

Research Article | DOI: https://doi.org/10.31579/2834-796X/028
Associations between High Sensitivity Troponin in the Emergency Department and Diagnosis of Myocarditis
- Ela Giladi 1,3*±
- Reut Ratzon 2±
- Ziad Arow 1,3
- Ilya Losin 1,3
- Alexander Omelchenko 1,3
- David Pereg 1,3
- Abid Assali 1,3
- Yoav Arnson 1,3
1 Department of Cardiology, Meir Medical Center,Kfar Saba, Israel.
2 Department of Emergency Medicine,Meir Medical Center,Kfar Saba, Israel.
3 Sackler School of Medicine,Tel Aviv University, Tel Aviv, Israel.
± These authors contributed equally to this work.
*Corresponding Author: Ela Giladi, MD. Department of Cardiology, Meir Medical Center, Kfar Saba, Israel.
Citation: Ela Giladi, Reut Ratzon, Ziad Arow, Ilya Losin, Alexander Omelchenko, et all, (2023), Associations between High Sensitivity Troponin in the Emergency Department and Diagnosis of Myocarditis, International Journal of Cardiovascular Medicine, 2(3); DOI:10.31579/2834-796X/028
Copyright: © 2023, Ela Giladi. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 29 May 2023 | Accepted: 20 June 2023 | Published: 27 June 2023
Keywords: myocarditis; troponin; diagnosis; prognosis
Abstract
Background: The diagnosis of myocarditis is challenging, and typically relieson clinical presentation, non-invasive imaging, and serum biomarkers. We examine if implementation of hsTnT has affected recognition of myocarditis and patient outcomes.
Methods: Retrospective analysisof >18-year-old patientsdiagnosed with myocarditis in Meir MedicalCenter since January 2000 to the end of April 2020. Patients were divided based on their diagnosis date - up to January 2014, for which there was a regular troponin test (REG group) and starting February 2014 for which there was a hsTnT test (HS group). We examined the difference in the rate of myocarditis diagnosis, mortality, and hospitalizations due to heart failure.
Results: We identified 262 patients who were diagnosed with myocarditis. There were no significant differences between the groups. After the implementation of hsTnT there was a two-fold increase in the diagnosis rate (0.0366 vs. 0.0625 cases per day; P<0.0001). The REG group presented with more ST changes (51% vs. 29%; p=0.006) and less cases of normal heart function (69% vs. 79%; P=0.048). There was a higher mortality rate in HS group (6 deaths vs. 2;p=0.011).
Conclusions : hsTnT test leadsto increase in myocarditis diagnosis and allows for diagnosing more mild case.
Introduction
Myocarditis is a potentially life-threatening inflammatory condition of the myocardium which most often occurs secondary to an infection but can also be immune-mediated due to exposure to toxic substances. Myocarditis is an uncommonand likely underdiagnosed condition which presents with a wide range of cardiac and extra-cardiac symptoms(1, 2). The incidence of myocarditis is difficult to determine as endomyocardial biopsy (EMB), the diagnostic gold standard, is seldom used (3, 4). The Global Burden of Disease study reported an incidence of 22 cases of myocarditis per 100,000 patients based on International Classification of Diseases (ICD) codes on hospital discharge documentation between 1990 and 2013 (5).
Myocarditis prognosis is variable and varies by disease cause and severity. When complicated by left ventricular (LV) dysfunction, heart failure (HF) or arrhythmia it is associated with a poor prognosis (6). Most of the available data relies on small series, animal experimental models and case reports (7, 8). Given the lack of consensus regarding the role of EMB and the excellent prognosis of patients with mild uncomplicated myocarditis, a recent agreement statement recommends that EMB be reserved for patients who are likely to have specific myocardial disorders associated with worse prognosesand specific treatment recommendations (9). Cardiac troponins are sensitive of myocyte injury in patients with clinically suspected myocarditis. However,they are non-specific and when normal do not exclude myocarditis (10, 11). In the past few years, highly sensitive troponin tests allow detection of minimal increase in serum troponin levels and can possibly identify more patients with myocarditis. A small study by Ukena et al. demonstrated that high sensitivetroponin-T (hsTnT) is a predictive marker for the diagnosis of acute myocarditis with a sensitivity of 83% and specificity of 80% using a cutoff of 50ng/L (12).
