

Case Report | DOI: https://doi.org/10.31579/2835-2882/027
Androgenic Alopecia in a Patient with Systemic Lupus Erythematosus
- Da Ponte María Noemí 1*
- Ocampos, Sara Elisa 1
- Mongelos, Andrea Belén 1
- Contreras, Romina 2
- Riveros, Rosalba 2
- Aldama, Arnaldo 3
1 Dermatology Resident.
2 Dermatologist. Teaching Assistant.
3 Dermatologist. Professor of Dermatology. Head of Chair.
*Corresponding Author: Da Ponte, María Noemí, Villa Elisa-Paraguay., Department of Dermatology Resident.
Citation: Da Ponte María Noemí, Ocampos Sara Elisa, Mongelos Andrea Belén, Contreras Romina, Riveros, Rosalba. (2023), Androgenic alopecia in a patient with systemic lupus erythematosus, Clinical Research and Studies, 2(6); DOI:10.31579/2835-2882/027
Copyright: © 2023, Da Ponte María Noemí. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 04 December 2023 | Accepted: 18 December 2023 | Published: 29 December 2023
Keywords: alopecia; lupus erythematosus; systemic; minoxidil
Abstract
Hair is not only a matter of personal image, below is a clinical case of a patient with long-standing androgenic alopecia and lupus with suboptimal results after some previous treatments, the management of alopecia is a medical challenge because it is not only an aesthetic condition but also possible risk factors for psychiatric pathologies, timely diagnosis and treatment is important.
There are numerous treatments for androgenic alopecia from topical treatments, oral route and mesotherapy among others. In this particular case, a satisfactory response is presented after starting oral and topical minoxidil.
Introduction
Hair has been important to humanity, in terms of religion, race, gender and ornament. [1] Alopecia affects the quality of life in 41% of patients and the female sex is more affected [2]
There are several causes of hair loss, which represents a challenge for the doctor when it comes to diagnosis and treatment. We must begin by classifying them into two large groups: scarring and non-scarring alopecia. Several types of alopecia may coexist depending on the underlying pathology, such as systemic lupus erythematosus, which is mostly non-scarring and, except for chronic cutaneous lupus, can manifest as telogen effluvium, diffuse alopecia or patchy alopecia. present other etiologies of alopecia. [3]
Androgenic alopecia or common baldness is explained by an increased sensitivity of hair follicles to androgens. It is genetically determined and varies depending on the location of the scalp, with the occipital area being the least affected. It was shown that women as well as men with common baldness have higher levels of 5-reductase enzyme activity in the follicles of the frontal region of the scalp when compared to other areas of the scalp. The pattern of alopecia is different according to sex; in men it usually begins as a bitemporal regression of the hairline and subsequently affects the frontotemporal and vertex areas, and in women it begins as diffuse hair loss that affects especially to the central area of the scalp. In the histopathology of this type of disease, the progressive miniaturization of the terminal hair follicles is observed. [6]
Androgenetic alopecia (AGA) is one of the most frequent reasons for dermatological consultation. Epidemiological studies of AGA in women are
less numerous, a study by Norwood showed a total prevalence of around 19% in a population of 1006 Caucasian patients. In recent years, the understanding of the pathophysiology of AGA has improved diagnosis and treatment options, it is important to mention the role of dermoscopy as a useful diagnostic tool for AGA. While the main treatment options remain topical minoxidil, systemic finasteride, and hair transplants, newer modalities are being investigated. [4]
We report the following case of a patient with SLE associated with long-standing androgenetic alopecia who had received several oral and topical treatments.
Case Presentation
47-year-old female patient, radiologist, known SLE carrier, treated with methotrexate 15 milligrams weekly, hydroxychloroquine 200 milligrams per day, and folic acid 10 milligrams per day for approximately 10 years.
He consulted the dermatology service due to a 10-year history of hair loss accompanied by itching. He received treatment with minoxidil 5% lotion, desonide foam, and finasteride 1 milligram for 3 months with little improvement.
