

Research Article | DOI: https://doi.org/10.31579/2834-8508/015
An Investigation of Three Different Types of Physiotherapy Treatment for Osteoarthritis of the Knees
1Multan Institute of Health Sciences, University of Sargodha, Pakistan
2Government College University Faisalabad, Pakistan
*Corresponding Author: Sadia Zafar, Multan Institute of Health Sciences, University of Sargodha, Pakistan.
Citation: Sadia Zafar, Anita Shahzadi (2023), An Investigation of Three Different Types of Physiotherapy Treatment for Osteoarthritis of the Knees. Archives of Clinical and Experimental Pathology. 2(3); Doi:10.31579/2834-8508/015
Copyright: Copyright: © 2023 Sadia Zafar, This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 11 May 2023 | Accepted: 31 May 2023 | Published: 16 June 2023
Keywords: osteoarthritis, physiotherapy treatment, 15-week period, five evaluations.
Abstract
Medium to long-term findings are reviewed for the nature and application of a physical therapy based on knee osteoarthritis. In a wide population-based sample, patients who had knee pain and prevalent osteoarthritis were enrolled. Fifty patients with Osteoarthritis were treated with periodic knee bath with ultrasound, wax baths and ultrasound. To each strategy, repetitive exercises were applied. The patients were hired over a span of 15 weeks. Everyone endured discomfort, swelling, and reduced mobility. Patients were assigned to one of three care groups by a randomization code. Five evaluations were conducted by an independent investigator prior to admission into the investigation and at the end of weeks 5, 10 and 15. Regardless of the medication, statistically meaningful changes in particular index were found after five weeks. Among the dominant and non-dominant knees, there was no difference in results. All five tests demonstrated a substantial increase in all patient classes at the completion of fifteen weeks of treatment. Ultrasound at the dosage used to be little better at helping patients than wax baths.
1. Introduction
Knee pain is one of the most common presenting complaints in family practice, and the most common cause of knee pain in older people is osteoarthritis [2]. Osteoarthritis of the knee is an example of a condition that is frequently treated by physical therapy with or without drugs. Current guidelines on the management of knee Osteoarthritis suggest that interventions such as physical therapy [1]. However, considering the prevalence of the problem and the potential costs of this approach to the community, the evidence base to support these guidelines has been limited. Many other reported studies have been flawed by lack of randomization, control group, or blinded evaluation and most have only short-term follow up. Two systematic reviews report the results of these evaluations as well as providing descriptions of the interventions, evaluation of methodological quality, and standardized effect sizes [3]. The heterogeneity of knee pain and knee osteoarthritis causes further problems. The evidence base comes mostly from patients recruited from secondary care rather than the community, and concentrates on tibiofemoral joint and patello-femoral osteoarthritis. However, people with knee pain in the community are likely to differ from those who access secondary care [6]. Patient observation at the Bansal Global Hospital, Delhi, revealed that the employ of ultrasound was effective in the therapy of knee osteoarthritis, and that this was improved directly afterwards by providing a periodic knee washes. For the treatment of osteoarthritis in the knees, a number of physiotherapy strategies are available; most treatments are intended to alleviate the effects of stiffness and pain, although there have been less prohibited comparisons of traditional physiotherapy strategies [7]. Both patients and practitioners have access to regular fitness routines that, if carefully administered, can be supplemented at home by the application of wax. We wanted to equate this basic regime with the two other more complex types of physiotherapy mentioned above, which are commonly available in the Physiotherapy Departments of the hospital, to see whether they had some benefits.
2. Materials & Methods
Fifty patients were recruited for the investigation, all with osteoarthritis of the knees and all seeking care at Bansal Global Hospital, Delhi. With the consent of the specialist involved, patients were hired and the proposal had the consent of the central medical ethics committee. Participants of both chronic knee pain and radiographic evidence of prevalent activity of the patello-femoral joint, without advanced improvements in thetibiofemoral joint and without hip disease were chosen. Many of the patients complained of knee pain and swelling and reduced mobility. Both patients had a halfhour conversation with the physiotherapist on diagnosis, prognosis, clothing, weight loss, and exercise at the baseline appointed. There was support for general fitness.
Patients were assigned to one of three groups at random:
Exercise & Wax:
This treatment is performed for 5 weeks. A qualified physiotherapist was given routine activities in the hospital. The wax procedure involved dipping the knees 10 times into molten wax, and covering each knee in a blanket lined with grease proof tape. The patient sat comfortably for 20 minutes [8].
