

Case report | DOI: https://doi.org/10.31579/2834-8508/025
An Unexpected Occupational Hazard: Chronic Beryllium Disease in a Jeweller
- Miguel Jose Teixeira 1
- Lizelle Nagel 2
- Dante Plekker 3
- Cassandre van der Merwe 2
- Sylvia van den Berg 2,4
1The Ampath Allergy Clinic, Pretoria, South Africa
2Department of Immunology, Ampath Laboratories, Pretoria, South Africa
3Specialist Physician/Pulmonologist, Netcare Kuilsrivier Hospital, Cape Town, South Africa
4Department of Paediatrics and Child Health, University of Pretoria, Steve Biko Academic Hospital, Pretoria, South Africa
*Corresponding Author: Miguel Jose Teixeira, The Ampath Allergy Clinic, Pretoria, South Africa.
Citation: Miguel Jose Teixeira, Lizelle Nagel, Dante Plekker, Cassandre van der Merwe, and Sylvia van den Berg, (2024), An Unexpected Occupational Hazard: Chronic Beryllium Disease in a Jeweller, Archives of Clinical and Experimental Pathology, 3(1); DOI:10.31579/2834-8508/025
Copyright: © 2024, Miguel Jose Teixeira. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 25 January 2024 | Accepted: 14 February 2024 | Published: 29 February 2024
Keywords: beryllium, chronic beryllium disease, occupational health, interstitial lung disease, lymphocyte proliferation test
Abstract
Beryllium is used widely in industry due to its favourable elemental properties. Its extraction and incorporation into alloys and composites generate hazardous fumes and dust. Chronic beryllium disease (CBD) is an occupational interstitial lung disease that clinically resembles sarcoidosis. We present a case of a 33-year-old jeweller who developed CBD from exposure to dust while grinding unfinished gemstones. While workplace protection exists for beryllium workers, the health risks are unrecognised in artisans. While most cases are diagnosed in industry, some are linked to novel or unexpected hazards. Lymphocyte proliferation testing to metals is a key investigation in patients with occupational asthma or pneumoconiosis.
Abbreviations
Beryllium - Be
Occupational Health and Safety Administration - OHSA
Chronic Beryllium Disease - CBD
High Resolution Computed Tomography - HRCT
Human Immunodeficiency Virus - HIV
Angiotensin-Converting Enzyme - ACE
Bronchoalveolar Lavage Fluid - BALF
Beryllium Sensitization - BeS
Interstitial Lung Disease - ILD
Lymphocyte Proliferation Test - LPT
Beryllium Lymphocyte Proliferation Test - BeLPT
Peripheral Blood Mononuclear Cells - PBMC
Pokeweed Mitogen - PWM
Acute Respiratory Distress Syndrome - ARDS
Diffuse Alveolar Damage - DAD
Electron Probe X-ray Microanalysis (EPMA)
United States (US)
Aluminium Lymphocyte Proliferation Test - AlLPT
Epithelial-Mesenchymal Transition (EMT)
Hard Metal Lung Disease (HMLD)
Introduction
Beryllium (Be) is used widely in many industries due to its favourable elemental properties. While inert in solid metal form, its chemical extraction and incorporation into metal alloys and composite materials generate hazardous vapours and dust. The United States produces 60% of the world’s beryllium, and protection of beryllium workers is well-established under the Occupational Health and Safety Administration (OHSA)1. However, the health risks may be unrecognised in novel or artisanal industries where beryllium exposure may result from new or unexpected hazards.
Case Report
A 33 year old man presented with a history of progressive shortness of breath, dry cough and weight loss over the past 12 months. He is a smoker with prior diagnoses of asthma and inhalant allergy. His airway symptoms failed to improve with therapy. Coughing episodes were sometimes accompanied by fever, chills and myalgia. On enquiry into his occupational history, the patient revealed that he has been working as a jeweller for the past 13-14 years. The work entails cutting, grinding, faceting and polishing of gemstones. He also melts and casts various metal alloys while crafting jewellery. The patient lives in a suburban neighbourhood in Cape Town, and doesn’t keep animals.