Highly sensitive troponin test had become feasible at our medical center Since February 1st, 2014. The aims of this study were to detect trends in myocarditis diagnosis with the use of hsTnT, and to determine if different lab studies led to any difference in the clinicalcharacterization and prognosis of the patients diagnosed with myocarditis.
Methods
Study design: A retrospective single center cohort study. The cohort included patients newly diagnosed with acute myocarditis at Meir Medical Center between January 1st, 2000, and April 30th, 2020. The source of data was Meir Medical Center's computerized records which contain all themedical information, including imaging studies, obtained during an emergencyroom visit, hospital admissions and outpatient follow-up. Potentially eligiblepatients were identified by screening for patients with an ICD-9 diagnosis or an imagingreport of myocarditis. Eligibility criteria were age 18 years or older and newly diagnosed myocarditis with a positive troponin test. Patients younger than 18 and those with missing data were censored from the cohort.
Clinical diagnosis of acute myocarditis was based on constellation of signs and symptoms, electrocardiogram (ECG) findings and cardiac biomarkers typically seen inmyocarditis, with exclusion of acute coronary syndrome.
All relevantcases were manually retrieved and examined.Baseline characteristics collected were demographic data, lab studies including baseline troponin,cardiovascular risk factors(diabetes mellitus, hypertension, dyslipidemia and smoking), presenting symptoms and vital signs at admission (Table 1). Positive troponin tests were defined as >0.1 mg/L (100 ng/L) for the "regular" troponin test (REG group) and >14 ng/L (0.014 mg/L) for the hsTnT test (HS group).
ECG strips were examined for ST segment deviation or T wave abnormalities. Echocardiography findings include biventricularfunction and evidenceof pericardial effusion.Radiological characteristics of myocarditis were determined from reports of all available cardiac MRI studies. Due to the different periods in which cases were collected, follow-up was limited to 6 years in both groups. Patients were followed for repeated admissions due to heart failure and for all-cause mortality.
Statistical methods
The Patients were grouped by date of admission and type of troponin test used upon diagnosis. The first group was composed of patients diagnosed with myocarditis between January 1st, 2000, and January 31st, 2014, in the REG group and the second group was composed of patients diagnosed with myocarditis from February 1st, 2014, to April30th, 2020 in theHS group.
The primary outcome was myocarditis diagnosis rate after HS-troponin test employment in the emergency room setting. Secondary outcomes were the mild myocarditis cases diagnosed (normalLV function and no cardiac sequela),hospitalization for heart failure and overall mortality.
Data are presented as median (inter-quartile range [IQR]) for continuous variablesand frequency (%) for categorical variables. Baseline characteristics between patients were compared using two-sample t-test was used for continuous data and a χ2 test, for categorical data.The cumulative incidence of the primary outcome over follow-up period and corresponding 95% confidence intervals (CI) was calculated for each group with death as competing risk and comparison of the two groups using logrank test. Clinically statistical significance was determined as P<0> The study was approved by the Institutional Ethics Committees in accordance with the Declaration of Helsinki
Results
The study cohort included 262 consecutive patients newly diagnosed with acute myocarditis. The REG included 121 patients; HS group included 141 patients. Clinical characteristics, risk factors and demographic features are presented in Table 1.
