

Research Article | DOI: https://doi.org/10.31579/2835-785X/070
Assess Health Belief Model of Breast Cancer and Its Preventive Measures among Beni-Suef University Female Workers
1 Lecturer of Maternal & Newborn Health Nursing, Faculty of Nursing, Beni-Suef University, Egypt.
2 Demonstrator of Maternal & Newborn Health Nursing, Faculty of Nursing, Beni-Suef University, Egypt.
3 Professor of Maternal and Newborn Health Nursing, Faculty of Nursing, Beni-Suef University, Egypt.
*Corresponding Author: Hanan Elzeblawy Hassan, Professor of Maternal and Newborn Health Nursing, Faculty of Nursing, Beni-Suef University, Egypt.
Citation: Fatma Saber Nady, Sahar Gamal Zaki, Hanan Elzeblawy Hassan, (2025), Assess Health Belief Model of Breast Cancer and Its Preventive Measures among Beni-Suef University Female Workers, International Journal of Clinical Research and Reports. 4(2); DOI:10.31579/2835-785X/070
Copyright: © 2025, Hanan Elzeblawy Hassan. This is an open-access artic le distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 07 February 2025 | Accepted: 17 February 2025 | Published: 28 February 2025
Keywords: assessment; health belief model; breast cancer; female workers
Abstract
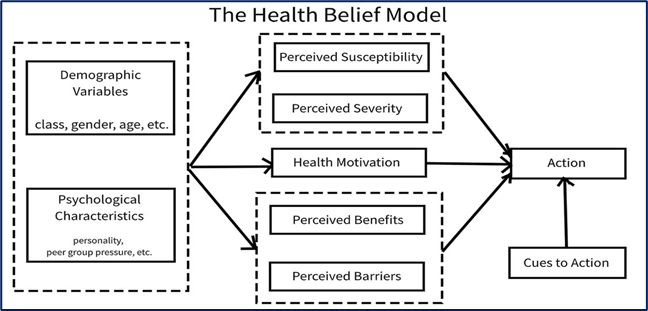
Background: Breast cancer, a disease originating from the breast, is characterized by benign tumors within the breast membrane. The Health Belief model (HBM) addresses perceived disease severity, susceptibility, benefits, barriers, and self-efficacy. Enhancing the HBM by including self-efficacy can better explain individual health behaviors and improve understanding of disease severity and benefits
Aim: The current study was conducted to assess health belief model of breast cancer and its preventive measures among Beni-Suef university female workers.
Subjects and Methods: Design: A descriptive design was utilized. Sample and Settings: 323 working women at Beni-Suef University. Tools: Tool I: A Structured Interviewing Questionnaire Sheet. Tool II: Health Belief Model Questionnaire.
Results: It revealed that for sub-item of health belief model, strongly agreement was reported as; perceived susceptibility (37.8%), perceived seriousness (40.6%), perceived benefits (14.2%), perceived barriers (17.6%), perceived cues to action (18%), and perceived self-efficacy beliefs (16.1%).
Conclusion: Based on the findings of the present study, it can be concluded most of the studied female workers had negative attitude toward all sub-items of health belief model regarding breast cancer, breast self-examination, and breast cancer preventive measures.
Recommendations: Implement an educational program based on health belief model to enhance women’s all item of beliefs including susceptibility, seriousness, benefits, barriers, cues to action, and self-efficacy regarding breast cancer and preventive measures.
Introduction
Breast cancer is a disease that originates from the breast and emerges mostly from the epithelial cells lining the milk ducts [1-5]. Although carcinomas are cancerous by definition, benign tumors of the breast contained inside the basement membrane are described as ductal carcinoma in situ (DCIS) and lobular carcinoma in situ (LCIS) [6-10].
The Health Belief model is a conceptual theoretical framework that has been widely utilized to address issues related to perceived disease severity, perceived susceptibility to the disease, perceived advantages of seeking preventive actions, and perceived obstacles to seeking those actions [11-14].
The four elements of the HBM perceived susceptibility, severity, benefits, and barriers—were expanded in 1988 to include self-efficacy. A person's belief in their ability to act successfully is known as self-efficacy. An attempt was made to enhance the HBM by including self-efficacy to better explain individual variations in health behaviors [15].
The subjective estimation of one's vulnerability to the emergence of a health issue is known as perceived susceptibility. According to the HBM, people who believe they are vulnerable to a certain health issue will take action to lower their chance of experiencing that issue [16].
People who don't think they are susceptible to a certain ailment might not believe they are. While some may accept the chance of contracting the sickness, they think it is implausible. People who think they have little chance of getting sick are more likely to take risks or participate in dangerous practices. People are more inclined to take actions to lower their chance of contracting a sickness when they believe there is a high chance they will be directly impacted by it [17-19].
The subjective evaluation of the seriousness of a health issue and its possible outcomes is known as perceived severity. According to the Health Belief Model (HBM), people who view a particular health issue as serious are more likely to take action to stop it from happening or lessen its severity. Perceived seriousness includes opinions about the illness itself, such as whether it is terminal or may result in pain or impairment, as well as more general effects on the capacity to perform social and occupational duties [20].
