

Review Article | DOI: https://doi.org/10.31579/2835-2882/054
A Review on The Combating of Covid-19 In Africa
1Department of Public Health, National Open University of Nigeria, Uromi Community Study Centre, Uromi, Edo State, Nigeria.
2Lassa Fever Enable Study CEPI/ISTH Irrua, Edo State, Nigeria.
*Corresponding Author: Kenneth Iyevhobu, Department of Public Health, National Open University of Nigeria, Uromi Community Study Centre, Uromi, Edo State, Nigeria.
Citation: Kenneth Iyevhobu and Airefetalor, A.I, (2024), A Review on The Combating of Covid-19 In Africa, Clinical Research and Studies, 3(4); DOI:10.31579/2835-2882/054
Copyright: © 2024, Kenneth Iyevhobu. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 05 August 2024 | Accepted: 14 August 2024 | Published: 22 August 2024
Keywords: mycotoxins; aflatoxin; fumonisin
Abstract
The World Health Organization (WHO) is an agency of the united nation, founded on 7th April 1948 operating in 147 countries with an ambitious objective – ‘the attainment by all peoples of the highest possible level of health’. As the name implies it is an organization whose core objectives are to achieve a high level of health standard for the world through underlying function such as directing and coordinating the health system, assessing and monitoring health situation as well as provide technical support, relief materials among others. The current Coronavirus Disease (COVID-19) outbreak has affected over 200 countries including Nigeria. It is one of the largest respiratory disease outbreaks affecting several countries simultaneously and a novel strain of Coronavirus (SARS-CoV 2) has been identified as the causative agent. Sequel to the advice of the International Health Regulation Emergency Committee, the Director-General of WHO declared the COVID-19 outbreak a Public Health Emergency of International Concern (PHEIC) on 30 January 2020 and characterized it as a pandemic on 11 March 2020. The World Health Organization (WHO), the UN’s health agency, has played a crucial role in tackling the COVID-19 pandemic, ever since the first cases were identified in the Chinese city of Wuhan in December. Owing to the nature of the African continent, the World Health Organization observed that the impact of COVID-19 on Africa could be different due to the continents demographics, health system, risks exposure and economic factors. The World Health Organization in the African region put some strategic objectives in place to ensure all countries in the continent are able to provide the response capacities at all levels to curtail the spread and manage the impact of the pandemic.
Introduction
Novel coronavirus named severe acute respiratory coronavirus 2 (SARS-CoV-2) was first identified in a seafood market in Wuhan City, Hubei Province in China, at the end of 2019 (Zhu, Zhang, Wang, Li, Yang, Song, Zhao, Huang, Shi & Lu, 2020). The contagious respiratory illness caused by this novel coronavirus is called coronavirus disease 2019 or, in short, COVID-19 (Wu, Chen & Cai, 2020). The World Health Organization (WHO) declared it as a pandemic on 11th March 2020 due to its serious and rapid spread (World Health Organization, 2020-d). Four months after its emergence, the virus had spread to many countries and officially infected over 25 million people and claiming over 865,644 lives on 2nd September 2020 (Worldometer Statistics, 2020). From February, COVID-19 cases soared across most of Europe, the United States, Australasia, Asia and on to Africa. Until now, the novel coronavirus continues to wreak havoc on daily life around the globe, affecting 213 countries, infecting 8,018,963 people and killing 436,138 people (until 15 June 2020; Worldometer, 2020).
Meanwhile WHO’s secure funding from governments has stagnated and it has become reliant on voluntary contributions from governments and other actors usually earmarked for particular activities favoured by the donor. In recent years, the Bill & Melinda Gates Foundation has become one of the biggest voluntary contributors to WHO. As a result of the acute funding pressures, Director-General Margaret Chan initiated in 2010 the launch of what became a fresh effort to reform how the organization functions (Moeti, 2020).