There was no clubbing, pallor, lymphadenopathy, jaundice or peripheral oedema on physical examination. The respiratory examination was unremarkable. Chest radiography revealed bilateral diffuse infiltrates and nodules (Figure 1). Spirometry indicated a mixed pattern of airway disease, significantly reduced FEV1 and FVC (36% and 46% of predicted respectively) and a decreased FEV1/FVC ratio of 78%. The bronchodilator challenge showed no reversibility. Diffusion capacity was 43% of predicted, indicating significant interstitial disease. High resolution computed-tomography (HRCT) revealed dense bilateral pulmonary infiltrates affecting all zones of the lungs (Figure 2). The full blood count, inflammatory markers, total IgE, autoimmune screen, and serum angiotensin-converting enzyme (ACE) levels were within normal limits. The patient tested negative for Human Immunodeficiency virus (HIV). Bronchoalveolar lavage fluid (BALF) analysis showed increased lymphocytes (10%) and neutrophils (19%), and no eosinophils. Tuberculosis and fungal investigations were negative. Transbronchial biopsy revealed non-caseating granulomas.
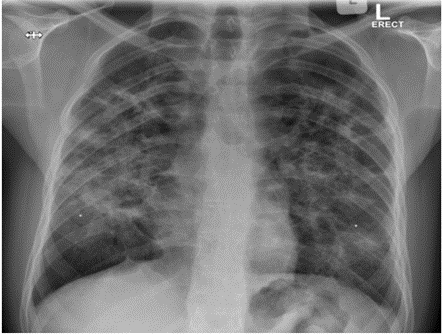
Figure 1: Erect Postero-Anterior X Ray - Diffuse bilateral infiltrates and nodules.
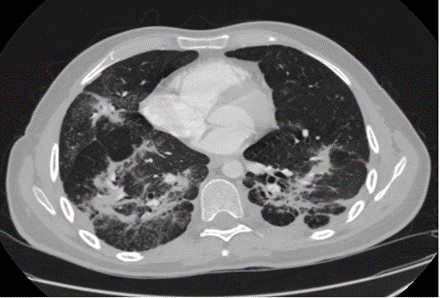
Figure 2: High Resolution Computed Tomography - Dense bilateral pulmonary infiltrates with underlying nodules.
Gemstone cutting and grinding generate dust that may contain beryllium. Metal ions are potent haptens, and a population of metal-specific memory T lymphocytes may establish itself in the body following exposure in predisposed individuals2. Re-exposure activates the resident metal-specific memory T cells to induce lymphocyte proliferation3. Lymphocyte proliferation in the presence of beryllium is a useful test for CBD, and a beryllium lymphocyte proliferation test (BeLPT) was ordered to screen for beryllium sensitization (BeS).
The patient’s peripheral blood mononuclear cells (PBMC) were isolated and exposed to beryllium sulphate tetrahydrate in cell culture. Lymphocyte proliferation was assessed after 6 days using Ki-67 staining and flow cytometry on a BD FACS Canto flow cytometer. Lymphocyte proliferation is reported as a stimulation index (SI) that is calculated as the ratio between the mean fluorescence intensity (MFI) of the stimulated lymphocytes and negative control lymphocytes. An SI of 4 - 9 is considered positive, and ≥10 strongly positive. A strongly positive SI of 22 was observed, confirming that the patient is sensitised to beryllium (Figure 3). Chronic beryllium disease was diagnosed based on the finding of non-caseating granulomas and BeS. A personal protection plan was negotiated with the patient’s employer and the patient was prescribed 40 mg prednisone daily to control the granulomatous inflammation.

