

Case Report | DOI: https://doi.org/10.31579/2835-8465/006
Atypical Presentation of Forearm Compartment Syndrome in a Case of Vascular Type Ehlers-Danlos Syndrome
- Tsang Yeung *
- Esther Ching San Chow
Department of Orthopaedics and Traumatology, United Christian Hospital, Hong Kong.
*Corresponding Author: Tsang YEUNG, Department of Orthopaedics and Traumatology, United Christian Hospital, Hong Kong.
Citation: Tsang Yeung and Esther C. S. Chow, (2023), Atypical Presentation of Forearm Compartment Syndrome in a Case of Vascular Type Ehlers-Danlos Syndrome. Orthopaedics Case Reports, 2(3); DOI:10.31579/2835-8465/006
Copyright: © 2023, Tsang Yeung, This is an open-access artic le distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 09 May 2023 | Accepted: 25 May 2023 | Published: 14 June 2023
Keywords: compartment syndrome; ehlers-danlos syndrome; Hong Kong; Chinese; pseudoaneurysm; saphenous vein graft
Abstract
We describe a 30-year-old Chinese gentleman with vascular type Ehlers-Danlos Syndrome (“vEDS”) presents with spontaneous right forearm compartment syndrome due to pseudoaneurysms along the radial artery. There was no history of injury. Urgent CT Angiogram showed multiple pseudoaneurysms along radial and ulnar arteries. Emergency fasciotomy and reconstruction of radial artery with saphenous vein graft was performed. After subsequent skin grafting, his right forearm wound healed well eventually and his right upper limb function was preserved.
Pathological examination of the diseased radial artery showed variable smooth muscle thickness, partial loss of muscle wall, aneurysmal dilatation, fibrinoid necrosis and inflammation. Genetic test showed a heterozygous missense variant c. 1852G>C in COL3A1 gene, which has not been reported and is likely pathogenic of vascular type of Ehlers-Danlos Syndrome.
There was no complication or rupture of reconstructed radial artery up to 4 four years’ follow-up. We believe that autologous saphenous vein grafting is a safe, durable option to reconstruct a long segment of arterial defect in this group of patients.
Introduction
Compartment syndrome of limbs is an orthopaedic emergency, which is usually caused by trauma. Spontaneous presentation of compartment syndrome without any injury or pre-existing coagulopathy is extremely rare. Proper management of compartment syndrome includes timely diagnosis and urgent fasciotomy to decompress the muscle compartments to prevent muscle necrosis and the need for amputation [1].
We would like to present a case of spontaneous forearm pseudoaneurysm presented as compartment syndrome in a young Chinese gentleman with vascular type Ehlers-Danlos Syndrome (“vEDS”), which is a rare connective tissue disorder characterised by rupturing of fragile vessels and internal organs. There are published case reports of spontaneous compartment syndromes over different parts of body in patients with vEDS. But to our knowledge, such presentation of vEDS has not been reported in Chinese Population.
Case Report
A 30-year-old gentleman labelled as Ehlers-Danlos Syndrome (“EDS”) due to positive family history, with past history of epilepsy, admitted to our unit in year 2017 with bilateral forearm redness and swelling for 2 days, with right side being more severe. There was no recent history of epileptic convulsion, insect bite or trauma. The patient did not complain of any paraesthesia of both upper limbs.
On admission, he had normal blood pressure and was afebrile. His bilateral forearms were mildly erythematous with bruising, mildly tender and with increase in temperature. His bilateral wrists movement was normal. White blood cell count was 17.2 x 109/L and C-reactive Protein (CRP) was 190.1 mg/L. He was therefore treated as cellulitis initially with antibiotics.
