

Review Article | DOI: https://doi.org/10.31579/2835-9291/008
Aspergillosis of the Genito-Urinary tract and Kidney Including: The Penis, Scrotum, Testis, Urinary Bladder, Ureter, Renal Pelvis, Vulva, Vagina, Uterus, Fallopian Tubes, the Ovaries, as well as the Kidney: A Review and Update
- Anthony Kodzo-Grey Venyo *
North Manchester General Hospital, Department of Urology, Delaunays Road, Manchester. M8 5RB. United Kingdom.
*Corresponding Author: Anthony Kodzo-Grey Venyo, North Manchester General Hospital, Department of Urology, Delaunays Road, Manchester. M8 5RB. United Kingdom.
Citation: Anthony Kodzo-Grey Venyo, (2023), Aspergillosis of the Genito-Urinary tract and Kidney Including: The Penis, Scrotum, Testis, Urinary Bladder, Ureter, Renal Pelvis, Vulva, Vagina, Uterus, Fallopian Tubes, the Ovaries, as well as the Kidney: A Review and Update., International Journal of Clinical Case Studies,2(3); DOI:10.31579/2835-9291/008
Copyright: © 2023, Anthony Kodzo-Grey Venyo. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 23 May 2023 | Accepted: 13 June 2023 | Published: 29 June 2023
Keywords: aspergillosis; kidney; urogenital tract; renal pelvis; urinary bladder; penis; prostate; seminal vesicle; fallopian tube; ovary antifungal treatment; surgical excision; renal transplant recipient; immunosuppression
Abstract
Aspergillosis is a fungal infection that can afflict various organs of the body. Aspergillosis on rare occasions can afflict the kidney and urogenital tract of human beings. Aspergillosis of the kidney and the female and male urogenital tract does manifest with non-specific symptoms that simulate the symptoms of common bacterial infections and diseases of the kidney and because of this there tends to be delay in the diagnosis of some cases of aspergillosis of the kidney and urogenital tract or the case could easily be misdiagnosed. Aspergillosis of the kidney and urogenital tract in human beings tend to affect individuals who have predisposing factors including transplant recipients and individuals who have depression of their immune systems as well as other factors listed in the article. Some of the presentations of aspergillosis involving the kidney and the urogenital system include:
- Kidney (a) incidental diagnosis in an asymptomatic individual based upon radiology imaging undertaken for something else. (b) loin pain, fever, hematuria, weight loss, felling unwell, hematuria.
- Ureter and Renal Pelvis – loin to groin pain that tends to simulate ureteric colic, fever, hematuria, passing flakes of material in urine, feeling unwell and other symptoms and at times a history of immunosuppression including transplantation of an organ
- Urinary bladder: Lower urinary tract symptoms, hematuria, passing flaky fleshy material in urine, retention of urine as well as loin pain if the lesion is obstructing the ureteric orifice.
- Prostate and seminal vesicle: Lower urinary tract symptoms, dysuria, fever, hematuria, retention of urine, weight loss and feeling unwell.
- Testis and epididymis: testicular pain, fever, feeling unwell, weight loss.
- Penis: lesion on penis, mass on penis, ulcer of penis, bleeding from penis, sloughy material on penis, feeling unwell.
- Vulva: lesion or mass on vulva, bleeding from vulva, ulcer from vulva, discharge from vulva.
- Vagina: Bleeding from vagina, ulcer in vagina, slough from vagina.
- Cervix: Bleeding from vagina, slough and discharge from vagina, lower abdominal and suprapubic pain / discomfort.
- Uterus: Bleeding from the vagina, lower abdominal and suprapubic discomfort and pain, discharge from vagina as well as slough.
- Fallopian tube: lower abdominal and suprapubic pain simulating pelvic inflammatory disease and acute abdomen, fever and feeling unwell plus weight loss.
- Ovary: Lower abdominal and suprapubic pain, simulating pelvic inflammatory disease or fallopian tube-ovarian mass or abscess
Diagnosis of the infection tends to be made based upon culture of Aspergillus from the lesion and upon pathology examination of a swab of the lesion or the excised lesion. Radiology imaging including ultrasound scan, computed tomography scan, and magnetic resonance imaging scan tend to be undertaken to ascertain the extent of the lesion. A history of previous treatment for aspergillosis as well as a history of immunosuppression or other predisposing factors tend to obtained in the history. When a patient has undergone antibiotic treatment for a presumed bacterial infection of the kidney and the urogenital infection without any response then clinicians need to have a high index of suspicion to suspect the possibility of Aspergillosis.
Treatment of the lesion does entail utilization of an appropriate antifungal agent that the Aspergillus species is susceptible to in addition to excision of the lesion to remove the source of the lesion. Because there could be recurrence of the lesion a long-period of methodical follow-up is required.
Introduction
It has been stated that invasive aspergillosis, which is a severe fungal infection, usually tends to affect patients who have immunocompromising conditions such as diabetes mellitus, hematological malignancy and neutropenia [1,2]. It has also been pointed out that Aspergillosis that is limited to the urinary tract is an uncommon type of invasive aspergillosis, which had been reported to more frequently involve the lung [1].
It has additionally been iterated that invasive fungal infection of urinary tract, which is more commonly found in immunocompromised patients, does remain a great challenge with regards to both its clinical diagnosis and its treatment [1]. It has been explained that there are three main routes of transmission of aspergillosis, with the inclusion of ascending infections which most often has tended to be from indwelling urinary bladder catheters, trauma or surgical interventions and hematogenous spread, has tended to be common in immunocompromised patients. It has been pointed out that Candida is the commonest fungal pathogen causing urinary tract infection which is followed Aspergillus [1,2]. Aspergillosis infection on rare occasions can affect various organs of the body, including the penis, scrotum, testis and intra-scrotal organs, urinary bladder, renal pelvis or the kidney. Aspergillosis can also affect the vulva [3,4], vagina and cervix [5,6], uterus, fallopian tube [7], and ovary. Aspergillosis could be superficial or invasive. Aspergillosis of the kidney and genitourinary tract does manifest with non-specific symptoms and hence its diagnosis may be missed initially or there may be some delay in the diagnosis. Because of the rarity of aspergillosis of the kidney and the genitourinary tract, majority of clinicians globally may not be familiar with the manifestations, diagnostic features, treatment and outcome following treatment of the various organs of the body. The ensuing article on aspergillosis of the kidney and the urogenital tract is divided into two parts: (A) Overview, and (B) Miscellaneous Narrations and Discussions Related to Aspergillosis of the kidney and the genitourinary tract.
Methods:
Various internet data bases were searched including: Google; Google Scholar; Yahoo; and PUBMED. The search words that were used included: Aspergillosis of penis; Aspergillosis of Scrotum; Aspergillosis of testis; Aspergillosis of bladder; Aspergillosis of ureter; Aspergillosis of renal pelvis; Aspergillosis of vulva; Aspergillosis of vagina; Aspergillosis of cervix; Aspergillosis of uterus, Aspergillosis of fallopian tube; and Aspergillosis of ovary. One hundred and fifty-four (154) references were identified which were used to write the article on aspergillosis of the kidney and the urogenital tract is divided into two parts: (A) Overview, and (B) Miscellaneous Narrations and Discussions Related to Aspergillosis of the kidney and the genitourinary tract.
Results:
[A] Overview
General Statements:
- Aspergillus is a terminology that is utilized for a genus which consists of several hundred mould species that are found in various climates globally [8].
- It has been iterated that Aspergillus was first catalogued in 1729 by an Italian priest and biologist called Pier Antonio Micheli. Viewing the fungi under a microscope, Micheli was documented to be have been reminded of the shape of an aspergillum (holy water sprinkler), from Latin spargere (to sprinkle), and as well as that Michelli named the genus accordingly [8] [9].
- Aspergillum is stated to be an asexual spore-forming structure which is common to all Aspergillus species; as well as it has been documented that about one-third of species are also known to have a sexual stage [9].
- It has been documented that whilst some species of Aspergillus are known to cause fungal infections, other species of aspergillus are of commercial importance. [8]
- Aspergillosis is a terminology that is utilized for a fungal infection which usually tends to afflict the lungs [8] [10], which is caused by the genus Aspergillus, which is a common mould which has tended to be breathed in frequently from the air around, but which has been stated not to usually affect majority of people. [1] [8] [11].
- Aspergillosis is stated to generally afflict individuals who have a number of lung diseases including asthma, cystic fibrosis, or mycobacteria tuberculosis, or individuals who have had stem cell or organ implant surgery, as well as individuals who are not capable of fighting infection in view of the medicaments, they take including steroids as well as treatments for malignant tumors [10] [12].
- It has additionally been iterated that aspergillosis could affect the skin [12] [13].
- It has been pointed out that Aspergillosis does tend to afflict human beings, birds and other animals [8] .
- It has been iterated that Aspergillosis does tend to occur in chronic or acute forms which have been documented to be clinically very distinct [8].
- It has been pointed out that majority of cases of acute aspergillosis have tended to afflict people who have severely compromised immune systems, including individuals who have been undergoing bone marrow transplantation [14].
- It has been documented that chronic colonization or infection by aspergillosis could emanate in complications in people who have been afflicted by underlying respiratory illnesses, including: asthma [8] [15],cystic fibrosis, [16] sarcoidosis [8], [17], tuberculosis infection, or chronic obstructive pulmonary disease [18].
- It has also been iterated that most often, aspergillosis does tend to occur in the form of chronic pulmonary aspergillosis (CPA), aspergilloma, or allergic bronchopulmonary aspergillosis (ABPA) [8] [19] .
- Some forms of pulmonary aspergillosis have been documented to be intertwined; for example, ABPA and simple aspergilloma could emanate into the development into CPA [8] .
- It has been pointed out that other, non-invasive manifestations of aspergillosis do include: fungal sinusitis which could both be allergic in nature and also with established fungal balls, ear infection that is referred to as otomycosis, eye infection that is referred to as aspergillosis keratitis, nail infection that is referred to as onychomycosis. [8]. However, it has been pointed out that most often, these aspergillosis infections tend to be less severe, and curable following treatment with effective antifungal medicaments. [8] It has been pointed out thar the most commonly Aspergillus pathogens that tend to be encountered include Aspergillus fumigatus, and Aspergillus flavus which are ubiquitous organisms that have the capability of living under extensive environmental stress [8].
- It has been documented that majority of individuals who are afflicted by Aspergillosis, have been postulated to have inhaled thousands of Aspergillus spores daily but without effect due to an efficient immune response [8] .It has furthermore, been stated that taken together, the major chronic, invasive, and allergic forms of aspergillosis do account for about 600,000 deaths annually globally. [15, 20-23].
- It is worth noting that Aspergillosis, though rare, can afflict various organs of the body including the penis, scrotum, testis, prostate, kidney and the urinary tract including the urinary bladder, vulva, vagina, uterus, fallopian, tubes, ovaries as well as various other organs of the body.
Growth and Distribution:
- Aspergillus has been defined as a group of conidal fungi which refers to fungi that are in an asexual state. Some of the fungi are stated to be known however, to have a telemorph or sexual state in the Ascomycota. Aspergillus has been stated to have DNA evidence, all members of the genus Aspergillus are stated to be members of the phylum Ascomycota [8].
- It has been iterated that members of the genus possess the ability to grow whereby a high osmotic pressure does exist with high concentration of sugar, salt, and others. [8] Aspergillus species had also been stated to be highly aerobic and they tend to be found in almost all oxygen-rich environments, where they do commonly grow as moulds upon the surface of a substrate, as an emanation of the high oxygen tension [8].
- It had been pointed out that fungi grow commonly upon carbon-rich substrates like monosaccharides including monosaccharides such as glucose as well as polysaccharides such as amylose [8].
- It has been iterated that Aspergillus species tends to be found as common contaminants of starchy foods including bread and potatoes, and they tend to grow in or upon many plants and trees [8].
- It has furthermore been stated that in addition to growth upon carbon sources, many species of Aspergillus do tend to demonstrate oligotrophy, whereby they are capable of growing within nutrient-depleted environments, or environments that have a complete lack of key nutrients [8].
- It has been explained that Aspergillus niger constitutes a a prime example of this; in that it could be found growing upon damp walls, as a major component of mildew. [8]
- Several species of Aspergillus, including A. niger and Aspergillus fumigatus, would readily colonise buildings [4], favouring warm and damp or humid areas such as bathrooms and around window frames [5].
Aspergillus tends to be found in millions of pillows.[6]
- Commercial Importance of Aspergillus
- It has been iterated that Species of Aspergillus are important medically as well as commercially [8] .
- It has also been stated that some species of Aspergillus could cause infection in human beings as well as in other animals [8].
- It has been iterated that some infections that are found in animals had been studied for many years, while other species that are found in animals had been described as new and specific to the investigated disease, and others had been known as names already in use for organisms such as saprophytes [8].
- It has been documented that more than 60 Aspergillus species constitute medically relevant pathogens [8] [24].
- It has been documented that with regard to human beings, a range of diseases such as infection to the external ear, skin lesions, and ulcers classed as mycetomas tend to be found [8].
- It has also been pointed out that other Aspergillus species are important in commercial microbial fermentations [8]. For example, alcoholic beverages such as Japanese sake often tend to be made from rice or other starchy ingredients (like manioc), rather than from grapes or malted barley [8].
- It has additionally, been stated that typical microorganisms that are utilized to make alcohol, such as yeasts of the genus Saccharomyces, cannot ferment these starches. [8] Therefore, koji mold such as Aspergillus oryzae is utilized to first break down the starches into simpler sugars [8] [25], to make soy sauce, first you add aspergillus mold to the soy beans and grains to produce a mixture called koji.
- Members of the genus are said also to be sources of natural products which could be utilised in the development of medicaments so as to treat human disease.[8] [26].
- It has been iterated that Aspergillus spp. are known for the production of anthraquinone which has commercial importance in view of its antibacterial and antifungal properties[8] [27].
- It has been iterated that perhaps the largest application of Aspergillus niger constitutes the major source of citric acid; this organism accounts for over 99% of global citric acid production, or more than 1.4 million tonnes (>1.5 million US tons) per year [8].
- A. niger is also commonly utilized for the production of native and foreign enzymes, with the inclusion of: glucose, oxidase, lysozyme, as well as lactase [8] [28].
- It has been pointed out that in these instances, the culture tends to be rarely grown upon a solid substrate, even though this is still common practice in Japan; nevertheless, it is more often grown as a submerged culture in a bioreactor. [8]. In this way, the most important parameters could be strictly controlled, as well as maximal productivity could be achieved. [8] It has additionally been stated that this process also does make it far easier to separate the chemical or enzyme of importance from the medium, and hence it is therefore far more cost-effective [8].
Research:
The ensuing summations had been made regarding utilization of Aspergillus in research projects: [8]
- Aspergillus nidulans (Emericella nidulans) had been utilized as a research organism for many years and it was utilized by Guido Pontecorvo in order to demonstrate parasexuality in fungi [8].
- It has been pointed out that recently, Aspergillus nidulans was one of the pioneering organisms to have its genome sequenced by researchers at the Broad Institute [8].
- It has been documented that as of 2008, a further seven Aspergillus species had had their genomes sequenced: the industrially useful A. niger (two strains), Aspergillus oryzae, and Aspergillus terreus, as well as the pathogens Aspergillus clavatus, Aspergillus fischerianus (Neosartorya fischeri), Aspergillus flavus, as well as Aspergillus fumigatus (two strains) [8] [29].
- It has been pointed out that Aspergillus fischerianus has hardly ever been pathogenic; however, it is very closely related to the common pathogen Aspergillus. fumigatus; it was sequenced in part to better understand A. fumigatus pathogenicity.[8] [30]
- Sexual Reproduction
- It has been documented that out of the 250 species of aspergilli, about 64% do not have any known sexual state. [8] [31]. Nevertheless; it has been pointed out that many of these species likely have an as yet unidentified sexual stage. [8] and that sexual reproduction does occur in two fundamentally different ways in fungi. These are outcrossing (in heterothallic fungi) in which two different individuals do contribute nuclei, and self-fertilization or selfing (in homothallic fungi) in which both nuclei are derived from the same individual [8].
- It has also been iterated that in recent years, sexual cycles had been discovered in many species which were previously considered to be asexual and that these discoveries do reflect recent experimental focus on species of particular relevance to humans. [8]
- Aspergillus fumigatus is known to be the commonest species to cause disease in immunodeficient human beings [8].
- In 2009, Aspergillus fumigatus had been known to have a heterothallic, fully functional sexual cycle [8] [32].
- It has furthermore been iterated that isolates of complementary mating types are required for sex to occur [8] .
- It has been pointed out that Aspergillus flavus is the major producer of carcinogenic aflatoxins in crops globally [8].
- It has also been stated that Aspergillus is also an opportunistic human and animal pathogen, which causes aspergillosis in immunocompromised individuals. [8]
- It has been documented that in 2009, a sexual state of this heterothallic fungus was found to arise when strains of opposite mating types of Aspergilli were cultured together under appropriate conditions [8] [33].
- It has been iterated that Aspergillus lentulus constitutes an opportunistic human pathogen which causes invasive aspergillosis that is associated with high mortality rates [8].
- It was stated that in 2013, Aspergillus. lentulus was found to have a heterothallic functional sexual breeding system. [8] [34].
- It has been stated that Aspergillus. terreus is commonly utilized in industry to produce important organic acids and enzymes, and Aspergillus terreus was the initial source for the cholesterol-lowering drug lovastatin [8].
- It was stated that in 2013, Aspergillus. terreus was found to be capable of sexual reproduction when strains of opposite mating types were crossed under appropriate culture conditions. [8] [35].
- It has been iterated that these findings with Aspergillus species are consistent with accumulating evidence, from studies related to other eukaryotic species, that sex was likely to be present in the common ancestor of all eukaryotes. [8] [36] [37]
- It has been documented that Aspergillus nidulans, which is a homothallic fungus, is capable of self-fertilization. [8]
- It has also been iterated that selfing does entail activation of the same mating pathways that are characteristic of sex in outcrossing species, for example self-fertilization does not bypass the required pathways for outcrossing sex, however. it instead requires activation of these pathways within a single individual. [8] [38]
- It has been stated that among those Aspergillus species which do depict a sexual cycle, the overwhelming majority in nature are homothallic (self-fertilizing). [39]
- It has been explained that this observation does indicate that Aspergillus species could generally maintain sex though little genetic variability tends to be produced by homothallic self-fertilization. [8]
- It has been pointed out that Aspergillus fumigatus, which is a heterothallic (outcrossing) fungus which occurs in areas that have widely different climates and environments, also does display little genetic variability either within geographic regions or on a world-wide scale, [8] [40] again indicating sex, in this case outcrossing sex, could be maintained even when little genetic variability has been produced.
Genomics:
- It has been pointed out that the simultaneous publication of three Aspergillus genome manuscripts in Nature in December 2005, had established the genus as the leading filamentous fungal genus for comparative genomic studies. [8]
- It has also been stated that like majority of major genome projects, these efforts had been collaborations between a large sequencing centre and the respective community of scientists. For example, the Institute for Genome Research (TIGR) had worked with the Aspergillus. fumigatus community. Aspergillus. nidulans had been sequenced at the Broad Institute. Aspergillus. oryzae had been sequenced in Japan within the National Institute of Advanced Industrial Science and Technology. The Joint Genome Institute of the Department of Energy had released sequence data for a citric acid-producing strain of Aspergillus. niger. TIGR, which has now been renamed the J. Craig Venter Institute, was at the time of publication spearheading a project on the Aspergillus flavus genome. [8] [41]
- It has been documented that Aspergillus is typified by high levels of genetic diversity and, utilizing protostome divergence as a scale, Aspergillosis is as diverse as the Vertebrates phylum even though both inter and intra-specific genome structure is relatively plastic. [8] [42]
- It has also been stated that the genomes of some Aspergillus species, such as Aspergillus flavus as well as Aspergillus. oryzae, are more-rich and around 20% larger in comparison with others, such as A. nidulans and A. fumigatus. [8]
- It has been explained that many mechanisms could explain this difference, even though the combination of segmental duplication, genome duplication, and horizontal gene transfer acting in a piecemeal fashion had been well-supported. [8] [43]
- It has been explained and pointed out that Genome sizes for sequenced species of Aspergillus do range from about 29.3 Mb for Aspergillus. fumigatus to 37.1 Mb for Aspergillus. oryzae, whilst the numbers of predicted genes vary from about 9926 for Aspergillus. fumigatus to about 12,071 for A. oryzae. The genome size of an enzyme-producing strain of Aspergillus. niger had been noted to be of intermediate size at 33.9 Mb. [8] [44]
Pathogens:
- It has been explained that some Aspergillus species tend to cause serious disease in human beings and animals, and that the commonest pathogenic species are Aspergillus fumigatus and Aspergillus flavus, which produces aflatoxin that is both a toxin and a carcinogen, and which could contaminate foods such as nuts. [8]
- It has been documented that the most common Aspergillus species causing allergic disease are Aspergillus fumigatus and Aspergillus clavatus [8].