Exercises via Ultrasound:
The workout regimen, was similar to the 5 weeks completed in care group 1. The ultrasound dosage stayed steady with a 3 MHz beam at 250W/cm2 for 5 minutes per knee. Treatment using a constant beam was done in water [9]. Exercise via Periodic Knees Baths and Ultrasound: This therapy lasts for 5 weeks and is normal. As for care group 2, ultrasound was used, and a typical periodic knee bath procedure was used for 10 minutes per knee. The fitness routine was the same as in another group [10]. Patients were examined by an impartial physiotherapist after the investigation, without knowledge of the procedure, instantaneously earlier to therapy (week 0) and at 5, 10 and 15 weeks of treatment. In this concurrent community investigation, treatment was for 15 weeks only. Along with the above-mentioned treatment, some regular exercises are also added. The exercises included:
A. Vastus Medialis Oblique 23 muscle contractions in sitting position like squeezing a rolled-up towel between the knees
B. Exercise 1 with gluteal muscle contractions at the same time
C. Controlled sitting to standing squeezing a rolled-up towel between the knees to encourage contraction of the vastus medialis oblique muscle
D. Controlled small knee bends squeezing a rolled-up towel
E. Controlled stepping up and down steps, emphasizing contraction of the vastus medialis oblique muscle and correct posture
F. 10 maximal isometric quadriceps contractions in mid-range (roughly 70°) using a resistive rubber band and
G. Controlled balancing on one leg for as long as possible.
All exercises were tailored to the patient’s ability to perform them without pain, e.g., they started the exercise sitting at a height they could stand up from without experiencing pain. Exercises were progressively modified by doing lower knee bends, standing up from lower chairs, and stepping up and down from higher steps [11]. Normal demographic details were identified upon entry to the inquiry and the diagnosis of osteoarthritis was confirmed. It noticed the dominant hand and registered the occupation of the patient. The following clinical evaluations were conducted during this and any subsequent evaluation:
Joint Size:
This was the diameter measured using an ordinary tape measure of each tibiofemoral and patellofemoral joint of each leg.
Visual Analogue Scale:
A typical horizontal 25 cm line with ends numbered 'no pain' and 'unbearable pain' uses a graphic analogue scale for pain.
The Articular Index:
At the end of each therapy cycle, the Articular Index was done by the same observer who, using a visual analogue scale, also measured discomfort and reported the length of stiffness in the morning and after sitting. The choice of the patient for one or another medication time was observed at the conclusion of the investigation [4].
Each joint was scored as 0 = no pain; 1 = recorded pain; 2 = pressure wincing; 3 = knee withdrawal when the joint is palpated.
Schober’s test:
The movement range was using a process similar to the Schober spine test. At the location of the knee, a tape measure was fixed and stretched around the length of the knee and over the tibiofemoral and patellofemoral joints. Both the knee joints were then flexed and stretched, tracking the subsequent motion of the tape over the tibiofemoral and patellofemoral joints on a pen mark. With each knee, this was done [5].
Activities Score:
Patients were asked to walk, run, jumping and sitting. There was a record of their abilities to execute these basic everyday activities.For statistical use, the measurements for tibiofemoral and patellofemoral joint and the range of movement of the knee were summated.
3. Statistical Analysis
In the contrast of therapies, mathematical research utilized the Kruskal-Wallis H Test or analysis and was extended to serial shifts in measures. On any baseline evaluation, the groups were good balanced and displayed no statistically meaningful difference. For every of the care groups, Table 1 & Figure 1 displays the average value for each measurement over 15 weeks.
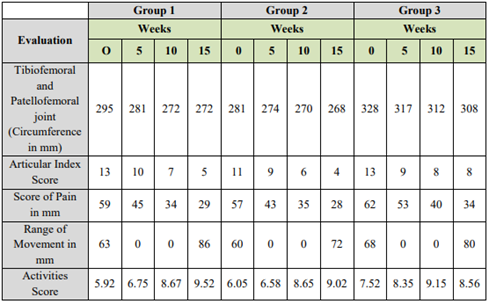
Table 1. Average Value of Each Measurement with Each Therapy
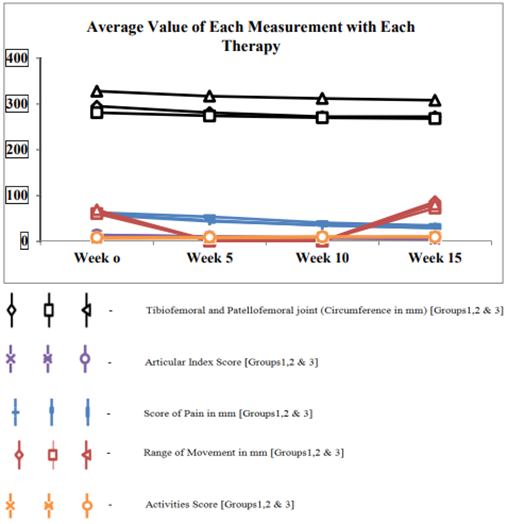
Figure 1. Average Value of Each Measurement with Each Therapy
For each evaluation, the 3 therapy classes were compared to see how further progress was correlated with each one therapy. Table 2 displays the results.
