seeking individuals’, health care professional may also detect i) Phimosis ii) Meatal stenosis, iii) bladder distension, iv) ballooning of the foreskin when voiding v) Lymphadenopathy in rare cases. The aims of management are to minimize sexual and urinary dysfunctions, exclude penile cancer, treat premalignant disease, diagnose and treat sexually transmitted infections. The goal of the therapy is to reduce inflammation, prevent complications and eradicate infection. Topical antimicrobials (Clotrimazole & Bacitracin topicals), corticosteroids (Betamethasone topical), and immunosuppressants (Pimecrolimus) are used. Public health significance of Balanitis is due to its potential association with penile cancer, lichen sclerosis and scarring.
Materials & Methods: This article is based on three cases managed in the recent months in an adolescent, adult and elderly individuals, supported by literature review on epidemiology & management practices
Introduction
Balanitis is inflammation of the glans penis affecting approximately 3% of the global male population more common in uncircumcised males [1,2]. Most cases of balanitis are due to infection, despite coming across nonspecific (no aetiology) cases in clinical practice. While its burden is reported to be 12 to 20% of uncircumcised males and boys below the age of 4 in India, in the United States, it accounts for approximately 11 percent of males seen in urology clinics. Balanoposthitis is the inflammation of the mucosa of the glans and prepuce of the penis and is easily curable [2] It is classified as infectious, irritant, or traumatic. Balanoposthitis/Balanitis are the most common opportunistic human mycosis, especially in diabetic persons with unsatisfactory Glycaemic control, poor personal hygiene. Circumcision has a possible role in preventing /deferring development of balanoposthitis / balanitis. Phimosis refers to the inability to retract the foreskin, while paraphimosis refers to foreskin trapped in the retracted position [3]. Balanitis involving the foreskin and prepuce of the Penis is termed Balanoposthitis. Phimosis and paraphimosis are clinical diagnoses that that represent complications secondary to Balanitis or Balanoposthitis and are urologic emergencies warranting urgent surgical intervention [1,3]. Predisposing factors include poor hygiene or over washing, use of over-the-counter medications, and non-retraction of the foreskin [4] A complication of both these conditions among recurrent cases is constricting phimosis, or inability to retract the foreskin from the glans penis. Other complications include meatal stenosis, urethral strictures, urinary retention, and vesicoureteral reflux [5]. The aims of management are to minimize sexual and urinary dysfunctions, exclude penile cancer, treat premalignant disease, diagnose and treat sexually transmitted infections [6] Health care providers in India usually suspect a sexually transmitted Illness (STI) as the primary cause of Balanitis among adults, but it is neither sexually transmitted infection (STI), nor it is contagious, though certain STIs do cause balanitis, to make it look like an STI. Most commonly Yeast (Fungal) infections cause balanitis, though some bacterial infections, viral infections and skin conditions, also cause balanitis in people who lack genital hygiene [6,9]. Public health significance of Balanitis is due to its potential association with penile cancer, lichen sclerosis and scarring, and its possible link to underlying conditions like diabetes. This article is to attract attention of stake holders towards a public health strategy due to its potential association with penile cancer, lichen sclerosis and scarring. Based on three cases managed in the recent months in an adolescent, adult and elderly individuals, supported by literature review on epidemiology & management practices. While most of these cases fall under primary health care, national policies and approaches must include prevention of urological emergencies, minimize sexual and urinary dysfunctions, diagnose and treat sexually transmitted infections as early as possible, exclude penile cancer and treat pre-malignant disease.
Case Report 1:
Just last week a young school by of about 14 years walked into my consultation room with his father with the complaints of redness and pain and swelling under the foreskin in the tip of the Penis along with difficulty in urinating and a foul-smelling discharge. There was no history of recent trauma or sexual activity. His answer for any sexual activity was in negation even when his father was made to wait outside for secrecy. Physical examination revealed Poor hygiene, a tight foreskin (phimosis), and the accumulation of smegma was seen that could have led to irritation, infection, and inflammation. Both side lymphadenopathy was also noted. Though Balanitis common in those under the age of four I can affect children of all ages.