- It has been pointed out that other species of Aspergillus are important as agricultural pathogens. [8]
- It has been iterated that Aspergillus spp. does cause disease on many grain crops, especially maize, and some variants do synthesize mycotoxins, with the inclusion of aflatoxin. [8]
- It has additionally been stated that Aspergillus could cause neonatal infections. [8] [45].
- It has been pointed out that Aspergillus. Fumigatus, which is the most common species, infections tend to be primary pulmonary infections and they could potentially become a rapidly necrotizing pneumonia with a potential to disseminate. [8]
- It has additionally been iterated that the organism could be differentiated from other common mold infections based upon the fact that it does take on a mold form both in the environment and in the host, unlike Candida albicans, which is a dimorphic mold within the environment and a yeast within the body. [8]
Aspergillosis:
- It has been stated that Aspergillosis is a terminology that is utilized for a group of diseases that are caused by Aspergillus species. [8]
- It has also been stated that the commonest Aspergillus species among paranasal sinus infections that are associated with aspergillosis is Aspergillus fumigatus. [8] [46]
- The symptoms of Aspergillosis had been documented to include fever, cough, chest pain, or breathlessness, which also tend to be the symptoms associated with many other illnesses, so the diagnosis of Aspergillosis could be difficult. [8]
- It has been pointed out that often, only patients who have already weakened immune systems or those patients who suffer other lung conditions tend to be susceptible to Aspergillosis. [8]
- Some authors had iterated that with regard to human beings, the major forms of Aspergillosis disease do include; [8] [47] [48]
- It has been explained that acute invasive aspergillosis, is a form which does grow into surrounding tissue, more common in those who have weakened immune systems such as AIDS or chemotherapy patients. [8]
- It has been pointed out that allergic bronchopulmonary aspergillosis, does tend to affect patients who have respiratory diseases such as asthma, cystic fibrosis, as well as sinusitis. [8]
- It has been explained that aspergilloma is a "fungus ball" which could form within cavities such as the lung. [8]
- Disseminated invasive aspergillosis, which is an infection that is spread widely through the body. [8]
- It has been iterated that fungal infections from Aspergillus spores do remain one theory or postulate of sickness and untimely leading to death of some early Egyptologists and tomb explorers. [8]
- It has been stated that ancient spores which grew upon the remains of food offerings and mummies that had been sealed within tombs and chambers could have been blown around and inhaled by the excavators, which had been ultimately linked to the notion of the curse of the pharaohs. [8] [49]
- It has been pointed out that Aspergillosis of the air passages had also been frequently reported in birds, and certain species of Aspergillus had been known to infect insects. [8] [24]
- It had also been pointed out that majority of people do inhale Aspergillus into their lungs every day. [8] [50]. Nevertheless, it has been explained that it is generally only the immune-compromised individuals who get sick with Aspergillosis. [8] [50].
Epidemiology:
- It has been stated that: Aspergillosis, has been iterated to affect more than 14 million individuals globally, [8] [51], with allergic bronchopulmonary aspergillosis (ABPA, >4 million), severe asthma with fungal sensitization (>6.5 million), and chronic pulmonary aspergillosis (CPA, ~3 million) being found to be considerably more prevalent in comparison with invasive aspergillosis (IA, >300,000).
- Other documented common Aspergillosis conditions have been documented to include Aspergillus bronchitis, Aspergillus rhinosinusitis which tends to afflict many millions of individuals, otitis externa, as well as Aspergillus onychomycosis which has been stated to affect 10 million individuals globally. [8] [52] [53]
- It has been suggested that alterations in the composition of and function of the lung microbiome as well as mycobiome had been documented be associated with an increasing number of chronic pulmonary diseases such as COPD, cystic fibrosis, chronic rhinosinusitis and asthma. [54].
Risk Factors:
Presentation:
- The manifestations of Aspergillosis of various organs of the kidney and genitourinary system have all been non-specific and therefore a high index of suspicion is required from all clinicians because the symptoms always simulate symptoms of more common diseases of the kidney and the urogenital system organs.
- In some cases of recurrence of Aspergillosis of the kidney and the urogenital tract a history of previous treatment for Aspergillosis of an organ short alert all clinicians to the likelihood of Aspergillosis recurrence affecting organs including the kidney and urogenital symptoms.
- Penis – some of the symptoms including aggravating skin eruptions and ulceration as well as discharge and bleeding from the penis which are non-specific symptoms that tend to be the manifesting symptoms or more common lesions of the penis and clinicians need to be aware that they need to have a high index of suspicion of aspergillosis of the penis in patients present with these types symptoms in order not to have a delay in diagnosing the disease or misdiagnosing the lesion.
- Prostate – individuals who have aspergillosis of the penis would tend to manifest with lower urinary tract symptoms (LUTS), urinary retention and at times fever and in view of the rarity of aspergillosis of the prostate gland, unless a clinician is aware of the fact that aspergillosis of the penis though rare, could present with symptoms that simulate the symptoms of benign prostatic hyperplasia (BPH), carcinoma of the prostate, and acute / chronic bacterial prostatitis there could be a delay in the diagnosis of the infection or the case could be misdiagnosed initially.
- Testis and seminal vesicle – An individual who has aspergillosis of the testis and epididymis would tend to manifest with fever, pain and swelling within the testis and feeling unwell and these symptoms do simulate the symptoms of acute or chronic bacterial epididymoorchitis and this would generally to lead to delay of the correct diagnosis of the infection or the diagnosis could initially be considered to be that of acute bacterial epididymoorchitis or chronic bacterial epididymoorchtis including tuberculous epididymorchitis. A history of predisposing conditions including, the patient having undergone renal transplant transplantation or any organ transplantation with immunosuppression of combination chemotherapy for some other malignancy, or a history of having undergone previously treatment for disseminated aspergillosis in the recent past should alert the clinician to have a high index of suspicion to include aspergillosis of the testis and epididymis as a differential diagnosis.
- Urinary bladder – An individual who has aspergillosis of the urinary bladder, depending upon the area of urinary bladder affected would tend to manifest with non-specific symptoms including: lower urinary tracts symptoms (LUTS) such as urinary frequency, urgency, urge incontinence, dysuria, supra-pubic pain, loin pain, discharge of fleshy material within the urine, visible hematuria, and loin pain as well as fever on some occasions or the patient could be admitted because of retention of urine. A history of having been recently treated for disseminated aspergillosis, or aspergillosis, elsewhere should alert the clinician to the possible diagnosis of a rare case of aspergillosis of the urinary bladder, especially if the individual has predisposing factors as discussed later on in the article.
- Ureter and renal pelvis – An individual who has aspergillosis of the ureter and renal pelvis including aspergillosis of the urinary bladder involving the ureteric orifice may present with fever, intermittent colicky loin to groin pain that simulates an upper urinary tract ureteric colic, fever, passage of blood within the urine as well as passage of fleshy material within the urine. Most often clinicians would tend to make a provisional diagnosis of ureteric colic and radiology imaging to depict the lesion which would quite often be provisionally diagnosed as a calculus. A history of previous endoscopy procedure of the ipsilateral ureter and renal pelvis with uretero-renoscopy plus insertion of a ureteric stent, or a previous history of treatment for disseminated aspergillosis as well as predisposing factors and passage of fleshy material within the urine should alert the clinician to suspect the possibility of aspergillosis of the ipsilateral upper urinary tract manifesting in a way that simulates ureteric colic.
- Kidney – An individual who has aspergillosis of the kidney may or may not have a history of previous treatment for disseminated aspergillosis, or aspergillosis of a single organ or no previous treatment for aspergillosis. Aspergillosis of a kidney could be diagnosed in an asymptomatic individual who undergoes radiology imaging including ultrasound scan of abdomen and renal tract, computed tomography (CT) scan of abdomen and pelvis / renal tract, magnetic resonance imaging (MRI) scan of abdomen / renal tract that was undertaken as part of radiology imaging for something else and the kidney lesion could then be incidentally found, or the individual could manifest with feeling unwell, having fever, weight loss, loin pain, visible hematuria, or passing fleshy material within the urine. These symptoms are non-specific and a high index of suspicion would be required to include aspergillosis of the kidney as a differential diagnosis whilst undertaking investigations to establish a definite diagnosis.
- Vulva and vagina – An individual who has aspergillosis of the vulva may present with a lesion upon the vulva or within the vagina, an ulceration on the vulva, bleeding from the vulva, sloughing from the vulva in addition to fever and sensation of being unwell or weight loss and a feeling of being not well. These symptoms are non-specific and a high index of suspicion would be required to establish a quick diagnosis of aspergillosis of the vulva and
- Cervix – An individual who has aspergillosis of the cervix could present with bleeding from the vagina, finding she has a lesion / mass within the deeper part of her vagina, passing flakes of tissue from her vagina, being unwell, having weight loss, having suprapubic discomfort, or the finding of abnormality in cytology / pathology examination of the individual’s cervical smear cytology examination. These manifestations are non-specific and a high index of suspicion is required to establish the diagnosis.
- Uterus - An individual who has aspergillosis of the uterus could present with bleeding from the vagina, passing flakes of tissue from her vagina, being unwell, having weight loss, having suprapubic discomfort. These manifestations are non-specific and a high index of suspicion is required to establish the diagnosis.
- Fallopian tube – An individual who has aspergillosis of the fallopian tube may present with acute or chronic pain in her suprapubic / pelvis region and this may not be associated with bleeding per vagina, or discharge from her vagina and would be found to be tender within her suprapubic region, mimicking pelvic inflammatory disease. There could also be the possibility of bleeding per vagina of passing flakes of tissue from the vagina. These symptoms are non-specific and unless a history of previous treatment elsewhere for disseminated aspergillosis or aspergillosis of a single organ or the patient having predisposing conditions and not responding well to adequate antibiotic treatment should enable the clinician have a high index of suspicion for aspergillosis of the fallopian tube. At times the diagnosis would tend to be made when a laparotomy or laparoscopy is undertaken for an acute lower abdominal pain for sepsis, tube-ovarian mass or possibly ectopic pregnancy or when the patient has not responded to appropriate antibiotic treatment for a provisionally diagnosed pelvis inflammatory disease (PID)/pelvis abscess.
- Ovary - An individual who has aspergillosis of the ovary may present with acute or chronic pain in her suprapubic / pelvis region and this may not be associated with bleeding per vagina, or discharge from her vagina and would be found to be tender within her suprapubic region, mimicking pelvic inflammatory disease. These symptoms are non-specific and unless a history of previous treatment elsewhere for disseminated aspergillosis or aspergillosis of a single organ or the patient having predisposing conditions and not responding well to adequate antibiotic treatment should enable the clinician have a high index of suspicion for aspergillosis of the fallopian tube. At times the diagnosis would tend to be made when a laparotomy or laparoscopy is undertaken for an acute lower abdominal pain for sepsis, tube-ovarian mass or possibly ectopic pregnancy or when the patient has not responded to appropriate antibiotic treatment for a provisionally diagnosed pelvis inflammatory disease (PID)/pelvis abscess.
Diagnosis:
Considering that Aspergillosis can affect various organs of the body and the commonest Aspergillus infection does tend to involve, the diagnosis of Aspergillosis would tend to be associated with the clinician having a high index of suspicion for the diagnosis of Aspergillosis. Nevertheless, the ensuing summations related to modes of diagnosis of various organs of the body:
- It has been pointed out that upon chest radiograph (chest X-ray) and computed tomography (CT) scan, pulmonary aspergillosis classically does tend manifest as or depict a halo, and subsequently later, an air crescent sign. [8] [57]
- With regard to hematologic patients who are afflicted by invasive aspergillosis, the galactomannan test could make the diagnosis of Aspergillosis in a non-invasive way. [8]
- False-positive Aspergillus galactomannan test results had been reported in patients on intravenous treatment with some antibiotics or fluids which contained gluconate or citric acid such as some transfusion platelets, parenteral nutrition, or PlasmaLyte [8]. [58] [59]
- Upon microscopy histopathology examination of specimens of tissues that are afflicted by Aspergillosis, Aspergillus species tends to be reliably illustrated by utilization of silver stains for examples by utilization of, Gridley stain or Gomori methenamine silver. [8] [60]
- It has been pointed out that these stains in cases of Aspergillosis do depict the fungal walls as having grey-black colour. It has also been pointed out that the hyphae of Aspergillus species do range with regards to diameter from 2.5 to 2.5 to 4.5 μm as well as they tend to contain septate hyphae; [8] [61]; nevertheless, these tend not to be apparent, and in such scenarios, they might be mistaken for Zygomycota [8] [60]
- It has also been pointed out that upon microscopy histopathology examination, Aspergillus hyphae tend to be found to depict dichotomous branching which is progressive and primarily at acute angles of about 45 degrees (45°) [8] [60]
Treatment:
The general treatment of Aspergillosis has been summated as follows: [8]
- It has been documented that the current medicaments that are utilized for the treatment of aggressive invasive aspergillosis include: Voriconazole and liposomal amphotericin B in combination with surgical debridement / excision of the lesion. [8]. [62]
- With regard to other allergic bronchopulmonary aspergillosis that are less aggressive, it has been stated that the findings had suggested utilization of oral steroids for a prolonged period of time, preferably for a period 6 months to 9 months in cases of allergic aspergillosis of the lungs. [8] [63]
- It has been iterated that Itraconazole tends to be given with steroids, as it is regarded as being associated with a "steroid-sparing" effect, causing the steroids to be more effective, and thus enabling utilization of a lower dose. [63] [64]
- It has been pointed out that other medicaments are utilized including: amphotericin B, casofungin in combination therapy only, flucytosine in combination therapy only, or itraconazole, [63] [65] [66] for the treatment of Aspergillosis fungal infection. Nevertheless; a growing proportion of infections have been reported to be resistant to the triazoles. [8] [63] [67]
- It has been reported that Aspergillosis fumigatus which is the most commonly infecting species, is intrinsically resistant to fluconazole [8] [63] [68].
[b] Miscellaneous Narrations Methods And Discussions From Some Case Reports, Case Series, And Studies Related To Aspergillosis Of The Kidney, And The Genito-Urinary Tract In Males And Females.
Li, et al. [69] reported a 61-year-old man who was admitted to the Urology Clinic of Huashan Hospital of Fudan University in Shanghai, China, because he had an aggravating skin erosion and bleeding on his glans. He stated that the problem had begun with a reddish rash which was found upon his coronary groove 3 years prior to his presentation, which was subsequently ensued by his development of swelling and extravasation of purulent secretion. The patient had been previously undergone treatment with utilization of unknown creams and oral antibiotics at a local private clinic. The lesion was noted to have deteriorated over a period of time. His glans was found to have eroded and was bleeding upon his manifestation to the clinic of the authors. Furthermore, the corpus cavernosum of his penis had detached from his glans and a urethral perforation was noted which had occurred upon the ventral side of his penis. The patient reported that he had difficulty with sexual activity as well as with voiding urine. All of the treatments he had tried within other hospitals had been noted to be not effective and his undergoing of partial amputation of his penis was suggested before he came to the hospital of the authors. The patient did not have any past history of immunodeficiency or penile injury. He underwent a series of serological studies, which included human immunodeficiency virus (HIV), rapid plasma reagin (RPR), herpes simplex virus (HSV) and tissue cultures for screening bacteria and Mycobacterium tuberculosis, within the hospital of the authors. Li et al. [67] reported that all of the test results were noted to be negative. In view of this, a penile biopsy was undertaken, and pathology examination of the biopsy specimen had shown features of chronic inflammation with fungal infection of the glans penis. The specimen was then sent for fungal culture. Seven days after the specimen was cultured, a velvety, golden-yellow mould was noted to have grown on Czapek’s agar. Based on the morphological features of the fungus, a diagnosis of A. flavus infection was made. He underwent treatment which included medication and surgery. Firstly, the patient underwent insertion of suprapubic cystostomy and debridement. Pursuant to the surgery, the penile lesion was washed with 0.5% neomycin solution daily in order to prevent bacterial infection and in order to eliminate necrotic tissue. Meanwhile, he received treatment in which he received itraconazole, 200 mg, twice per day, which was combined with tinidazole, 400 mg, twice per day, intravenously for 20 days. One month subsequently, vitalized tissue was found at the site of his penile lesion. He underwent plastic surgery to close his wound and to repair his ruptured urethra in a one-stage procedure. His glans was sutured onto the corpus cavernosum in two layers and the urethral perforation was sutured transversely with 4-0 absorbable suture (Ethicon’s coated Vicryl suture, Ethicon, Inc., Johnson & Johnson Medical, China). Twenty days following his operation, his wound was found to be completely healed, and the patient was able to urinate spontaneously normally and he did experience a return of his erections. During the patient’s 1-year follow-up assessment, his natural urination and erection were found to have persisted without the occurrence of urethral stricture.
Li et al. [69] iterated the ensuing summations:
- Balanitis is a common clinical condition which tends to be encountered in male patients who manifest to urology clinics, and which could be caused by different pathological entities.
- Diabetes mellitus, HIV infection and iatrogenic immunosuppression tend to be found to be the underlying medical conditions in patients who are diagnosed as having fungal balanitis. [70] Nevertheless, balanitis which is caused by Aspergillus had only been reported on rare occasions.
- Cutaneous aspergillosis could be classified as either (i) primary cutaneous aspergillosis, following direct inoculation of Aspergillus at sites of skin injury, or (ii) secondary aspergillosis, which does occur via haematogenous spread [71].
- According to the case history and the serological tests they had undertaken, the reported patient had none of the aforementioned underlying medical conditions which tend to be commonly associated with fungal balanitis. The only possible risk factor that the reported patient had possessed for fungal balanitis was his long-term utilization of unknown creams which could have contained glucocorticoids, which might have suppressed his local immune responses.
- The clinical manifestation of cutaneous aspergillosis is typified by the presence of violaceous macules, papules, plaques or nodules, haemorrhagic bullae, ulcerations with central necrosis with or without eschar formation, pustules or subcutaneous abscesses [71]
- With regards to their reported patient, macules and papules were initially visualized at the patient’s coronary groove. The lesion had deteriorated over a period of time, with the development of swelling, extravasation of purulent secretion, tissue erosion and bleeding. He developed urethral perforation following his development of an abscess upon the ventral side of the penis which became ulcerated.
- Even though the patient had manifested with the typical symptoms of cutaneous aspergillosis, the infrequency of penile aspergillosis had led to misdiagnosis before he came to their hospital.
- The diagnosis of aspergillosis does depend upon pathological examination of specimens of the lesion and fungal culture, which was not undertaken within the other hospitals.
- The appropriate therapy of cutaneous aspergillosis should include a combination of antifungal chemotherapy and surgical debridement, if necessary.
- The antifungal medicaments that tend to be commonly utilized to treat cutaneous aspergillosis have been documented to include: amphotericin-B, [72] terbinafine, [73] [74] caspofungin, [75] itraconazole as well as flucytosine [76]
- It has been iterated that despite treatment with efficacious antifungal therapy, combined surgical therapy should still be recommended in the treatment of these patients [77] [78]
- With regards to their reported case, they chose itraconazole as their antifungal agent. Plastic surgery was undertaken in order to close the wound and repair the urethral perforation after the tissue at the site of the lesion had healed and became vitalized.
- Through their reported case, they had hoped to reiterate the appropriate diagnostic and treatment methods which should be utilized in cases of penile aspergillosis. In their case, pathology examination of the biopsy specimen had demonstrated features of chronic inflammation and fungal infection at the glans, which had led them to undertake fungal culture in order to identify the exact pathogen. The patient had recovered completely pursuant to his on being given effective antifungal medication and pursuant to the undertaking of plastic surgery.
Khawand et al. [79] reported report a rare case of primary prostatic aspergillosis in a well-controlled diabetic man who manifested with acute retention of urine into their clinic. This case report has reminded clinicians that on rare occasions aspergillosis of the prostate gland could present as acute retention on rare occasions for which clinicians need to have a high index of suspicion.
Roux et al. [80] stated the following:
- Treatment of chronic lymphocytic leukaemia (CLL) has been rapidly evolving, with emerging new medicaments.
- Alemtuzumab is a monoclonal antibody recognizing CD52 antigen which had been approved for the treatment of relapsing-refractory CLL.
- A frequent side effect of Alemtuzumab is its immunosuppression and patients who are treated with alemtuzumab do have the risk for the development of fungal infections such as aspergillosis.
- Roux et al. [80] reported a patient who had developed an uncommon localization of aspergillosis: prostatic and renal, after undergoing treatment by utilization of alemtuzumab monotherapy. During the week 8 of the patient’s alemtuzumab treatment, the patient manifested with: fever, urinary frequency and urologic symptoms. Roux et al. [80] reported that persistence of the patient’s fever with common antibiotic therapy led to the undertaking of a tomography which had shown features of prostatic and renal abscess that measured 70mm and 29mm. Based upon this it was decided to undertake prostate biopsy. Histopathology examination of the prostate biopsy specimens demonstrated features of a suppurative abscess with ischemic necrosis and fungal proliferation, with branched fungal hyphae. Direct examination was negative. Culture on Sabouraud's agar demonstrated a mould which was identified as Aspergillus fumigatus. The organism was reported to be susceptible to voriconazole (MIC: voriconazole 0,25ug/mL). Roux et al. [80] concluded that in view of the fact that the main side effect of alemtuzumab is immunosuppression, they had to research fungal infections such as Aspergillosis, particularly in patients who have fever that is resistant to common antibiotic therapy.