Figure 3: (A) BeLPT Negative Control (Unstimulated), gated to show resting CD3+ lymphocytes at baseline (blue). (B) BeLPT Positive Control (stimulated with Pokeweed Mitogen/PWM), gated to show CD3+ lymphocytes proliferating in response to PWM in the P4 window. (C) BeLPT Patient test (Stimulated with Beryllium), gated to show proliferation of CD3+ lymphocytes in response to beryllium in the P4 window.
Discussion
Beryllium exposure is an ongoing occupational hazard. It causes chronic beryllium disease (CBD) in susceptible individuals after inhalation of beryllium dust or fumes[1,4]. Most cases are diagnosed in workers in the beryllium extraction and composite materials production industries. Other high-risk industries include metal working (aerospace, weapons, shipbuilding, automobile manufacturing), nuclear power generation, mining, construction, consumer electronics and dental product manufacturing[4,5]. To our knowledge, this is the first reported case of CBD diagnosed in a jeweller.
Gemstone cutters are exposed to various mineral and metal dusts during jewellery manufacturing. The beryls are a group of minerals that include emerald, aquamarine, beryl and bertrandite, and grinding these minerals aerosolize beryllium dust[6]. Gemstone cutters may also be exposed to nickel, aluminium, silica, chromium and lead present within minerals and grinding discs6. There have been no prior reports of adverse health effects in gemstone cutters, but health monitoring has been recommended[6]. The evidence of harm is limited, but the health risks may well be underestimated. Assessing this occupational risk is challenging since jewellers work with a variety of precious minerals and metals, and respiratory exposures are often mixed. Gemstones like ruby, sapphire and quartz do not contain beryllium but do contain other harmful elements like silica and aluminium[6].
Beryllium is poorly soluble and accumulates in the tissues. Attempts at chelation have been unsuccessful[4]. Acute pneumonitis occurs at high exposures, but CBD is not clearly dose-dependent4,5. Beryllium sensitization (BeS) is a key first step in CBD pathogenesis, and can be screened for with a beryllium lymphocyte proliferation test (BeLPT)1,4. The BeLPT can also be performed on lymphocytes from bronchoalveolar lavage fluid where it shows enhanced specificity7. CBD results from a chronic type-IV hypersensitivity reaction in the pulmonary interstitium. Beryllium ions are presented by antigen-presenting cells to naive CD4+ T cells, triggering immune activation, cytokine release, inflammation, and formation of beryllium-specific memory T cells4,8. Re-exposure induces lymphocytic alveolitis that progresses to granuloma formation8. HLA-DBP1 E69 has been associated with a higher risk of BeS and CBD1. Beryllium also enhances the innate immune response by inducing activation and maturation of macrophages and dendritic cells, which augments antigen presentation, cell differentiation, cytokine secretion and T cell responses8. Disease latency from exposure to symptom onset is variable, and symptoms are mostly respiratory[1,4]. A mortality rate of 30% has been reported, and is mostly due to chronic respiratory failure[1,4].
Spirometry may show restrictive, obstructive or mixed patterns, but may also be normal in early disease[1,4]. Impaired gas exchange during cardiopulmonary exercise testing is an early finding[1,4]. Chest radiography findings resemble those of pulmonary sarcoidosis, but perihilar and mediastinal lymphadenopathy is less frequent[4,7]. Lung nodules are the most common finding on HRCT, together with ground glass infiltrates and thickening of bronchial walls and/or interlobular septae. Honeycombing, subpleural cysts and calcifications may be seen in advanced disease[4]. The hallmark histological finding in both CBD and sarcoidosis is non-caseating granulomas[4]. Bronchoalveolar lavage and transbronchial biopsy provide essential confirmatory evidence. A differential cell count on BALF includes counting of macrophages, lymphocytes, neutrophils and eosinophils[9]. A differential diagnosis of abnormal BALF cell counts is presented in Table I. Lymphocyte counts >25% are highly suggestive of CBD. Lymphocyte subset analysis is not routinely recommended[9].