A person's assessment of the severity of a disease, the events that transpired after a diagnosis and their personal feelings on the consequences of a particular medical condition are all included in the concept of perceived severity. Potential medical ramifications include pain, incapacity, and death; potential social ramifications include effects on work, family life, and social relationships. When perceived severity and susceptibility are combined, the result is called perceived threat [21-23]. For example, a person may believe that breast cancer is not a serious medical condition, but if that person believes that missing work for several days would have a significant financial impact, that person may believe that breast cancer is a particularly serious condition [24-26].
The advantages of acting are another factor that influences health-related behavior. An individual's evaluation of the worth or effectiveness of adopting a health-promoting action to lower the risk of disease is known as perceived benefits. Regardless of objective information about the efficacy of a certain action, a person is likely to engage in it if they believe it will lessen their vulnerability to a health problem or lessen the severity of the problem. For instance, those who think that eating a healthy diet protects against breast cancer are more likely to eat healthily than others who think that eating a good diet won't stop breast cancer from happening [27].
The perceived benefits construct is a person's evaluation of the value or utility of a fresh activity in reducing the likelihood of becoming unwell. Perceived benefits of adopting a health action, or the health benefits of carrying out a health action, are the determining factor in attitudes toward changing one's behavior. Perceived benefits have a big impact on screenings and other secondary prevention measures. It is well-accepted that early identification of breast cancer increases the likelihood of survival [21].
Perceived obstacles to action also influence health-related behaviors. Perceived barriers pertain to an individual's evaluation of the impediments to altering their behavior. Obstacles may keep someone from engaging in a health-promoting behavior, even if they think that doing so will significantly lessen the threat that their health condition poses. Put another way, for behavior to change, the perceived advantages must exceed the perceived obstacles. The perceived cost, inconvenience, risk (such as adverse effects from medical procedures), and discomfort (such as pain or emotional distress) associated with the conduct are examples of perceived barriers to taking action. Examples of obstacles to practicing BSE include the belief that doing breast self-examination is unpleasant and the lack of access to inexpensive healthcare [28-29].
Perceived impediments are linked to negative aspects of a health-seeking action. It has to deal with how expensive, painful, uncomfortable, distressing, and unpleasant the action is. They could consist of tangible, mental, or emotional elements. Lack of access to care, the expense of treating the illness, the effect on social networks and support systems, the effect on one's family life, and one's line of work can all be barriers to receiving breast cancer treatment. These challenges won't be accepted until the lady feels that the benefits of her health-seeking actions exceed the drawbacks [16]. Individual traits, such as demographic, psychosocial, and structural factors, can influence how health-related actions are evaluated, including their perceived seriousness, susceptibility, advantages, and barriers. Among other things, demographic factors include age, sex, race, ethnicity, and level of education. Social class, personality, and peer and reference group pressure are a few examples of psychosocial variables. Among other things, knowledge of a particular disease and previous exposure to it are examples of structural variables. According to the HBM, changing certain factors may have an indirect impact on health-related behaviors by influencing perceptions of risk, benefits, barriers, and severity [30-34].
According to the HBM, engaging in behaviors that promote health requires a cue, or trigger. Both external and internal cues can prompt behavior. Internal signals to action include physiological cues (pain, illness, etc.). Events or information from close friends and family, the media, or medical professionals that encourage the adoption of healthy behaviors are examples of external cues [35].
Cues to action are situations that might arise from within or without and start a decision-making process about the best way to pursue health. While media messages, social interactions, and the influence of significant others are instances of external cues to take action, disease signs and symptoms are examples of interior cues. If a woman does not think her advanced-stage breast cancer is severe, strong and persuasive cues to action may cause her to change her mind and seek treatment [36].
A dentist's reminder postcard, a friend or family member's illness, public health awareness efforts, and product health warning labels are a few instances of cues to action. Individual differences exist in the perceived seriousness, advantages, impediments, and receptivity of cues required to elicit action [37].
For instance, after watching a public service announcement, people who think they are at high risk for a serious illness and who already have a relationship with a primary care physician may be easily convinced to get screened for the illness; in contrast, people who think they are at low risk for the same illness and who also lack consistent access to healthcare may need stronger external cues to get screened [15]. Self-efficacy is the person's belief in their ability to act successfully is known as self-efficacy. An attempt was made to enhance the HBM by including self-efficacy to better explain individual variations in health behaviors [15]. Originally, the model was created to explain health-related one-time activities like getting a vaccine or going through a cancer screening. In due course, the HBM was extended to include more significant, long-term behavioral changes, including quitting smoking, exercising, and altering one's diet. The model's creators understood that a crucial element of changing health-related behavior was self-efficacy, or the belief in one's capacity to influence changes in outcomes [38].
Aim of the study:
The current study was conducted to assess health belief model of breast cancer and its preventive measures among Beni-Suef university female workers.
Materials and Methods
Research design:
The study employed a descriptive research design to achieve its objectives.
Subjects and Settings:
323 working women from Beni-Suef University make up this group.