- Abbas et al. [81] stated that aspergillosis of the prostate gland is rare infection and by the time of the report of their case in 1995, 3 cases of aspergillosis of the prostate gland had previously been reported. Abbas et al. [81] had reported a case of localized invasive aspergillosis of the prostate gland in a non-immunocompromised patient who had chronic urinary retention and recurrent urinary tract infections. The patient underwent transurethral resection of prostate (TURP) which was followed by the undertaking of open prostatectomy for massive prostate gland enlargement. They stated that no systemic antifungal treatment was required to provide cure of the aspergillosis of the prostate gland. This case should also remind all clinicians that with regard to immunocompromised individual males, they could on rare occasions develop aspergillosis of the prostate gland and they could present with acute retention of urine.
Hemal et al. [82] stated the following:
- Aspergillosis v to the urinary tract is a rare disease which has tended to be encountered most often in patients who have altered immune status.
- By the time of the report of their case in 1999, only 19 cases of renal aspergillosis including 3 with AIDS and 4 cases of isolated aspergillosis of the prostate gland had been reported.
- They had reported the first case of concomitant renal and prostatic aspergillosis in a non-immunocompromised patient who had manifested with pyrexia of unknown origin and with dysuria.
- The diagnosis of aspergillosis was based upon the demonstration of typifying hyphal elements upon direct microscopy examination and isolation of the fungus within the culture of pus from the kidney.
- In view of obstructive prostatic enlargement as well as his left non-functioning renal mass, transurethral resection of the prostate and left nephrectomy, were undertaken in a single session with successful outcome.
- Ansari et al. [83] reported the first case of aspergillus mycotic aneurysm ensuing concomitant prostatic and renal aspergillosis. The patient had undergone left nephrectomy and transurethral resection of prostate for aspergillus infection one year earlier. He again manifested with lower urinary tract symptoms (LUTS) as well as backache and his clinical examination had demonstrated visible pulsations in his epigastrium. He had computed tomography (CT) -scan of abdomen, which demonstrated a pseudoaneurysm of the abdominal aorta. The aneurysm was repaired in situ with homo-grafting and omental wrap. Nevertheless, the patient died as a sequel of septicaemia on the tenth postoperative day. Ansari et al. [83] iterated the following:
- With regards to aspergillosis infection, Adjunctive surgery tends to be usually essential as medical management alone has tended to be unsatisfactory.
- It is imperative that these cases should be followed-up closely in order to detect the disease recurrence and complications at the earliest opportunity.
- Ludwig et al. [84] stated that aspergillosis of the prostate gland is a rare finding with only ten cases reported prior to the report of their case in 2005 based upon evidence they had obtained in the literature. Ludwig et al. [84] reported the first case of systemic aspergillosis, which had predominantly manifested with prostatic involvement and, clinically, with urinary retention in an immunocompetent host. Routine transurethral resection was undertaken due to the clinical assessment finding of benign prostatic hyperplasia with sub-vesical obstruction. Concomitant prostatic aspergillosis was diagnosed without signs of systemic infection. Ludwig et al. [84] also reported that in the clinical follow-up of the patient it was found that his systemic aspergillosis became rapidly progressive that required the undertaking of complex surgical interventions and long-term antifungal therapy.
- Thomas et al. [85] stated that fungal prostatitis is a rare, the presentation of which tends usually to simulate the presentations of benign prostatic hypertrophy and it usually has tended to be diagnosed unexpectedly pursuant to the undertaking of surgery to relieve prostatic obstruction. They iterated that to their knowledge, they had reported the first case of aspergillosis of the prostate gland which had developed as a complication of an indwelling urinary bladder catheter. Thomas et al. [85] stated that this unusual presentation of invasive aspergillosis had occurred in a patient who was at risk for the development of invasive fungal disease because of utilization of chronic steroids as well as recent administration of broad-spectrum antibiotics.
Stuart et al. [86] stated the following:
- Aspergillosis which is limited to the urinary tract is a rare disease, and this type of aspergillosis tends to be seen most often in patients who have altered immunity, especially patients who have diabetes mellitus.
- The disease has 3 patterns, 2 of which had been previously described.
- Stuart et al. [86] reported the first case which had documented the ascending route of infection. Stuart et al. [86] the following recommendations:
- Multiple urine cultures might be required for the proper identification of aspergillosis
- Histopathology examination and culture of sloughed tissue and fungus balls shed per urethram are the essential means of establishing a reliable diagnosis.
- Successful treatment of this disease which is localized to the urinary tract does require having a high index of suspicion in certain clinical settings, prompt diagnosis, a combination of systemic and local antifungal chemotherapy, and surgical drainage when necessary.
Valerio et al. [87] stated the ensuing:
- Human cancer of the prostate gland, is the second most frequently diagnosed cancer globally, and its incidence rate has continued to increase.
- Advanced cancer of the prostate gland is more difficult to treat than to treat early forms due to its chemotherapy resistance.
- There is need for the identification of more effective agents which could inhibit the progression of advanced prostate cancer.
- Demethoxyfumitremorgin C (DMFTC) had been isolated from the fermentation extract of the marine fungus Aspergillus fumigatus.
Valerio et al. [87] reported that they had examined Antiproliferative activity of DMFTC against human prostate cancer PC3 cells through cell cycle analysis by flow cytometry, the fluorescent nuclear imaging analysis with propidium iodide (PI), and proteins expression related to cell cycle arrest and apoptosis were investigated via Western blotting. DMFTC inhibited PC3 cells growth through G1 phase cell cycle arrest and apoptosis induction. They found that it activated the tumour suppressor p53 and the Cdk inhibitor p21, which regulate the cell progression into the G1 phase. They additionally found the following: PI-positive late apoptotic non-viable cells were increased and the expression levels of the G1-positive downstream regulators cyclin D, cyclin E, Cdk2, and Cdk4 were decreased by DMFTC treatment. Valerio et al. [87] concluded that their results had suggested that DMFTC induces G1 arrest and apoptosis induction through regulation of p53/p21-dependent cyclin-Cdk complexes, and it might be a useful therapeutic agent for the treatment of human advanced prostate cancer.
Even though a number of case reports of clinical aspergillosis infection of the prostate gland had been published, the lesson learnt from this summation does indicate that medical and oncological pharmacological studies do indicate some Aspergillus species could be developed into medicaments suitable for the treatment of prostate cancer.
Davido et al. [88] in 2007, stated that disseminated aspergillar infection involving the genitourinary system is quite uncommon as well as often fatal. They also iterated that only one previous case of aspergillosis of the scrotum had been reported prior to 2007 and that in the previous report, the patient had died despite aggressive surgical debridement. Davido et al. [88] reported a case of aspergillosis involving the scrotum in which the patient did well following his undergoing of conservative medical management.
Kim and Park [89] stated the following:
- Human prostate cancer is the second most frequently diagnosed cancer worldwide, and its incidence rate continues to increase.
- Advanced prostate cancer is more difficult to treat in comparison with early forms due to its chemotherapy resistance.
- There is need for more effective agents which could inhibit the progression of advanced prostate cancer.
- Demethoxyfumitremorgin C (DMFTC) was isolated from the fermentation extract of the marine fungus Aspergillus fumigatus.
- Antiproliferative activity of DMFTC against human prostate cancer PC3 cells was examined through cell cycle analysis by flow cytometry studies, the fluorescent nuclear imaging analysis with propidium iodide (PI), and proteins expression related to cell cycle arrest and apoptosis were investigated with the use of Western blotting. DMFTC inhibited PC3 cells growth through G1 phase cell cycle arrest and apoptosis induction. It activated the tumour suppressor p53 and the Cdk inhibitor p21, which regulate the cell progression into the G1 phase.
- Additionally, PI-positive late apoptotic non-viable cells were increased and the expression levels of the G1-positive downstream regulators cyclin D, cyclin E, Cdk2, and Cdk4 were decreased by DMFTC treatment. These results suggest that DMFTC induces G1 arrest and apoptosis induction through regulation of p53/p21-dependent cyclin-Cdk complexes, and it may be a useful therapeutic agent for the treatment of human advanced prostate cancer.
Mathew et al. [90] stated the ensuing:
- Pulmonary aspergillosis is a well-known clinical entity which does tend to occur in immunocompetent persons.
- Cutaneous aspergillosis, on the other hand, has been reported in cases of suppressed immunity.
- Recently, invasive aspergillosis had been reported in patients who had subtle immune dysfunction such as those who had critical illness and advanced cirrhosis.
Mathew et al. [90] reported a case of scrotal aspergillosis in association with Fournier’s gangrene and necrotizing fasciitis in a patient who had cirrhosis of the liver.
Martinez-Salas et al. [91] stated that: Invasive Aspergillus infection of the kidney and the upper urinary tract is extremely rare, and this had almost exclusively been diagnosed in immunocompromised patients, such as organ transplant, hematologic malignancies, and immunosuppressive therapies, infection of lower urinary tract is even less common, as bladder aspergillosis had only been reported in 6 publications prior to the publication of their article in 2022. so far, all of them in male patients.
Martinez-Salas et al. [91] reported a 74-year-old male who did not have any relevant medical background including diabetes mellitus or hypertension, who had undergone an uneventful transurethral resection of prostate (TURP) due to benign prostatic hyperplasia in another hospital four months earlier. Following his discharge from hospital, he was referred because of his ongoing symptoms which included: intermittent haematuria, mixed urinary incontinence, urinary urgency, incomplete emptying of his urinary bladder, urinary frequency with voiding between 15 times and 20 times per day, nocturia and intermittent low-grade pyrexia which had ranged between 37.2 and 38.0 °C, as well as right testicular pain and enlargement. He was admitted to the Emergency Department of the reporting hospital because of low-grade fever of 37.8 °C, as well as abdominal pain. Upon his clinical examination, his urinary bladder was found to be palpable and fixed upon suprapubic palpation, with severe pain upon suprapubic superficial palpation, and his right testis was enlarged, painful as well as indurated.
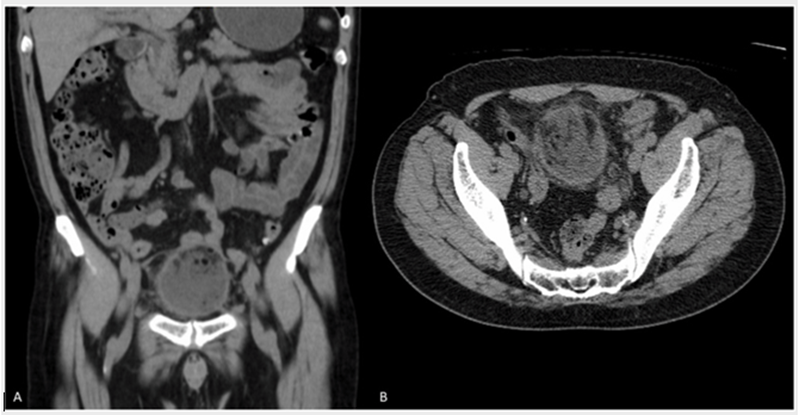
The results of his routine haematology and biochemistry blood tests were reported to have shown the following: leukocytosis (11,000/mm3) with neutrophilia (80%), and elevated serum creatinine (1.4 mg/dL) with an estimated glomerular filtration rate (eGFR) of 53 mL/min/1.73 m2 (CKD-EPI equation). His urinalysis reported the finding of abundant leucocytes, erythrocytes, and bacteria. He had ultrasound scan of renal tract which demonstrated bilateral pyelocaliceal dilation. The imaging of his urinary bladder was not satisfactory because of his severe pain upon transducer placement. He had computed tomography (CT) scan of abdomen with no contrast (due to his eGFR) and the CT scan showed bilateral pelvic and ureteric dilation, and a dysmorphic urinary bladder with a tumour with possible extravesical extension into the dome of his urinary bladder (see figure 1). He also had ultrasound scan of his testes which was reported to have demonstrated features that confirmed a diagnosis of right epididymitis.
Reproduced from:
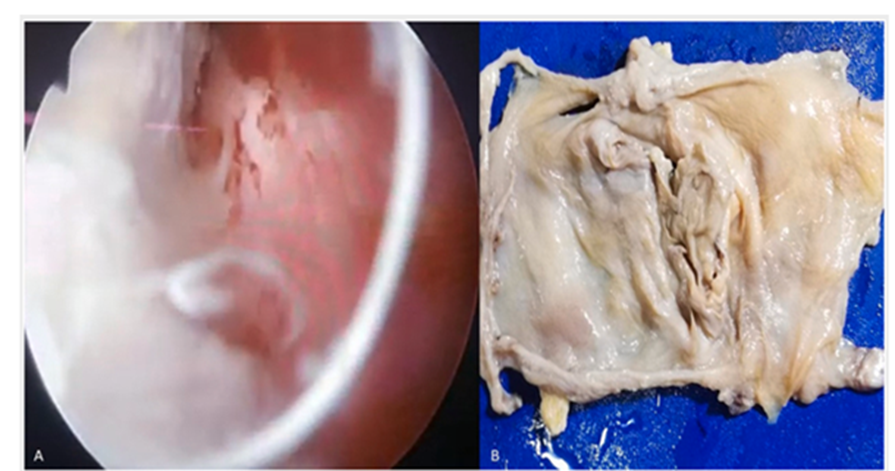
The patient was admitted to hospital and he was commenced on intravenous antibiotic treatment with Ertapenem. He underwent diagnostic work-up assessment which included a cystoscopy in which abundant mucous, detritus, and an intravesical whitish mass, was found. Resection with bipolar resectoscope of the urinary bladder mass was not possible, and due to the features of the intravesical mass a mini-suprapubic cystostomy was undertaken, extracting a whitish, gelatinous mass, which was macroscopically compatible with a fungal mass (see figure 2).
Reproduced from: [91]
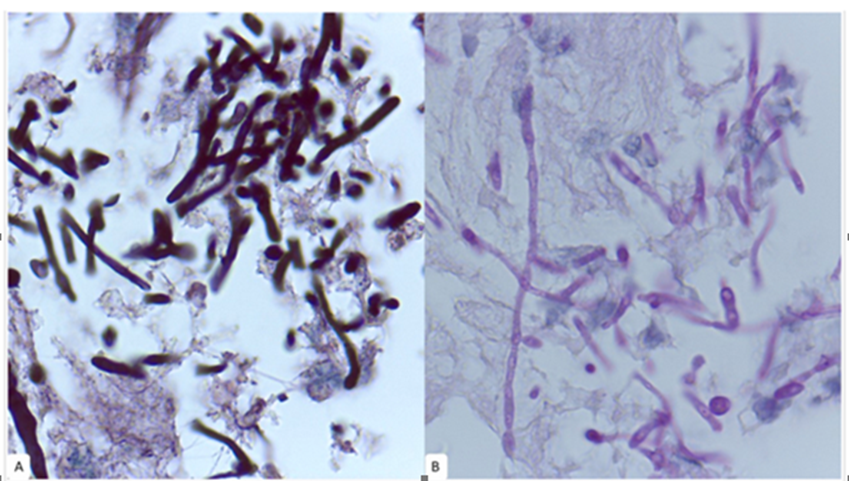
Histopathology examination of the resected urinary bladder mass specimen revealed that the bladder mucosa had been infiltrated by abundant hyaline filamentous fungi of the Ascomycota phylum, with septate hyaline hyphae that was compatible with Aspergillus species (see figure 3). Urine specimens were taken for culture during the cystoscopy and microbiology examination of the urine was reported as demonstrating mixed Candida species and bacterial development. Additionally, he had serum galactomannan antigen test, HIV, Diabetes Mellitus, and hematologic pathologies work-up and this was reported as negative.
Reproduced from [91]
Based upon the microbiology results, antibiotic therapy was suspended and Isovuconazole was commenced. The patient was discharged on postoperative day 6 with transurethral silicone 18 Fr foley catheter and advised to complete 4-weeks of oral Isavuconazole. During his follow-up assessment, he underwent cystoscopy evaluation immediately after the last day of his savuconazole treatment, and the cystoscopy demonstrated normal mucosal macroscopic appearance of the urinary bladder. Histopathology examination of his random bladder biopsy specimens showed absence of Aspergillus species. His right epidydimitis also had resolved. His lower urinary tract symptoms (LUTS) and pyrexia had also disappeared. His kidney function had also improved in that he had a serum creatinine of 0.7 mg/dL (eGFR of 97mL/min/1.73 m2).
Martinez-Salas et al. [91] made the ensuing summating discussions:
- Aspergillus species is a ubiquitous environmental fungus of the Ascomycota Phylum that is found in plants, soils, decaying organisms, as well as within environmental aerosols.
- They produce asexual conidia which tend to be highly resistant and which could spread through surfaces and air.
- It is through these conidia that Aspergillus could enter the lower respiratory tract, where majority of Aspergillus infections could occur.
- It has been stated that the commonest invasive Aspergillus species are Aspergillus fumigatus (which accounts for 90% of the species, A. flavus and A. niger species.
- The first case of urinary bladder aspergillosis was reported in 1978 in a male patient who had Diabetes Mellitus and a previous abdominal surgical intervention, that was successfully treated with transurethral evacuation of bladder clots and fungal masses, and postoperative intravesical instillations of Amphotericin B and oral Nystatin for 25 days. [92]
- The most recent case was reported by Hameed et al. [93] in 2020, in a male patient who was unaware of having a diagnosis of Diabetes Mellitus who was admitted with urinary retention due to an intravesical bladder fungal mass that was treated with transurethral evacuation. There was no evidence of upper urinary tract involvement in the case. [93]
- With regard to their reported case, therapy with Isavuconazole was discussed among the attending specialists and was decided based on several assumptions. First, the patient's immune status was not known and it was assumed to be immunocompromised. Secondly, the patient had at least two possible sites of Aspergillus infection which included his urinary bladder and his right testis, as well as a disseminated disease was a possibility. Thirdly, his preliminary pathology findings were inconclusive of a specific fungus; hence, the possibility of Mucorales infection was considered. Previous reports of Isavuconazole treatment had been reported in both Mucorales and Aspergillus infections, especially in the case of patients who were immunocompromised. [94].
Martinez-Salas et al. [91] made the ensuing conclusions:
- Aspergillosis of the lower genitourinary tract aspergillosis is an extremely rare disease, especially in immunocompetent patients.
- Certain possible risk factors should be taken into consideration including: male gender, immunocompromised status, as well as a history of previous intravesical catheter or transurethral surgery.
- Persistent lower urinary tract symptoms without improvement despite antibiotic and medical therapy in the presence of an unknown atypical bladder mass should raise the suspicion of fungal infections.
- When it is possible, transurethral resection or evacuation of fungal mass should be undertaken and systemic antifungal treatment, with Isavuconazole or other antifungal drugs should be individualized.
Hood et al. [95] iterated that to their knowledge they had described the first case of prostatitis and epididymoorchitis which had been caused by Aspergillus fumigatus in a patient who had AIDS. Hood et al. [95] reported a 37-year-old man who had HIV infection and who did not have any pre-existing kidney disease, who was admitted with a 2-week history of dysuria as well as polyuria which had not responded to treatment with Co-Amoxiclav. The patient’s reported previous AIDS-defining illnesses included: Mycobacterium avium, candidiasis of the oesophagus, as well as recurrent bacterial pneumonitis. His clinical examination demonstrated tenderness in his supra-pubic region as well as tenderness within his prostate gland. The results of his laboratory blood were summated to include the following: Hb 9.9 g/dL, mean corpuscular value (MEV) 127 fl, WBC count 3.6 x 109 / L, neutrophils 1.27 x109 / L, CDT lymphocyte count 21 x 10 6 / L. The results of his urinalysis were reported as follows: WBC count > 10.106 /L and RBC < 1>
- Even though rare, Aspergillosis prostatitis alone, or Aspergillossis epididymoorchitis alone or Aspergillosis prostatitis which is ensued by unilateral or bilateral epididymoorchitis could affect some individuals and hence all clinicians and urologists need to have a high index of suspicion for this rare disease I order to establish an early diagnosis of the infection.
- All clinicians including urologists should be aware of the fact that if they treat their patients for a presumed bacterial prostatitis and or epididymoorchitis with the usual antibiotics and the symptoms persist or do not resolve, then they should quickly test for the possibility of the infection being Aspergillosis and biopsies of the prostate and epididymis for histopathology examination and culture should be quickly undertaken.
- Aspergillosis of the prostate gland and epididymis and testis potentially could be severe infections that would require effective treatment to be undertaken quickly.
Marr et al. [96] stated that stablishing of a rapid diagnoses of invasive aspergillosis (IA) is a priority and tests that detect galactomannan and β-D-glucan are available, but are technically cumbersome and rely upon invasive sampling (blood or bronchoalveolar lavage. Marr et al. [96] optimized a lateral flow dipstick assay utilizing the galactofuranose-specific monoclonal antibody (mAb476), which recognizes urine antigens after Aspergillus fumigatus pulmonary infection in animals. Marr et al. [96]] obtained urine samples from a cohort of 78 subjects, who were undergoing evaluation for suspected invasive fungal infections, and stored frozen until testing. The urine was processed by centrifugation via desalting columns and exposed to dipsticks. Reviewers who were blinded to the clinical diagnoses graded results. Western blots were performed on urine samples from 2 subjects to characterize mAb476-reactive antigens. Marr et al. [96] summarized the results as follows:
- Per-patient sensitivity and specificity for diagnosis of proven or probable IA in the overall cohort was found to be 80% (95% confidence interval [CI], 61.4%–92.3%) and 92% (95% CI, 74%–99%), respectively.