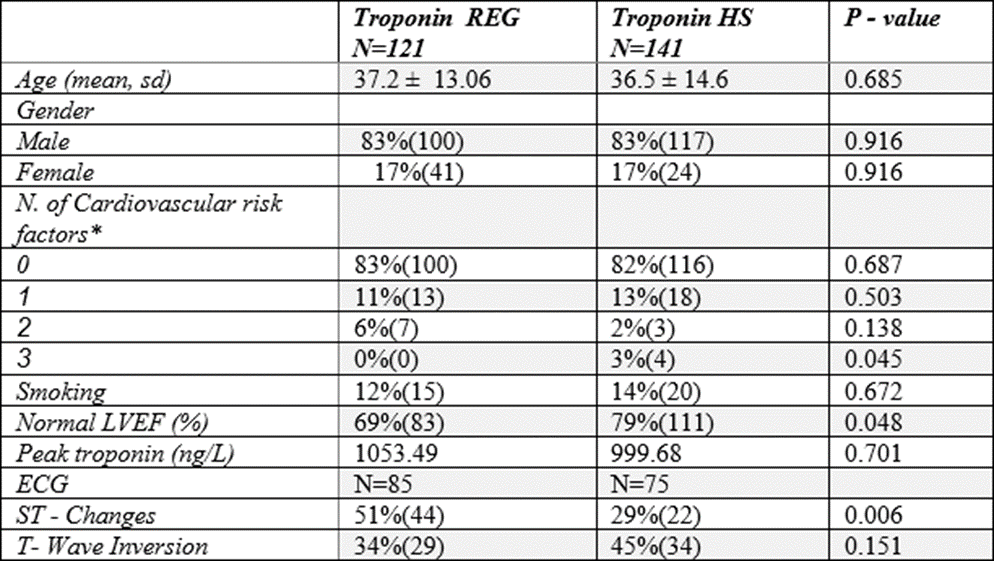
*Cardiovascular risk factors:Diabetes, Hypertension, Dyslipidaemia
LVEF= left ventricular ejection fraction
Table 1: Baselinecharacteristics
Mean age was 37.2 ± 13.6 years in the REG group and 36.5 ± 14.62 in HS group (p=0.685), most of patients were male (83% in the two groups). Mean troponin values were 1053.49 ± 944.78 in REG group and 999.68 ± 1264.23ng/L in HS group(p=0.701).Myocarditis diagnosisrate: Using hsTnT, there was a nearly two-fold increase in the incidence rate of myocarditis (0.063 patients per day, a patient every 16 days and 0.037 patients per day- a patient every 7 days, respectively), with statistically significance of P<0>.
Clinical and prognosis outcomes: Only 50% of patients in each group had complete ECG data. Higherdegree of ST segment changes were observed in REG group, 51% vs. 29% (44/87 patients and 22/75 patients respectively), p=0.006,as presented in figure 1. No significant difference was found in T wave abnormalities between the groups (P=0.151). Patients in the HS group patients had higher rates of normal LV function in echocardiography. Of 141 patientsin HS group, 111 patients (79%)had normal LV function comparedto 83 of 121 patients (69%) in REG group, p=0.048 (figure 2). During follow-up period, only 3 patients were subjected to recurrent hospitalization due to exacerbation of heart failure, of which 1 in REG group and 2 in HS group, with no statistical significance. Eight patients have died duringfollow-up, with higher all-cause mortality rate in HS group (6/140 patients) compared with REGgroup (2/121 patients), with P=0.011 (figure 3).
