

Case report | DOI: https://doi.org/10.31579/2834-796X/024
Acute Myocardial Infarction due to Coronary Embolism in a young Woman with Mechanical Aortic Valve Prosthesis and Anomalous Origin of two Coronary Vessels: Case Report
- Fernando Araque-Villaquirán 1
- Raúl Vallejo-Serna 2
- Mónica Fernandes-Pineda 3
- Álvaro Herrera-Escandón 4
1,2 Internist, Department of Internal Medicine, Hospital Universitario del Valle, Cali, Colombia.
3 Third-year Internal Medicine Resident, Department of Internal Medicine, Universidad del Valle, Cali, Colombia.
4 Internist, Cardiologist, Department of Internal Medicine, Hospital Universitario del Valle, Cali, Colombia.
*Corresponding Author: *Corresponding Author: Mónica Fernandes-Pineda, Hospital Universitario del Valle, Santiago de Cali - Colombia.
Citation: Fernando A, Villaquirán, Raúl V. Serna, Mónica F. Pineda, Álvaro H.-Escandón, (2023), Acute Myocardial Infarction due to Coronary Embolism in a young Woman with Mechanical Aortic Valve Prosthesis and Anomalous Origin of two Coronary Vessels: Case Report, International Journal of Cardiovascular Medicine, 2(3); DOI:10.31579/2834-796X/024
Copyright: © 2023, Mónica Fernandes-Pineda. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 22 May 2023 | Accepted: 05 June 2023 | Published: 08 June 2023
Keywords: case report; myocardial infarction; coronary thrombosis; mechanical valve thrombosis
Abstract
Introduction : Myocardial infarction due to embolic occlusion of the coronary arteries is rare. The presence of mechanical prosthetic valves carries an increased risk of thromboembolic events.
Objective : Coronary embolism is potentially fatal. We present in this case that the lack of pharmacological adherence and the lack of education in a patient with high thromboembolic risk could be cause of coronary embolism.
Case Report : We present the case of a young woman with a history of aortic insufficiency which was corrected with a mechanical valve prosthesis at 8 years of age and who was in treatment with warfarin. She was admitted to the emergency department in the context of acute ST elevation myocardial infarction. Coronary angiography showed an occlusive lesion in the left anterior descending artery and a thrombotic lesion in the first obtuse marginal artery. As an incidental finding, an anomalous origin of the right coronary artery and the second obtuse marginal artery were found independently from the left coronary sinus. Two years before hospital admission, she voluntarily discontinued anticoagulation.
Conclusion : Permanent anticoagulation, close clinical follow-up and patient education are the most important measures to prevent new events in the future.
Introduction
Valvulopathies affect approximately 2.5% of adults in developed countries. Since 1960, mechanical prosthetic valves have been used for the management of valvular disease. Their main complication is the development of device thrombosis or embolic phenomena, with estimated annual incidences of 0.3-1.3% and 0.7-6%, respectively [1]. The risk is increased in the first few months after implantation, depending on the anatomical position of the valve and its association with other thromboembolic risk factors (e.g., atrial fibrillation).
We present a case of embolic acute myocardial infarction with ST elevation in a young woman with an aortic prosthetic valve who had voluntarily discontinued anticoagulation.
Case Report
A 23-year-old woman from the Colombian Pacific region presented with a history of mitral insufficiency and mechanical valve prosthesis implantation at 8 years old. She was anticoagulated with warfarin until 2 years ago when she voluntarily discontinued medical management. She came to the emergency department complaining of severe oppressive chest pain radiating to her right upper limb for the past 8 hours, without any other associated symptoms. There were no previous reports of substance abuse. Upon physical examination, she was afebrile with a blood pressure of 121/76 mmHg, heart rate of 82 bpm, and respiratory rate of 19 rpm. Auscultation revealed a grade III/VI holosystolic murmur at the mitral area and a grade III/VI diastolic murmur at the aortic area, with no signs of acute heart failure or other relevant findings. The electrocardiogram showed sinus rhythm with ST segment elevation in leads V1 to V3 and ST segment depression in the inferior wall, along with pathological Q waves in leads DI and aVL, indicating signs of left ventricular hypertrophy. An urgent coronary angiography was performed 12 hours after admission, revealing a chronic total occlusion in the mid-proximal segment of the anterior descending artery (Figure. 1) and a thrombotic lesion with 90% stenosis in the first obtuse marginal artery (Figure. 2). No other angiographically significant lesions were found, but there was evidence of loss of mobility of one of the leaflets of the double-disc mechanical valve due to "in situ" thrombus formation.