COVID-19 pandemic, originating from Wuhan (China) in December 2019, has taken the world by storm. The first case in Nigeria was reported on 27 February 2020 (Nigeria Coronavirus, 2020). Since then, the disease has continued to spread like wild fire. Four months on, there are 198,883 confirmed cases and 4,035 deaths in Nigeria (Nigeria Coronavirus, 2020). Covid-19 (Sars-CoV-2) is a dangerous infectious disease with the risk of life-threatening pulmonary complications (Guan, Ni, Hu, Liang, Ou & He, 2020; Li, Guan, Wu, Wang, Zhou & Tong, 2020).
It is a disease which affects the respiratory system of a person, presenting signs and symptoms ranging from mild ones such as fever, dry cough and common cold, to severe ones such as pneumonia, Middle East Respiratory Syndrome (MERS) and Severe Acute Respiratory Syndrome (SARS) (WHO, 2020). It is transmitted from person to person through direct contact with one who is infected, or when infected respiratory droplets land on the nose, mouth, or eyes of a healthy individual (Okoli & Bwawa, 2020).
Since the number of infected people and the mortality rates increase worldwide, many countries decided for a nationwide lockdown (Klompas, Morris, Sinclair, Aearson & Shenoy, 2020). Further strategies focus on early diagnosis of Sars-CoV-2 infection, which is known to result in flu-like symptoms, such as fever, sore throat and dry cough (Chen, Zhou, Dong, Qu, Gong & Han, 2020; Guan et al., 2020; Singhal, 2020). Social contact with infected people is considered as a high-risk situation and, therefore, several institutions, including hospitals, implemented screening areas including temperature controls at the entrance (Bitar, Goubar & Desenclos, 2009; Gostic, Gomez, Mummah, Kucharski & Lloyd-Smith, 2020; Klompas et al., 2020).
For obvious reasons, healthcare setups are most likely to be congested with infected patients. Infection control practices to limit spread of this viral disease should focus on targeting patients/ visitors right at the point of entry into hospitals. Considerable time can lapse during physician encounter and subsequent period waiting for results of investigations. Spread of infection to others during this period is very likely. Outside of hospitals, body temperature is not an effective COVID-19 screening tool for multiple reasons (Bwire & Paulo, 2020). However, recording body temperature would provide the quickest way to separate suspected infectious patients from others in the emergency departments (McAlister et al., 2021). This is important because patients are known to avoid self- reporting fever during pandemics (Tay, Low, Zhao, Cook & Lee, 2015). Fever is a common symptom of COVID-19, typically appearing 2-14 days after exposure. In view of the above, it becomes important to review combating COVID-19 in Africa from its onset till date.
Covid-19 In Africa
The spread of COVID-19 is accelerating across the world. In Africa, most countries have now confirmed cases and the number of fatalities is rising. If allowed to spread unmanaged, the impact on African citizens and economies will be substantial. According to OECD (2020), a fatal impact of the COVID-19 pandemic on the African health system could lead to a state of social and economic crises which may directly result in drastic effect on economies and societies (OECD, 2020). The pandemic could cripple the economy since it has a high chance to overburden the health sector, hence the need to invest in the health system in the continent (Sherrad-Smith et al., 2020; Glatman-Freedman et al., 2021).
Africa may yet be worst hit by this invisible disease. Africa’s already fragile health systems, coupled with a high burden of respiratory and diabetic diseases and densely packed urban agglomerations, are likely to increase the vulnerability of the continent and the lethality of the virus. According to Dr Tedros Adhanom Ghebreyesus of the World Health Organization (WHO), Africa should "wake up" to the COVID-19 threat and prepare for a worst-case scenario. The speed with which countries can detect, report and respond to outbreaks can be a reflection of their wider institutional capacity. Epidemics are a reality test for public governance and leadership, not only at country level, but also at regional and continental levels, as well as in connection with the wider network of multilateral actors and partners (Nahtulya & Mavhinga, 2020).