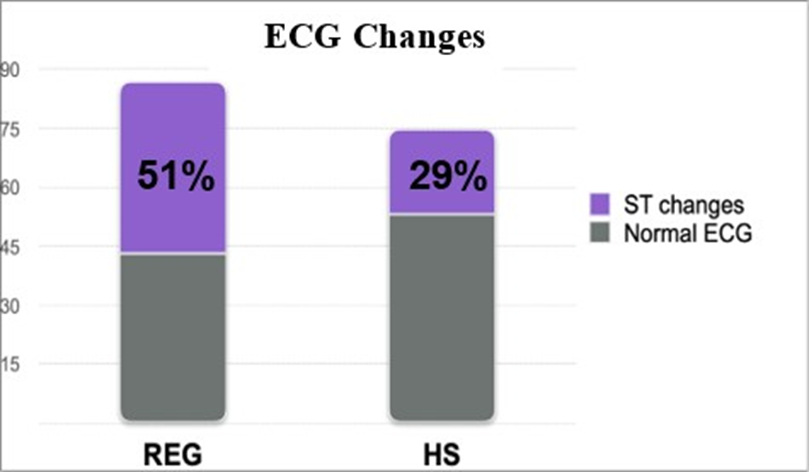
Figure 1: Changersin ECG
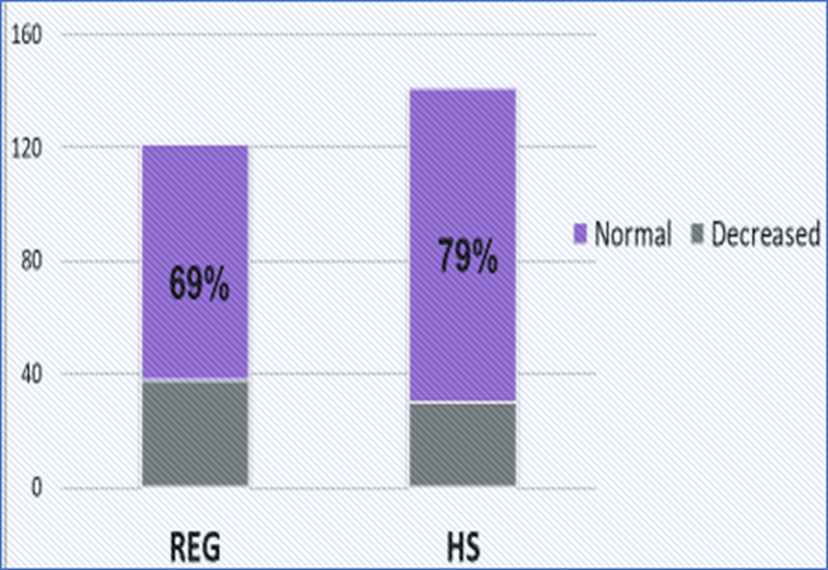
Figure 2: LV Function
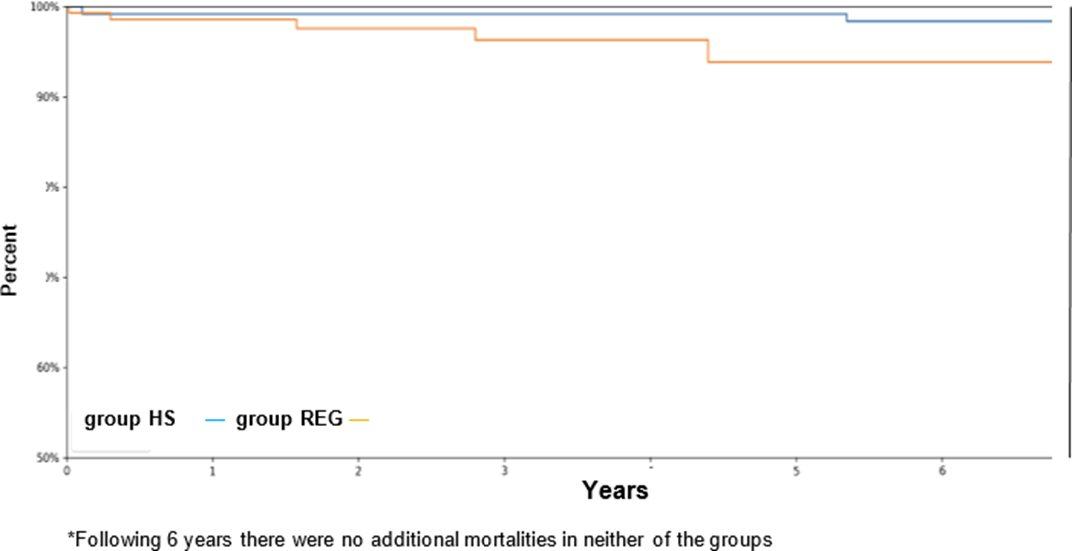
Figure 3: Kaplan-Meier curve for mortality
Discussion
Louis criteria, myocarditis can be predicted with a diagnostic accuracy of our research shows that the use of hsTnT in the ER results in improved identification rates of myocarditis. The improved recognition rate led to identification of comparatively less severe cases with intact LV function. The patients’ demographics and clinical features were comparable across the groups,with male gender predominance. There was no significant difference regarding cardiovascular risk factors and smokers between the groups. These figures were comparable with previous reports of acute myocarditis (14,15). Young adults are most frequently affected. The mean age of adult patients with myocarditis has been reported to range from 20 to 51 years (16,17).