Tools of data collection:
Tool I: A Structured Interviewing Questionnaire Sheet
The data includes women's personal and socio-demographic information such as age, education, marital status, residence, and family income (6 items).
Tool II: Health Belief Model Questionnaire:
Subscale (1): perceived susceptibility to breast cancer as (Health status has a role in the development of breast cancer; the possibility of me getting breast cancer increases my anxiety, Doing breast self-examination reduces the risk of breast cancer. Having a family member with breast cancer increases your chance of getting breast cancer in the future. Exercise reduces the incidence of breast cancer.
Subscale (2) perceived severity included (Breast cancer is a hopeless disease; how I feel about myself will change if I get breast cancer, my financial condition will be affected if I get breast cancer, Having breast cancer results in problems that take a long time. If I get breast cancer, my situation will be much more dangerous than having any other disease.
Subscale (3) perceived benefits concluded (Doing breast self-examination will not make me feel disturbed by breast cancer and make me feel healthy, breast self-examination helps me find a tumor early and prevent my future problem, I have a lot to gain by doing a breast self-examination, eating a healthy diet reduces my chance of getting breast cancer, doing a medical examination will help me find any tumor in the breast and reduce complications).
Subscale (4): perceived barriers of breast cancer (Performing a breast examination by a doctor is an undesirable practice, doing a medical breast examination or mammography is financially expensive. Doing a breast examination by a doctor consumes time. A medical breast examination interferes with my activities. A medical examination of the breast by a doctor is painful.
Subscale (5): Cues to action included adopting healthy eating habits and always following the doctor's instructions because I think it benefits my health. Taking vitamins if I'm not properly fed, Always looking for information that benefits my health, doing regular check-ups, and also going for an examination for any problem.
Subscale (6): self-efficacy of breast cancer If I want to do a breast cancer screening, I think I can solve the difficulties of screening. If I knew that screening had many benefits, even if others objected, I would still do it. It's easy for me to insist on regular breast cancer screening. If I have breast cancer, I think I can effectively deal with the resulting emergency. You follow a healthy diet to reduce the risk of breast cancer.
Scoring system
On a five-point Likert scale, the responses were scored as follows: strongly disagree (1), disagree (2), neutral (3), agree (4), and strongly agree (5), with a total score of 300 degrees. The total attitude score was calculated and divided into three categories:
- Positive belief: for scores of ≥75%. ≥ 225 degrees
- Neutral belief: for scores of 50%–74%. (150-225) degrees
- Negative belief: for scores of <50>
Question numbers (2 and 9) related to susceptibility, the second group related to seriousness (12 questions), and the fourth group related to the barrier (13 questions) had a reversed scoring system of the HBM Likert scale. For the four subscales, higher scores indicate extremely healthy beliefs, but for the subscale concerning barriers and perceived seriousness, higher scores indicate more negative health beliefs.
Statistical Design:
The data was analyzed using SPSS version 20 to compare women's understanding and use of preventive behaviors, using mean, standard deviation, number, and percentage distribution.
Results
Figure (2) shows that 37.8% of females were strongly agreeing regarding the possibility of getting BC will increases her anxiety, regarding the perceived susceptibility of breast cancer.
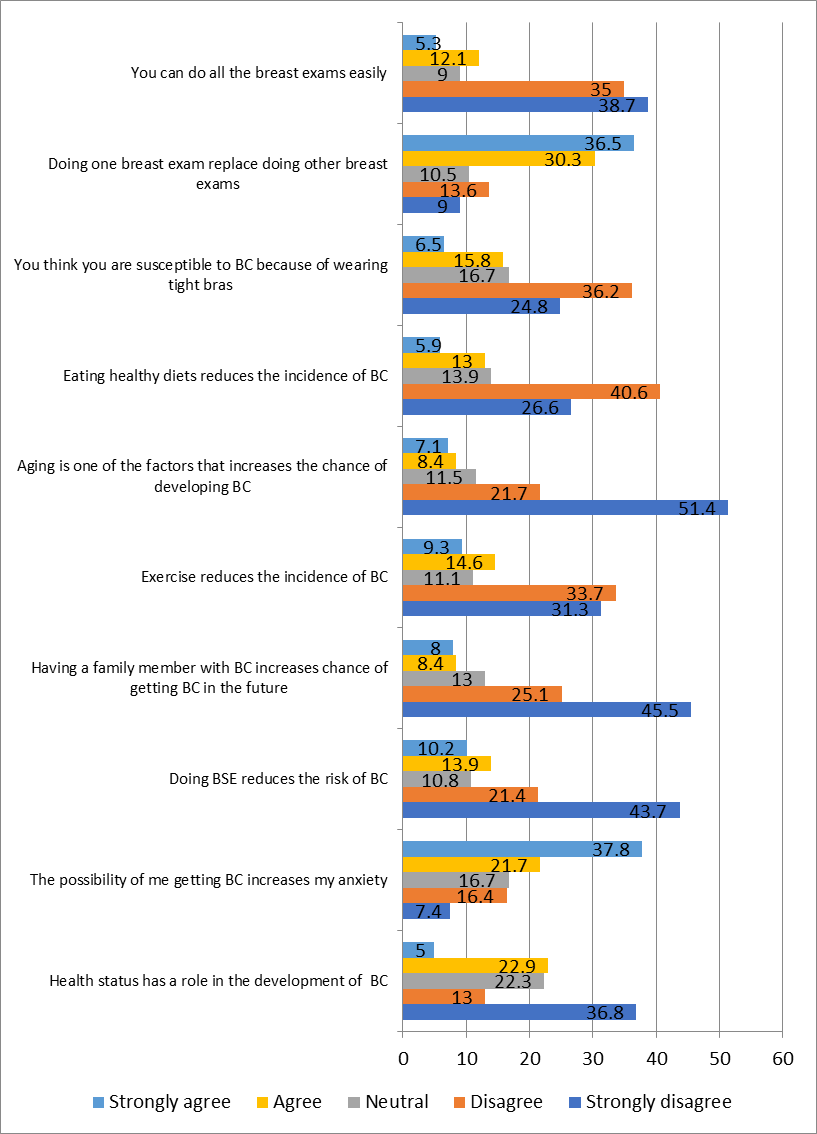
Figure 2: Female workers’ susceptibility beliefs regarding breast cancer and its preventive measures as measured by the health belief model.