Following the coronavirus outbreak in China in late December, and its spread to parts of Asia, Europe, the Middle East and the US, Africa seems to have been spared a major outbreak for months, recording its first confirmed case only on 14 February in Egypt. Though Africa has close ties with China, its risk of importation of COVID-19 based on travel exposure to China is lower compared to Europe (1% to 11% respectively) according to The Lancet, perhaps explaining the relatively late spread of the virus on the continent. As of 25 March, numbers stay limited in comparison to other regions: 43 African countries are now treating 2,412 patients with coronavirus, and 64 deaths have been registered. At this stage, however, it remains questionable whether these low figures reflect reality or a lack of robust data (Watch Human Right, 2020).
Nevertheless, while there is no common agreement by experts about whether and when the COVID-19 pandemic might or will explode in Africa, there are signals that Africa is particularly vulnerable to the virus and its lethality could be higher in the continent. In cooperation with the African Union Commission (AUC) and the WHO, Africa CDC established the Africa Taskforce for Coronavirus (AFCOR), with six work streams (WHO, 2020):
• laboratory diagnosis and subtyping
• surveillance, including screening at points of entry and cross-border activities
• infection prevention and control in healthcare facilities
• clinical management of people with severe COVID-19
• risk communication
• supply-chain management and stockpiles
This has led to the continent notably stepping up its preparedness measures for COVID-19. As of 7 March, at least 43 African laboratories in 43 African countries have already been trained to diagnose the virus while in the beginning of February only two laboratories - in Senegal and South Africa - had been capable to test for the virus. Several training exercises for incoming analysts as well as African experts and countries have been held to prepare for and enhance events-based surveillance. 22 AU member states were trained to strengthen infection prevention and control capacities in healthcare facilities and with the airline sector. Using a free online training course by the WHO 11,000 African health workers have been trained on the virus and the Africa CDC has trained government officials from 26 countries in public information management. In addition, individual countries in Africa are taking necessary steps to enhance their preparedness and to limit the risk of spreading. For example, Nigeria trained rapid response teams in all 36 states which can be deployed in the case of an outbreak, Kenya opened a quarantine centre in Nairobi for suspected cases and Rwanda has put up mobile hand washing sets for public transport passengers (WHO, 2020).
Globally, cases of the Alpha variant have been reported in 195 countries, territories or areas (hereafter countries; two new countries added since last week), while 145 countries (3 new country since last week) have reported cases of the Beta variant; and 99 countries have reported cases of the Gamma variant (4 new countries since last week, with 1 report of the Gamma variant from last week being discarded upon sequencing). The Delta variant has been reported in 192 countries (seven new countries since last week (Teyssou, Delagrèverie & Visseaux, 2021): 2 under verification and 5 verified), across all six WHO regions as of 5 October (Offiong, 2020; Watch Human Right, 2020). And in the most populous countries on the continent, vaccination rates are still very low. In Nigeria, only 1.9 doses of vaccines have been administered per 100 people, in Ethiopia it's 1.8 and in Kenya 2.8 doses. It's slightly higher in Egypt at 4.5 doses, and in South Africa, it is 7.1 (Emary, Golubchik & Aley, 2021).
COVID-19 in Nigeria
Nigeria is one of the 210 countries affected globally. The first case was confirmed in Lagos State on 27 February 2020. This index case was a 44-year old man, an Italian citizen who returned from Milan, Italy, on 24 February and presented at a health facility on 26 February 2020 (Nigeria Centre for Disease Control, 2020-a). Following the confirmation of the index case, 216 people were identified as contacts to be followed up. Of these, 45 travelled out of Nigeria and one of the remaining 176 contacts was confirmed to be positive for COVID-19 on 9 March 2020 (Nigeria Centre for Disease Control, 2020-b).