Lymphocytic Pattern (>15% Lymphocytes) | Eosinophilic Pattern (>1% Eosinophils) | Neutrophilic Pattern (>3% Neutrophils) |
Sarcoidosis | Eosinophilic Pneumonias | Collagen Vascular Disease |
Nonspecific Interstitial Pneumonias | Hypersensitivity Pneumonitis | Idiopathic Pulmonary Fibrosis |
Hypersensitivity Pneumonitis | Asthma, Bronchitis | Aspiration Pneumonia |
Drug-Induced Pneumonitis | Bone Marrow Transplant | Bacterial & Fungal Infections |
Radiation Pneumonitis | Churg-Strauss Syndrome | Bronchitis |
Collagen Vascular Diseases | Allergic Bronchopulmonary Aspergillosis | Asbestosis |
Cryptogenic Organizing Pneumonia | Bacteria, Fungal, Helminthic & Pneumocystis Infections | Acute Respiratory Distress Syndrome (ARDS) |
Lymphoproliferative Disorders | Hodgkin’s Disease | Diffuse Alveolar Damage (DAD) |
(Adapted from: Meyer KC, Raghu G, Baughman RP, Brown KK, Costabel U, Du Bois RM, et al. An official American Thoracic Society clinical practice guideline: the clinical utility of bronchoalveolar lavage cellular analysis in interstitial lung disease. American journal of respiratory and critical care medicine. 2012 May 1;185(9):1004-1014.)
Table I: Differential Diagnosis of abnormal BALF cell counts
Epithelioid granulomatous reactions may be seen in sarcoidosis, fungal pneumonia, pulmonary tuberculosis, atypical mycobacterial pneumonia and pneumoconiosis caused by beryllium, aluminium, nickel, titanium, chromium, palladium, silica, mercury and zirconium dusts[4,10]. The signature pathological lesions in CBD and sarcoidosis are non-caseating granulomas, which consists of aggregated epithelioid histiocytes with a collar of mostly CD4+ T cells[4,10],. CBD patients are often misdiagnosed with pulmonary sarcoidosis due to the clinical similarity, and a detailed occupational history and metal LPT testing is required to make the distinction. Beryllium particles are present within granulomas in CBD patients and can be identified using mass spectroscopy or electron probe X-ray microanalysis (EPMA), but this is no longer routinely required[4]. The current diagnostic criteria for CBD are summarised in Table II. BeLPT testing has high variability and tests should be repeated for confirmation, especially if borderline or negative. A single BeLPT detects BeS with 68% sensitivity and 96.6% specificity[4]. Repeat testing improves the sensitivity to 88%[4]. Beryllium skin patch testing is no longer recommended since it may induce BeS[4].
DEFINITE | PROBABLE |
|
|
2. Evidence of BeS which may include:
| 2. Evidence of BeS which may include:
|
| 3. Compatible imaging findings | 3. Compatible imaging findings Or BALF lymphocytosis >15%
|
| 4. BALF lymphocytosis >15% | |
| 5. Non-caseating granulomas |
(Adapted from Balmes JR, Abraham JL, Dweik RA, Fireman E, Fontenot AP, Maier LA, et al. An official American Thoracic Society statement: diagnosis and management of beryllium sensitivity and chronic beryllium disease. Am J Resp Crit Care Med. 2014 Nov 15; 190(10): 34-59.)
Table II: Diagnostic criteria for CBD
Management includes avoiding further beryllium exposure as well as suppressing the ongoing immune response to beryllium[4]. Lifelong therapy is required, and systemic corticosteroids are considered first-line for patients with significant symptoms of pulmonary functional decline[1,4]. Steroid sparing agents such as infliximab, cyclophosphamide, methotrexate, azathioprine and mycophenolate mofetil can also be used based on treatment approaches for sarcoidosis[1,4]. Patients with severely impaired gaseous exchange may benefit from infliximab[1],. The therapeutic efficacy of infliximab was evaluated in CBD patients, and improved lung function and quality of life was reported[1].