Figure (3) shows that 40.6% of females were strongly agreeing regarding thinking about breast cancer scares her and make her feel nauseous, regarding the perceived seriousness of breast cancer.
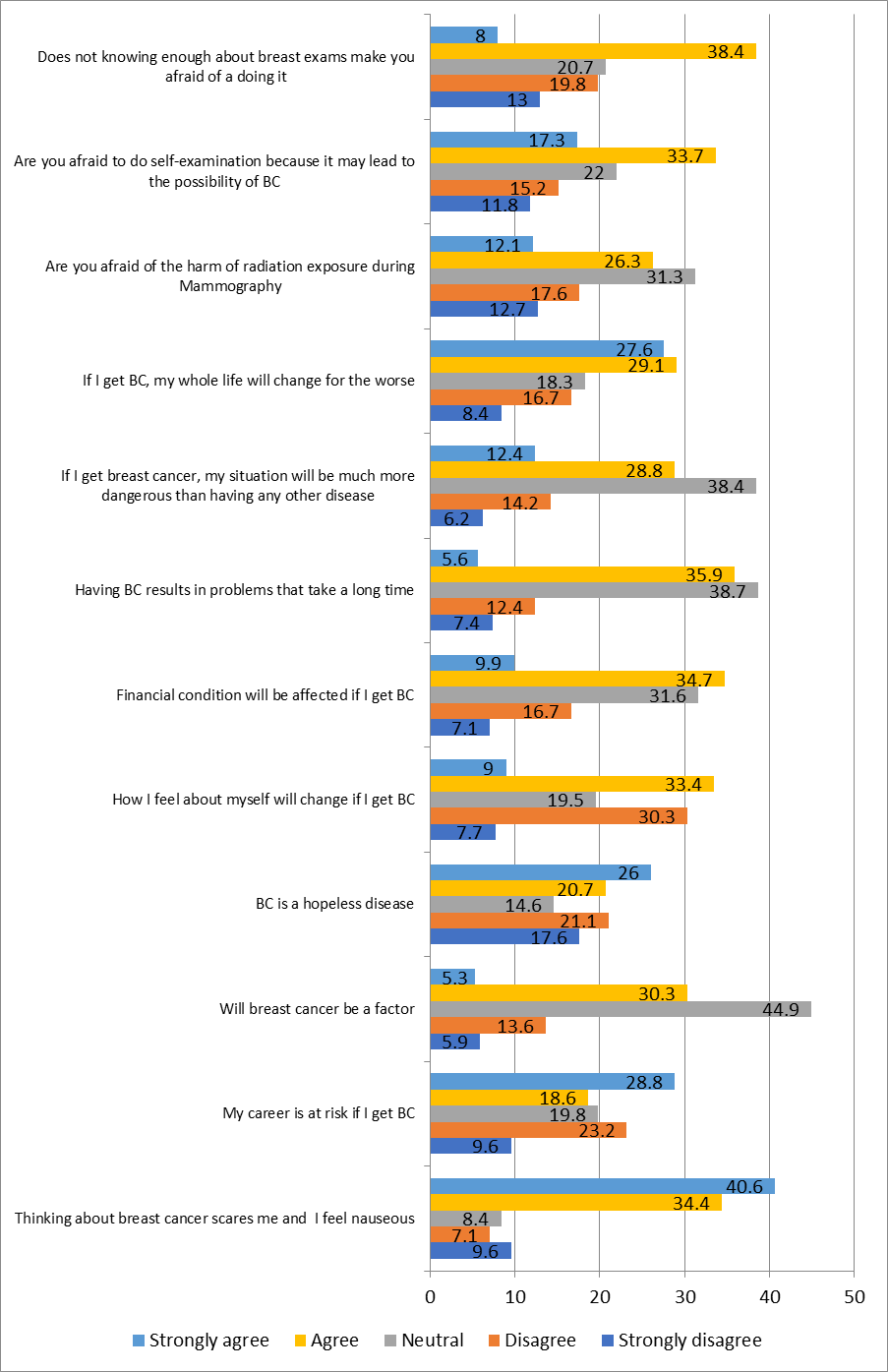
Figure 3: Female workers’ seriousness beliefs regarding breast cancer and its preventive measures as measured by the health belief model
Figure (4) shows that 14.2% of females were strongly agreeing regarding that she have a lot to gain by doing a BSE, regarding the perceived benefits.