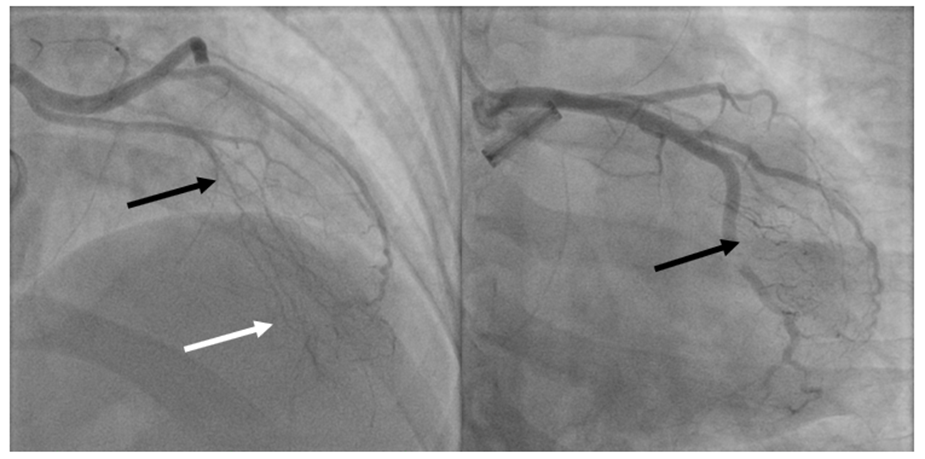
Figure 1 : Left side) Chronic occlusion of the left anterior descending artery at the junction of the proximal to mid segment (black arrow) with hetero and homocoronary collateral circulation (white arrow). Right side) Marginal obtuse artery with luminal filling defect consistent with thrombus causing subocclusion and TIMI 2 flow (black arrow).
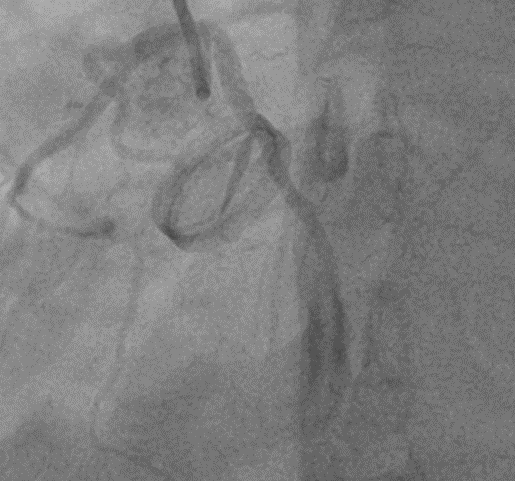
Figure 2 : Loss of mobility of one of the hemi-discs of a double-disc mechanical prosthesis due to "in situ" thrombus.
As an incidental finding, an anomalous origin of the right coronary artery and the second obtuse marginal artery independently from the left coronary sinus was observed. Due to the high risk of valve thrombosis, initial management included low-molecular-weight heparin and warfarin anticoagulation until reaching target international normalized ratio (INR) levels. Laboratory tests showed a positive cardiac troponin I level of 6,530 ng/ml (upper limit: 0.12 ng/ml). Transesophageal echocardiography revealed akinesis without thinning of the anterolateral and inferolateral walls, with an ejection fraction of 47% by Simpson's method. The aortic mechanical prosthesis was in an appropriate position with restricted leaflet movement posteriorly and evidence of pannus formation and marked turbulence in anterograde flow, with a maximum velocity of 3.2 m/s and a mean gradient of 22.5 mmHg. There was severe mitral regurgitation secondary to anterior leaflet perforation.
With these findings, the patient underwent aortic prosthesis replacement with a Medtronic mechanical prosthesis size 23. Aortic annulus enlargement was performed using a heterologous pericardial patch with the Manougian technique. Mitral valve repair was also conducted by closing the anterior leaflet perforation. Fresh thrombi were found on both discs' hinges of the aortic mechanical prosthesis, along with severe subvalvular pannus. Due to the presence of epicardial-pericardial adhesions from previous surgery, it was not possible to perform revascularization of the anterior descending artery. Therefore, coronary angioplasty was indicated. In the second coronary angiography performed 25 days after admission, complete resolution of the thrombotic lesion in the obtuse marginal artery was observed, while the total occlusion of the anterior descending artery persisted. Percutaneous revascularization was not feasible due to the small caliber of the vessel. It was decided to continue with medical treatment, psychological support, and education. The patient was discharged after 41 days of hospitalization without complications, with an INR of 3.2, and with instructions for strict medical follow-up.