The diagnosis of myocarditis did not result in an increased occurrence of cardiac complications during the follow-up duration. This correlates with previous publications mentioned patients presenting with acute myocarditis and preserved left ventricular function have a good prognosis with a high rate of spontaneous improvement without sequelae (13,14). Nevertheless, in up to 30% of patients with biopsy-proven myocarditis, progression to dilatedcardiomyopathy (DCM) can occur and is associated with a poor prognosis (4).
Myocarditis is a challenging diagnosis, mainly as there is no pathognomonic clinical presentation, and the disease may present as a variety of non-inflammatory myocardial conditions. Myocarditis has a wide diversity of clinical manifestations, which may range from subclinical to fulminant heart failure.
The gold standard for the diagnosis of myocarditis is the EMB. According to the Dallascriteria, acute myocarditis is defined as the histologic evidence of lymphocytic infiltrates in association with myocyte necrosis (18).
However, subjected to sampling error,variation in expert interpretation, alteration with other markers of viral infection and immune activation in the heart, EBM seldom is used in clinical routine, and is usually reserved for selected cases with severe or rapidly progressive symptoms (1). Thus, the diagnosis is commonlyestablished by clinicalpresentation, cardiac biomarkers, and noninvasive imaging findings. Cardiac MRI is a beneficial tool for the diagnosis of myocarditis, with high sensitivity and specificity. This modality can detect intracellular and interstitial edema, capillary leakageand hyperemia that support the diagnosis of myocarditis (Lake Louis criteria) and in severe cases cellular necrosis and interstitial fibrosis.Based on the Lake 78% (19). In our study, however, cardiac MRI was only attainable during later period, and for only a small number of patients (12,8.5%). In REG group there were no patients diagnosed with the assistance of MRI. In patients with a history suggestive of myocarditis, an increased cardiac troponin implies myocardial injury, particularly when measured with an assay with high precision. Experimental and clinical studies suggest that serum hsTnT can be a useful diagnostic tool early in the course of myocarditis (20,21). Cardiac biomarkers in fulminant myocarditis can reachlevels similar to those in patients with transmural myocardial infarctions caused by epicardial coronary occlusions (2). Multiple mechanisms are causative of cardiac troponin leakage in these situations, not solely restricted to irreversible cardiomyocyte necrosis. Potential pathways also include increased left–ventricular filling pressures with subsequent myocardial wall stress,toxicity from inflammatory cytokines, oxidative stress,catecholamine excess and direct cellular damage. However, an absence in hsTnT rise does not rule out myocarditis (22). Observational studies had failed to prove a significant correlation between the magnitude of troponin measured and prognosis (23-25). In our study, the mean troponin-T peak in the REG group was 1053.49 ng/L compared with 999.68 ng/L in the HS group. Like previousreports, we couldnot find a correlation with maximal troponin levels and mortality. This points towards the significance of troponin as a diagnostic rather than prognostic tool. Despite the common use of ECG as an availablescreening tool, the sensitivity for myocarditis is merely 47%. The most frequently seen ECG findings are nonspecific T-wave changes. Occasionally, the ECG changes may mimic acute myocardial infarction or pericarditis with ST-segment elevation, ST-segment depression, PR depression, and pathologic Q waves (26,27). In recent studies, QRS prolongation was an independent negative predictor for survival, while Q-waves and repolarization abnormalities were unrelated to outcome or inflammatory histological features on EMB (28). In referral populations, new-onset supraventricular or ventricular arrhythmias occur in up to 55% of patients (29), they are often non-sustained and rarely cause hemodynamic compromise. The occurrence of abnormal QRS complexes, axis deviation, or new left bundle branch block is associated with higher rates of mortality or cardiac transplantation (15,26,30).