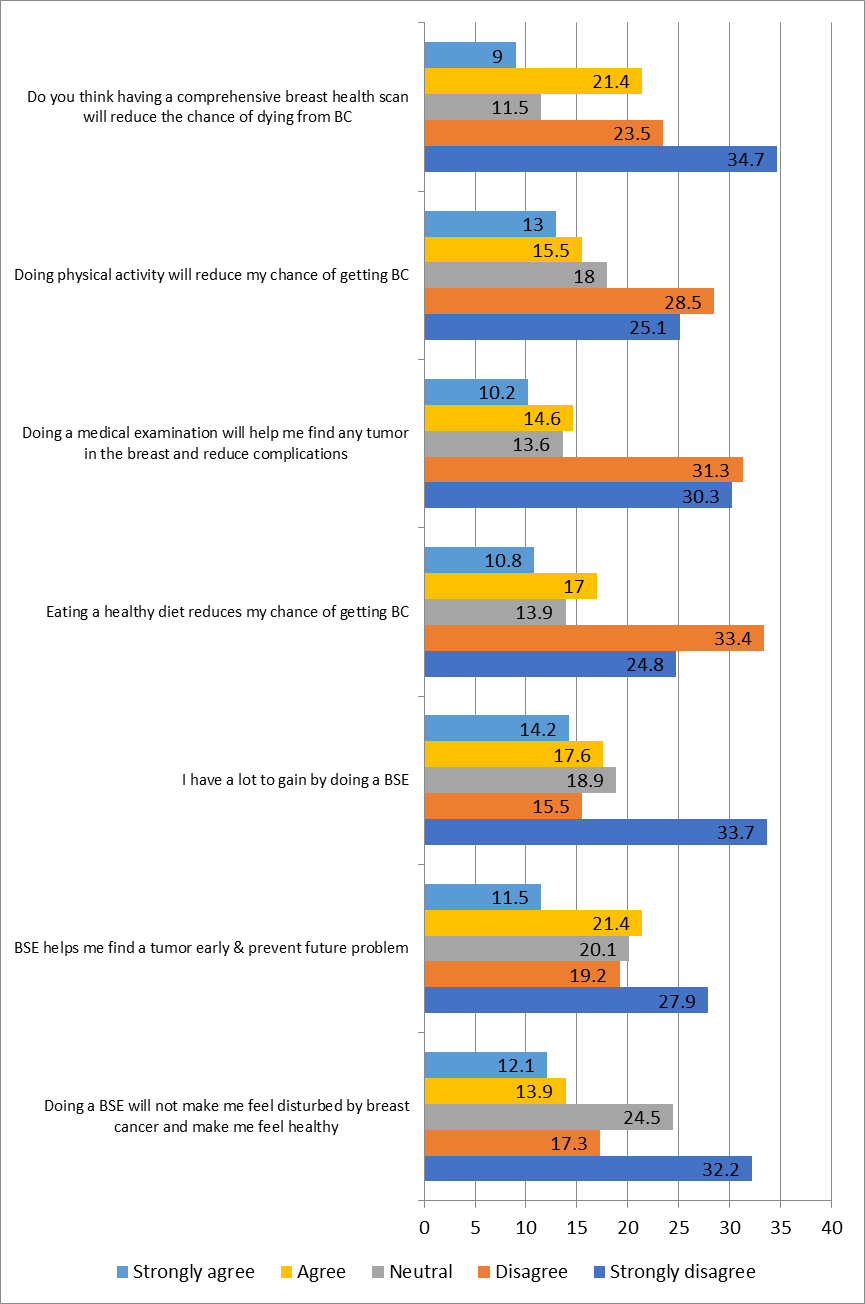
Figure 4: Female workers’ benefits beliefs regarding breast cancer and its preventive measures as measured by the health belief model
(n=323, X2 =10.683, p value = 0.030*)
Figure (5) shows that 17.6% of females were strongly agreeing regarding the medical examination of the breast by doctor is painful, regarding the perceived barriers beliefs regarding breast cancer.