- Within the subgroup that had cancer, the sensitivity was 89.5% (95% CI, 66.7%–98.7%) and specificity was 90.9% (95% CI, 58.7%–99.8%); among all others, sensitivity and specificity were 63.6% (95% CI, 30.8%–89.1%) and 92.9% (95% CI, 66.1%–99.8%), respectively.
- Eliminating lung transplant recipients who had airway disease increased the sensitivity in the non-cancer cohort (85.7% [95% CI, 42.1%–99.6%]).
- Semiquantitative urine assay results had correlated with serum galactomannan indices.
- Western blots had demonstrated mAb476-reactive antigens in urine from cases, that ranged between 26 kDa and 35 kDa in size.
- Marr et al. [96] concluded that urine testing utilizing mAb476 could be used as an aid to diagnose IA in high-risk patients.
Hoenig et al. [97] stated the following:
- Early diagnosis of invasive aspergillosis (IA) does remain challenging, with available diagnostics being limited by inadequate sensitivities and specificities.
- Triacetylfusarinine C, a fungal siderophore which had been demonstrated to accumulate in urine in animal models, is a potential new biomarker for diagnosis of IA.
Hoenig et al. [97] developed a method which allowed absolute and matrix-independent mass spectrometric quantification of TAFC. Hoenig et al. [97] determined urine TAFC, normalized to creatinine, in 44 samples from 24 patients who had underlying hematologic malignancies and probable, possible or no IA according to current EORTC/MSG criteria and these were compared to other established biomarkers measured in urine and same-day blood samples. Hoenig et al. [97] summarized the results as follows: TAFC/creatinine sensitivity, specificity, positive and negative likelihood ratio for probable versus no IA (cut-off ≥ 3) were 0.86, 0.88, 6.86, 0.16 per patient. Hoenig et al. [97] made the following conclusions:
- For the first time, they had provided proof for the occurrence of TAFC in human urine.
- TAFC/creatinine index determination in urine demonstrated promising results for the diagnosis of IA offering the advantages of non-invasive sampling.
- Sensitivity and specificity of the tests were similar as reported for GM determination in serum and bronchoalveolar lavage, the gold standard mycological criterion for IA diagnosis.
- Hoenig et al. [97] declared the highlights from their study as follows:
- Diagnosis of invasive aspergillosis (IA) is unsatisfying with current methods.
- New method for the quantification of an Aspergillus siderophore (TAFC) had been established.
- The determination of TAFC in urine had yielded promising results for diagnosing IA.
- Detection in urine does offer the advantage of non-invasive sampling
- Rocus et al. [98] stated the following summations studies related to Utility of Aspergillus Antigen Detection in Specimens Other than Serum Specimens:
- The detection of circulating galactomannan in serum is an important tool for the early diagnosis of invasive aspergillosis.
- A commercial enzyme-linked immunosorbent assay (Platelia Aspergillus; BioRad) had been demonstrated to be both highly sensitive and specific for detection of galactomannan in serum samples.
- Despite the fact that this assay had been validated for serum samples, specimens of other body fluids were being increasingly utilized for the detection of galactomannan, including urine, bronchoalveolar lavage fluid, and cerebrospinal fluid.
- Their review of the literature had revealed that galactomannan could be detected in each of these samples from patients who have invasive aspergillosis with higher sensitivity than was the case with culture, as well as early in the course of the infection.
- Nevertheless, the evidence thus far had been based upon case reports which were predominantly retrospective studies which often had included heterogeneous patient populations and limited numbers of cases of proven infection.
- Clearly, well-designed prospective studies with systematic sampling and utilization of consensus case definitions would be required in order to compare the performance of antigen detection in samples other than serum specimens with that in serum specimens.
Sakamoto et al. [99] reported an unusual case of fungus ball formation of Aspergillus in the bladder without any evidence of disseminated and renal aspergillosis. Sakamoto et al. [99] reported a 49-year-old man whose main complaint was progressively worsening dysuria after he had undergone a stomach operation for which he was admitted. He underwent cystoscopy which demonstrated many ball-like masses on the retro-trigone and left wall of his urinary bladder. Histopathology examination of his urinary bladder mass revealed that the masses were composed of many Aspergilli. This case summation has demonstrated that Aspergillosis of the urinary tract does manifest with non-specific symptoms.
Salgia et al. [100] reported a well-controlled diabetic patient who had presented with recurrent attacks of renal colic and passage of soft masses per urethra, which were identified as aspergillus fungus balls; he was treated with amphotericin B, pursuant to which he was free of renal colic and his urine cultures were negative for aspergillus. This summation has highlighted the fact that Aspergillosis of the urinary tract may manifest with symptoms that simulate renal colic and at times soft masses may be passed in the urine of patients.
Siddappa et al. [100] stated that a urinary bladder infection of Aspergillus with no evidence of dissemination is uncommon. Siddappa et al. [100] reported a case of Aspergillus infection with transitional cell carcinoma of the urinary bladder without any evidence of systemic involvement. Siddappa et al. [100] reported a 65-year-old male diabetic whose main complaints included: intermittent painful visible haematuria and nocturia and who had undergone nephroureterectomy a year and a half earlier for transitional cell carcinoma of right renal pelvis. He underwent cystoscopy which had revealed his urinary bladder mucosa having fixed broad tumour with encrustation and bleeding upon touch at the right vesical-ureteric junction. The tumour was resected. The histopathology examination diagnosis of the resected tumour was a high-grade transitional carcinoma with Aspergillus infection. Fungal culture of his urine obtained after his urinary bladder wash yielded Aspergillus fumigatus.
Adam et al. [102] stated that Aspergillus is ubiquitous globally and that it is found primarily in soil, dust, vegetation, and decaying matter. They also stated that while disseminated aspergillosis does affect the testis, only 1% of the time, as well as that testicular aspergillosis in the absence of disseminated disease is exceedingly rare, as was demonstrated in their reported case.
Heylen et al. [103] stated that transplant recipients are at risk for the development of invasive aspergillosis (IA), associated with a significant mortality rate, as well as renal transplant–specific risk factors had not been established. Heylen et al. [103] identified forty-one adult kidney transplant recipients who were diagnosed with proven or probable IA from 1995 through 2013 by the searching of the computerized patient files in the University Hospitals Leuven. The control population in their 1:2 case-control study consisted of the 2 patients who had received a kidney transplant immediately before and after each identified patient and who did not develop IA (n = 82). Heylen et al. [103] summarized the results as follows:
- Leukopenia following kidney transplant had increased the risk of IA among all patients (odds ratio [OR], 2.345 [95% confidence interval {CI}, 1.084–5.071]).
- For early-onset infection which occurred during the first 3 months after transplantation, a longer duration of renal replacement therapy pretransplant and the occurrence of leukopenia were risk factors (OR per year, 1.192 [95% CI, 1.006–1.413] and OR, 3.346 [95% CI, 1.063–10.527], respectively), whereas donor cytomegalovirus seropositivity increased the risk for late-onset IA which occurred >3 months after transplant) (OR, 3.677 [95% CI, 1.388–9.743]).
- The twelve-week mortality rate was 39%.
- Disseminated infection, leukopenia, and the height of the serum galactomannan index were found to be associated with an increased risk of death (hazard ratio [HR], 5.080 [95% CI, 1.740–14.830]; HR, 3.198 [95% CI, 1.183–8.649]; and HR, 1.371 [95% CI, 1.123–1.674], respectively).
Heylen et al. [103] made the following conclusions:
- Prolonged renal replacement therapy preceding kidney transplant does increase the risk for the development of IA early after transplant.
- The height of the serum galactomannan index does predict mortality.
Najafi et al. [104] stated that an Aspergillus fungal ball is a rare cause of ureteral obstruction which had been attributed to indwelling catheters, stents, antibiotics, anastomotic leaks, obstruction, and immunosuppressive therapy and other immunocompromised states. Najafi et al. [104] reported a case of unilateral ureteral obstruction which was caused by Aspergillus terreus following the undertaking of ureteroscopic lithotripsy and ureteric stenting in a 45-year-old diabetic man. They reported that the patient was successfully treated with endoscopic removal of the fungal mass and oral voriconazole. Najafi et al. [104] also reviewed briefly the clinical features, treatment, and outcome in 9 previously reported diabetic patients with ureteral obstruction due to aspergillosis and they found that obstructive uropathy related to Aspergillus mass could be suspected in diabetic patients who had a history of manipulation, impaired kidney function, and persistent passage of a soft mass in urine. They stated that direct microscopy and culture of multiple urine and ureteral washing are necessary in order to establish an early diagnosis of aspergillosis associated ureteric obstruction and that antifungal treatment and endoscopic removal of the mass are needed to reduce morbidity. Smaldone et al. [105] stated that
Ureteric obstruction as a result of a primary aspergillus infection is rare and that early clinical suspicion in immunosuppressed patients is essential to establish the diagnosis. Smaldone et al. [105] reported a case of a 50-year-old diabetic woman who had manifested with acute renal failure, sepsis, and bilateral ureteral obstruction. Her initial management included insertion of bilateral percutaneous nephrostomy tubes. Urine culture from both of her left and right renal pelvis grew Aspergillus flavus. They reported that the left-sided obstruction resolved with antifungal therapy. Nevertheless, her right ureteral obstruction had persisted and was managed with ureteroscopy and removal of the fungal bezoar.
Ahuja et al. [106] stated that fungal bezoar of the kidney is a rare clinical entity, which usually tends to be seen in a diabetic, immunocompromised, or chronic alcoholic patient who has had prolonged catheterization and that angio-invasive fungal infections such as aspergillosis tend to be associated with severe renal lesions and kidney failure with high morbidity and mortality rates. Ahuja et al. [106] reported a patient who developed complete obstruction of the left ureter as a result of Aspergillus fungal balls which were successfully removed ureteroscopically.
Choi et al. [107] stated that ureteric obstruction could develop in immunocompromised patients with an Aspergillus fungal infection as well as that infections could progress to invasive aspergillosis, which is highly lethal. Choi et al. [107] reported a case of a 56-year-old man who had alcoholic cirrhosis of the liver and diabetes mellitus. He had ureteric aspergilloma, discovered as a saprophytic whitish mass. This was treated by ureteroscopy removal; nevertheless, he refused antifungal treatment. His condition progressed to invasive aspergillosis, and he died from sepsis and hepatorenal syndrome.
Zhu et al. [108] stated that aspergillus osteomyelitis had been reported as a result of dissemination in solid organ transplant recipients and that vertebral osteomyelitis is one of the most common forms of Aspergillus osteomyelitis. They additionally stated that an Aspergillus fungal ball is a rare cause of ureteric obstruction. Zhu et al. [108] reported an unusual case of simultaneous vertebral osteomyelitis and ureteric obstruction which was caused by Aspergillus. flavus in a hepatic transplant recipient, who had been successfully treated with sequential intravenous and oral itraconazole solution.
Vuruskan et al. [109] stated the following:
- Mycotic infections in various organ transplant recipients do generally represent severe and often fatal complications.
- Aspergillosis which has been isolated from the urinary tract occurs quite infrequently in renal transplant recipients.
- Besides, fungus balls are uncommon causes of ureteric obstruction.
Vuruskan et al. [109] reported a 51-year-old patient who was diagnosed as having ureteric obstruction that was caused by aspergillosis in the early post-renal transplant period, who unfortunately died with the clinical picture of disseminated infection and its complications.
Guleria et al. [110] reported a patient who had ureteric aspergilloma as the cause of ureteric obstruction in the patient who was a renal transplant recipient. He was treated with oral itraconazole 600 mg/day. Four days later he underwent ureteroscopic resection The patient was a 30-year-old Indian male, who had undergone renal transplantation of a kidney and subsequently developed the aspergilla the mass. He had amphotericin irrigation which was continued in April 1995. His basic disease was for 10 days and he also had itraconazole at a dose of chronic glomerulonephritis of unknown aetiology. The kidney donor was his mother and there was a one, one, one mismatch on the A, B and Dr loci, respectively. The transplant operation was reported to have been uneventful and there was good primary function. Six days subsequently following a decrease in his urine output and an increase in his serum creatinine he was pulsed with three doses of methyl prednisolone. There was no response and a subsequent biopsy was taken of the transplanted kidney and pathology examination of the biopsy specimen demonstrated features of severe cellular rejection. He was given a 10-day course of OKT3. His rejection responded and he was discharged home with a serum creatinine of 1.6 mg/dl on triple drug immunosuppression. He did well for 13 months pursuant to his operation. Following the finding of an increase in his serum creatinine to 2.1 mg/dl he was admitted for evaluation. He had an ultrasound scan which demonstrated moderate hydronephrosis. He had a percutaneous nephrostogram which demonstrated a stricture at the lower end of the ureter. He was operated and the transplant ureter was anastomosed to his native ureter. He made an uneventful recovery and he was discharged home with a serum creatinine of 1.8 mg/dl. Four months subsequently, he manifested with anuria. His clinical examination showed that he was nonfebrile, with a Spores of Aspergillus are dangerous opportunistic leucocyte count of 6800 wbc/mm3, and a serum creatin- pathogens in the renal transplant recipient. Aspergillus ine concentration of 3.8 mg/dl. An urgent ultrasound usually a ects the lungs, central nervous system, scan showed hydroureteronephrosis. On cystoscopy a sinuses and skin. We describe ureteric aspergilloma large white friable mass was seen at the lower end of causing obstruction as a novel aspergillus related complication in immunosuppressed transplant recipients. the ureter. This was biopsied, a retrograde pyelogram performed, and a double J stent inserted. The biopsy revealed nonpigmented, septate filaments which showed repeated dichotomous branching. A percutaneous nephrostomy was performed to irrigate the ureter with amphotericin B 50 mg/l at a rate of 25 ml/h, with outflow provided by an indwelling Case report bladder catheter. He was administered oral itraconazole 600 mg/day. Four days later he underwent ureteroscopic resection A 30-year-old Indian male underwent a live related of the mass. The amphotericin irrigation was continued renal transplant in April 1995. His basic disease was for 10 days and the itraconazole at a dose of 400 mg/day for 8 weeks. A repeat nephrostogram 4 weeks later showed no filling defect and the urine was negative for hyphae. He was at the time of report of the case 3 months on their follow-up and was well with a serum creatinine of 2.4 mg/dl. The urine was negative for hyphae and he had minimal hydronephrosis on ultrasound examination.
Kueter et al. [111] stated that mycelial clumps or bezoars (fungus balls) as a cause of upper urinary tract obstruction are rare, with fewer than 60 cases that had been previously reported as well as that anuria due to bilateral ureteric obstruction with mycelial clumps is very rare. Kueter et al. [111] reported that a man who had bilateral ureteric obstruction that was caused by Aspergillus flavus and they described his diagnosis and treatment. Kueter et al. [111] stated that it was remarkable that radiology imaging modalities, including excretory urography, computed tomography, and retrograde ureteropyelography, did not identify filling defects to indicate a fungal causation of the ureteric obstruction, even in the presence of a rapidly progressing /process. They stated that for this reason, one should consider a fungal infestation in high-risk patients who have obstructive uropathy of unknown aetiology.
Rao et al. [112] stated the following:
- Fungal infections of the urinary tract usually tend to be encountered pursuant to prolonged antibiotic utilization, instrumentation and indwelling urinary catheters.
- These type-of-infections, tend to be mostly encountered in immuno-compromised patients.
- Candida is the commonest among the fungal infections of the urinary tract followed by Aspergillus infection.
Rao et al. [112] reported the case a 26-year-old diabetic female who had manifested with abdominal pain, fever, nausea and vomiting. She had undergone insertion of double-J ureteric stenting 15 days to 20 days earlier. The cause of her symptoms was not detected till the patient underwent computed tomography scan of her renal tract (C.T Scan KUB) with excretory urography which demonstrated the displaced D-J stent. Then on performing replacement of her D-J stent, cystoscopy examination was undertaken and the tissue sample was sent for microbiological and histopathological examination. On Microbiological examination, Aspergillus flavus was isolated from the tissue, which was culprit behind the disease. Patient was then treated with anti-fungal medications, following which she gradually improved.
Haq et al. [113] stated the following:
- Primary renal aspergillosis is rare in diabetic patients.
- The diagnosis of localized primary renal Aspergillus infection in diabetic patients does require careful investigations due to its benign manifestation and lack of associated systemic clinical features.
- There is also paucity of information related to the role of conservative treatment of such localized infection with antifungal agents only. Here, we describe a case of localized renal aspergillosis in a type 2 diabetic patient with a brief review of literature.
Haq et al. [113] reported a case of unilateral renal aspergillosis following intracorporeal pneumatic lithotripsy (ICPL) in a type 2 diabetic man. The man manifested with mild pain in his left lumbar region and periodic expulsion of whitish soft masses per urethra, which yielded growth of Aspergillus fumigatus. He was treated initially with amphotericin B; nevertheless, it was stopped after 2 weeks, as he could not tolerate the medication. He was subsequently, successfully treated with oral itraconazole.
Haq et al. [113] made the following conclusions:
- Localized renal aspergillosis could be suspected in diabetic patients who manifest with a history of urinary tract instrumentation, mild lumbar pain, passage of suspicious masses in urine and persistent pyuria.
- Examination of the suspicious substances that are expelled per urethra is essential for the diagnosis as routine multiple urine analysis may yield negative results.
- Conservative treatment with oral itraconazole alone is effective in cases that are associated with incomplete obstruction.
Yoon et al. [114] stated that urinary tract obstructions which is caused by Aspergillus bezoars had been reported on rare occasions. Yoon et al. [114] also stated that they had described in their article an unusual case which was caused by an isolate of the Aspergillus nidulantes subgenus, and they had reviewed the literature on 13 additional cases of ureteric obstruction due to renoureteric aspergillosis so as to provide the characteristics of this disease entity. Yoon et al. [114] reported that their case had manifested with a unilateral ureteric obstruction and acute renal failure due to Aspergillus bezoars. The patient was immunocompromised and she had received corticosteroid therapy for chronic obstructive lung disease and bronchiectasis. She was treated successfully with antifungal chemotherapy, which included amphotericin B followed by oral voriconazole for about two months and she had a percutaneous nephrostomy for one month. The patient's renal function completely recovered after she had undergone haemodialysis maintenance for six months.
Krishnamurthy et al. [115] reported a sixty-year-old previously healthy male patient who had manifested with anuric renal failure of sudden onset. He was detected to have Aspergillus fumigatus fungal balls within his renal pelvis, ureters and urinary bladder which were removed and his renal function improved. He was treated with itraconazole and he was sent home. Three weeks later he again manifested with anuria and renal failure. He had recurrence of the obstruction with the same fungus. The fungal ball was removed, a double ‘J’ stenting was undertaken and he was treated with amphotericin B and itraconazole. Krishnamurthy et al. [115] pointed out that they had reported a previously healthy patient who had no evidence of immunosuppression who had manifested with an obstructive anuric renal failure due to isolated renal aspergillosis.
Bibler et al. [116] stated that fungus balls of the renal collecting system are rarely of organisms other than Candida. Bibler et al. [116] reported a case of obstructing aspergilloma which was associated with acute ureteral colic. They stated that the clinical features of their reported case were characteristic of renal aspergillomas that had been described in 10 additional cases that had been reported in the literature. They stated that ten of the 11 patients were male. Each of the patients did have an underlying disease which had predisposed to them to having fungal infection. Even though all 11 patients were cured, diagnostic evaluation was often protracted as commoner causes of ureteral obstruction were excluded. Successful treatment of the disease had entailed evacuation of the obstructing hyphal mass; open surgical procedures were necessary in five instances. Bibler et al. [116] recommended that systemic amphotericin B should be reserved for patients who have residual infection following removal of the fungus ball. Bibler et al. [116] stated that their report had emphasized the need to consider aspergilloma in the differential diagnosis of acute ureteropelvic obstruction in the appropriate patient population.
Yoon et al. [117] stated that urinary tract obstructions that had been caused by Aspergillus bezoars had been reported on rare occasions. Yoon et al. [117] reported in their article an unusual case which was caused by an isolate of the Aspergillus nidulantes subgenus, and they also reviewed the literature on 13 additional cases of ureteric obstruction that was caused by renoureteric aspergillosis in order to provide the characteristics of the disease entity. Their reported case manifested with unilateral ureteric obstruction as well as acute renal failure due to Aspergillus bezoars. The patient was stated to be immunocompromised after having received corticosteroid treatment for chronic obstructive lung disease and bronchiectasis. She was successfully treated antifungal chemotherapy including: amphotericin B which was followed by oral voriconazole for about two months and she had percutaneous nephrostomy for one month. The patient’s renal function was reported to have completely recovered after undergoing maintenance haemodialysis for six months.