The country has continued to experience an increase in the number of cases, which has spread across several states. While majority of the initial cases were imported, most of the new cases have no travel history or contact with such people. This is highly suggestive of ongoing community transmission (Curran, Dol & Boulos, 2021). Under the current circumstances, the Primary Health Care (PHC) Centres remain the most likely port of call for community members who develop symptoms that could be suggestive of COVID-19.
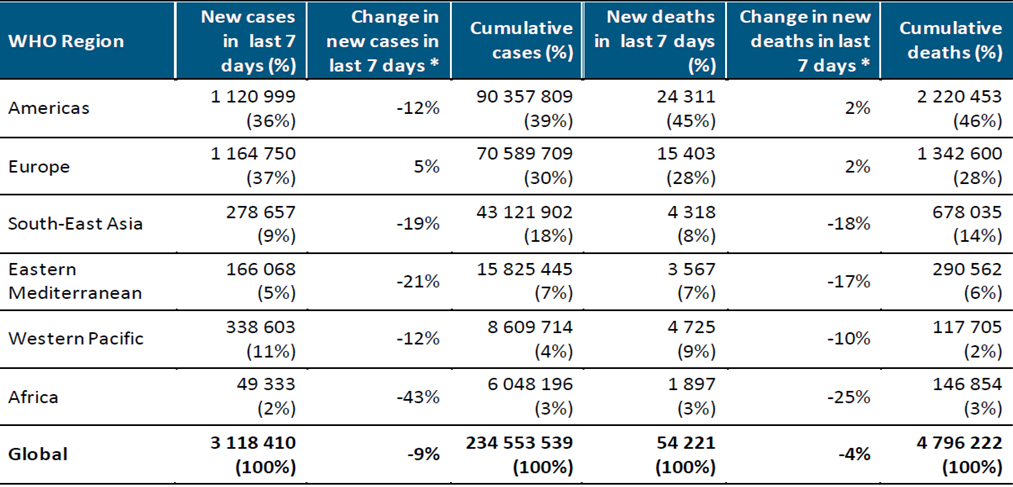
*Percent change in the number of newly confirmed cases/deaths in past seven days, compared to seven days prior (WHO, 2020)
Table 1: Newly reported and cumulative COVID-19 cases and deaths, by WHO Region, as of 3 October 2021**
The Primary Health Care system is the bedrock of the country’s health system (Federal Ministry of Health, Nigeria, 2019) and the Community Health Workers (CHWs) are considered to be its backbone for several reasons (Mailman School of Public Health, 2017). In addition to contributing to several successful immunization, maternal, newborn, child health and reproductive health services, CHWs also played a critical role in the epidemic response to the 2014 Ebola Viral Disease Outbreak (EVD) across several West African countries, including Nigeria (Perry et al., 2016). In the face of continued COVID-19 community transmission, the health system may likely become overwhelmed with increased risk of health workers’ infection (Curran et al., 2021). Considering the fact that most people use the PHC centres, especially those in the rural and hard-to-reach areas, it is important that the staff should be adequately informed and resourced to provide first level care such as screening and referral of patients. On this ground, we described the current situation of the outbreak and argued the need for effective engagement of community health workers for appropriate responses to COVID-19 (Hagan, 2021).
With enhanced surveillance systems deployed across Nigeria, the Nigeria Centre for Disease Control (NCDC) continues in its effort to detect, respond and control the spread of the coronavirus disease (COVID-19) outbreak in Nigeria. The Federal Government of Nigeria through the Presidential Task Force on COVID-19 (PTF COVID-19) and the Federal Ministry of Health continue to work collaboratively to review national response strategies and institute measures to effectively curb the spread of the disease (Glatman-Freedman et al., 2021). Furthermore, the NCDC-led national Emergency Operations Centre (EOC) continues to meet daily for coordination of national response activities with relevant Ministries, Department and Agencies (MDAs) and partners. The NCDC has also supported 23 states to establish Public Health Emergency Operations Centre (PHEOC) to strengthen state-level preparedness for and response to the disease outbreak. This whole-of-government approach is vital to combating the disease in Nigeria (Hagan, 2021).