Case Report 2:
A 38 years old unmarried medium built male patient reported in the outpatient department of an Ayurvedic College, with chief complaints of redness, mild swelling and itching over the head of penis underneath the foreskin, whitish areas over penis, pain with irritation in the affected area, discharge with foul smell, sometimes off and on dryness over the affected parts with episodes of remission since last 4 years. Patient history did not reveal any evidence of use of latex condoms, sexual activity, history of fever or diabetes, or any urethral discharge but had mild swelling in the groin (Lymph node) region associated with mild pain. He gave history of buying over the counter medication for local application which gave relief, but the same problem used to reappear after few months. The sleep was sometimes disturbed but appetite, bowel habits and micturition were all normal. He showed recent blood investigations reports including STD & HIV/AIDS which were normal. On examination - PR - 78/min, Regular, BP - 110/70 mmHg, Temperature – Afebrile, Respiratory Rate – 16/min rhythmical. No systemic abnormalities were found. The Penis and scrotum examination revealed erythema, circular lesion, greyish-whitish scales over glans penis including area adjacent to glans, below the preputial skin and mild whitish discharge was observed, mild tenderness along with foul smell was also present. There was no evidence of any kind of urethral discharge or inguinal lymphadenopathy were observed during examination. Routine blood investigations except raised ESR, fasting blood sugar, HIV/AIDS test and PCR for herpes simplex virus were negative.
Sl . No | Name of the Medicine | Dosage | Schedule | Total Duration |
1 | Nimbadi churan | 1.5 gm | All the three drugs were mixed and given three times daily | 4 weeks along with Khadirarishat 15 ml + equal amount of water |
Chopchinyadi churan | 1.5 gm | |||
Gandhak rasayan | 250 mg | |||
2 | Saptabinshati guggul | 2 tablets(1gm) | Thrice in a day | 4 weeks with lukewarm water |
3 | Syrup Trifla rasayan | 10 ml | Twice a day | 4 weeks with equal water |
Table 3: Treatment Schedule
The symptomatologic changes were observed from day 7 and completely relieved by the end of 4 weeks with no recurrence.
Case 3: Primary syphilis without chancre & other STIs– A common cause of balanitis in 1970’s
A 42-year-old heterosexual male patient came to a Skin &VD Clinic of a Public Sector Hospital, in 2023 and complained of a painless, hard erythema nodule with a whitish scale in his coronal sulcus of the penis for about a week. In history revealed exposure to multiple sex partners in the past one year. Initial examination by a postgraduate student recorded an infiltrative, hard erythematous lesion surrounding the coronal sulcus of the patient’s penis, with mild erosion and a small amount of exudation. There was a whitish pseudo-membrane-like covering on the surface of the erythematous lesion in the coronal sulcus, mimicking a candidal balanitis. The result of the fungus microscopic examination was negative, while the laboratory findings showed positive results in serologic syphilitic testing -VDRL. The patient was diagnosed with primary syphilis and treated with a dose of benzylpenicillin of 2.4 million units intramuscularly. The skin lesions disappeared after 60 days of penicillin Injection.
Balanitis in 1970’s: Gonorrhoea, a sexually transmitted bacterial infection was common in 1970’s initial years of our professional career. It infects the urethra, and in some cases, caused Balanitis. Other STIs like chlamydia, genital herpes, and trichomoniasis also used to cause urethritis, leading to balanitis in 1970’s. Cases used to present with redness, swelling, pain, and discharge from the penis, especially under the foreskin if present and inguinal lymphadenopathy. Most often we diagnosed
clinically by examining the penis and VDRL test treated with long acting Benzathine Penicillin injection and advocated sex using condoms.