During patient’s stay, progressive right forearm swelling was noted. Repeated physical examination found tense forearm compartments, and there was also limited right wrist and fingers movement; the radial pulse was weakened. Left forearm compartments were not tense. There was no numbness over bilateral upper limbs. (Figure 1)

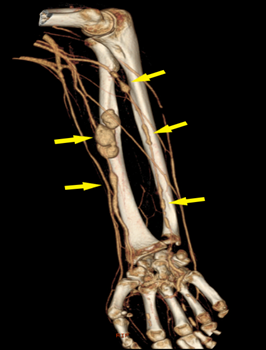
Compartment pressure was measured and found to be up to 62mmHg. An urgent CT angiogram of the right forearm showed multiple pseudoaneurysms along radial and ulnar arteries. (Figure 2)
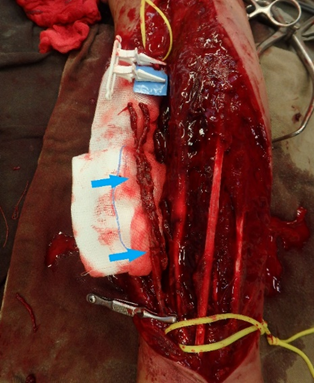
Urgent forearm fasciotomy was performed. Intraoperatively, a 15cm segment of the radial artery was found to be thinned-wall and friable, with multiple sites of rupture. (Figure 3) The pathological segment was excised and reconstructed with a saphenous vein graft. (Figure 4 & 5) Circulation of the right upper limb was restored. The fasciotomy wounds were covered with full thickness skin graft 6 days after the index operation. (Figure 6)


Microscopic examination by pathologist found that the radial artery was with variable smooth muscle thickness, partial loss of muscle wall, aneurysmal dilatation, fibrinoid necrosis and pseudoaneurysm surrounded by moderately dense mixed inflammatory infiltrate and fibroblastic reaction. There was absence of internal elastic lamina and loss of muscle wall at the aneurysmal sites. There was also variable decrease in elastic fibers and smooth muscle cells in the tunica media. Similarly, the adjacent small to medium sized veins had focal deficient or fragmented elastic fibers noted in the tunica media.
Genomic investigation has been carried out and it confirmed that the patient has a heterozygous variant in the COL3A1 gene which is a missense variant c. 1852G>C in exon 26.
It has been 4 years after the operation. Upon follow-up, the wound healed well and patient has good right-hand function and he can write nicely with his right hand. To our knowledge, there was no complications or rupture of the reconstructed radial artery. (Figure 7)

The patient has consented to the publication of this manuscript.
Discussion
Ehlers-Danlos syndrome (“EDS”) is a group of hereditary connective tissue disorders, caused by various defects in the synthesis of collagen. Its overall prevalence lies between 1 in 10,000 to 25,000 in general population [2]. EDS has different subtypes. Type IV or the vascular type Ehlers-Danlos Syndrome (“vEDS”), described by Andras Barbaras in 1967 [3], consists of 5 to 10% of EDS [2]. It is due to pathogenic variants in COL3A1 gene and it is inherited in an autosomal dominant manner [2]. Due to defects in type III collagen, body tissues and organs of patients with vEDS are fragile. Signs of vEDS include: Characteristic facial appearance (thin vermilion of lips, small chin, thin nose, large eyes), acrogeria (skin on the hands and feet appears prematurely aged) and thin translucent skin [4]. In majority of patient, the diagnosis was only made when there is at least one major complication happened, which is defined as arterial rupture, dissection or organ rupture, like sigmoid colon perforation and perforated gravid uterus The risk of having complication at age of 20 is 25% and rises to more than 80% by age of 40. The average age at the time of the first major complication was 23.5 years old. Median life expectancy of patient with vEDS is 48 years [5].
Prior to this case report, compartment syndrome as a complication of vEDS has also been reported in literatures from different countries. The first case was reported in 1992 with spontaneous bleeding from a gluteal artery resulting in a gluteal compartment syndrome and sciatic neuropathy [6]. There were also cases of abdominal compartment syndrome, compartment syndromes over legs, upper arm and forearm, due to rupture of peroneal artery, posterior tibial artery and ulnar artery. Cases of compartment syndrome in vEDS patients reported in literature are listed in (Table 1)
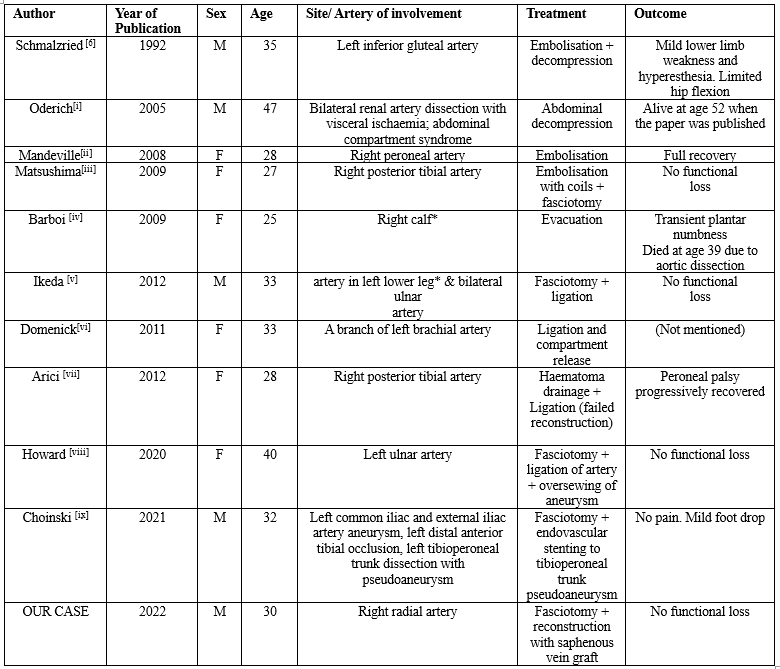
* Cases reported as past medical history, not the index condition presented
The challenge in these cases of compartment syndrome in vEDS patient is that surgeons also need to tackle the pseudoaneurysms and maintaining adequate blood flow to the limbs apart from performing facsiotomy. Moreover, care has to be taken to avoid profuse bleeding from the fragile or ruptured major vessels. Surgical options of treating pseudoaneurysm were described in those case reports, such as endovascular coil embolization [6,8,9], oversewing of the ends of ruptured pseudoaneurysm with pledgeted suture [14], stenting [15], or ligation of the artery [11-14] if another patent artery suppling the involved limb is present. Yet, endovascular intervention is not free of risk. Rupture and pseudoaneurysm formation at access site [16] and arterial complication secondary to placement of the embolization coils [17] have been reported. Gentle, meticulous technique and careful soft tissue handling are utmost important to minimize intra-operative complications.