Shohab et al. [118] stated the following:
- Aspergillosis is primarily a pulmonary disease so that renal aspergillosis usually has tended to be secondary to hematogenous spread from lungs.
- Primary renal aspergillosis, although a rare clinical entity, is still encountered in immuno-compromised individuals.
- Renal aspergillosis might emanate in the formation of focal abscesses, fungal bezoars and might cause ureteric obstruction.
- Treatment does tend to involve stabilization of the patient and removal of fungal bezoars along with administration of anti-fungal agents.
Shohab et al. [118] reported the case of localized primary renal aspergillosis with fungal bezoar formation in a 2 years old immuno-competent child who had manifested with sepsis and acute renal failure and who was successfully managed by nephroscopic removal of fungal bezoar and intravenous voriconazole. The other kidney required nephrectomy for xanthogranulomatous pyelonephritis.
Lee et al. [119] reported a 72-year-old woman who had presented to their emergency room with severe right flank pain that had developed 2 days earlier. She also presented with mild fever, nausea, vomiting, and decreased urine output. She was found to have a non-functioning left kidney and a history of chronic renal failure with usual serum creatinine levels of about 2.0 mg/dl. She was neither a diabetic nor immunocompromised. Her initial blood pressure was recorded as 130/70 mmHg and her body temperature was recorded as 37.2℃. Her clinical examination demonstrated a right costovertebral angle tenderness. The results of her initial blood tests were reported as showing leukocytosis with a white blood cell count of 12,700/mm3 and an elevated creatinine level of 5.8 mg/dl. Her serum glucose level was 102 mg/dl. Her urinalysis revealed haemato-pyuria. She had a non-enhanced CT scan of the abdomen which demonstrated hydronephrosis of her right kidney and atrophy of her left kidney. The CT scan also demonstrated a 7 cm dumbbell-shaped lesion with areas of high attenuation within her dilated right renal pelvis and upper ureter, which had indicated a pelviureteral stone as the cause of the ureteric obstruction (see figure 4). In order to relieve the obstruction of the single functioning kidney, a right percutaneous nephrostomy catheter was inserted upon an emergency basis. She had antegrade pyelography which showed a radiolucent filling defect within her right renal pelvis and upper ureter, which was considered to be the radiolucent stone. The culture of her urine which was drained from the nephrostomy yielded Enterococcus faecalis. Following 2 weeks of her hospitalization, the patient's serum creatinine level decreased to 2.2 mg/dl. Upon ureteroscopy, a movable light yellow "stone" was found within her right upper ureter. Nevertheless, it was not fragmented at all with utilization of an EMS lithoclast and it could not be removed endoscopically. For removal of the obstructive lesion which had been presumed to be a stone, the patient underwent a right pyelotomy, and the large dumbbell-shaped "stone" was removed intact (see figure 5 A). It had a putty-like consistency and it was not firm. Histopathological examination of the removed lesion demonstrated clumps of fungal organisms that were suggestive of Aspergillus (see figure 5C). Furthermore, Gram-positive cocci with calcifications were observed within the specimen. The tissue culture of the specimen had yielded both Aspergillus species and Enterococcus faecalis. Postoperatively, the patient was treated with an additional antifungal agent, itraconazole. The patient did not develop any subsequent urinary tract infections and was well at her 20 months follow-up.
Lee et al. [119] made the ensuing summating discussions:
- Only about 60 cases of fungal bezoars of the urinary tract had been reported. [111] [118] [119] [120]
- The great majority of the fungal bezoar infections of the urinary tract had been associated with Candida species.
- There had been fewer than 20 cases of Aspergillus bezoars of the urinary tract reported by the time of publication of their case. [111] [121].
- Even though almost all aspergillosis in the urinary tract had occurred in patients who had predisposing conditions, such as diabetes mellitus, treatment with immunosuppressive agents or antibiotics, intravenous drug abuse, and malignancy [111] [120] [121] [122], the patient in their reported case had a history of only mild chronic renal failure.
- Additionally, the initial non-enhanced CT scan findings did not raise suspicions of a fungus ball, but rather it gave the impression of a large pelvi-ureteral stone.
- The urine cultures of the patient yielded only Enterococcus species. Therefore, the patient was initially misdiagnosed as having a pelviureteric calculus and an associated bacterial infection.
- In view of its excellence at finding urinary stones and its value for revealing other causes of abdominal pain, non-enhanced helical CT has become the imaging modality of choice for the evaluation of majority of patients who have suspected renal colic [123]
- Nevertheless, early diagnosis of a fungus ball has remained challenging.
- The CT findings of fungal bezoars of the urinary tract are not specific, and they have rarely been described. [111] [124]
- While in the majority of reported cases, radiolucent filling defects could be visualized upon excretory or retrograde urography.
- It was remarkable that in their reported case the fungus ball was observed as a stone-like lesion with high attenuation areas on nonenhanced CT. These findings had seemed to be derived from the encrustations of the fungus ball, in view of the fact that the pathological examination had demonstrated calcifications with bacterial organisms as well as mycelial clumps.
- The development of a fungus ball accompanied by encrustation or even hard stone formation had previously been reported [125], even though no information on the appearance of the fungus ball on CT was reported.
- It is worth taking note of the that fungus balls with encrustations could be visualized as lesions that contain areas of high attenuation, simulating a urinary stone upon non-enhanced CT.
- Of course, in order to establish a diagnosis of fungal infections promptly, a high index of suspicion in certain clinical settings cannot be overemphasized.
- Furthermore, it has been stated that multiple large-volume urine cultures could be necessary to identify Aspergillus, because a single negative culture is insufficient evidence of fungal sterility. [126]
- Some authors had suggested that large fungal bezoars in the upper urinary tract could be managed safely and effectively by endourological methods [127]
- With regard to their reported case; however, pyelotomy was more adequate for the removal of the fungal bezoar completely without causing further damage to the solitary functional kidney.
- Fungus balls within the upper urinary tract that are not too large could be initially treated with antifungal agents prior to the surgery [105] [122]
- In their reported case, antifungal therapy was not considered preoperatively due to the fact that the patient had been misdiagnosed as having a urinary calculus.
Reproduced from: [119]
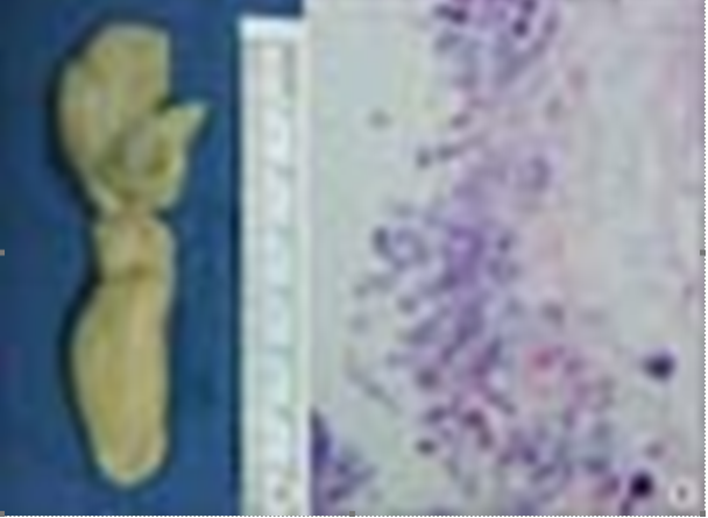
Reproduced from: [119]
Paul et al. [128] stated the following:
- Primary renal aspergillosis is a rare urological entity and immune-compromised persons are commonly prone to it.
- The clinical presentation simulates that of usual bacterial pyelonephritis.
Paul et al. [128] reported a case of localised unilateral renal aspergillosis with obstructive uropathy that was associated with a hypoplastic contralateral kidney in a young man, which had occurred after the endoscopic removal of impacted right upper ureteric calculus in a non-immunocompromised patient. In view of impaired renal function, he was initially managed by means of percutaneous nephrostomy and DJ stent removal which was followed by oral voriconazole treatment for 3 weeks. He responded well to the treatment. Subsequently, the patient was found to be free of renal colic, fever and urine culture negative for Aspergillus.
Ullah et al. [129] stated the following:
- Primary renal aspergillosis, although a rare clinical entity, is still encountered in immune compromised individuals.
- Renal aspergillosis could emanate in the formation of focal abscesses, fungal bezoars and may cause ureteric obstruction.
- Treatment does involve stabilization of patient and removal of fungal bezoars along with administration of anti-fungal agents.
Ullah et al. [129] in their report, stated that they had described the case of localized primary renal aspergillosis with fungal bezoars formation in a 55 years old female, diabetic, hypertensive, who had manifested with upper urinary tract obstruction and she was successfully managed by endoscopic removal of fungal bezoars and intravenous amphotericin followed by oral itraconazole.
Warshawsky et al. [130] stated that the recent increased utilization of steroids, immunosuppressive agents and cytotoxic drugs had been associated with a rise in the incidence of significant fungal disease. Warshawsky et al. [130] reported the first case of bilateral renal aspergillosis without disseminated involvement. Warshawsky et al. [130] stated that a multitherapeutic approach, which included surgical evacuation of masses of hyphae, parenteral antimycotic chemotherapy and topical instillations of amphotericin B, were necessitated in order to clear the kidneys, as well as that newer systemic agents such as 5-fluorocytosine and rifampicin were also utilized.
Pérez-Arellano et al. [122] stated the following:
- In their article they had described a case in which acute renal colic was found to be associated with elimination of multiple hyphal masses of Aspergillus flavus.
- Also, they had reviewed the literature on similar cases and they had found a similar pattern which was characterized by a marked male predominance, association with at least one underlying medical condition which predisposes the individual to fungal infection, the presence of local symptoms mimicking acute ureteral colic, and the absence of systemic manifestations.
- Moreover, their data had suggested that Aspergillus balls should be suspected when a diabetic and intravenous drug user manifests with acute renal colic and that non-obstructive renal aspergillosis might be initially treated with itraconazole.
Chang et al. [131] stated that even though rare, aspergillosis could cause obstructive uropathy and that this generally does tend to occur in patients who have immunosuppressive conditions. Chang et al. [131] reported the case of aspergilloma that caused ureteric obstruction in a 79-year-old man who had no immunosuppressive conditions. He had a computed tomography scan which demonstrated that his left pelvicalyceal system and ureter had shown mild dilation, without a definite obstructive lesion. The fungal bezoar was removed utilizing ureteroscopy. The patient was successfully treated with antifungal medicament.
Sivasubramanian et al. [132] stated the following:
- Urinary tract aspergillosis is not common even in the era of increased frequency of invasive mycoses.
- Experience related to urinary tract aspergillosis is largely a function of isolated case reports and rare case series or reviews.
- Most of the cases do tend to involve transplant recipients predominantly following renal transplantation but it has also been in other immunocompromised states such as AIDS and uncontrolled diabetes mellitus.
- Majority of cases of urinary tract aspergillosis represent haematogenous spread to renal parenchyma, often in the absence of recognized disseminated infection, manifesting as small or large abscesses, infarcts, renal insufficiency or urinary drainage system fungal balls with obstructive uropathy.
- Diagnosis of urinary tract aspergillosis usually tends to be made on the basis of renal tissue aspiration and urine cultures.
- Newer anti-Aspergillus medications notably voriconazole does offer less toxic treatment options and are quite successful in combination with drainage measures that are undertaken to relieve urinary stasis.
Devisoglu et al. [133] reported a 70-year-old man who was had diabetes mellitus and who had manifested with acute obstructive non-oliguric renal failure. He had a CT-scan of abdomen which revealed obstructive hydronephrosis and irregular thickening of the wall of his urinary bladder. He underwent cystoscopy, and samples of tissue were taken for pathology examination and they were found to be positive for Aspergillus spp. on histology, which had indicated infection of the urinary bladder wall. The patient was treated successfully by means of a percutaneous nephrostomy as well as a 30-day course of caspofungin.
Nain et al. [134] stated that ureteric aspergilloma is an uncommon cause of ureteric colic as well as ureteric obstruction. Nain et al. [134] reported a rare entity in a 58-year-old man who had manifested with abdominal pain. The case was stated to be that of unilateral ureteric aspergilloma in a middle-aged man. He underwent ureteroscopy which revealed yellow pus like ball that was removed and submitted for pathology examination. To their surprise histopathology examination of the specimen revealed features that confirmed the diagnosis of aspergilloma. The patient underwent treatment with voriconazole.
Eisenberg et al. [135] reported a case of aspergillosis of the kidney which could not be attributed to any of the factors that classically predispose to fungal infection (immunosuppressive, antibiotic or steroid therapy and diabetes). The patient was reported to have severe obstruction of the ureteropelvic junction, which, the authors believed had caused stasis of urine and, in turn, the propagation of a colony of Aspergillus.
Maquera-Afaray et al. [136] stated that primary renal aspergillosis is not common and mainly does affect people who have immune system impairment and/or genitourinary disease. Maquera-Afaray et al. [136] reported the case of a male new-born child with Down syndrome and congenital heart disease, who had undergone surgery for anorectal malformation and who manifested with persistent fever and impaired kidney function secondary to kidney abscesses due to Aspergillus. The reported patient responded favourably to antifungal treatment and percutaneous drainage but the child died following heart surgery. Maquera-Afaray et al. [136] made the following conclusions:
- To the best of their knowledge, only seven cases of renal aspergillosis had been reported in children worldwide by the time of publication of their case, and their reported case was the second in a new-born child.
- Aspergillus species should be considered among the fungal etiological agents of genitourinary tract infections in order to establish adequate antifungal treatment to achieve therapeutic success against filamentous fungi.
Singal et al. [137] stated the following:
- Fungal infections of the urinary tract usually tend to be encountered pursuant to prolonged antibiotic utilization, instrumentation and indwelling urinary catheters. Candida is the most frequent causative fungus.
- Nevertheless, infections with Aspergillus flavus had been reported previously in immune-compromised hosts.
Singhal et al. [137] reported a 32-year-old immunocompetent man who was diagnosed to have urinary tract infection caused by Aspergillus flavus following instrumentation for the removal of a ureteric stone. The infection was symptomatic, and it was associated with abdominal pain and subsequent passage of fungal masses per urethra. Patient was treated successfully with a prolonged course of broad-spectrum antifungal agent itraconazole.
Songkhla et al. [138] stated the following:
- Aspergillosis is an infectious disease that is caused by pathogenic mold in Genus Aspergillus which is common in immunocompromised individuals especially in neutropenic patients.
- Nevertheless, aspergillosis in immunocompetent hosts has been considered to be uncommon and renal aspergillosis in immunocompetent patients is a rare clinical entity.
- Songkhla et al. [138] reported a case of right renal aspergillosis which was predisposed to by renal instrumentation. The patient responded well with systemic voriconazole and stent removal.
Park et al. [139] stated the following:
- Invasive aspergillosis (IA) is a leading cause of infectious mortality in patients who have undergone a hematopoietic stem cell transplant (HSCT); the mortality due to IA has ranged from 70% to 93% in HSCT patients.
- Early diagnosis and treatment represent the cornerstones for the good prognosis of IA.
- Primary renal aspergillosis is an extremely rare manifestation in patients who have undergone HSCT, and the risk factor for this uncommon manifestation is not well known.
Park et al. [139] reported a patient who had developed primary renal aspergillosis and renal stones in both the kidneys following HSCT. Invasive renal aspergillosis was diagnosed after the patien t had undergone a nephrectomy, which was undertaken to treat massive renal hematoma
Vuruskan et al. [140] stated the following:
- Mycotic infections in various organ transplant recipients do represent severe and often fatal complications.
- Aspergillosis which is isolated from the urinary tract does tend to occur quite infrequently in renal transplant recipients.
- Besides, fungus balls are rare causes of ureteral obstruction.
Vuruskan et al. [140] reported a 51-year-old patient who had a diagnosis of ureteric obstruction which was caused by aspergillosis in the early post-renal transplant period, who unfortunately died with the clinical picture of disseminated infection and its complications.
Meng et al. [141] stated that renal aspergillosis (RAsp) is a rare complication in liver transplant (LT) recipients. Meng et al. [141] reported RAsp in two LT recipients. They iterated that in both patients, RAsp had occurred more than 90 days pursuant to allogenetic orthotropic LT, and all the clinical findings were unspecific. RAsp had involved unilateral kidney in Case one and bilateral kidneys in Case two. Both computed tomography (CT) and magnetic resonance imaging (MRI) imaging scans had revealed renal abscesses, with progressively enhanced walls and separations and unenhanced alveolate areas post contrast agent administration. Upon unenhanced CT images they demonstrated inhomogeneous hypo-attenuation. On fat-suppressed T2-weighted images (T2WIs), the walls and separations of the abscesses had shown slightly low signal intensity and the central parts of the lesions had shown slightly high signal intensity. Both on CT and MRI scans, there were some hints of renal infarction or chronic ischemia. Both patients were treated by radical nephrectomy which was followed by adjuvant antifungal therapy. Both patients recovered well. Meng et al. [141] summated the following as core tips:
- Their paper had reported renal aspergillosis (RAsp) in two liver transplant (LT) recipients more than 90 days after they had received allogenetic orthotropic LT, and they had described the computed tomography and magnetic resonance imaging manifestations of renal lesions, including the abscesses and surroundings.
- The findings in their report might help improve the diagnosis of RAsp.
- After undergoing radical nephrectomy which was followed by adjuvant antifungal treatment, both patients had recovered well without mortality from Rasp
Sadagah et al. [142] reported a 29-year-old Saudi man who had had a recent living non-related kidney transplantation in Pakistan. His early post-transplantation course was complicated by acute cellular rejection (Banff Class IB) which had been managed successfully with utilization of pulse steroid and anti-thymocyte globulin. The patient represented to the emergency room of the authors on the fortieth day pursuant to his transplantation with a complaint of decreased urine output and passing white particles in his urine. This manifestation was three weeks following his treatment for cellular rejection, his urine fungal culture demonstrated a growth of Aspergillus fumigatus, and he had ultrasound radiology imaging of his allograft kidney which demonstrated mild to moderate hydronephrosis with echogenic materials within the renal pelvis. Biopsy of the transplanted kidney was undertaken and pathology examination of the biopsy specimen revealed features of severe necrotizing granulomatous inflammation and fungal elements which were consistent with aspergillus species. The patient was treated with voriconazole as an antifungal agent and he was weaned from immunosuppressive medicament. The patient eventually did require intermittent haemodialysis and he underwent surgical allograft nephrectomy.
Sadagah et al. [142] made the ensuing conclusions:
- Suboptimal environmental and infection prevention and control precautions could explain this type of infection.
- It is important for clinicians to have a high index of suspicion and to investigate for fungal infection as a rare cause of obstructive uropathy in high-risk patients.
Sharmin et al. [143] made the ensuing iterations related to Aspergillosis of the urinary tract:
- Urinary tract aspergillosis is not common even in the era of increased frequency of invasive mycoses.
- Experience has been largely from isolated case reports and few case series or reviews.
- Most of the majority of cases that had been reported had involved transplant recipients predominantly following renal transplantation but it had also been reported in other immunocompromised states such as AIDS and uncontrolled diabetes mellitus.
- Majority of cases had represented haematogenous spread to renal parenchyma, often in the absence of a recognized focus of infection, manifesting as small or large abscesses, infarcts, renal insufficiency or urinary drainage system fungal balls with obstructive uropathy.
- Diagnosis of aspergillosis of the urinary tract usually had tended to be made upon the basis of renal tissue aspiration, urine cultures or by histopathology of the suspicious mass which had been passed through urinary tract.
- The effective management of invasive aspergillosis had tended to include strategies to optimize prevention and early antifungal treatment, immunomodulation, and, in some instances, the undertaking of surgery.
- Newer anti-Aspergillus medications notably voriconazole do tend to offer less toxic treatment options and they have tended to be quite successful in combination with drainage measures to relieve urinary stasis.
Sharmin et al. [143] reported a case of primary urinary tract aspergillosis with fungal bezoars formation in a 37years old woman, diabetic, hypertensive, who had manifested with intermittent urinary tract obstruction and who was successfully managed by oral voriconazole for six weeks as itraconazole was found refractory.