Berylliosis was first described as an occupational lung disease in 1943[1]. The United States (US) of the 1940’s was inundated by an occupational epidemic linked to rapid industrialization, and the link to beryllium exposure became evident over time[1]. Disease registries were established and the first regulations on allowable beryllium exposure established in 1949[1]. These regulations were later adopted by the US Occupational Health and Safety Administration (OHSA) in 1971[1]. The original regulations limited beryllium exposure per 8-hour shift to ≤2.0 ug/m3 [1,4]. Ambient air emissions were also restricted to ≤0.01 mg/m3 [4]. Evidence of “safe” levels of exposure was still lacking at the time, but the regulations did curb rates of acute beryllium pneumonitis which is a dose-dependent disease[1,4]. However, cases of CBD continued to occur in facilities compliant with the regulations of the time[1,4]. With evidence increasingly showing inadequate protection of workers, the allowable exposure over an 8-hour shift was reduced to ≤0.2 ug/m3 in 19994. OHSA implemented the new limits in 2018[1]. Any facility extracting beryllium or manufacturing beryllium-containing materials should implement a prevention plan to minimise inhalational and cutaneous exposure4. Personal protective equipment should be supplied to front-line workers and includes a filtering full face mask or negative pressure respirator with coveralls, gloves and overshoes4. Production processes should be optimised and access-controlled to prevent non-essential exposure of office workers, security guards, cleaners etc.[4]. Front-line workers should undergo annual medical surveillance and BeLPT testing, with further evaluation for CBD if BeLPT results are positive[1,4]. Rigorous workplace control and compliance with housekeeping rules have been shown to reduce rates of BeS[1,4]. OSHA recommends avoidance of further exposure in patients with BeS or established CBD, but this will not necessarily halt progression[1].
The complexity of materials used in industry can make it difficult to identify a single causative agent, as occupational exposure often involves multiple substances that may cause disease through different mechanisms. In addition to beryllium, gemstones also contain silicate, aluminium, nickel, chromium and cobalt which may contribute to disease pathogenesis[6].
Silicosis is a progressive interstitial lung disease (ILD) that is linked to inhalation of silica dust[5]. Silica is toxic to macrophages and induces macrophage apoptosis with release of inflammatory mediators in the lung parenchyma[5]. This inflammatory reaction recruits fibroblasts which ultimately cause fibrosis[5]. Workers in the mining, quarrying and sandblasting industries are historically most at risk[5]. Artificial stone manufacturing is a novel emerging hazard that is driving a new wave of silicosis cases amongst manufacturers of quartz, granite and quartzite kitchen and bathroom countertops[5].
Aluminosis is an occupational ILD that affects aluminium shavers and polishers that inhale aluminium dust[5,11]. Lung histology and an aluminium LPT (Al-LPT) is useful to make the diagnosis[11]. Mineralogical analysis of BALF or lung biopsy tissue may show high levels of aluminium[11].
Nickel exposure may cause interstitial fibrosis, COPD or asthma[12]. Nickel has also been associated with lung and nasal cancers[12]. Nickel exposure induces inflammation and epithelial-mesenchymal transition (EMT), a process during which epithelial cells lose cell-to-cell adhesions and acquire mesenchymal properties[12]. Aberrant EMT may lead to fibrosis, tissue destruction and malignant transformation[12].
Chromium is used to create durable alloys and is sometimes combined with tungsten and cobalt in the manufacturing of tools and hip prostheses[13]. A case of granulomatous lung disease secondary to systemic absorption of cobalt and chromium from a damaged hip prosthesis has been reported[13]. Chromium has also been linked to lung cancer[13].
Hard metal lung disease (HMLD) results from inhalation of tungsten carbide and cobalt dust[14]. The two metals are usually heated together and compacted into a durable heat and stress-resistant alloy that is used to sharpen drills, polish gemstones and manufacture dental prostheses[14]. Cobalt is widely regarded as the primary cause, but tungsten carbide and cobalt may also have synergistic effects[14]. Cobalt acts as a hapten to induce an IgE-mediated response. HMLD presents with occupational asthma, acute allergic alveolitis or fibrotic ILD[14].