In case of a long segment of artery is involved, we recommend reconstruction with vein autograft, like what we have done in our case, as synthetic conduit might not be a feasible alternative option as those of small caliber (d <6mm>
We aware that the major limitation of our case report is that a single case lacks generalizability to confirm the safety and durability of auto-vein-grafting in patients with vEDS. We would therefore recommend further study on the use of autologous vein graft with longer duration of follow-up.
Last but not least, the missense variant c. 1852G>C in the COL3A1 gene detected in this patient changed the 618th codon from Glycine to Arginine. It is classified as likely pathogenic by American College of Medical Genetics (ACMG) guideline. This variant has not been reported in literatures or Human Gene Mutation Database. A different missense change c. 1853G>T in the same codon has been reported as disease causing for vEDS phenotypes in previous study [20,21].
Conclusion
Although rare, acute limb compartment syndrome could happen spontaneously in patient with vEDS. High index of suspicion of compartment syndrome, timely urgent fasciotomy and vascular intervention with meticulous technique and gentle soft tissue handling during operation are the keys to prevent complications. We believe that autologous saphenous vein grafting is a safe, durable option to reconstruct a long segment of arterial defect in this group of patients. However, in view of underlying fragility of patient’s own veins, further study is recommended to confirm the long-term outcome of using autologous vein graft in treating patients with vEDS.
References
- Via AG, Oliva F, Spoliti M, Maffulli N. (2015). Acute compartment syndrome. Muscles Ligaments Tendons J. 2015; 5(1):18-22.
View at Publisher | View at Google Scholar - Germain DP. (2007). Ehlers-Danlos syndrome type IV. Orphanet J Rare Dis 2007; 2:32.
View at Publisher | View at Google Scholar - Barabas AP, (1972). Vascular complications in the Ehlers-Danlos syndrome, with special reference to the (arterial type) or Sack's syndrome. J Cardiovasc Surg (Torino) 1972, 13:160-167.
View at Publisher | View at Google Scholar - Byers PH. Vascular Ehlers-Danlos Syndrome. 1999 Sep 2 [updated 2019 Feb 21]. In: Adam MP, Ardinger HH, Pagon RA, Wallace SE, Bean LJH, Gripp KW, Mirzaa GM, Amemiya A, editors. GeneReviews® [Internet]. Seattle (WA): University of Washington, Seattle; 1993–2021.
View at Publisher | View at Google Scholar - Pepin M, Schwarze U, Superti-Furga A, Byers PH. (2000). Clinical and genetic features of Ehlers-Danlos syndrome type IV, the vascular type. N Engl J Med. 2000 Mar 9; 342(10):673-680
View at Publisher | View at Google Scholar - Schmalzried TP, Eckardt JJ. (1992). Spontaneous gluteal artery rupture resulting in compartment syndrome and sciatic neuropathy. Report of a case in Ehlers-Danlos syndrome. Clin Orthop Relat Res. 1992 Feb; (275):253-257.
View at Publisher | View at Google Scholar - Oderich GS, Panneton JM, Bower TC, Lindor NM, Cherry KJ, Noel AA, Kalra M, Sullivan T, Gloviczki P. (2005). The spectrum, management and clinical outcome of Ehlers-Danlos syndrome type IV: a 30-year experience. J Vasc Surg. 2005 Jul; 42(1):98-106.