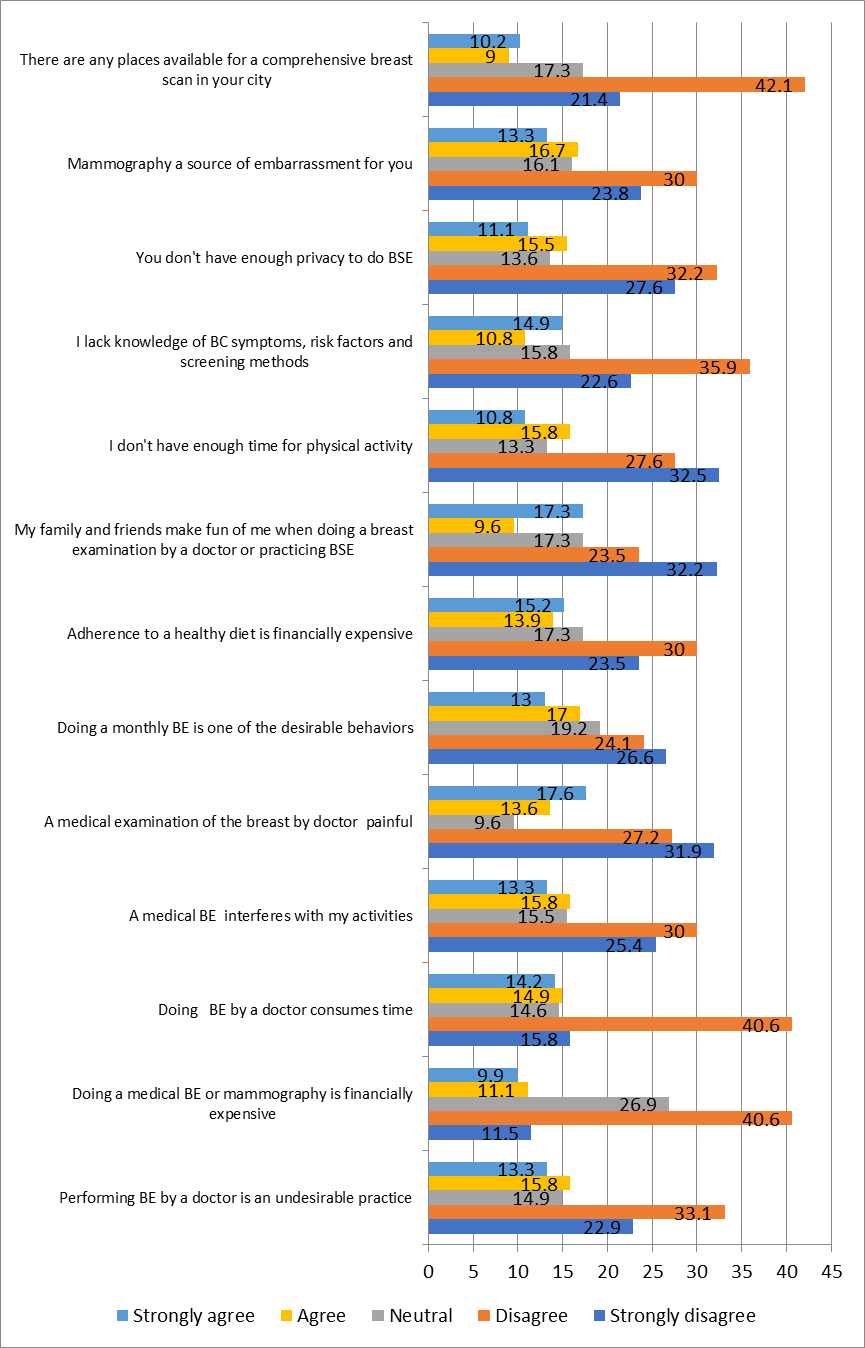
Figure 5: Female workers’ barriers beliefs regarding breast cancer and its preventive measures as measured by the health belief model.
Figure (6) shows that 18% of females were strongly agreeing regarding the importance of doing regular check-ups and also going for an examination for any problem, regarding the perceived cues to action regarding breast cancer.