In our study, more ST changes were present in the REG group than the HS group (51% and 29%, respectively), and no differences were noted in T wave changes. It should be mentioned that measuring QRS interval or T wavelength was not possible due to physical lack of ECG stripes from 20-year-old files, and only ECG reports were available.
Echocardiography is important for evaluation of myocardial damage and heart failure, and for assessment of ventricular thrombi and pericardial effusion. Nevertheless, there are no specific echocardiographic features of myocarditis. Segmental or globalwall motion abnormalities are non-specific and can masquerade as myocardial infarction. Patients with fulminant myocarditis tend to present with a non-dilated, thickened, and a hypocontractile left ventricle, where as patients with mild myocarditis usually present with normal wall thickness. Right ventricular dysfunction is rare but an important predictor of mortality or cardiac transplantation (31).
The REG group of patients included more patients with ECG changes and a higher fraction of patients with left ventricular dysfunction on echocardiography. Thus, it is assumed that HS troponin test had increased the diagnosis rate of patients with mild myocarditis that is not reflected by ECG or echocardiographic findings.
There were more mortality cases in the HS group compared to REG group (6/140 vs. 2/121 patients respectively). This could be partially explained by under diagnosed patients that were not included in the REG group. Our study had several limitations. First, it is of retrospective nature, which is prone to selection bias. Second, myocarditis diagnosis was also debatable.
Myocarditis is traditionally defined by lymphocytic infiltrated in association with myocyte necrosis not characteristic for ischemic damage (32). The diagnosis of myocarditis in this study was based on clinical suspicion, evidence of myocardial injury,and the exclusion of an acute coronaryevent. It could be that events identified as myocarditis were in fact atherosclerotic heart disease without significant coronary stenosis, and vice versa, thus a more accurate diagnosis might have affected study results. Third, the study expands over a period of 20 years, during this time some of the documentation was manually retrieved, which may have led to emitting of undiagnosed cases.Some patient files had only partial data, such as a single troponin test, and that could impact peak troponin calculations. Different follow up periods could have also affected outcomes for recurrent hospitalizations. Fourth, the study was conducted in a singlecenter in Israel,clinical practicemay vary from different centers in Israel and other countries.
Conclusion:
hsTnT test in suspected myocarditis cases can increase the diagnostic yield and allow detection of more mild cases. More data is necessary to establish its prognostic value.
Acknowledgments
The authors declare that no funds, grants, or other support were received during the preparation of this manuscript. The authors have no relevant financial or non-financial interests to disclose. All authors contributed to the study conception and design. Material preparation, data collection and analysis were performed by Dr. Reut Ratzon and Dr. Ela Giladi. The first draft of the manuscript was written by Dr. Ela Giladi and all authors commented on previous versions of the manuscript. All authors read and approved the final manuscript. The authors affirm that human research participants provided informed consent for publication.
References
- Blauwet LA, Cooper LT. (2010) Myocarditis. Prog Cardiovasc Dis. 52(4):274-88.
View at Publisher | View at Google Scholar - Kociol RD, Cooper LT, Fang JC, Moslehi JJ, Pang PS, Sabe MA, et al. (2020) Recognition and Initial Management of Fulminant Myocarditis: A Scientific Statement From the American Heart Association. Circulation. 141(6): e69-e92.
View at Publisher | View at Google Scholar - Richardson P, McKenna W, Bristow M, Maisch B, Mautner B, O'Connell J, et al. (1996) Report of the 1995 World Health Organization/International Society and Federation of Cardiology Task Force on the Definition and Classification of cardiomyopathies. Circulation. 93(5):841-2.