Albin et al. [144] reported a 68-year-old man who had type 2 diabetes mellitus, coronary artery disease, and CLL, who had manifested with progressive generalized weakness, unintentional 35 lb weight loss, right flank discomfort, bladder spasms, as well as urinary retention over the preceding 3 months. She was diagnosed as having chronic lymphocytic leukaemia (CLL) 11 years earlier. His treatment was initially bendamustine plus rituximab, and the treatment was then changed to ibrutinib; he received venetoclax monotherapy for the preceding one year, which stabilized his disease. The evaluation of his symptoms over the 3 months preceding his admission had included repeated urinalyses which showed evidence of sterile pyuria and 6 repeated urine cultures for bacteria which had not yielded any growth. He had computerized tomographic (CT) scan which demonstrated right nephromegaly, hydronephrosis, and perinephric fat stranding. He next had a positron emission tomography CT (PET CT Scan) which demonstrated no abnormal extrarenal fluorodeoxyglucose-uptake and absent function of the right kidney. He subsequently underwent cystoscopy with retrograde pyelography which had shown resolved collecting system dilatation and no filling defects or endoscopic abnormalities. Prior to his admission, he had undergone treatment with multiple courses of oral antibiotics, intermittent straight catheterization, and dose reduction of venetoclax without any obvious clinical improvement. During his hospital admission, his clinical examination demonstrated that he was a frail, cachectic-appearing man who had a temperature of 97.7o F. His abdomen, upon palpation, was non-tender, and there was no suprapubic or costovertebral angle tenderness. The results of his laboratory studies were reported to have demonstrated a white blood cell (WBC) count of 8100 cells/μL with absolute neutrophil count of 7200 cells/μL and lymphocyte count of 580 cells/μL, hemoglobin 7.4 g/dL, and creatinine 1.3 mg/dL. His urinalysis revealed too numerous to count WBC and many red blood cells. His Westergren erythrocyte sedimentation rate was recorded as 108 mm/hour, and his C-reactive protein level was reported to be 18.5 mg/dL. He had a non-contrast CT scan of his abdomen and pelvis which had had illustrated persistent hydroureteronephrosis with perinephric fat stranding and patchy hypoattenuation of the right kidney. His three post-admission bacterial urine cultures had remained without any growth. He underwent cystoscopy with right ureteric catheterization which yielded purulent material, and a double-J ureteric stent was inserted. Bacterial, fungal, and mycobacterial cultures were sent to the laboratory from this purulent material, and a green mold was found upon the Sabouraud’s dextrose agar after 2 days; several days later, this was identified and confirmed as Aspergillus fumigatus. He was commenced on treatment with voriconazole at a dose of 200 mg every 12 hours after a loading dose of 400 mg every 12 hours on the first day, and venetoclax was stopped. A right percutaneous nephrostomy tube was inserted through which 30 mL amphotericin B deoxycholate (25 mg suspended in 200 mL sterile water) was instilled to filter dependently through his ureterovesicular axis every 8 hours. His serum beta-D-glucan level was greater than 500 pg/mL and his serum galactomannan was 6.33 units. No other sites of disseminated Aspergillus infection had been found.
Following 2 weeks of his antifungal treatment, he had CT scan of abdomen and pelvis which showed progression of his disease, with enlarging hypoechoic lesions within the inferior perinephric region and a 4.8-cm abscess within the prostate gland (see figure 6). He underwent cystoscopy, trans-urethral deroofing of the prostatic abscess, and suprapubic tube insertion. A fungal ball which was found to be adhering to the ureteric stent was removed. Histopathology examination of his prostate specimens revealed necrosis as well as abundant septate hyphae

One week subsequently, he underwent en bloc nephrectomy and excision of the percutaneous nephrostomy tract. The right kidney was found to be markedly enlarged, and multiple casts which had been composed of hyphae were extracted from the patient’s right proximal ureter. Macroscopy pathology of the specimen demonstrated a diffusely necrotic and purulent kidney without any viable parenchyma; histopathology examination of the surgical specimen demonstrated necrosis and abundant septate hyphae (see figure 7). His Voriconazole treatment was continued with marked clinical improvement; the levels of his serum galactomannan and beta-D-glucan had decreased to 0.05 units and undetectable, respectively, following 9 months of his treatment.
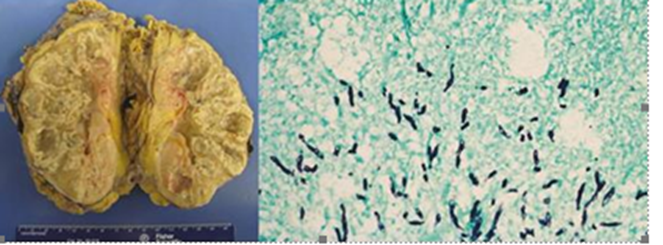
Reproduced from: [144]
Albin et al. [144] made the ensuing conclusions:
- Primary genitourinary aspergillosis is an uncommon presentation of invasive aspergillosis, affecting renal and prostatic parenchyma in addition to the genitourinary collecting system.
- Management of primary genitourinary aspergillosis tends to be made difficult by poor urinary levels of existing antimold agents and the immunocompromised status of the affected hosts.
- Invasive fungal infections do remain uncommon in CLL relative to other haematological malignant tumours; nevertheless, the introduction of novel targeted treatments had altered the spectrum and frequency of infections in this population.
- Ongoing surveillance for opportunistic infections, such as that noted in their reported patient, is warranted in patients who are receiving venetoclax.
Mousavi et al. [145] stated the following:
- Renoureteral aspergillosis following ureteroscopic lithotripsy and insertion of ureteral stent is an uncommon clinical entity.
- Due to inadequate sterilization of the instrument during the ureteroscopy and
- insertion of ureteric stent, a localized aspergillus infection might occur which
- might cause pyuria, ureteric obstruction, perinephric abscess as well as hydronephrosis.
Mousavi et al. [145] reported a case of unilateral ureteric obstruction which was caused by Aspergillus terreus following ureteroscopy lithotripsy in a 45-years-old diabetic man. He manifested with the complaint of passing whitish soft mass along with urine and hydronephrosis in his left kidney. Three months prior to his hospital admission, he had
undergone ureteroscopy lithotripsy for removal of stone and a ureteric stent (DJ catheter) had been inserted for 3 weeks. However, in view of abnormal discharge and persistent obstruction the ureteric stent was changed and he was prescribed antibiotics for some time. As he had not responded to his antibiotic treatment, he underwent retrograde pyelography and removed the ureteric stent and a new ureteric stent was inserted. Within his ureteric washing and urine specimen, whitish soft materials were found to be visible and a mesh of fungal hyphae were seen in direct microscopy exam and culture in SDA yielded growth of Aspergillus terreus. He was treated initially with itraconazole; nevertheless, it was stopped after 25 days in view of the persistent whitish mass within his urine as well as in view of his other sign and symptom. The isolate was reported to be susceptible to caspofungin (0.038 lg ml1), posoconazole (0.032 lg ml1), itraconazole (0.032 lg ml1) and voriconazole (0.023 lg ml1) in E-test antifungal susceptibility test. The endoscopic removal of fungal mass was done and Martínez-Girón et al. [146] stated that urinary bladder aspergillosis is an unusual infection. Martínez-Girón et al. [146] reported the case of a 79-year-old man who had clinical records of transitional cell carcinoma diagnosed 5 years preceding his manifestation. The presence of a fruiting body and septate hyphae within his urine cytological smears were the key for a final diagnosis of fungal bladder infection caused by Aspergillus niger. Hameed et al. [93] reported a 52-year-old man who had presented to surgery emergency department of the authors with acute retention of urine for 12 hours. He had also complained of progressive dysuria and visible haematuria together with low-grade fever for the preceding 15 days. He had a history of lower urinary tract symptoms (LUTS) over the preceding 6 months. He was a shopkeeper by occupation, and he did not have any known comorbidities or significant family history. Upon his clinical examination, he was found to be febrile with enlarged prostate on digital rectal examination and a palpable bladder per his abdominal examination. A Foley catheter was inserted, and bladder irrigation with diluted povidone iodine was commenced after obtaining urine samples. Examination of his urine revealed his urine was full of RBCs (>50/high power field) and pus cells (>20/hpf). His urine culture was sterile. His White Blood Cell counts were 12,000/microlitre with absolute eosinophil count of 850. His blood sugar charting was deranged with fasting blood sugar of 174 mg/dL and post-prandial blood sugar level of 228 mg/dL. His HbA1c level was 11.2 g%. He was previously unaware of his diabetic mellitus status. He had ultrasound scan (USG) of abdomen which demonstrated hyperechogenic contents within his urinary bladder and thickened urinary bladder wall ~7 mm (see figure 8); both of his kidneys lookd normal with no evidence of any abnormal echogenic focus or hydronephrosis.
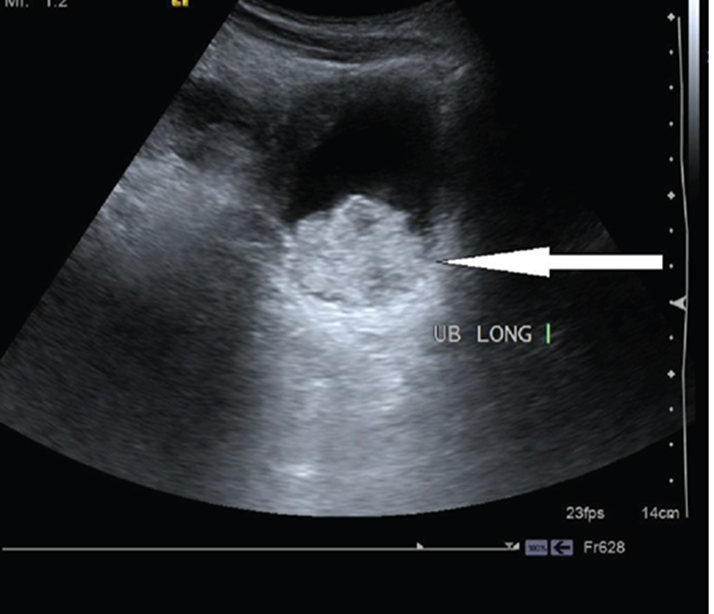
In order to ascertain the cause of the patient’s acute retention of urine, haematuria, and LUTS, patient underwent cystoscopy which demonstrated membranous urethritis, median lobe prostatic enlargement, as well as white fluffy cotton-like balls in his urinary bladder (see figure 9). His urinary bladder wash fluid was sent for both bacterial and fungal culture, and fluffy balls were sent for histopathology examination (HPE). HPE demonstrated fungal hyphae which were septate with acute angle branching and PAS stain positivity of the specimen was indicative of Aspergillus (see figure 10). No growth was identified upon Sabouraud’s dextrose agar inoculation of the urinary bladder wash fluid. To screen the patient for immunodeficiency, an enzyme immune assay test for HIV 1 and 2 was undertaken and found out to be negative. Additional tests for confirmation of Aspergillus-like galactomannan antigen and β-D-glucan were not undertaken due to the financial constraints for the patient. The patient was treated with systemic voriconazole and his urinary bladder irrigation with diluted povidone iodine. He was asymptomatic after 14 days of treatment. He underwent check cystoscopy after 4 weeks, which revealed that his urinary bladder and urethra were normal without any evidence of fungal balls.
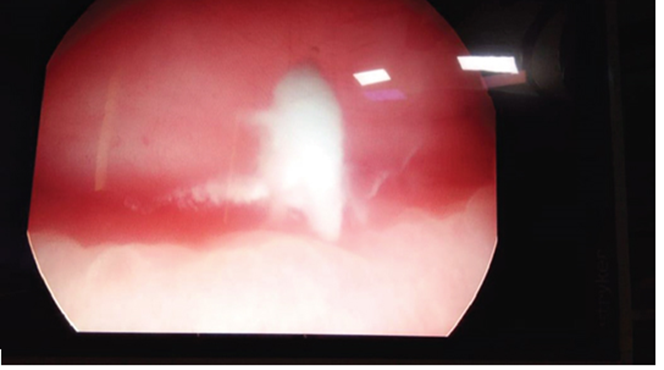
Hameed et al. [93] made the following conclusions:
• Fungal infections of the urinary tract even though they tend to be rare should always be kept in mind as a differential diagnosis in patients who have persistent urinary tract infection (UTI).
• In case of sterile pyuria with lower urinary tract symptoms, fungal cystitis should be taken into consideration as a possible diagnosis.
• Early diagnosis and complete treatment are required in order to control the dissemination of disease and to have a favourable prognosis.
• Fungal balls very rarely could also cause acute retention of urine in the setting of severe lower urinary tract symptoms.
Gowardhan et al. [147] described the pathology of a unique case of fallopian tube aspergillosis in a 45-year-old woman. She manifested with lower abdominal pain and lump within her lower abdomen over the preceding 2 months to 3 months. Clinically she was diagnosed as having a benign ovarian tumour which had had involved her right ovary. Macroscopy pathology examination of her excised lesion demonstrated dilated fallopian tube containing yellow material. Microscopy pathology examination of the excised specimen revealed Aspergillous filaments which were surrounded by dense infiltrate of neutrophils and lymphocytes. Prashant et al. [147] stated that although Aspergillous salpingitis is a rare entity, the correct diagnosis is of great importance for the indication of proper treatment.
Kim et al. [148] stated that common clinical manifestations of aspergillosis in renal transplant recipients include fever and pulmonary infiltrates; however, involvement of the reproductive system is rare. Kim et al. [148] reported a case of pelvic aspergillosis with tubo-ovarian abscess in a renal transplant patient. The patient had received a cadaveric renal transplantation, and two episodes of acute rejection which he had developed were treated with methylprednisolone pulse therapy. Surgical biopsy specimens of pelvic abscess were detected by ultrasonogram and CT revealed Aspergillus. The patient underwent treatment with amphotericin B, and at the time of the report of the case, the patient was well with normalization of erythrocyte sedimentation rate and C-reactive protein.
Borsa et al. [149] stated the following:
- The vast majority of vaginal fungal infections tend to be caused by Candida species.
- Nevertheless, vaginitis cases that are caused by molds are very rare.
- Aspergillus protuberus had been previously known as a member of Aspergillus section Versicolores which could cause opportunistic infections in immunocompromised patients; nevertheless, it had recently been described as a separate species.
- Even though the members of Aspergillus section Versicolores had been isolated rarely in cases of pulmonary infections, eye infections, otomycosis, osteomyelitis and onycomycoses, to the best of their knowledge, there had been no published case of human infection caused by Aspergillus protuberus.
- In their report, the first case of persistent vaginitis due to Aspergillus protuberus in an immunocompetent patient was presented.
Borsa et al. [149] reported a 42-year-old female patient who was admitted to their hospital with the complaints of pelvic pain, vaginal itching and discharge during one month. Her symptoms had been persistent despite treatment with miconazole nitrate and clotrimazole therapies for a probable candida vaginitis. Microscopy examination of her cervical smear demonstrated fungal structures such as branched, septate hyphae together with the conidial forms. Thereafter, a vaginal discharge sample was taken for microbiological evaluation and similar characteristics of fungal structures were found in the microscopic examination as was observed within her cervical smear. Then, preliminary result was reported as Aspergillus spp. At the same time, the sample was plated on Sabouraud dextrose agar (SDA) in duplicate and incubated at room temperature and at 37°C. After 5 days, white, powdery and pure-looking fungal colonies were found in SDA which was incubated at room temperature, while the other medium had remained sterile. The culture was submitted to the CBS-KNAW Fungal Biodiversity Center for further characterization. Phenotypic identification demonstrated that the isolated strain had belonged to the Aspergillus section Versicolores. The strain was grown for 7 days upon malt extract agar and then ITS regions were amplified and sequenced from isolated DNA for genomic characterization. The obtained sequences were compared with the NCBI database and internal databases of the CBS-KNAW Fungal Biodiversity Centre and confirmed as Aspergillus section Versicolores. As a result of recent changes in classification of fungi, analysis of partial β-tubulin and calmodulin sequences had also been utilized in order to obtain a detailed and precise characterization. Eventually, the strain had been identified as Aspergillus protuberus which was documented to be a recently accepted species that is distinct from Aspergillus section Versicolores. As the patient could not be contacted following receipt of the preliminary report, detailed demographical information, probable origin and route of transmission of the agent and prognosis of infection had remained obscure. Borsa et al. [149] concluded that the first case of vaginitis which is caused by Aspergillus protuberus was described in the report with the support of clinical, pathological, microbiological and molecular data.
Elad et al. [150] stated that Aspergillus terreus was isolated from organs of a German Shepherd pup which was removed from the bitch by caesarean intervention. During the ensuing days the bitch developed signs of canine disseminated aspergillus and it was euthanized. The fungus was isolated from a necrotic lesion within the uterus and other organs. Elad et al. [150] stated that to the best of their knowledge, their reported case was the first report of trans-uterine transmission of Aspergillus terreus during a case of canine disseminated aspergillosis.
Babrel et al. [151] stated the following:
- An Aspergilloma is referred to as Mycetoma or fungus ball.
- Aspergillus spp refers to a fungus which is known to cause acquired and nosocomial infections in human beings. Isolated Ovarian Aspergillosis as well fungal infections of ovary are very rare.
- Aspergillus fumigatus, is the most commonly infecting species.
- Anti-fungal prophylaxis should be provided to high-risk patients.
- Posaconazole is often administered as prophylaxis in immunocompromised patients.
Babrel et al. [151] reported a 50-year P2L2 postmenopausal woman, who presented with pain in her lower abdomen over the preceding 6 months. She also had a history of loss of weight (10kgs) over the preceding 1 year. Her medical and surgical history were not contributory. Upon her per vaginal examination, her uterus was found to be atrophic retroverted with restricted mobility. A vague non tender cystic to firm mass was felt within her left adnexa which was not separate from the uterus and her right fornix was free. Her blood investigation including CA125 was within normal range. She had ultrasound scan which was reported to be suggestive of complex cystic lesion with fine septations and thick internal echoes that were noted within her left adnexa and within her pouch of Douglas, calcifications were found. Her left ovary could not be seen separately from the mass. The rest of her abdomen and pelvis was normal. She had a computed tomography (CT) scan of abdomen pelvis which showed a left complex ovarian cyst. A clinical diagnosis of TO mass was made. She underwent exploratory laparotomy which demonstrated a left side tuboovarian mass which was excised. Upon histopathological examination of the excised mass, the left ovary was found to be showing dense xanthogranulomatous inflammation with suppurations, eosinophilic abscesses and fungal hyphae with septae and branching which resembled Aspergillosis. Babrel et al. [151] concluded that fungal infection of ovary is an extremely rare entity, while treating infective ovarian pathology they must consider antifungal treatment with antibacterial treatment.
Walker et al. [152] stated that an intact bitch with a history of mating was presented with severe lameness and a vulvar discharge. A mixed lytic, proliferative tibial lesion and open pyometra were diagnosed. Bone biopsy and uterine culture demonstrated disseminated aspergillosis. Walker et al. [152] stated that their reported case was the first report of Aspergillus pyometra with dissemination following mating in the dog.
Gupta et al. [153] stated the following:
- Fungi represent ubiquitous organisms and they significantly alter the post-transplant course.
- They are a major cause of morbidity and mortality and more so within developing countries.
Gupta et al. [153] studied the clinical profile, aetiology, risk factors, treatment, and outcome of fungal infections in post-renal transplant recipients. The study was a cross-sectional observational retrospective study which started from January 2014 to June 2017 wherein renal transplant recipients with invasive fungal infection were included and they were followed-up. With regard to the results, Gupta et al. [153] reported the following:
Amongst 550 renal transplant recipients, 56 (10.2%) patients had developed invasive fungal infection. The mean age of the patients was 40.61 ± 10.06 (13-66) years and mean duration of acquiring infection post-transplant was 25.33 ± 23.65 (1-96) months. The male to female ratio was 3:1. Fever was the commonest manifestation observed in 89.3% of the patients. Cough (76.8%), breathlessness (64.3%), sputum (55.3%), hypoxia (50%), and haemoptysis (10.7%) were the other common clinical symptoms at manifestation. The mean serum creatinine at presentation was 1.70 mg/dl. The commonest invasive fungal infection that was isolated was Mucormycosis 15 (26.7%), which was followed by Aspergillosis 13 (23.2%), Pneumocystis jiroveci 12 (21.4%), Cryptococcus 6 (10.7%), Candida 4 (7.1%), Histoplasmosis 3 (5.3%), Phaeohypomycosis 2 (3.5%), and 5 (8.9%) patients did have undetermined fungal aetiology. Twenty (35.7%) of the patients had evidence of dual infection. Utilization of antithymocyte globulin 27 (48.2%), post-transplant diabetes mellitus 18 (32.1%), Cytomegalovirus (CMV) infection 16 (28.5%), anti-rejection therapy 9 (16%), and Hepatitis C infection 7 (12.5%) were identified as risk factors. Ten (17.8%) of the patients had graft loss and 12 (21.4%) of the patients died in the study period. Gupta et al. [153] concluded that invasive fungal infection is a serious threat to renal transplant recipients and that patient and graft survival was significantly affected by fungal infection in the developing world.