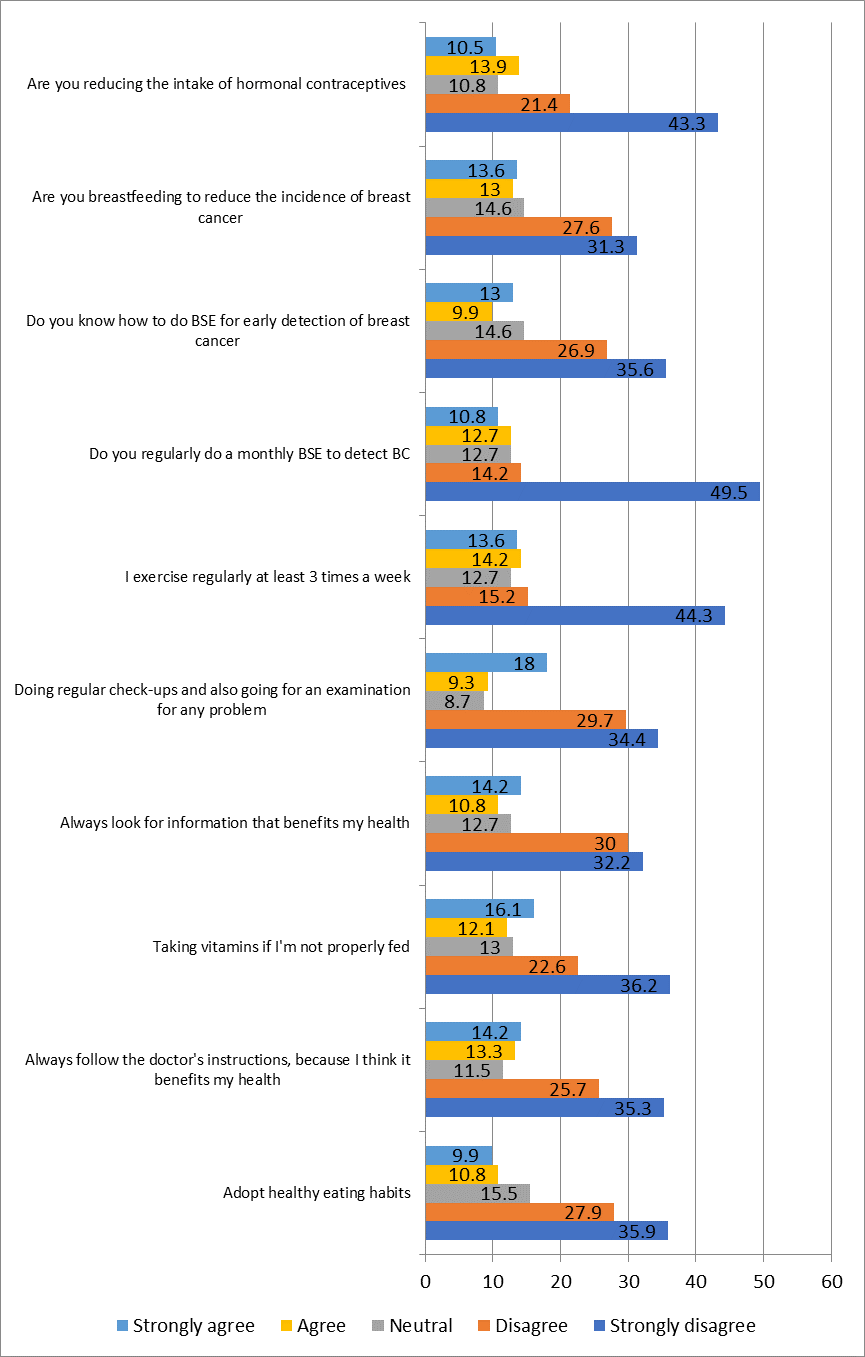
Figure 6: Female workers’ cues to action beliefs regarding breast cancer and its preventive measures as measured by the health belief model
Figure (7) shows that 16.1% of females were strongly agreeing regarding if they knew that screening had many benefits, even if others refused, they would still do it, regarding the perceived self-efficacy beliefs regarding breast cancer.
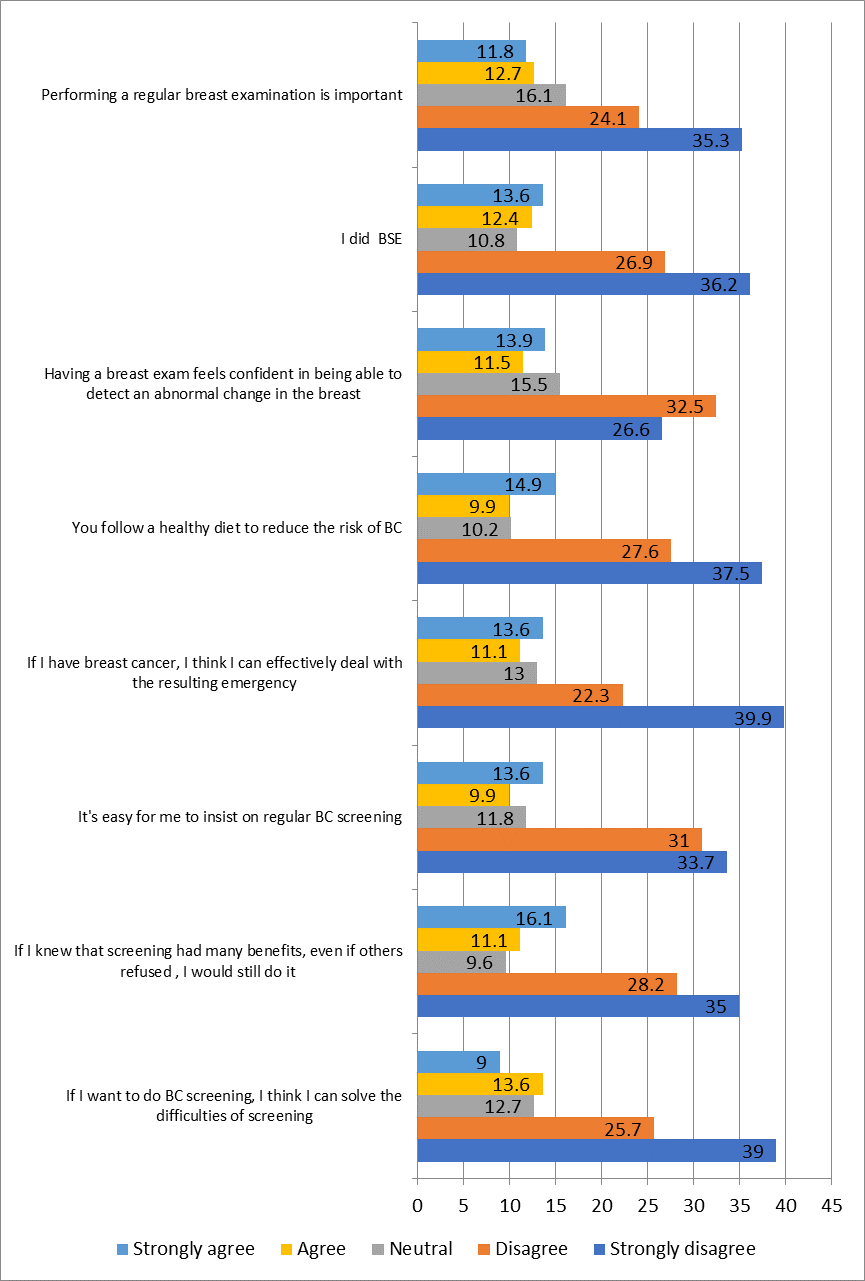
Figure 7: Female workers’ self-efficacy beliefs regarding breast cancer and its preventive measures as measured by the health belief model.