View at Publisher | View at Google Scholar - Kindermann I, Barth C, Mahfoud F, Ukena C, Lenski M, Yilmaz A, et al. (2012) Update on myocarditis. J Am Coll Cardiol. 59(9):779-92.
View at Publisher | View at Google Scholar - Global Burden of Disease Study C. Global, regional, and national incidence, prevalence, and years lived with disability for 301 acute and chronic diseases and injuries in 188 countries, 1990-2013: a systematic analysis for the Global Burden of Disease Study 2013. Lancet. 2015;386(9995):743-800.
View at Publisher | View at Google Scholar - Ammirati E, Cipriani M, Moro C, Raineri C, Pini D, Sormani P, et al. (2018) Clinical Presentation and Outcome in a Contemporary Cohort of Patients With Acute Myocarditis: Multicenter Lombardy Registry. Circulation. 138(11):1088-99.
View at Publisher | View at Google Scholar - Caforio AL, Marcolongo R, Basso C, Iliceto S. (2015) Clinical presentation and diagnosis of myocarditis. Heart. 101(16):1332-44.
View at Publisher | View at Google Scholar - Caforio ALP, Malipiero G, Marcolongo R, Iliceto S. (2017) Myocarditis: A Clinical Overview. Curr Cardiol Rep. 19(7):63.
View at Publisher | View at Google Scholar - Cooper LT, Baughman KL, Feldman AM, Frustaci A, Jessup M, Kuhl U, et al. (2007) The role of endomyocardial biopsy in the management of cardiovascular disease: a scientific statement from the American Heart Association, the American College of Cardiology, and the European Society of Cardiology. Circulation. 116(19):2216-33.
View at Publisher | View at Google Scholar - Heymans S. (2007) Myocarditis and heart failure: need for better diagnostic, predictive, and therapeutic tools. Eur Heart J. 28(11):1279-80.
View at Publisher | View at Google Scholar - Lauer B, Niederau C, Kuhl U, Schannwell M, Pauschinger M, Strauer BE, et al. Cardiac troponin T in patients with clinically suspected myocarditis. J Am Coll Cardiol. 1997;30(5):1354-9.
View at Publisher | View at Google Scholar - Ukena C, Kindermann M, Mahfoud F, Geisel J, Lepper PM, Kandolf R, et al. (2014) Diagnostic and prognostic validity of different biomarkers in patients with suspected myocarditis. Clin Res Cardiol. 103(9):743-51.
View at Publisher | View at Google Scholar - Anzini M, Merlo M, Sabbadini G, Barbati G, Finocchiaro G, Pinamonti B, et al. (2013) Long-term evolution and prognostic stratification of biopsy-proven active myocarditis. Circulation. 128(22):2384-94.
View at Publisher | View at Google Scholar - Caforio AL, Calabrese F, Angelini A, Tona F, Vinci A, Bottaro S, et al. (2007) A prospective study of biopsy-proven myocarditis: prognostic relevance of clinical and aetiopathogenetic features at diagnosis. Eur Heart J. 28(11):1326-33.
View at Publisher | View at Google Scholar - Magnani JW, Danik HJ, Dec GW, Jr., DiSalvo TG. (2006) Survival in biopsy-proven myocarditis: a long-term retrospective analysis of the histopathologic, clinical, and hemodynamic predictors. Am Heart J. 151(2):463-70.
View at Publisher | View at Google Scholar - Cooper LT, Jr., Berry GJ, Shabetai R. (1997) Idiopathic giant-cell myocarditis--natural history and treatment. Multicenter Giant Cell Myocarditis Study Group Investigators. N Engl J Med. 336(26):1860-6.
View at Publisher | View at Google Scholar - Kyto V, Saukko P, Lignitz E, Schwesinger G, Henn V, Saraste A, et al. (2005) Diagnosis and presentation of fatal myocarditis. Hum Pathol. 36(9):1003-7.