Gupta et al. [154] reported a 59-year-old man who had well controlled type-2 diabetes mellitus and who had presented to the emergency department of their hospital with fever, abdominal pain as well as acute kidney injury (AKI). The results of his laboratory evaluation were reported as follows: Hemoglobin (Hb) 13.6 gm/dL, total leucocyte count (TLC) 8,250 cells/cm3 with 85% neutrophils with platelets 1,39,000 lakh/cu.mm and raised creatinine (4.60 mg/dL). Blood and his urine culture grew carbapenem resistant Klebsiella pneumoniae (CR KP) which was suggestive of complicated urinary tract infection (UTI) with bacteraemia. The patient was commenced on polymyxin-E combination therapy. He had ultrasound scan (USG) of his abdomen which demonstrated left grade-2 hydroureteronephrosis with right renal concretions. He had computed tomography (CT) scan which demonstrated a small left lower ureteric calculus which causing mild-moderate left hydroureteronephrosis. On the polymyxin and meropenem combination therapy, the patient clinically improved and he had a repeat blood culture which did not yield any growth but the patient was found to be persistently febrile. There was a progressive increase in his peripheral TLC to 16860 cells/cm3 and increase in the level of his C-reactive protein (CRP) to 321 mg/L. Infectious Diseases (ID) consultation was sought at that point. A review of his medical and surgical history had revealed that the patient had earlier on undergone a urological procedure for stone removal with insertion of a double-J (DJ) ureteric stent into his left kidney 7 months preceding his admission, in another institute. A few days after the procedure, he had developed fever with flank pain and admitted into hospital in view of his development of complicated urinary tract infection (UTI) with CR KP. He had ultrasound scan of renal tract (USG KUB) which revealed an evolving abscess within his left kidney with right kidney pyelonephritis. He had renogram in the form of 99m Tc-DTPA renogram which demonstrated that his renal function study was suggestive of impaired perfusion and cortical uptake in the right kidney and hydronephrosis, obstruction and impaired cortical function of the left kidney. In view of the hydronephrosis, a percutaneous nephrostomy was inserted into his left kidney and the bilateral DJ stents were removed and replaced. Cultures were not repeated at that point. He had a magnetic–resonance (MR) urography undertaken, one month later which demonstrated filling defects and bilateral renal cortical cysts. He underwent cystoscopy with bilateral retrograde pyelogram with ureteroscopy and bilateral nephroscopy removal of slough material. Both of his right and left renal calyceal slough material, on histopathology examination showed amorphous material along with numerous fungal hyphae which were noted to be slender, septate with acute angled branching. Culture of the amorphous material grew Aspergillus flavus. The patient subsequently received voriconazole for a period of 2 months. He did not have a repeat radiology imaging before stopping his antifungal treatment. Subsequently, the patient became asymptomatic for subsequent 3 months until when he was admitted again with complicated urinary tract infection (UTI) with CR KP. In view of his left-sided grade II hydroureteronephrosis, a percutaneous nephrostomy (PCN) tube was inserted. The cultures and histopathology from the nephrostomy specimen were found to be negative this time for Aspergillus. Nevertheless, based upon his recent past medical history, a diagnosis of relapse of urinary tract aspergillosis was considered. He was commenced on amphotericin-deoxycholate (AmB-d) (1.0 mg/kg/day) and 5-flucytosine (5-FC) in renally modified doses. The patient responded well to this treatment and he became afebrile. The percutaneous nephrostomy (PCN) tube was removed after 2 months which was followed by the removal of the DJ stents. The combination antifungal therapy was administered for a period of 3 months with close monitoring of the patient’s renal function and the treatment was discontinued following clinical and microbiological cure along with radiological stability. The patient had been doing well at his 5-year follow up.
Gupta et al. [154] made the following conclusions:
- •Post-urosurgical aspergillosis is a life threatening and rare manifestation of invasive aspergillosis.
- •Post-Urosurgical aspergillosis does require a high index of clinical suspicion particularly in patients who present with urinary tract infection (UTI) as well as obstructive uropathy pursuant to undergoing an invasive genitourinary procedure.
- This does have implications for sending appropriate intra-operative specimen for fungal cultures as well besides the histopathology.
- The achievement of successful outcome does depend upon a combined surgical and medical approach with good effective source control and appropriate mold-active antifungal agents achieving effective urinary levels for the right duration of time.
- Good infection control practices with high-level disinfection with 2% glutaraldehyde or plasma sterilization does need to be emphasized the for prevention of nosocomial fungal infections.
Conclusions:
- Aspergillosis, though rare, can afflict different organs of the body including the kidney as well as male and female urogenital tract.
- The symptoms associated with aspergillosis of the kidneys as well as the male and female urogenital tract tend to be non-specific and hence a high index of suspicion is required in order to diagnose this rare infection as well as to avoid misdiagnosis of the infection as bacterial infection or other disease.
- Treatment of aspergillosis of the kidney and the urogenital tract does entail utilization of an appropriate aspergillosis sensitive antifungal medication as well as excision of the lesion to remove the aspergillus aspergillum to prevent extension of the infection
- Appropriate long-term period of follow-up of patients who have undergone treatment of aspergillosis of the kidney and urogenital tract organ is required to pick up any recurrent lesion.
- The predisposing factors for the development of aspergillosis of the kidney and the urogenital tract of both males and females should be well known by all clinicians in order to establish an early diagnosis of this rare infection.
Conflict of interest
None
Acknowledgements:
Acknowledgements to:
[1] Urology Case Reports and Elsevier for granting permission for reproduction of their figures and journal articles under Copyright © 2022 The Authors. This is an open access article under the CC BY-NC-ND license http://creativecommons.org/licenses/by-nc-nd/4.0/.
In other words, Elsevier has granted copyright permission which stated the following: This article is available under the Creative Commons CC-BY-NC-ND license and permits non-commercial use of the work as published, without adaptation or alteration provided the work is fully attributed. For commercial reuse, permission must be requested below.
[2] Case Reports in Urology and Hindawi Publishing Limited for granting copyright permission under copy right: Copyright © 2020 Tariq Hameed et al. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
[3] The Korean Journal of Urology which is now through a change of name is now called: based upon Journal title changes from Korean Journal of Urology to Investigative and Clinical Urology and the Korean Urological Association for granting permission for reproduction of contents and figures from their Journal article under copy Right.
[4] Open Forum Infectious Diseases and the Oxford University Press and their Associated Groups for granting Copy Right Permission for reproduction of figures and contents of their Journal article under copyright Creative Commons. This is an open access article distributed under the terms of the Creative Commons CC BY license, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited. You are not required to obtain permission to reuse this article.
References
- Zhou L, Zhao H, Chen Z, Zhu L. (2017). Urinary tract aspergillosis in a patient with chronic kidney disease. BMJ Case Rep. bcr2017221638.
View at Publisher | View at Google Scholar - Patterson TF, Thompson GR 3rd, Denning DW, Fishman JA, Hadley S, et al. (2016). Practice Guidelines for the Diagnosis and Management of Aspergillosis: 2016 Update by the Infectious Diseases Society of America. Clin Infect Dis. 63(4): e1-e60. EPub.
View at Publisher | View at Google Scholar - Baggish MS, Ventolini G. (2008). Vulvovaginal colonization by Aspergillus species in nonimmunocompromised women. Journal of Gynecologic Surgery24(2):55-60.
View at Publisher | View at Google Scholar - de Misa RF, Castro V, Suárez J, Perera A. (2000). Pruritic vulvar nodule in a black woman. Archives of Dermatology. 136(9):1165-1170.
View at Publisher | View at Google Scholar - Deb P, Srivastava A. (2009). Aspergillus in a cervico-vaginal smear of an adult postmenopausal female: An unusual case. Journal of Cytology/Indian Academy of Cytologists. 26(3):123 – 124.
View at Publisher | View at Google Scholar - GuPtA P, GoyAl S, KAuShAl M. (2016). Concomitant aspergillus species infection and squamous cell carcinoma diagnosed on Pap smear. Turk Patoloji Derg. 32(1):54-56.
View at Publisher | View at Google Scholar - VidulaPrashant Gowardhan, Anne R Wilkinson, SadhanaD Mahore, Radhika Mhatre. (2015). Aspergillus salpingitis: A rare case report. Journal of Basic and Clinical Reproductive Sciences. 4(2):97.
View at Publisher | View at Google Scholar - Wikipediathefreeencyclopedia. Aspergillus
View at Publisher | View at Google Scholar - Bennett J W (2010). An Overview of the Genus Aspergillus
View at Publisher | View at Google Scholar - Thornton C R. (2020). Detection of the 'Big Five' mold killers of humans: Aspergillus, Fusarium, Lomentospora, Scedosporium and Mucormycetes. In Gadd G M, Sariaslani S (eds.). Advances in Applied Microbiology. Academic-Press 4–22.
View at Publisher | View at Google Scholar - (2021). ICD-11-ICD-11 for Mortality and Morbidity Statistics. World Health Organization.
View at Publisher | View at Google Scholar - Kutzner H, Kempf W, Feit J, Sangueza O (2021). Fungal Infections. Atlas of Clinical Dermatopathology: Infectious and Parasitic Dermatoses. Hoboken: Wiley Blackwell. 103-104.
View at Publisher | View at Google Scholar - Johnstone R B (2021). Mycoses and Algal infections. Weedon’s Skin Pathology Essentials (2nd ed.).
View at Publisher | View at Google Scholar - Invasive pulmonary aspergillosis Aspergillus & Aspergillosis Website. The Aspergillus Website.
View at Publisher | View at Google Scholar - Denning DW, Pashley C, Hartl D, Wardlaw A, Godet C, et al. (2014). Fungal allergy in asthma state of the art and research needs. Clinical and Translational Allergy. 4 (1): 14.
View at Publisher | View at Google Scholar - Warris A, Bercusson A, Armstrong-James D (2019).
View at Publisher | View at Google Scholar - Denning DW, Pleuvry A, Cole DC (2013). Global burden of chronic pulmonary aspergillosis complicating sarcoidosis. The European Respiratory Journal. 41 (3): 621–626.
View at Publisher | View at Google Scholar - Smith N L, Denning D W (2011). Underlying conditions in chronic pulmonary aspergillosis including simple aspergilloma. The European Respiratory Journal. 37 (4): 865–872.
View at Publisher | View at Google Scholar - Goel A. (2015). Pumonary aspergilloma. Mediconotebook. Retrieved 2023.
View at Publisher | View at Google Scholar - Guinea J, Torres-Narbona M, Gijón P, Muñoz P, Pozo F, et al. (2019). Pulmonary aspergillosis in patients with chronic obstructive pulmonary disease: incidence, risk factors, and outcome. Clin Microbiol Infect16(7):870-877.
View at Publisher | View at Google Scholar - Chen J, Yang Q, Huang J, Li L. (2013). Risk factors for invasive pulmonary aspergillosis and hospital mortality in acute-on-chronic liver failure patients: a retrospective cohort study. International Journal of Medical Sciences. 10 (12): 1625–1631.
View at Publisher | View at Google Scholar - Garcia-Vidal C, Upton A, Kirby KA, Marr KA. (2008). Epidemiology of invasive mold infections in allogenic stem cell transplant-recipients: biological risk factors for infection according to time after transplantation. Clinical Infectious Diseases. 47 (8): 1041–1050.
View at Publisher | View at Google Scholar - Nam HS, Jeon K, Um SW, Suh GY, Chung MP, et al. (2019). Clinical characteristics and treatment outcomes of chronic necrotizing pulmonary aspergillosis: a review of 43 cases. Int J Infect Dis. 14(6); e 479-482.
View at Publisher | View at Google Scholar - Thom C, Church M (1926). The Aspergilli. Baltimore: The Williams & Wilkins Company.
View at Publisher | View at Google Scholar - Spiegel A (2014). Are You Using the Right Soy Sauce? Here’s How to Find Out. The Huffington Post. Archived from the original on 2017-08-06.
View at Publisher | View at Google Scholar - Fenical, William; Jensen, Paul R. & Cheng, Xing C., (2000).
View at Publisher | View at Google Scholar - Toma, Maria Afroz; Nazir, K. H. M. Nazmul Hussain; Mahmud, Md Muket; Mishra, Pravin; Ali, et al. (2021). Isolation and Identification of Natural Colorant Producing Soil-Borne Aspergillus niger from Bangladesh and Extraction of the Pigment. Foods. 2021; 10 (6): 1280
View at Publisher | View at Google Scholar - (2016). Gras notification for Acid Lactase from Aspergillus oryzae Expressed in Aspergillus niger. Food and Drug Administration Archived from the Original on Section 2.
View at Publisher | View at Google Scholar - Wortman JR, Gilsenan JM, Joardar V, Deegan J, Clutterbuck J, et al. (2009). The 2008 update of the Aspergillus nidulans genome annotation: a community effort. Fungal Genet Biol. 2009 Mar;46 Suppl 1(Suppl 1): S2-13.
View at Publisher | View at Google Scholar - Description – Aspergillus Comparative. Broad Institute Archived. from the original on 22 November 2009
View at Publisher | View at Google Scholar - Dyer P S, O'Gorman C M. (2011). A fungal sexual revolution: Aspergillus and Penicillium show the way
View at Publisher | View at Google Scholar - O'Gorman C M, Fuller H, Dyer P S. (2009). Discovery of a sexual cycle in the opportunistic fungal pathogen Aspergillus fumigatus
View at Publisher | View at Google Scholar - Horn B W, Moore GG, Carbone I. (2009). Sexual reproduction in Aspergillus flavus. Mycologia. 101 (3): 423–429.
View at Publisher | View at Google Scholar - Swilaiman S S, O'Gorman C M, Balajee S A, Dyer P S. (2013). Discovery of a sexual cycle in Aspergillus lentulus, a close relative of A fumigatus. Eukaryotic Cell. 12 (7): 962–969.
View at Publisher | View at Google Scholar - Arabatzis M, Velegraki A. (2013). Sexual reproduction in the opportunistic human pathogen Aspergillus terreus. Mycologia. 105 (1): 71–79.
View at Publisher | View at Google Scholar - Malik S B, Pightling A W, Stefaniak L M, Schurko A M, Logsdon J M. (2007).An expanded inventory of conserved meiotic genes provides evidence for sex in Trichomonas vaginalis. PLOS ONE. 3 (8): e2879.
View at Publisher | View at Google Scholar - Heitman J, Sun S, James T Y. (2013). Evolution of fungal sexual reproduction. Mycologia. 105 (1): 1–27.
View at Publisher | View at Google Scholar - Paoletti M, Seymour FA, Alcocer M J, Kaur N, Calvo A M, et al. (2007). Mating type and the genetic basis of self-fertility in the model fungus Aspergillus nidulans. Current Biology. 2007 August; 17 (16): 1384–1389.
View at Publisher | View at Google Scholar - Dyer P S, O'Gorman C M. (2012). Sexual development and cryptic sexuality in fungi: insights from Aspergillus species. FEMS Microbiology Reviews. 2012 January; 36 (1): 165–192.
View at Publisher | View at Google Scholar - Rydholm C, Szakacs G, Lutzoni F. (2006). Low genetic variation and no detectable population structure in aspergillus fumigatus compared to closely related Neosartorva species. Eukaryotic Cell. 5 (4): 650–657.
View at Publisher | View at Google Scholar - Machida M, Gomi K, (2010). eds. Aspergillus: Molecular Biology and Genomics. Caister Academic Press. ISBN 978-1-904455-53-60.
View at Publisher | View at Google Scholar - Gibbons JG, Rokas A. (2013). The function and evolution of the Aspergillus genome. Trends in Microbiology. 2013 January; 21 (1): 14–22.
View at Publisher | View at Google Scholar - Khaldi N, Wolfe KH. Gadagkar S (ed.). (2008). Elusive origins of the extra genes in Aspergillus oryzae. PLOS ONE.2008 Aguust; 3 (8): e3036.
View at Publisher | View at Google Scholar - Bennett J W. (2010). An Overview of the Genus Aspergillus. Aspergillus: Molecular Biology and Genomics. Caister Academic Press. ISBN 978-1-904455-53-60.
View at Publisher | View at Google Scholar - Cloherty J. (2012). Manual of neonatal care. Philadelphia: Wolters Kluwer Health/Lippincott Williams & Wilkins. ISBN 978-1-60831-777-866;
View at Publisher | View at Google Scholar - Bozkurt MK, Ozçelik T, Saydam L, Kutluay L. A (2008). case of isolated aspergillosis of the maxillary sinus. Kulak Burun Bogaz Ihtisas Dergisi (in Turkish). 18 (1): 53–55. PMID 18443405.
View at Publisher | View at Google Scholar - (2014) MedScape. Archived from the original on 2014-02-23.
View at Publisher | View at Google Scholar - Wilson W R, Sande M A, Drew W L, (2001). eds. Current diagnosis & treatment in infectious diseases. Lange Medical Books/McGraw-Hill.
View at Publisher | View at Google Scholar - Di Paolo N, Guarnieri A, Garosi G, Sacchi G, Mangiarotti AM, et al. (1994). Inhaled mycotoxins lead to acute renal failure. Nephrology, Dialysis, Transplantation. 9 4: 116–120. PMID 7800243
View at Publisher | View at Google Scholar - (2012). Centers for Disease Control and Prevention CDC 24/7 Saving Lives Protecting People TM Fungal Diseases Aspergillosis | Types of Fungal Diseases | Fungal DiseasesCDC
View at Publisher | View at Google Scholar - Bongomin F, Gago S, Oladele R O, (2017). Denning D W. Global and Multi-National Prevalence of Fungal Diseases-Estimate Precision. Journal of Fungi. 3 (4): 57.
View at Publisher | View at Google Scholar - Bongomin F, Batac C R, Richardson M D, Denning D W A (2018). Review of Onychomycosis Due to Aspergillus Species. Mycopathologia. 2018 June; 183 (3): 485–493.
View at Publisher | View at Google Scholar - Aspergillus bronchitisAspergillus & Aspergillosis Website
View at Publisher | View at Google Scholar - Durack J, Boushey HA, Lynch SV (2016). Airway Microbiota and the Implications of Dysbiosis in Asthma. Current Allergy and Asthma Reports. 16 (8): 52.
View at Publisher | View at Google Scholar - Dagenais T R, Keller N P. (2009). Pathogenesis of Aspergillus fumigatus in Invasive Aspergillosis.ClinicalMicrobiologyReviews. 22 (3): 447–465.
View at Publisher | View at Google Scholar - Feys S, Gonçalves SM, Khan M, Choi S, Boeckx B, et al. (2022).
View at Publisher | View at Google Scholar - The Lancet Respiratory Medicine. 10 (12): 1147–1159. (22)00259-4.
View at Publisher | View at Google Scholar - Curtis A M, Smith GJ, Ravin C E. (1979). Air crescent sign of invasive aspergillosis
View at Publisher | View at Google Scholar - Fortún J, Martín-Dávila P, Alvarez ME, Norman F, Sánchez-Sousa A, et al. (2009). False-positive results of Aspergillus galactomannan antigenemia in liver transplant recipients. Transplantation. 87 (2): 256–260.
View at Publisher | View at Google Scholar - Martín-Rabadán P, Gijón P, Alonso Fernández R, Ballesteros M, Anguita J, et al. (2012). False-positive Aspergillus antigenemia due to blood product conditioning fluids. Clinical Infectious Diseases. 55 (4): e22–e27.
View at Publisher | View at Google Scholar - Kradin R L, Mark E J. (2008). The pathology of pulmonary disorders due to Aspergillus spp. Archives of Pathology & Laboratory Medicine. 132 (4): 606–614.
View at Publisher | View at Google Scholar - Mycoses: Aspergillosis. Mycology Online. Archived from the original on 7 December 2008.
View at Publisher | View at Google Scholar - Kontoviannis D P, Lionakis MS, Lewis RE, Chamilos G, Healy M, et al. (2005).Zygomycosis in a tertiary-care cancer center in the era of Aspergillus-active antifungal therapy: a case-control observational study of 27 recent cases. The Journal of Infectious Diseases. 191 (8): 1350–1360.
View at Publisher | View at Google Scholar - Aspergillosis-Wikipedia.From Wikipedia, the freeencyclopedia.
View at Publisher | View at Google Scholar - Walsh T J, Anaissie E J, Denning D W, Herbrecht R, Kontoyiannis D P, et al. (2008). Treatment of aspergillosis: clinical practice guidelines of the Infectious Diseases Society of America. Clinical Infectious Diseases. 46 (3): 327–360.
View at Publisher | View at Google Scholar - Herbrecht R, Denning D W, Patterson T F, Bennett J E, Greene R E, et al. (2002). Invasive Fungal Infections Group of the European Organisation for Research and Treatment of Cancer and the Global Aspergillus Study Group.
View at Publisher | View at Google Scholar - Cornely OA, Maertens J, Bresnik M, Ebrahimi R, Ullmann AJ, et al. (2007). AmBiLoad Trial Study Group. Liposomal amphotericin B as initial therapy for invasive mold infection: a randomized trial comparing a high-loading dose regimen with standard dosing (AmBiLoad trial). Clin Infect Dis. 15;44(10):1289-1297.
View at Publisher | View at Google Scholar - Denning DW, Park S, Lass-Florl C, Fraczek MG, Kirwan M, et al. (2011). High-frequency triazole resistance found in nonculturable Aspergillus fumigatus from lungs of patients with chronic fungal disease. Clin Infect Dis. 52(9):1123-1129.
View at Publisher | View at Google Scholar - Perea S, Patterson T F. (2002). Antifungal resistance in pathogenic fungi. Clinical Infectious Diseases. 35 (9): 1073–1080.
View at Publisher | View at Google Scholar - Li BK, Wang X, Ding Q. (2009). A case report of severe Aspergillus flavus penile infection. Asian J Androl. 2009 Sep;11(5):638-640. doi: 10.1038/aja.2009.45. Epub
View at Publisher | View at Google Scholar - Lisboa C, Ferreira A, Resende C, Rodrigues AG. (2009). Infectious balanoposthitis: management, clinical and laboratory features. Int J Dermatol. 48(2):121-124.
View at Publisher | View at Google Scholar - Mishri LK, Catherine MS, Mohammed B, Mohammed S, Asha K. (2000). Cutaneous and paranasal aspergillosis in an immunocompetent patient. Int J Dermatol 39: 835–836.