4. Penile Carcinoma Secondary to Balanitis:
A 65-year-old Rural Indian male presented in my clinic with a chief complaint of urinary retention, a recurring issue he had experienced over the past two years. He attributed the current episode to difficulty urinating after a day spent with a sex worker, prompting to seek this consultation. On initial examination, the patient appeared alert and comfortable, displaying no signs of acute distress. The genital examination revealed the presence of white, sclerotic plaques on the foreskin and glans penis. The patient's gave medical history of recurrent urethral strictures, meatal stenosis. Over the past decade, he had undergone multiple surgical interventions, and symptoms of urinary retention were temporarily alleviated until their recurrence two years ago. He also revealed receiving treatment for genital warts, like topical applications creams, & cryotherapy which were effective in eliminating the warts, with no recurrence. The patient reported a longstanding history of Balanitis Xerotica Obliterans (BXO), affecting the foreskin, and glans penis for over past 12 years and a mass on the head of his penis for two years prior to his current presentation. Suspecting a Penile cancer, I referred the case for a biopsy of the penile mass. The histological examination confirmed the presence of squamous cell carcinoma prompting surgical resection & chemotherapy in a public sector tertiary hospital.
Discussions:
Children under the age of 5 years and uncircumcised men with poor personal hygiene are most affected by balanitis. Lack of aeration and irritation because of smegma and discharge surrounding the glans penis causes inflammation and oedema. Though uncommon, complications of balanitis include phimosis cellulitis, Meatal stenosis with urinary retention though rarely accompany balanitis. In few cases, balanitis contributes to the "buried penis syndrome." Diabetes is the common underlying condition associated with adult balanitis. Older age has been identified as a risk factor for candidal balanitis & penile cancer. Balanitis xerotica obliterans (BXO) /Penile lichen sclerosis is a progressive sclerosing inflammatory dermatosis of the glans penis and foreskin.

The most common causes of Balanitis or balanoposthitis are poor hygiene, inflammatory skin diseases, infections, sexually transmitted infections, and trauma. Infections that cause balanoposthitis are -Chlamydia, Penile yeast infection, Fungal infections, Gonorrhoea, Chancroid, Primary or secondary syphilis, Herpes simplex, Trichomoniasis & Human papillomavirus. Non-infectious factors that can cause balanoposthitis to include- Chronic balanitis, Injuries or accidents, Tight foreskin, Arthritis, Eczema, Irritation due to rubbing or scratching, Chemical exposure and Diabetes.
Epidemiology:
Balanitis or Balanoposthitis most common inflammatory disease of penis, affects population of infectious aetiology, commonly seen in uncircumcised male patients, including newborns. Prevalence of ~35% is seen in uncircumcised male patients with diabetes mellitus. Zoon balanitis is seen in third decade onward in uncircumcised men. Phimosis occurs in uncircumcised men of any age. Phimosis most of is the result of recurrent balanoposthitis causing scarring of the preputial ring, resulting from an inflammatory reaction to accumulated smegma, the accumulation of desquamated epithelial cells, sweat and debris. Bacteria adhere and colonize the mucosal surface of the prepuce

Balanitis primarily affects uncircumcised males because the moist, warm area under the foreskin is the ideal place for yeast and bacteria to grow. It can occur at any age and is more common in people who have tight foreskin that doesn’t easily move over the head of their penis known as phimosis. High risk factors include: i) Individual who don’t clean their penis or under their foreskin frequently ii) middle-aged or older men iii) Diabetics, because the increased glucose on their skin facilitates bacterial and fungal growth iv) Obese people v) Have sexually transmitted infections and vii) Have a sensitivity to chemical irritants. The complications of balanitis are phimosis & cellulitis, meatal stenosis with urinary retention [1,8,9]
Basically, two types of Balanitis are described in the literature:
1) Infectious type -most common, due to an infection (fungal, bacterial, viral, parasitic)
2) non-infectious types- a) Zoon’s balanitis: This chronic type accounts for up to 10% and affects uncircumcised, middle-aged and older men, causing an inflamed, discoloured penis head presenting as a well-demarcated shiny erythematous patch or plaque over the genital mucosa. b) Circinate balanitis: This type of balanitis is a result of reactive arthritis that develops in response to an infection in our body. In addition to inflammation and discoloration, circinate balanitis causes small lesions (sores) on the head of your penis c) Pseudoepitheliomatous keratotic & micaceous balanitis (PKMB): This very rare form of balanitis causes scaly warts or bumps on the head of the penis. It affects people over 60 d) Fixed drug eruption: is a skin lesion appears on areas of our skin because of certain medications or chemicals e) Lichen planus: is a skin condition that causes a rash to develop on one or more parts of our body [1.7,9]. Some types of balanitis are precancerous or cancerous conditions, such as i) Basal cell carcinoma- It’s the most common type of skin cancer that forms in the basal cells of the outer layer of our skin, causing lumps or bumps to form ii) Squamous cell carcinoma: A type of skin cancer that forms in the squamous cells in the outer layer of your skin, presenting as bumps, marks or lesions iii) Kaposi sarcoma: is the rare type of cancer affecting people with weakened immune systems iv) Extramammary Paget’s disease (EMPD): Another rare condition causes discoloured, scaly, itchy skin around our genitals [10].