View at Publisher | View at Google Scholar - Mandeville K, Bicknell C, Tran T, MacDermot K, Renton S. (2008). Pseudoaneurysm of the peroneal artery: presentation of Ehlers-Danlos syndrome type IV. Eur J Vasc Endovasc Surg. 2008 Sep; 36(3):353-355.
View at Publisher | View at Google Scholar - Matsushima K, Takara H. (2009). Endovascular treatment for a spontaneous rupture of the posterior tibial artery in a patient with Ehlers-Danlos syndrome Type IV: report of a case. Surg Today. 2009; 39(6):523–526.
View at Publisher | View at Google Scholar - Barboi A, Dennis C, Timins M, Peltier W, Klotz CM, Jaradeh S. (2009). Neuromuscular manifestations in a patient with ehlers-danlos syndrome type IV. J Clin Neuromuscul Dis. 2009 Dec; 11(2):81-87.
View at Publisher | View at Google Scholar - Ikeda K, Osamura N, Kasashima S. (2012). The bilateral ulnar artery involvement in Type IV Ehlers-Danlos syndrome - a case report. Hand Surg. 2012; 17(2):213-216.
View at Publisher | View at Google Scholar - Domenick N, Cho JS, Abu Hamad G, Makaroun MS, Chaer RA. (2011). Endovascular repair of multiple infrageniculate aneurysms in a patient with vascular type Ehlers-Danlos syndrome. J Vasc Surg. 2011 Sep; 54(3):848-850.
View at Publisher | View at Google Scholar - Arici V, Corbetta R, Fossati LG, Odero A. (2013). Acute first onset of Ehlers-Danlos syndrome type 4 with spontaneous rupture of posterior tibial artery pseudoaneurysm. Vascular. 2013 Feb; 21(1):43-45.
View at Publisher | View at Google Scholar - Howard R, Osborne N. (2020). Ruptured ulnar artery aneurysm in vascular Ehlers-Danlos syndrome. J Vasc Surg Cases Innov Tech. 2020 Feb 12; 6(1):71-74.
View at Publisher | View at Google Scholar - Choinski KN, Ilonzo N, Tadros RO, Olin JW, Phair J. (2021). Spontaneous compartment syndrome and endovascular repair of tibioperoneal trunk pseudoaneurysm in Ehlers-Danlos syndrome. J Vasc Surg Cases Innov Tech. 2021 Sep 28; 7(4):701-705.
View at Publisher | View at Google Scholar - Brooke BS, Arnaoutakis G, McDonnell NB, Black JH 3rd. (2010). Contemporary management of vascular complications associated with Ehlers-Danlos syndrome. J Vasc Surg. 2010 Jan;51(1):131-138; discussion 138-139.
View at Publisher | View at Google Scholar - Eagleton MJ. (2016). Arterial complications of vascular Ehlers-Danlos syndrome. J Vasc Surg. 2016 Dec; 64(6):1869-1880.
View at Publisher | View at Google Scholar - Ravi S, Qu Z, Chaikof EL. Polymeric materials for tissue engineering of arterial substitutes. Vascular. 2009; 17 Suppl 1(Suppl 1):S45-S54.
View at Publisher | View at Google Scholar - Shalhub S, Byers PH, Hicks KL, Charlton-Ouw K, Zarkowsky D, Coleman DM, Davis FM, Regalado ES, De Caridi G, Weaver KN, Miller EM, Schermerhorn ML, Shean K, Oderich G, Ribeiro M, Nishikawa C, Behrendt CA, Debus ES, von Kodolitsch Y, Powell RJ, Pepin M, Milewicz DM, Lawrence PF, Woo K. (2019). A multi-institutional experience in the aortic and arterial pathology in individuals with genetically confirmed vascular Ehlers-Danlos syndrome. J Vasc Surg. 2019 Nov;70(5): .1543-1554.
View at Publisher | View at Google Scholar - Frank M, Albuisson J, Ranque B, Golmard L, Mazzella JM, Bal-Theoleyre L, Fauret AL, Mirault T, Denarié N, Mousseaux E, Boutouyrie P, Fiessinger JN, Emmerich J, Messas E, Jeunemaitre X. (2015). The type of variants at the COL3A1 gene associates with the phenotype and severity of vascular Ehlers-Danlos syndrome. Eur J Hum Genet. 2015 Dec; 23(12):1657-1664.
View at Publisher | View at Google Scholar - Legrand A, Devriese M, Dupuis-Girod S, Simian C, Venisse A, Mazzella JM, Auribault K, Adham S, Frank M, Albuisson J, Jeunemaitre X. (2019). Frequency of de novo variants and parental mosaicism in vascular Ehlers-Danlos syndrome. Genet Med. 2019; 21:1568–1575.
View at Publisher | View at Google Scholar