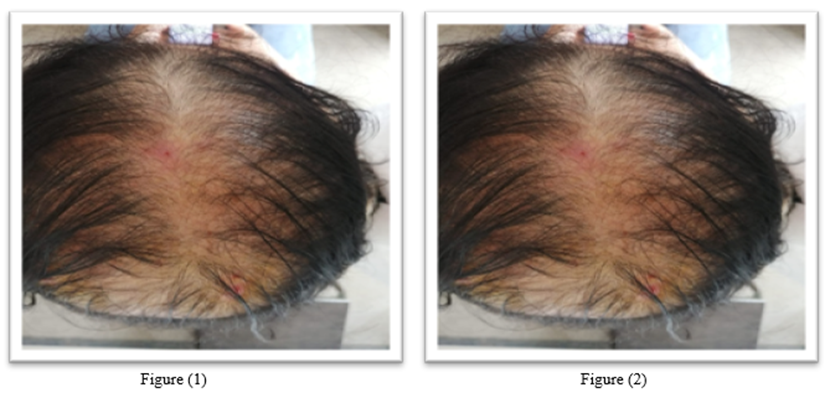
On physical examination, there was a diffuse reduction in hair density throughout the upper central part of the scalp (biparietal frontal area). Figure 1 and 2.

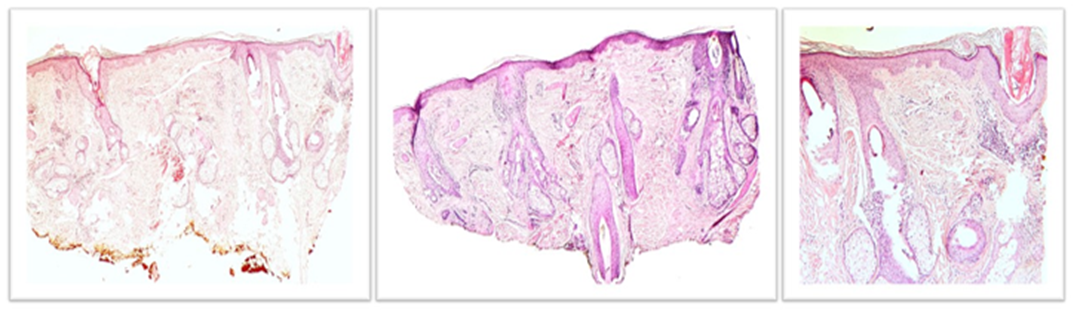
It was decided to take a scalp biopsy, the pathological diagnosis concluded: non-categorical findings, but that favor probable androgenetic alopecia in relation to collagenopathy. (Figure 3)

Subsequently, it was decided to start treatment with minoxidil 1 milligram orally once a day, minoxidil 5% lotion and clobetasol foam due to persistence of itching. A control laboratory was requested for the next consultation.
A control visit was carried out 3 months after starting oral minoxidil 1 milligram with good tolerance and topical minoxidil 5% lotion.


Laboratory control: Hemoglobin 13.9 g/dl, hematocrit 42.1%, white blood cells 5170/mm3, neutrophils 50% lymphocytes 43%, urea 27, creatinine 0.78 mg/dl, GOT 19 iu/l, GPT 23 iu /l total bilirubin 0.6 mg/dl, HDL 41 mg/dl, triglycerides 130 mg/dl, thyroid profile in range, ANA negative and antiDNA negative, C3 and C4 not consumed. Iron 33 (33-193), vitamin D 22 (greater than 30), transferrin 243 (200-360), ferritin 101 (13-150).
Discussion
Hair has always been an important issue for humanity and this is demonstrated in a study carried out with 65 patients diagnosed with androgenic alopecia who reported damage to their quality of life, as well as levels of depression and anxiety, 8 in the clinical case presented. Previously, the delay in diagnosis and timely treatment can be demonstrated, these patients should be treated by a multidisciplinary team including psychologists and psychiatrists depending on the severity of said associated disorders.
The treatments most used by dermatologists in Spain for androgenic alopecia in postmenopausal women were topical minoxidil, oral finasteride and nutricosmetics. 7-9, in this patient topical denoside, topical 5% minoxidil and finasteride were started as initial treatment. Topical corticosteroids initially taking into account the underlying pathology and that it could be the cutaneous manifestations of lupus disease.
In the largest open-label study, Tosti, treated 430 patients with male pattern alopecia type III to VI with topical minoxidil 1% lotion for at least 6 months. 18% of patients experienced new terminal hair growth that completely covered the bald area. After suspension, 33% of patients maintained good cosmetic appearance and new hair growth after 12 months of follow-up, 10 the oral minoxidil drug is another therapeutic option to topical minoxidil, being more effective than the latter and presenting better adherence to the treatment. treatment. The most common side effect is the hypertrichosis it produces, which usually appears in 25-50% of women at doses close to 1 mg daily 11. In this case, 5% minoxidil lotion and oral minoxidil were indicated with good results. a joint therapy, the patient did not report adverse reactions in the consultation, it is important to highlight that there are few publications on this oral and topical combination of minoxidil.