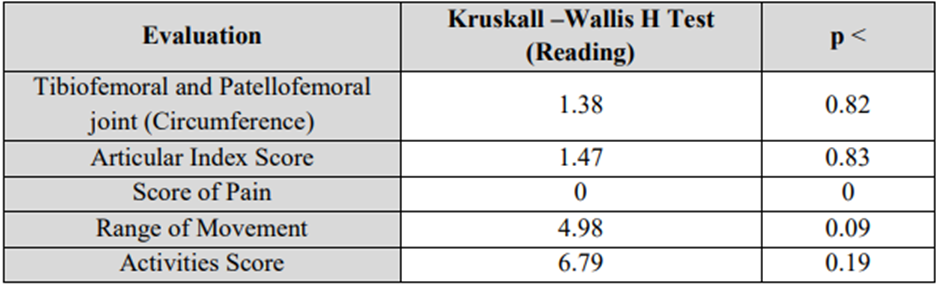
The task score was the only evaluation to indicate a meaningful difference (p<0>
Table 2. Kruskall-Wallis H Test or analysis by Ranks – Comparison of Treatments
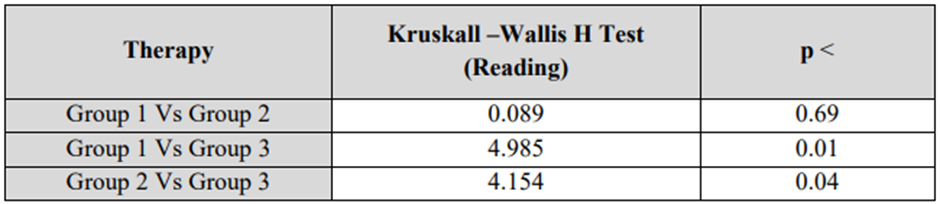
Table 3. Kruskall-Wallis H Test or analysis by Ranks – Comparison of Therapy (Activity Score)
Examination of patient reports showed two patients with a reduction in score. During the 15th week of the inquiry, patient No 7 experienced a generalized 'flareup' (after initial improvement). But for the pain score (visual analogue) and articular index of the left knee only, patient No 17 did not change or deteriorate in the investigation.
For any of the remaining four evaluations, no major variations could be shown and it thus is doubtful that, at 15 weeks, the three therapy groups varied substantially. For any calculation for each treatment, a distinction was made between week 0 and each following week.
Table 4 summarizes the findings. A marked increase was seen in nearly all outcomes in all three therapy classes, and a clinically meaningful increase was seen in 50 percent of patients following just 7 days of treatment.
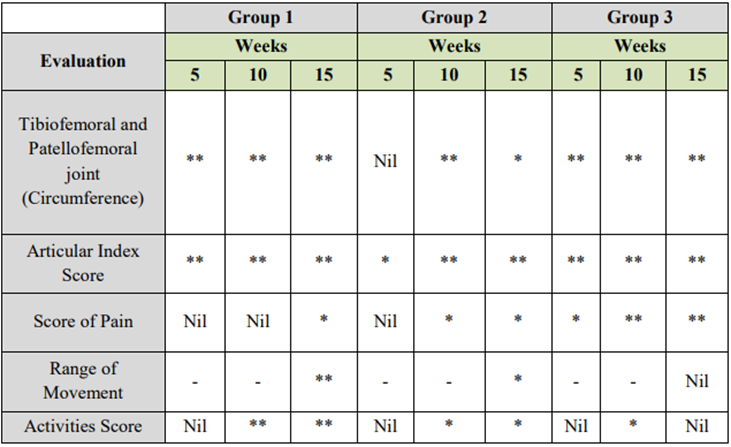
Nil – Represent No Significant Occur through the Measurement of Evaluation
* – Represent Significant at 0.05 (p<0>
** – Represent Significant at 0.01 (p<0>
Table 4. Applied Wilcoxon Rank Sum Test to the consecutive Modification in the Measurement of Evaluation
The probabilities of a disparity in reaction between the non-dominant and dominant hands were measured by measuring the various between the two knees between week 0 and week 15 for those measurements where the findings of the right and left knees were visible. The left knee was dominant in 45 of the 50 patients. [12] Using the Wilcoxon rank sum test practical to the tibiofemoral and patellofemoral joint size, range of movement, and articular index, distinctions were sought. On any of the three steps, the procedure was administered to all 50 patients, and also for any assessment of these steps. The reaction of the two knees to any care did not vary significantly.