Zirconium has also been implicated in ILD, but it is difficult to prove a definite link as most respiratory exposures are mixed[15]. A case was reported of a patient with occupational exposure over 15 years that presented with pneumoconiosis. Lung histology demonstrated birefringent particles that were identified as zirconium compounds[15]. In another case, a patient employed for 16 years in the nuclear industry developed persistent lung infiltrates prompting two lobectomies for suspected malignancy[16]. The patient was exposed to zircaloy during grinding and welding work, which is an alloy consisting of zirconium, tin, iron and chromium. Lung histology demonstrated epithelioid granulomas, and scanning transmission electron microscopy revealed zirconium as well as iron, silicon and chromium within the granulomas[16]. However, not all exposed workers develop zirconium-related granulomatous disease, suggesting that an unknown susceptibility factor may be required[16].
There is lack of evidence linking gold or platinum mining or metal crafting to occupational lung disease. A meta-analysis demonstrated silicosis in miners that extracted the ores in South Africa[17]. Several other substances present during ore extraction are known causes of chronic lung disease for example silica dust, coal and asbestos[17]. Platinum salts may be associated with occupational asthma via a haptenization process[18]. Employees sensitised to platinum salts may also manifest conjunctivitis, rhinitis, contact urticaria and eczema[19].
Indium has emerged as a novel cause of occupational lung disease[13]. Its thermal reflectivity and translucency to light makes it favourable for producing thin conductive coatings, with applications in touch screens and flat panel displays[13]. Indium exposure causes interstitial lung disease and emphysema[13]. Exposure cessation does not prevent progression, and lung transplantation may be required in some patients[13].
Conclusion
Cases of CBD are still being diagnosed today in regulated industries as well as incidentally in individuals exposed to previously unknown and unexpected hazards. We reported a case of chronic beryllium disease in a jeweller who was exposed to beryllium through grinding and polishing of beryl gemstones. The mixed nature of most respiratory exposures as well as the long disease latency may make it challenging to identify a primary cause. Other interstitial lung diseases like silicosis that once plagued mining communities are also re-emerging in novel and innovative industries such as artificial stone manufacturing, while exposures to rare earth metals are becoming increasingly common as a result of technological advancements in industries like consumer electronics and prosthesis manufacturing. Avoidance is often not possible in essential first-line workers, but exposure can be managed through personal protective equipment and workplace prevention and screening programmes. Workplace prevention strategies effectively prevent BeS as long as they are adhered to. Metals are strong haptens, and lymphocyte proliferation testing plays an important role in detecting metal sensitization in patients that are occupationally exposed. Workers who become sensitised during the course of their careers are likely to experience progression despite prevention of further exposure, and lifelong medical surveillance is required even after leaving the workplace.
Acknowledgements
Acknowledgements to Miss Heena Ranchod for administrative and procedural assistance.
Ethics granted by:
University of Witwatersrand, Johannesburg; Human Research Ethics Committee (Medical) - Protocol No: M230676
Conflicts of Interests
The authors declare no conflict of interest.
Funding
All administrative costs were covered by the authors.
References
- MacMurdo MG, Mroz MM, Culver DA, Dweik RA, Maier LA. (2020). Chronic beryllium disease: update on a moving target. Chest. 158(6): 2458-2466.
View at Publisher | View at Google Scholar - Roberts KR. (2022). A Comprehensive Summary of Disease Variants Implicated in Metal Allergy. J Toxicol Environ Health B Crit Rev. 25(6): 279-341.
View at Publisher | View at Google Scholar - Soares A, Govender L, Hughes J, Mavakla W, de Kock M, Barnard C, et al. (2010). Novel application of Ki67 to quantify antigen-specific in vitro lymphoproliferation. J Immunol Methods. 362 1(2):43-50.