View at Publisher | View at Google Scholar - Aretz HT, Billingham ME, Edwards WD, Factor SM, Fallon JT, Fenoglio JJ, Jr., et al. (1987) Myocarditis. A histopathologic definition and classification. Am J Cardiovasc Pathol. 1(1):3-14.
View at Publisher | View at Google Scholar - Friedrich MG, Sechtem U, Schulz-Menger J, Holmvang G, Alakija P, Cooper LT, et al. (2009) Cardiovascular magnetic resonance in myocarditis: A JACC White Paper. J Am Coll Cardiol. 53(17):1475-87.
View at Publisher | View at Google Scholar - Bachmaier K, Mair J, Offner F, Pummerer C, Neu N. (1995) Serum cardiac troponin T and creatine kinase-MB elevations in murine autoimmune myocarditis. Circulation. 92(7):1927-32.
View at Publisher | View at Google Scholar - Smith SC, Ladenson JH, Mason JW, Jaffe AS. (1997) Elevations of cardiac troponin I associated with myocarditis. Experimental and clinical correlates. Circulation. 95(1):163-8.
View at Publisher | View at Google Scholar - Jani SM, Nallamothu BK, Cooper LT, Smith A, Fazel R. (2017) Beating, Fast and Slow. N Engl J Med. 377(1):72-8.
View at Publisher | View at Google Scholar - Gilotra NA, Minkove N, Bennett MK, Tedford RJ, Steenbergen C, Judge DP, et al. (2016) Lack of Relationship Between Serum Cardiac Troponin I Level and Giant Cell Myocarditis Diagnosis and Outcomes. J Card Fail. 22(7):583-5.
View at Publisher | View at Google Scholar - Aquaro GD, Perfetti M, Camastra G, Monti L, Dellegrottaglie S, Moro C, et al. (2017) Cardiac MR With Late Gadolinium Enhancement in Acute Myocarditis With Preserved Systolic Function: ITAMY Study. J Am Coll Cardiol. 70(16):1977-87.
View at Publisher | View at Google Scholar - Eggers KM, Lindahl B. (2017) Application of Cardiac Troponin in Cardiovascular Diseases Other Than Acute Coronary Syndrome. Clin Chem. 63(1):223-35.
View at Publisher | View at Google Scholar - Morgera T, Di Lenarda A, Dreas L, Pinamonti B, Humar F, Bussani R, et al. (1992) Electrocardiography of myocarditis revisited: clinical and prognostic significance of electrocardiographic changes. Am Heart J. 124(2):455-67.
View at Publisher | View at Google Scholar - Dec GW, Jr., Waldman H, Southern J, Fallon JT, Hutter AM, Jr., Palacios I. (1992) Viral myocarditis mimicking acute myocardial infarction. J Am Coll Cardiol. 20(1):85-9.
View at Publisher | View at Google Scholar - Ukena C, Mahfoud F, Kindermann I, Kandolf R, Kindermann M, Bohm M. (2011) Prognostic electrocardiographic parameters in patients with suspected myocarditis. Eur J Heart Fail. 13(4):398-405.
View at Publisher | View at Google Scholar - Kuhl U, Pauschinger M, Seeberg B, Lassner D, Noutsias M, Poller W, et al. (2005) Viral persistence in the myocardium is associated with progressive cardiac dysfunction. Circulation. 112(13):1965-70.
View at Publisher | View at Google Scholar - Nakashima H, Katayama T, Ishizaki M, Takeno M, Honda Y, Yano K. (1998) Q wave and non-Q wave myocarditis with special reference to clinical significance. Jpn Heart J. 39(6):763-74.
View at Publisher | View at Google Scholar - Hazebroek MR, Everaerts K, Heymans S. (2014) Diagnostic approach of myocarditis: strike the golden mean. Neth Heart J. 22(2):80-4.
View at Publisher | View at Google Scholar - Guglin M, Nallamshetty L. (2012) Myocarditis: diagnosis and treatment. Curr Treat Options Cardiovasc Med. 14(6):637-51.
View at Publisher | View at Google Scholar