View at Publisher | View at Google Scholar - Aydin S, Ertugrul B, Gultekin B, Uyar G, Kir E. (2007). Treatment of two postoperative endophthalmitis cases due to Aspergillus flavus and Scopulariopsis spp. with local and systemic antifungal therapy. BMC Infect Dis. 7:87.
View at Publisher | View at Google Scholar - Zhang QQ, Li L, Zhu M, Zhang CY, Wang JJ. (2005). Primary cutaneous aspergillosis due to Aspergillus flavus: a case report. Chin Med J (Engl). 5;118(3):255-7.
View at Publisher | View at Google Scholar - Khan ZU, Ahmad S, Mokaddas E, Said T, Nair MP, et al. (2007). Cerebral aspergillosis diagnosed by detection of Aspergillus flavus-specific DNA, galactomannan and (1-->3)-beta-D-glucan in clinical specimens. J Med Microbiol. 56(Pt 1):129-132.
View at Publisher | View at Google Scholar - Heo CY, Eun SC, Baek RM, Minn KW. (2008). Free flap coverage of extensive soft tissue defect in cutaneous aspergillosis: a case report. J Korean Med Sci. 23(5):920-923.
View at Publisher | View at Google Scholar - Roilides E, Farmaki E. (2000). Human immunodeficiency virus infection and cutaneous aspergillosis. Arch Dermatol. 136(3):412-424.
View at Publisher | View at Google Scholar - Herron MD, Vanderhooft SL, Byington C, King JD. (2003). Aspergillosis in a 24-week newborn: a case report. J Perinatol. 23(3):256-259.
View at Publisher | View at Google Scholar - Nabil Khawand, George Jones, Mitchell Edson. (1989). Aspergillosis of prostate. Urology. 34(2): 00-101. ISSN 0090-4295,
View at Publisher | View at Google Scholar - Roux C, Thyss A, Gari-Toussaint M. (2013). Prostatic and renal aspergillosis due to Aspergillus fumigatus in a patient receiving alemtuzumab for chronic lymphocytic leukaemia, Journal de Mycologie Médicale, 23(4).
View at Publisher | View at Google Scholar - Abbas F, Kamal MK, Talati J. (1995). Prostatic aspergillosis. J Urol. 153(3 Pt 1):748-750.
View at Publisher | View at Google Scholar - Hemal AK, Talwar M, Dinda A. (1999). Concomitant renal and prostatic aspergillosis. Int Urol. Nephrol. 31(2):157-162.
View at Publisher | View at Google Scholar - Ansari MS, Nabi G, Singh I, Hemal AK, Bhan A. (2001). Mycotic abdominal aortic aneurysm: a fatal sequel to concomitant prostatic and renal aspergillosis. Case report and review of the literature. Urol. Int. 66(1):36-37.
View at Publisher | View at Google Scholar - Ludwig M, Schneider H, Lohmeyer J, Ermert L, Sziegoleit A, et al. (2005). Systemic aspergillosis with predominant genitourinary manifestations in an immunocompetent man: what we can learn from a disastrous follow-up. Infection. 33(2):90-92.
View at Publisher | View at Google Scholar - Thomas B. Campbell, Leo Kaufman, James L. Cook, (1992). Aspergillosis of the Prostate Associated with an Indwelling Bladder Catheter: Case Report and Review, Clinical InfectiousDiseases.14(4): 942–944.
View at Publisher | View at Google Scholar - Stuart M. Flechner, Jack W. McAninch, (1981). Aspergillosis of the Urinary Tract: Ascending Route of infection and Evolving Patterns of Disease. The Journal of Urology 125(4):598-601. (17)55119-8.
View at Publisher | View at Google Scholar - Valerio M, Fernandez-Cruz A, Fernandez-Yanez,Palomo J, Guinea J, Duran R, et al. Prostatic Aspergillosis in a Heart Transplant Recipient: Case Report and Review. The Journal of Heart and Lung Transplantation. 28(6): 636-646
View at Publisher | View at Google Scholar - Davido HT, Ryndin I, Köhler TS, Hadegard W, Monga M, et al. (2007). Aspergillosis of the scrotum: non-surgical management. Int J Urol. 2007 Feb;14(2):164-166.
View at Publisher | View at Google Scholar - Kim Y-S, Park S J. (2021). Aspergillus fumigatus-derived demethoxyfumitremorgin C inhibits proliferation of PC3 human prostate cancer cells through p53/p21-dependent G1 arrest and apoptosis induction Fisheries and Aquatic Sciences 24(1): 1-9. EISSN: 2234-1757.
View at Publisher | View at Google Scholar - Mathew M, Priya P, Mathew S. (2012). Scrotal Aspergillosis Associated with Fournier’s Gangrene in a Patient with Cirrhosis. Case Reports. Iranian Journal of Pathology. 7(1): 53-57.
View at Publisher | View at Google Scholar - Martínez-Salas AJ, Aquino-Matus JE, López-Vejar CE, Gutiérrez Díaz Ceballos ME, Noyola-Guadarrama A. (2022). Localized genitourinary tract Aspergillus infection in an immunocompetent patient: Bladder and epidydimal aspergillosis. Urol Case Rep. 42:102012.
View at Publisher | View at Google Scholar - Sakamoto S., Ogata J., Sakazaki Y., Ikegami K. (1978). Fungus ball formation of Aspergillus in the bladder. an unusual case report: Eur. Urol. 4(5):388–389.
View at Publisher | View at Google Scholar - Hameed T., Jain S.K., Ansari F.M., Dua A. (2020). Isolated fungal balls in urinary bladder presenting as acute retention of urine. Case Rep Urol. 2020:4601474.
View at Publisher | View at Google Scholar - Wu X., Venkataramanan R., Rivosecchi R.M., et al. (2020). Population pharmacokinetics of intravenous Isavuconazole in solid-organ transplant recipients. Antimicrob Agents Chemother. 27;64(2): e01728–19.
View at Publisher | View at Google Scholar - Hood SV, Bell D, McVey R, Wilson G, Wilkins EG. (1998). Prostatitis and epididymo-orchitis due to Aspergillus fumigatus in a patient with AIDS. Clin Infect Dis. 26(1):229-231.
View at Publisher | View at Google Scholar - Marr KA, Datta K, Mehta S, Ostrander DB, Rock M, et al. (2018). Urine antigen detection as an aid to diagnose invasive aspergillosis. Clinical Infectious Diseases. 2018 Nov 13;67(11):1705-1711.
View at Publisher | View at Google Scholar - Hoenigl M, Orasch T, Faserl K, Prattes J, Loeffler J, et al. (2019). Triacetylfusarinine C: A urine biomarker for diagnosis of invasive aspergillosis. J Infect. 2019 Feb;78(2):150-157.
View at Publisher | View at Google Scholar - Rocus R. Klont, Monique A. S. H. Mennink-Kersten, Paul E. Verweij, (2004). Utility of Aspergillus Antigen Detection in Specimens Other than Serum Specimens, Clinical Infectious Diseases, Volume 39, Issue 10, Pages 1467–1474,
View at Publisher | View at Google Scholar - [Sakamoto S. · Ogata J. · Salazaki Y. · Yoshilado S. · Ikegami K. (1978). Fungus Ball Formation of Aspergillus in the Bladder. Eur. Urol4: 388 – 389.
View at Publisher | View at Google Scholar - Salgia P, Mani MK. Renal aspergillosis--case report. Nephron. 1985;40(3):376-378.
View at Publisher | View at Google Scholar - Siddappa S, Mythri KM, Kowsalya R, Shivalingaiah M. (2012). An unusual case of non-disseminated bladder aspergillosis in a setting of transitional cell carcinoma. Indian J Med Microbiol. 30(1):106-108.
View at Publisher | View at Google Scholar - Adam J Singer, Bernard Kubak, Karl H Anders, (1998). Aspergillosis of the Testis in a Renal Transplant Recipient. Urology. 51(1): 119-121.
View at Publisher | View at Google Scholar - Heylen L, Maertens J, Naesens M, Van Wijngaerden E, Lagrou K, et al. (2015). Invasive aspergillosis after kidney transplant: case-control study. Clin Infect Dis. 60(10):1505-1511.
View at Publisher | View at Google Scholar - Najafi N, Shokohi T, Basiri A, Parvin M, Yadegarinia D, et al. (2013). Aspergillus terreus-related ureteral obstruction in a diabetic patient. Iranian Journal of Kidney Diseases. 7(2):151-155.
View at Publisher | View at Google Scholar - Smaldone MC, Cannon Jr GM, Benoit RM. (2006). Case report: bilateral ureteral obstruction secondary to Aspergillus bezoar. Journal of endourology. 1;20(5):318-320.
View at Publisher | View at Google Scholar - Ahuja A, Aulakh BS, Cheena DK, Garg R, Singla S, Budhiraja S. Aspergillus fungal balls causing ureteral obstruction. Urol J. 2009 Spring;6(2):127-9. PMID: 19472133. https://pubmed.ncbi.nlm.nih.gov/19472133/
View at Publisher | View at Google Scholar - Choi H, Kang IS, Kim HS, Lee YH, Seo IY. (2011). Invasive aspergillosis arising from ureteral aspergilloma. Yonsei Medical Journal. 1;52(5):866-868.
View at Publisher | View at Google Scholar - Zhu LP, Chen XS, Wu JQ, Yang FF, Weng XH. (2011). Aspergillus vertebral osteomyelitis and ureteral obstruction after liver transplantation. Transplant InfectiousDisease.13(2):192-199.
View at Publisher | View at Google Scholar - H. Vuruskan, A. Ersoy, N.K. Girgin, M. Ozturk, G. Filiz, I. et al. (2005). An Unusual Cause of Ureteral Obstruction in a Renal Transplant Recipient: Ureteric Aspergilloma, Transplantation Proceedings, Volume 37, Issue 5, Pages 2115-2117.
View at Publisher | View at Google Scholar - Guleria S, Seth A, Dinda AK, Kumar R, Chabbra RP, et al. (1998). Ureteric aspergilloma as the cause of ureteric obstruction in a renal transplant recipient. Nephrology, dialysis, transplantation: official publication of the European Dialysis and Transplant Association-European Renal Association. 1;13(3):792-793.
View at Publisher | View at Google Scholar - Kueter J C, MacDiarmid S A, Redman J F. (2002). Anuria due to bilateral ureteral obstruction by Aspergillus flavus in an adult male. Urology. 59(4): 601.
View at Publisher | View at Google Scholar - Rao P. (2015). Aspergillus infection in urinary tract post-ureteric stenting. Indian JournalofMedicalMicrobiology.1;33(2):316-319.
View at Publisher | View at Google Scholar - Haq JA, Khan MA, Afroze N, Haq T. (2007). Localized primary renal aspergillosis in a diabetic patient following lithotripsy–a case report. BMC infectious diseases. 7(1):1-4.
View at Publisher | View at Google Scholar - Young Kyung Yoon, Eun Hae Kang, Kwang Ho In, Min Ja Kim, (2010). Unilateral ureteral obstruction caused by Aspergillus, subgenus Nidulantes in a patient on steroid therapy: a case report and review of the literature, Medical Mycology, Volume 48, Issue 4, Pages 647–652,
View at Publisher | View at Google Scholar - Krishnamurthy, R., Aparajitha, C., Abraham, G. et al. (1998). Renal aspergillosis giving rise to obstructive uropathy and recurrent anuric renal failure. Geriatric Nephrology and Urology 8, 137–139
View at Publisher | View at Google Scholar - Bibler M R, John T. Gianis,(1987). Acute Ureteral Colic from an Obstructing Renal Aspergilloma, Reviews of Infectious Diseases, Volume 9, Issue 4, Pages 790–794.
View at Publisher | View at Google Scholar - Yoon YK, Kang EH, In KH, Kim MJ. (2010). Unilateral ureteral obstruction caused by Aspergillus, subgenus Nidulantes in a patient on steroid therapy: a case report and review of the literature. Medical mycology. 48(4):647-652.
View at Publisher | View at Google Scholar - Shohab D, Hussain I, Khawaja A, Jamil I, Raja NU, et al. (2014). Primary renal aspergillosis and xanthogranulomatous pyelonephritis in an immuno-competent toddler. J Coll Physicians Surg Pak. 1;24
View at Publisher | View at Google Scholar - Lee SW. (2010). An aspergilloma mistaken for a pelviureteral stone on nonenhanced CT: a fungal bezoar causing ureteral obstruction. Korean Journal of Urology. 1;51(3):216-218.
View at Publisher | View at Google Scholar - Ku JH, Kim DS, Kim JM, Kim YH, Jeon YS, et al. (1999). A case of anuria and urinary ascites in a premature infant due to bilateral ureteropelvic fungal bezoars. Korean J Urol. 40:1558–1562.
View at Publisher | View at Google Scholar - Irby PB, Stoller ML, McAninch JW. (1990). Fungal bezoars of the upper urinary tract. J Urol. 143:447–451.
View at Publisher | View at Google Scholar - Pérez-Arellano JL, Angel-Moreno A, Belón E, Francès A, et al. (2001). Isolated renoureteric aspergilloma due to Aspergillus flavus: case report and review of the literature. J Infect. 42:163–165
View at Publisher | View at Google Scholar - Bhayani SB, Siegel CL. Wein AJ, Kavoussi LR, Novick AC, et al. (2007). editors. Urinary tract imaging: basic principles. Campbell-Walsh urology. 9th ed. Philadelphia: Saunders;127–135.
View at Publisher | View at Google Scholar - el Fakir Y, Kabbaj N, Dafiri R, Imani F. (1999). Imaging of urinary Candida bezoars. Prog Urol. 9:513–517.
View at Publisher | View at Google Scholar - Sales JL, Mundy HB. (1973). Renal candidiasis: diagnosis and management. Can J Surg. 16:139–143.
View at Publisher | View at Google Scholar - Flechner SM, McAninch JW. (1981). Aspergillosis of the urinary tract: ascending route of infection and evolving patterns of disease. J Urol. 1981. 125:598–601.
View at Publisher | View at Google Scholar - Modi P, Goel R. (2007). Synchronous endoscopic management of bilateral kidney and ureter fungal bezoar. Urol Int. 78:374–376
View at Publisher | View at Google Scholar - Paul S, Singh V, Sankhwar S, Garg M. (2013). Renal aspergillosis secondary to renal instrumentation in immunocompetent patient. Case Reports. 11.
View at Publisher | View at Google Scholar - Ullah SR, Jamshaid A, Zaidi SZ. (2016). Renal aspergilloma presenting with pelvi-ureteric junction obstruction (PUJO). J Pak Med Assoc 1;66: 903-904.
View at Publisher | View at Google Scholar - Warshawsky AB, Keiller D, Gittes RF. (1975). Bilateral renal aspergillosis. The JournalofUrology.113(1):8-11.
View at Publisher | View at Google Scholar - Chang JB, Song PH, Choi JY. (2016). Ureteral Obstruction Caused by Aspergilloma in a Non-Immunosuppressive Patient. Urogenital Tract Infection. 31;11(3):118-120.
View at Publisher | View at Google Scholar - Sivasubramanian, G., Sobel, J.D. (2009). Urinary Tract Infections Caused by Aspergillus Species. In: Comarú Pasqualotto, A. (eds) Aspergillosis: From Diagnosis to Prevention. Springer, Dordrecht.
View at Publisher | View at Google Scholar - Erkan Dervisoglu, Emre Dikmen, Deniz Filinte & Ahmet Yilmaz (2008). Isolated bladder aspergillosis as the primary presentation of non-oliguric acute renal failure, Scandinavian Journal of Urology and Nephrology, 42:2, 189-191,
View at Publisher | View at Google Scholar - Nain PS, Singal R, Goyal A, Singh K, Matta H, et al. (2013). An awareness of a possible cause of obstruction due to a ureteric aspergilloma mistaken for stone. Maedica. 8(3):272 - 275.
View at Publisher | View at Google Scholar - Eisenberg RL, Hedgcock MW, Shanser JD. (1977). Aspergillus mycetoma of the renal pelvis associated with ureteropelvic junction obstruction. The Journal of Urology.118(3):466-467.
View at Publisher | View at Google Scholar - Maquera-Afaray J, Luna-Vilchez M, Portillo-Alvarez D, López JW. (2022). Primary renal aspergillosis in a newborn: a case report and review of the literature on children. The Turkish Journal of Pediatrics. 1;64(3):580-584.
View at Publisher | View at Google Scholar - Singal A, Grover C, Pandhi D, Das S, Jain BK. (2013). Nosocomial urinary tract aspergilloma in an immunocompetent host: An unusual occurrence. Indian Journal of Dermatology. 1;58(5):408.
View at Publisher | View at Google Scholar - Songkhla MN. (2020). Renal aspergillosis in an immunocompetent patient: a case report. Chonburi Hospital Journal-วารสาร โรง พยาบาล ชลบุรี. 2;45(2):133-136.
View at Publisher | View at Google Scholar - Park H, Lee MJ, Kim Y, Min YH, Kim SJ, et al. (2010). Primary renal aspergillosis and renal stones in both kidneys associated with hematopoietic stem cell transplant. The Korean journal of hematology. 45(4):275.
View at Publisher | View at Google Scholar - Vuruşkan H, Ersoy A, Girgin N, Öztürk M, Filiz G, et al. (2005). An unusual cause of ureteral obstruction in a renal transplant recipient: Ureteric aspergilloma. Transplantation Proceedings. 37(5), 2115-2117.
View at Publisher | View at Google Scholar - Meng XC, Jiang T, Yi SH, Xie PY, Guo YF, et al. (2014). Renal aspergillosis after liver transplantation: clinical and imaging manifestations in two cases. World Journal of Gastroenterology: WJG.
View at Publisher | View at Google Scholar - L. Sadagah, M. Alharbi, M. Alshomrani, A. Almalki, (2017). Renal Allograft Aspergillus Infection Presenting with Obstructive Uropathy: A Case Report, Transplantation Proceedings, Volume 49, Issue 1, Pages 193-197,
View at Publisher | View at Google Scholar - Sharmin F. (2018). Urinary Tract Aspergillosis in a Patient with Diabetes Who Underwent Total Abdominal Hysterectomy. Bangladesh Journal of Obstetrics & Gynaecology. 2018;33(1):74-77.
View at Publisher | View at Google Scholar - Albin OR, Soper N, Khurana I, Kauffman CA. (2019). Invasive genitourinary aspergillosis in a patient with chronic lymphocytic leukemia treated with venetoclax: Case report and review of the literature. In Open Forum Infectious Diseases (Vol. 6, No. 11, p. ofz457). US: Oxford University Press.
View at Publisher | View at Google Scholar - Mousavi B I T A, Najafi N, Zeinali A, Bassiri A, Parvin M, et al. (2011). Ureteral obstruction due to Aspergillus terreus in a diabetic patient following ureteroscopic lithotripsy: a case report. Abstract Number: P063.
View at Publisher | View at Google Scholar - Martínez-Girón R, Martínez-Torre S, Mosquera-Martínez J. (2015). Bladder aspergillosis detected by urine cytology. Diagn Cytopathol. 43(5):403-406.
View at Publisher | View at Google Scholar - Gowardhan V P, Wilkinson A R, Mahore S D, Mhatre R. (2015). Aspergillus salpingitis: A rare case report. Journal of Basic and Clinical Reproductive Sciences Medknow.4(2):97.
View at Publisher | View at Google Scholar - Kim SW, Nah MY, Yeum CH, Kim NH, Choi HS, et al. (2001). Pelvic aspergillosis with tubo-ovarian abscess in a renal transplant recipient. Journal of Infection. 1;42(3):215-217.
View at Publisher | View at Google Scholar - Borsa BA, Özgün G, Houbraken J, Ökmen F. (2015). İmmün kompetan bir hastada Aspergillus protuberus'un neden olduğu ilk inatçı vajinit olgusu [The first case of persistent vaginitis due to Aspergillus protuberus in an immunocompetent patient]. Mikrobiyol Bul49(1):130-4. Turkish.
View at Publisher | View at Google Scholar - D. Elad, D. Lahav, S. Blum, (2008). Transuterine transmission of Aspergillus terreus in a case of disseminated canine aspergillosis, Medical Mycology. 46(2):175–178.
View at Publisher | View at Google Scholar - Babre V, Bendre K, Niyogi G. A (2016). Rare Case of Ovarian Aspergilloma.
View at Publisher | View at Google Scholar - Walker JT, Frazho JK, Randell SC. (2012). A novel case of canine disseminated aspergillosis following mating. Can Vet J. 53(2):190-192.
View at Publisher | View at Google Scholar - Gupta K L, Ramachandran R, Kumar V, Rathi M, Kohli H S, et al. (2020). A Fungal infection in post-renal transplant patient: single-center experience. Indian J Pathol Microbiol
View at Publisher | View at Google Scholar - Gupta N, Vidyarthi A J, Ghosh P, Gautam D, Ahlawat K, et al. (2021). Successfully Treated Post-Urosurgical Urinary Tract Aspergillosis. Journal of Case Reports. Published On Line.
View at Publisher | View at Google Scholar