Discussion
The Health Belief model, a theoretical framework addressing disease severity, susceptibility, benefits, and barriers, was expanded in 1988 to include self-efficacy, a person's belief in their ability to act successfully, to better explain individual health behaviors [11-15]. The aim of the study was assess health belief model of breast cancer and its preventive measures among Beni-Suef university female workers.
Concerning female workers’ beliefs regarding breast cancer and its preventive measures as measured by the health belief model, it is discussed under the following headlines.
Firstly, regarding the studied female worker’s perceived susceptibility of breast cancer based on health belief model; the current study indicates progression in perceiving negative susceptibility as aging is one of the factors that increase the chance of developing BC, and having a family member with BC increases chance of getting BC in the future. Wondmu et al. (2022) found a significant difference in perceived susceptibility to breast cancer and breast self-exam using HBM between the intervention and control groups after breast cancer education [35].
Secondly, concerning perceived severity (seriousness) of breast cancer based on health belief model, the current study revealed that there was more than third of the studied women perceived that thinking about breast cancer scares her and she feels nauseous. Ştefănuţ et al. (2023) found significant differences in perceived severity of breast cancer and breast self-examination. Sharing information about the disease's consequences can enhance participants' understanding and motivation to take preventive action [39].
Thirdly, regarding the studied female worker’s perceived benefits of breast cancer based on health belief model, the current study presented that there was a marked progression in positive toward perceived benefits of breast cancer. Presentable percentage denotes that doing breast self-examination will not make her feel disturbed by breast cancer and make hear feel healthy. Elsawy et al. (2023) found significant differences in perceived benefits of breast self-examination and breast self-examination behavior among visually impaired women, possibly due to the health belief model emphasizing early detection and preventive behaviors [40].
Fourthly, in relation to the studied female worker’s perceived barrier of breast cancer based on health belief model, the current study revealed that there was a marked progression toward perceiving the barrier of breast cancer. About one-third of the studied women noted that their family and friends make fun of her when doing a breast examination by a doctor or practicing breast self-examination. El-kest et al. (2021) found significant differences in perceived barriers to breast and cervical cancer among female medical campus employees, possibly due to addressing misconceptions and fears about screening or lifestyle changes [41].
Fifty; regarding the studied female worker’s cues to action breast cancer based on health belief model, the current study revealed that there was about one fifth strongly agree that doing regular check-ups and also going for an examination for any problem toward cues to action of breast cancer. Wondmu et al. (2022) found a significant difference in cues to action regarding breast cancer and self-exam among female students, possibly due to educational materials like brochures, videos, and workshops encouraging screening, health services, and preventive behaviors [35].
Sixthly, concerning self-efficacy breast cancer based on health belief model, the present study illustrated that there was a positive beleif toward self-efficacy regarding BC. Acceptable percent of the studied females strongly agreed that if she knew that screening had many benefits, even if others refused, she would still do it. This finding supported by Mahmoud et al. (2020), who investigated the “effect of the health belief model-based education on preventive behaviors of breast cancer in Benha, Egypt,” and stated that there was a highly significantly increased post-model compared to the scores before model implementation. From the researcher's point of view, this finding may be related to the program often including skills training and resources, boosting participants’ confidence in their ability to perform preventive behaviors, such as self-examination or seeking medical advice [37].
Conclusion
Based on the findings of the present study, it can be concluded most of the studied female workers had negative attitude toward all sub-items of health belief model regarding breast cancer, breast self-examination, and breast cancer preventive measures.
Recommendations
- Implement an educational program based on health belief model to enhance women’s all item of beliefs including susceptibility, seriousness, benefits, barriers, cues to action, and self-efficacy regarding breast cancer and preventive measures.
References
- References
View at Publisher | View at Google Scholar