As other alternatives, these therapeutics are presented, such as the greater effectiveness of oral dutasteride compared to oral finasteride, and dutasteride microinjections are shown as a safe and potentially effective alternative in the treatment of androgenic alopecia in general 12, these alternatives are highlighted. treatment since each patient could respond differently, influenced by economic resources, origin, cultural beliefs and adverse reactions to oral drugs in most cases.
Hair loss generates significant stress, especially for women. It is essential to determine the cause for adequate treatment and take into account that several etiologies may coexist in the same patient. The importance of close follow-up is highlighted, which allows us to assess the response to different treatments.
Authors contribution statement:
MND, RC and RR conceived and designed the study, MND, SEO, ABM, RC, RR and AA contributed to data acquisition and interpretation. MND wrote the manuscript. All authors contributed to the discussion, review, and approval of the final manuscript.
Financing:
This case report was carried out through self-financing
The authors have no conflicts of interest
Special thanks to Dr. Luis Celias, Dermatopathologist, for his collaboration with the clinical case.
References
- Guerrero R., Kahn Ch M. (2011). Alopecias, Revista Médica Clínica las Condes, Volume22, Issue 6, Pages 775-783.
View at Publisher | View at Google Scholar - T titeca G, Goudetsidis L, Francq B, Sampogna F, Gieler U, et al. (2020). The psychosocial burden of alopecia areata and androgenetics : a cross-sectional study multicenter study among dermatological out-patients in 13 European countries _ J Eur Acad Dermatol Venereol . 2020 Feb ;34(2):406-4 J Eur Acad Dermatol Venereol . 2020 May;34(5):1
View at Publisher | View at Google Scholar - Feature Schilcrot F, et al. (2017). Diffuse scarring alopecia as a manifestation of cutaneous lupus. Skin ( Barc ).
View at Publisher | View at Google Scholar - Kaliyadan F, Nambiar A, Vijayaraghavan S. (2013). Androgenetic alopecia: an update _ Indian J Dermatol Venereol Leprol _ 79(5):613-25.
View at Publisher | View at Google Scholar - Rossani, G; Hernandez. (2018). Hair follicle growth induction and restoration with autologous growth factors in nonscarring scalp pathology. Cir. plastic _ iberolatinoam .- Vol. 44 - No. 2 April - May – June.
View at Publisher | View at Google Scholar - Bernardez C,et al. (2014). Histopathology of alopecias. Part I: nonscarring alopecia. Proceedings Dermosiphilogr .
View at Publisher | View at Google Scholar - Bernardez C, et al. (2014). Histopathology of alopecias. Part II: scar alopecia. Proceedings Dermosiphilogr .
View at Publisher | View at Google Scholar - Cisneros- Poireth DA, Morales-Miranda AY, Ugalde-Aguilar H, et al. (2021). Psychosocial impact and quality of life in patients with androgenic alopecia. Cosmetic, Medical and Surgical Dermatology. 19(1):7-11
View at Publisher | View at Google Scholar - Pindado-Ortega C, et al. (2018). Cross-sectional study about prescribing habits in androgenic alopecia of dermatologists in Spain in 2017. Actas Dermosifiliogr.
View at Publisher | View at Google Scholar - Clissold SP, Heel RC. (1987). Topical minoxidil. A preliminary review of its pharmacodynamic properties and therapeutic efficacy in alopecia areata and alopecia androgenetica. Drugs. Feb;33(2):107-122.
View at Publisher | View at Google Scholar - R. Gil-Redondo, OM Moreno-Arrones, S. Vañó -Galván, P. Jaén- Olasolo, Alopecia, (2019). Medicine - Accredited Continuing Medical Training Program, Volume 12, Issue 92, Pages 5394-5404, ISSN 0304-5412.
View at Publisher | View at Google Scholar - Reguero-del Cura L, et al. FR-Mesotherapy with dutasteride, a future alternative for the treatment of androgenetic alopecia. Actas Dermosifiliogr. 2020.
View at Publisher | View at Google Scholar