Diabetes mellitus is the most common underlying condition associated with balanitis in adults. In a study of patients with type 2 diabetes mellitus, treatment with dapagliflozin (a selective sodium-glucose transporter–2 [SGLT2] inhibitor that increases urinary glucose excretion) was found to be associated with an increased risk of vulvovaginitis or balanitis [3]. Other causes in teenagers and adults include i) Poor personal hygiene ii) Chemical irritants (soap, petroleum jelly) iii) Oedematous conditions, such as Rt. sided congestive heart failure, cirrhosis, and nephrosis, iv) Drug allergies (tetracycline, sulphonamide), v) Morbid obesity.
Causes: Common Pathogens that cause balanitis include- Candidal species, Group B and group A beta-haemolytic streptococci, Neisseria gonorrhoeae, Chlamydia species, Anaerobes (eg, Bacteroides), Human papillomavirus, Gardnerella vaginalis, Treponema pallidum (syphilis), Trichomonas species, Borrelia Vincentii and burgdorferi
Clinical Presentation & Findings: Patients with balanitis present with i) Penile discharge ii) Pain or difficulty with retraction of foreskin, iii) Erectile dysfunction, iv) Difficulty urinating /controlling urine stream v) Inability to insert a Foley catheter, vi) Tenderness and erythema of the glans penis, and vii) Itching
On Physical examination one can find i) Erythema and oedema of glans penis or foreskin ii) Foul odour iii) Discharge iv) Ulceration and/or plaque. Rarely the health care professional finds: i) Phimosis ii) Meatal stenosis, iii) bladder distension, iv) ballooning of the foreskin when voiding v) Lymphadenopathy.
Pathophysiology of Balanitis & Balanoposthitis:
Normally the foreskin of the Penis can be pulled back behind in about 50% of 1year old boys and almost 90% by the age of 3 years. After the age of 7 years, it is possible to pull the foreskin back over the glans (head) of the penis. In some boys it may not be possible until 14-15 years as was in our first case and is perfectly no reason of concern. Phimosis- an inability to retract the foreskin occurs up to the age of 10 years and the chances of phimosis reduce to less than 1% of teenagers of 16-18 year.
Desegregated Aetiology:
Balanoposthitis: Most commonly occurs in uncircumcised men, especially with diabetes, poor hygiene, due to buildup of smegma, tight foreskin. Skin conditions like contact dermatitis, Inflammatory dermatoses and Infections may also lead to this condition [4,5]. Candida balanitis accounts for 30 - 35% of infectious cases, Extensive survey of more than 60000 outpatients across India’s dermatologists revealed that up to 75% of individuals with Candida balanoposthitis were known cases of diabetes mellitus [8].
Aerobic bacteria: Staphylococcus aureus and group A Streptococcus, Gardnerella, uncommonly Anaerobic bacteria, Viruses, Parasites- Trichomonas, infections also contribute to Balanitis/ Balanoposthitis:
Zoon balanitis: Occurs due to Lack of circumcision, Poor hygiene, warmth, rubbing
Phimosis: It is either congenital or acquired. Congenital Phimosis is due to anomalous development, small preputial orifice, or abnormally long foreskin. Acquired Phimosis is mostly due to recurrent infections- balanitis / Balanoposthitis.
Paraphimosis: Often iatrogenic, after examination or instrumentation. It could be caused by malaria (Plasmodium falciparum) or metastatic carcinoma.
Cause specific clinical findings:
- Candidal balanitis may present as a white curd-like exudate and penile discharge. It is most common in patients with diabetes.