Table 5 displays the thorough measures of two patients to demonstrate the sequence of outcomes. Figure 2 and Figure 3 shows the demonstrate sequence of the results of the Patient 1(No. 7) and Patient 1(No. 17)
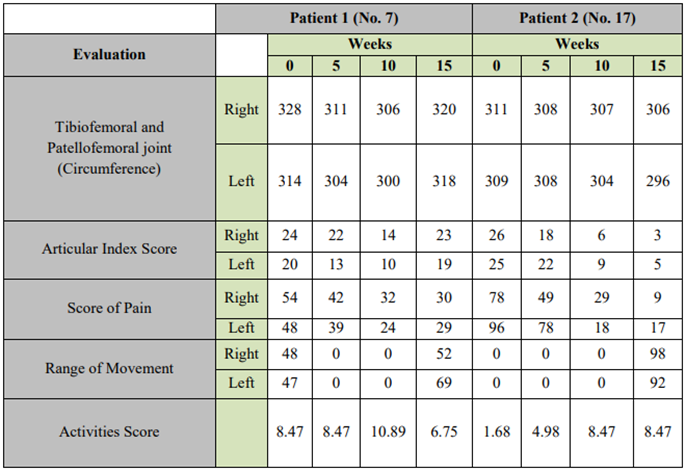
Table 5. Evaluation Score of the Individual Two Patients Patients
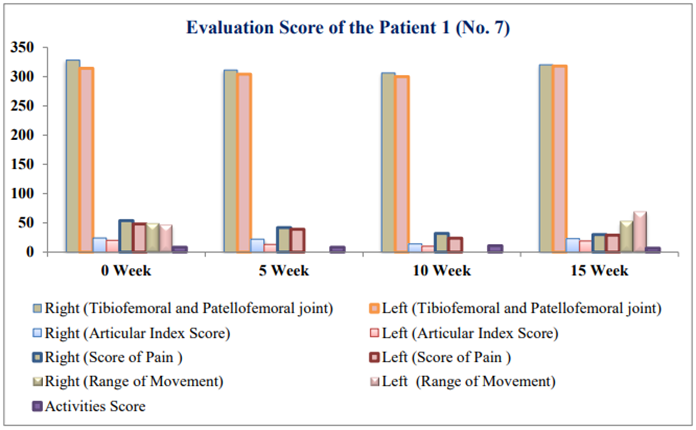
Figure 2. Evaluation Score of the Patient 1 (No. 7)
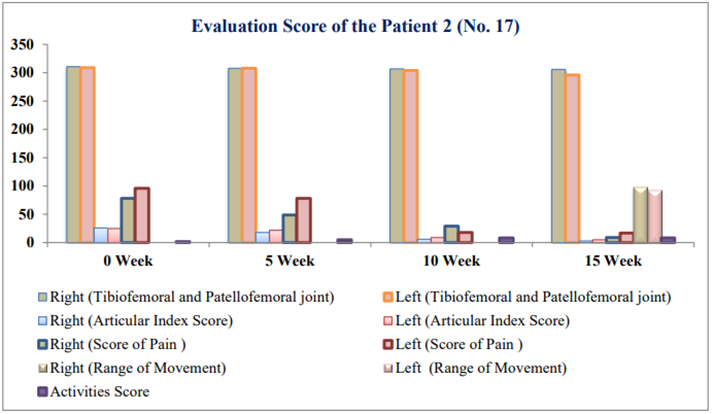
Figure 3. Evaluation Score of the Patient 2 (No. 17)
4. Conclusion
The employ of ultrasound alone, or ultrasound plus periodic knee baths, has little benefit over the employ of routine exercises and wax in the treatment of patients with knee osteoarthritis, although the findings indicated a substantial change with all the approaches used. The test knees suggest that wax had some benefits in this analysis. This is demonstrated by the ratings of the articular index and the spectrum of motion results. If therapy of wax at home is as successful as therapy at the hospital, the patient's wellbeing should be assured. Owing to the effects of the tension of the ride, vulnerability to freezing and unnecessary waits when waiting for the bus or ambulance service, journeys to the hospital for care are frequently counter-productive. The investigation procedure-imposed restrictions on the length and severity of the ultrasound to ensure that every patient received identical care. In regular practice, the dose will differ according to the patient's preferences and reaction. This may have a material effect on the outcomes, and a further analysis of the variable dosage with the fixed dose would be important additional research.