Discussion
Ischemic heart disease is the leading cause of death worldwide and is primarily associated with atherosclerosis. However, in up to 7% of cases, significant atherosclerotic lesions are not found, and coronary embolism is a cause of non-atherosclerotic myocardial infarction. It is estimated that coronary embolism accounts for 3% of all myocardial infarctions and typically affects the left coronary circulation [1], as in the case of our patient.
The main associated causes are atrial fibrillation, cardiomyopathies, presence of prosthetic valves, endocarditis, tumors, and prothrombotic states. There are reports of coronary thrombosis associated with acute SARS-CoV-2 infection during the pandemic caused by this entity [2]. Before the use of prosthetic valves, endocarditis was the main cause, but currently, atrial fibrillation is considered the primary cause [1]. Currently, prosthetic valves are the gold standard for managing severe valvulopathies in patients with low or intermediate surgical risk. Mechanical valves have a longer lifespan but carry a prothrombotic risk, requiring indefinite anticoagulation to prevent valve thrombosis and embolic events [3].
There are three types of coronary embolism: direct, paradoxical, and iatrogenic. Direct coronary embolism occurs when an embolus enters the coronary circulation from the left ventricle, left atrial appendage, pulmonary veins, aortic valve, or mitral valve [4].
The clinical, electrocardiographic, and echocardiographic manifestations of myocardial infarction due to coronary embolism are indistinguishable from those of atherosclerotic origin. It should be suspected in cases of sudden chest pain in patients with prothrombotic risk factors [5].
Currently, there are no guidelines for the management of coronary embolism. The aspiration of intracoronary thrombus has been compared to standalone angioplasty in patients with ST-elevation myocardial infarction (STEMI), but no additional benefit in terms of mortality has been demonstrated. However, patients with a high thrombotic burden, such as those with coronary embolism, may derive greater benefit from this approach [6]. There are reports of systemic thrombolysis in coronary embolism using tissue plasminogen activator (t-PA) with successful restoration of coronary flow. Karakoyun et al. [25] successfully and safely treated three patients with coronary embolism associated with prosthetic valves using low-dose intravenous t-PA. Additionally, there is a report of 48-hour intravenous bivalirudin infusion in coronary embolism of the distal right coronary artery with complete resolution of the thrombus without major bleeding [3]. Other therapies include balloon angioplasty, which has shown successful restoration of blood flow both as a standalone therapy and as a complementary therapy to thrombus aspiration [6].
Conclusions
We described the case of a young woman with a mechanical aortic valve prosthesis who voluntarily discontinued anticoagulation and subsequently experienced an acute myocardial infarction due to coronary embolism. This condition is potentially life-threatening, highlighting the importance of pharmacological adherence and patient education in a high-risk thrombosis patient. Multidisciplinary management, including permanent anticoagulation, strict clinical follow-up, and patient education, are crucial measures to prevent further events.
References
- Roudaut, R., Serri, K., & Lafitte, S. (2007). Thrombosis of prosthetic heart valves: diagnosis and therapeutic considerations. Heart (British Cardiac Society), 93(1), 137–142.
View at Publisher | View at Google Scholar - Prizel KR, Hutchins GM, Bulkley BH. Coronary artery embolism and myocardial infarction. Ann Intern Med. 1978 Feb;88(2):155-61.
View at Publisher | View at Google Scholar - Steinwender C, Hofmann R, Hartenthaler B, Leisch F. Resolution of a coronary embolus by intravenous application of bivalirudin. Int J Cardiol. 2009 Mar 6;132(3):e115-6.
View at Publisher | View at Google Scholar - Chikkabasavaiah N, Rajendran R. Percutaneous coronary intervention for coronary thrombo embolism during balloon mitral valvuloplasty in a pregnant woman. Heart Lung Circ 2016;25:e29-31.
View at Publisher | View at Google Scholar - Lacey MJ, Raza S, Rehman H, Puri R, Bhatt DL, Kalra A. Coronary Embolism: A Systematic Review. Cardiovasc Revasc Med. 2020 Mar;21(3):367-374.
View at Publisher | View at Google Scholar - Karakoyun S, Gürsoy MO, Kalçık M, Yesin M, Özkan M. A case series of prosthetic heart valve thrombosis-derived coronary embolism. Turk Kardiyol Dern Ars. 2014 Jul;42(5):467-71.
View at Publisher | View at Google Scholar