- Balanitis xerotica obliterans (penile lichen sclerosis) is a chronic dermatosis identified by whitish plaques involving the glans and foreskin [6,7].
- Zoon balanitis is a reddish velvety lesion on the glans, found in older, uncircumcised males. It can be asymptomatic or pruritic or cause dysuria [5, 9].
- Reactive arthritis consists of circinate and eroding lesions on the glans.
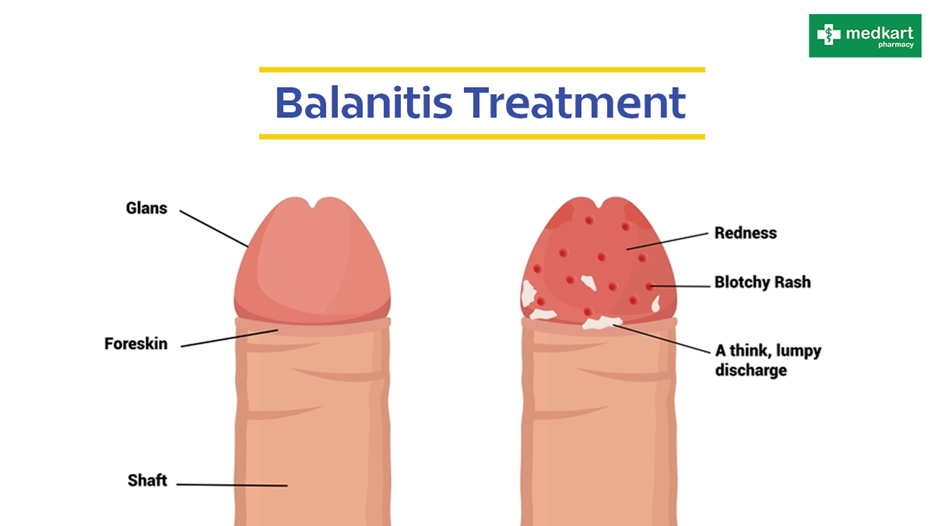
Normal Penis Balanitis Penis
Laboratory Investigation: Laboratory investigations are not usually necessary but may consider based on clinical suspicion. I) Serum glucose test ii) Culture of discharge iii) Syphilis serology test (VDRL), iv) Wet mount, v) Potassium hydroxide (for Candida), vi) HIV and human papillomavirus titres in selected cases and vii) Ultrasonography or bladder scan is used to detect urinary obstruction in severe balanitis.
Management:
The goal of balanitis treatment is to eradicate infection, reduce inflammation, and prevent complications. Topical antimicrobials (Clotrimazole & Bacitracin topicals), corticosteroids (Betamethasone topical), and immunosuppressants (Pimecrolimus) are used [3].
- Gentle retraction of the foreskin daily & soaking in warm water to clean penis & foreskin.
- In paediatric patients and patients with mild balanitis xerotica, a 2-month trial of topical corticosteroid therapy is recommended. The patient or mother must retract the foreskin gently and apply (0.05?tamethasone) twice a day. Good (65-95%) results are seen in boys older than 10 years compared with those aged 3-10 years.
- Topical steroids have had only limited success in patients with moderate-to-severe balanitis xerotica obliterans, due to distal scarring of the foreskin.
- In recurrent cases, 1% pimecrolimus cream instead of steroids, gives around a 65% success rate.
- In paediatric patients with suspected bacterial infection, applying bacitracin gives good result. For adults topical clotrimazole with probable candidal balanitis works better.
- Patients presenting to the ED with phimosis and severe urinary obstruction must get first Steroid cream and gentle retraction of the foreskin, if the phimosis is not too tight, is tried, If it fails surgical intervention is the option. The steps of circumcision involve:
- Without damaging the glans penis, dilate the foreskin using a clamp, under Local anaesthesia, analgesia, and/or sedation b) Then perform a dorsal slit incision by cutting the foreskin over the dorsal shaft of the penis to enlarge the foreskin opening under local anaesthesia and sedation c) Perform a formal circumcision, for nonspecific balanoposthitis
Cause specific Treatments:
- For Candidal balanitis -clotrimazole cream 1%; miconazole cream, 2%; apply twice daily until symptoms resolve.