5. Acknowledgements
We would like to thank the employees of the Department of Physiotherapy at Bansal Global Hospital, Delhi, for their assistance with the treatment of patients.
References
- Brosseau, L., Wells, G. A., Kenny, G. P., Reid, R., Maetzel, A., Tugwell, P., & Chen, L. The implementation of a community-based aerobic walking program for mild to moderate knee osteoarthritis (OA): a knowledge translation (KT) randomized controlled trial (RCT): Part I: The Uptake of the Ottawa Panel clinical practice guidelines (CPGs). BMC public health, 2012; 12(1), 871.
View at Publisher | View at Google Scholar - Hirano, K., Imagama, S., Hasegawa, Y., Ito, Z., Muramoto, A., & Ishiguro, N. Impact of low back pain, knee pain, and timed up-and-go test on quality of life in community-living people. Journal of Orthopaedic Science, 2014; 19(1), 164-171.
View at Publisher | View at Google Scholar - Petrella RJ. Is exercise effective treatment for osteoarthritis of the knee? Br J Sports Med 2000; 34: 326-31.
View at Publisher | View at Google Scholar - Migliore, A., Bella, A., Bisignani, M., Calderaro, M., De Amicis, D., Logroscino, G & Laganà, B. Total hip replacement rate in a cohort of patients affected by symptomatic hip osteoarthritis following intra-articular sodium hyaluronate (MW 1,500–2,000 kDa) ORTOBRIX investigation. Clinical rheumatology, 2012; 31(8), 1187-1196.
View at Publisher | View at Google Scholar - Yen, Y. R., Luo, J. F., Liu, M. L., Lu, F. J., & Wang, S. R. The anthropometric measurement of schober’s test in normal taiwanese population. BioMed Research International, 2015.
View at Publisher | View at Google Scholar - Dy, C. J., Franco, N., Ma, Y., Mazumdar, M., McCarthy, M. M., & Della Valle, A. G. Complications after patello-femoral versus total knee replacement in the treatment of isolated patello-femoral osteoarthritis. A meta-analysis. Knee Surgery, Sports Traumatology, Arthroscopy, 2012; 20(11), 2174-2190.
View at Publisher | View at Google Scholar - Hunt, M. A., Keefe, F. J., Bryant, C., Metcalf, B. R., Ahamed, Y., Nicholas, M. K., & Bennell, K. L. A physiotherapist-delivered, combined exercise and pain coping skills training intervention for individuals with knee osteoarthritis: a pilot investigation. The knee, 2013; 20(2), 106-112.
View at Publisher | View at Google Scholar - Kjeken, I., Grotle, M., Hagen, K. B., & Østerås, N. Development of an evidence-based exercise programme for people with hand osteoarthritis. Scandinavian journal of occupational therapy, 2015; 22(2), 103-116.
View at Publisher | View at Google Scholar - Henricsdotter, C., Ellegaard, K., Klokker, L., Bartholdy, C., Bandak, E., Bartels, E. M., & Henriksen, M. Changes in ultrasound assessed markers of inflammation following intra-articular steroid injection combined with exercise in knee osteoarthritis: exploratory outcome from a randomized trial. Osteoarthritis and Cartilage, 2016; 24(5), 814-821.
View at Publisher | View at Google Scholar - Al Malty, A. M., Jebril, M., AbuTariah, H., & Albostanji, S. The Effect of Paraffin Wax and Exercise vs. Exercise Treatment on Keyboard User's Hands Pain and Strength. Indian Journal of Physiotherapy & Occupational Therapy, 2014; 8(1), 171.
View at Publisher | View at Google Scholar - Tanaka, R., Ozawa, J., Kito, N., & Moriyama, H. Efficacy of strengthening or aerobic exercise on pain relief in people with knee osteoarthritis: a systematic review and meta-analysis of randomized controlled trials. Clinical rehabilitation, 2013; 27(12), 1059-1071.
View at Publisher | View at Google Scholar - Divine, G., Norton, H. J., Hunt, R., & Dienemann, J. A review of analysis and sample size calculation considerations for Wilcoxon tests. Anesthesia & Analgesia, 2013; 117(3), 699-710.
View at Publisher | View at Google Scholar