View at Publisher | View at Google Scholar - Balmes JR, Abraham JL, Dweik RA, Fireman E, Fontenot AP, Maier LA, et al. (2014). An official American Thoracic Society statement: diagnosis and management of beryllium sensitivity and chronic beryllium disease. Am J Resp Crit Care Med. 190(10): 34-59.
View at Publisher | View at Google Scholar - Carroll MB, Kanne JP. (2022). Imaging of Occupational and Environmental Lung Disease. Semin Respir Crit Care Med. 43(6):874-886.
View at Publisher | View at Google Scholar - Wegner R, Heinrich-Ramm R, Nowak D, Olma K, Poschadel B, Szadkowski D. (2000). Lung function, biological monitoring, and biological effect monitoring of gemstone cutters exposed to beryls. Occup Environ Med. 57(2): 133-139.
View at Publisher | View at Google Scholar - Rossman MD. (1996). Chronic beryllium disease: diagnosis and management. Environ Health Perspect. 104(5): 945-947.
View at Publisher | View at Google Scholar - Fontenot AP. (2018). Immunologic Effects of Beryllium Exposure. Ann Am Thorac Soc. 15(2): 81-85.
View at Publisher | View at Google Scholar - Meyer KC, Raghu G, Baughman RP, Brown KK, Costabel U, Du Bois RM, et al. (2012). An official American Thoracic Society clinical practice guideline: the clinical utility of bronchoalveolar lavage cellular analysis in interstitial lung disease. Am J Respir Crit Care Med. 185(9):1004-1014.
View at Publisher | View at Google Scholar - Valeyre D, Brauner M, Bernaudin JF, Carbonnelle E, Duchemann B, Rotenberg C, et al. (2023). Differential diagnosis of pulmonary sarcoidosis: a review. Front Med. 10:1150751.
View at Publisher | View at Google Scholar - Taiwo OA. (2014). Diffuse parenchymal diseases associated with aluminum use and primary aluminum production. J Occup Environ Med. 56(5):71-72.
View at Publisher | View at Google Scholar - Lee HW, Jose CC, Cuddapah S. (2021). Epithelial-mesenchymal transition: Insights into nickel-induced lung diseases. Semin Cancer Biol. 76:99-109.
View at Publisher | View at Google Scholar - Wyman AE, Hine SE. (2018). Update on Metal-Induced Occupational Lung Disease. Curr Opin Allergy Clin Immunol. 18(2): 73–79.
View at Publisher | View at Google Scholar - Zheng M, Marron RM, Sehgal S. (2020). Hard Metal Lung Disease: Update in Diagnosis and Management. Curr Pulmonol Rep 9:37-46.
View at Publisher | View at Google Scholar - Bartter T, Irwin RS, Abraham JL, Dascal A, Nash G, Himmelstein JS, et al. (1991). Zirconium compound-induced pulmonary fibrosis. Arch Int Med. 151(6): 1197-1201.
View at Publisher | View at Google Scholar - Werfel U, Schneider J, Rodelsperger K, Kotter J, Popp W, Woitowitz HJ, et al. (1998). Sarcoid granulomatosis after zirconium exposure with multiple organ involvement. Eur Respir J. 12(3):750-750.
View at Publisher | View at Google Scholar - Dube G, Chiluba BC. (2021). Burden of Silicosis in the South African Mining Sector and its Effects on Migrant Labour from Neighboring Countries. J Prev Rehab Med. 3(1):20-25.
View at Publisher | View at Google Scholar - Jumat MI, Hayati F, Rahim SS, Saupin S, Lukman KA, Jeffree MS, Lasimbang HB, Kadir F. (2021). Occupational lung disease: A narrative review of lung conditions from the workplace. Ann Med Surg. 64:102245.
View at Publisher | View at Google Scholar - Cristaudo A, Sera F, Severino V, De Rocco M, Di Lella E, Picardo M. (2004). Occupational hypersensitivity to metal salts, including platinum, in the secondary industry. Allergy. 60(2):159-164.
View at Publisher | View at Google Scholar