- For Anaerobic infection metronidazole 400-500 mg twice daily for 1 week.
- For Aerobic infection: Trimovate cream applied once daily; erythromycin 500 mg four time a day for 1 week; or co-amoxiclav 375 mg 3 times daily for 1 week.
- Lichen sclerosis: ultrapotent topical steroids such as clobetasol propionate applied once daily until remission, then gradually reduced.
- Lichen planus: moderate to ultrapotent topical steroids depending on severity.
- Zoon balanitis: Needs circumcision followed by topical steroids with or without antibacterials 1 or 2 weekly.
- For Psoriasis topical steroids with or without antibiotic and antifungal are good
- Eczema: hydrocortisone 1% applied once or twice daily until resolution of symptoms.
- Seborrheic dermatitis- antifungal cream with a mild to moderate steroid.
- Bowenoid papulosis: imiquimod 5% cream; laser resection.
- Premalignant conditions: surgical excision.
Complications:
- A 2017 meta-analysis inferred that a higher risk (3.8-fold) of penile cancer is there in individuals with a history of balanitis [3].
- Balanitis can be the first sign of underlying diabetes,
- Need for frequent urinary catheterization,
- May also lead to obesity,
Early diagnosis and treatment of balanitis are crucial to prevent complications.
Conclusion:
Balanitis and balanoposthitis, inflammation of the glans and foreskin respectively, are common in uncircumcised men and can lead to complications like phimosis, paraphimosis, and potentially penile cancer, highlighting the importance of public health initiatives for prevention and early detection. Balanitis and balanoposthitis can cause pain, itching, and discomfort, impacting sexual function and overall well-being.
Maintaining good hygiene, especially in uncircumcised males, is crucial for preventing balanitis and balanoposthitis. Prompt diagnosis & treatment can prevent complications and improve outcomes. Circumcision significantly reduces the risk of balanitis & balanoposthitis.
Public health campaigns can raise awareness about the importance of hygiene, early detection, and make available the treatment at primary health care level.
References
- Inflammatory Balanitis / phimosis https://www.pathologyoutlines.com/11/14/2024
View at Publisher | View at Google Scholar - Balanoposthitis easily curable, https://www.maxhealthcare.in/
View at Publisher | View at Google Scholar - Balanoposthitis/balanitis association in case of uncontrolled T2DM attending tertiary care hospital in Bihar, India, Gautam Sanjay Kumar et.al, International Journal of Academic Medicine & Pharmacy (www.academicmed.org), ISSN (O): 2687-5365.
View at Publisher | View at Google Scholar - Balanitis- Overview, Mark J Leber, https://emedicine.medscape.com/ID 777026/ Feb 12, 2025
View at Publisher | View at Google Scholar - Balanitis - Update of Clinical Spectrum and Management. Relhan V, et, al, Zoon's Indian J Dermatol. 2024 Jan-Feb. 69 (1):63-73.
View at Publisher | View at Google Scholar - 10 Years' Experience in Balanitis Xerotica Obliterans: A Single-Institution Study. Pradhan A, et.al. Eur J Pediatr Surg. 2018 Aug 21.
View at Publisher | View at Google Scholar - Balanitis xerotica obliterans: has its diagnostic accuracy improved with time? Boksh K, et.al, JRSM Open. 2017 Jun. 8 (6):2054270417692731.
View at Publisher | View at Google Scholar - Diabetes and balanoposthitis. Kalra S, et.al. (2016). J Pak Med Assoc. 66 (8):1039-1041.
View at Publisher | View at Google Scholar - Zoon balanitis: A comprehensive review. Dayal S, et.al, Indian J Sex Transm Dis. 2016 Jul-Dec.37 (2)
View at Publisher | View at Google Scholar - Penile Carcinoma Secondary to Balanitis Xerotica Obliterans, Ali Z Ansari et.al, https/ www/Cureus. 2024 May 2;16(5): e59555. Doi: 10.7759/cureus.59555
View at Publisher | View at Google Scholar