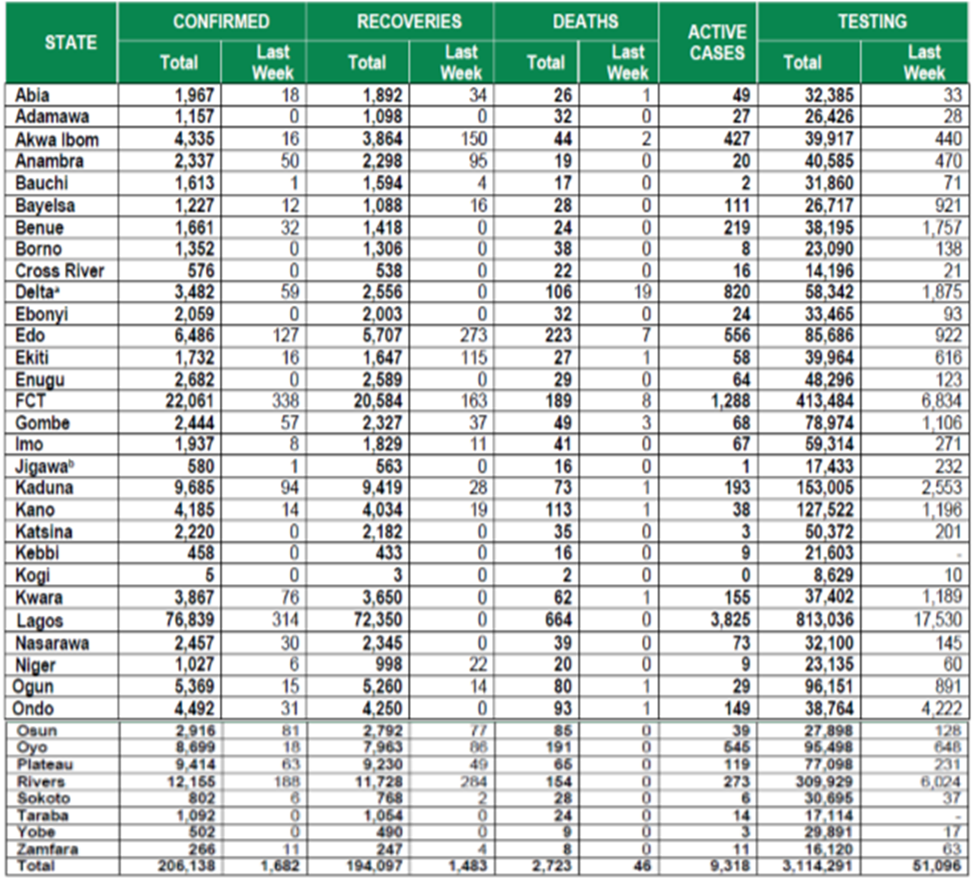
Table 2: States with reported laboratory-confirmed COVID-19 cases, recoveries, deaths, samples tested and active cases.
NB: aThis includes backlog of deaths reported from Delta State from weeks 33 and 35-38 b12 rather than 6 discharges erroneously reported for Jigawa on 24th September was corrected for on 29th September (Nigeria Centre for Disease Control, 2020-b; Teyssou et al., 2021)
COVID-19 in Edo State
Edo State Government, confirmed the death of two more persons on the 17th of September 2021 who were not inoculated with the COVID-19 vaccines, raising the total number of mortalities recorded in the third wave of the pandemic to 59 (Emary et al., 2021). Head of the State COVID-19 Case Management, Dr. Ebomwonyi Osagie, disclosed this to journalists during the daily press briefing on COVID-19 in Benin City. He said the state, in the last 24 hours, also collected 461 samples and recorded 97 new cases and 20 more recoveries. “In the last 24 hours, Edo State collected a total of 461 samples across laboratories in Edo state, confirmed 97 new cases, with 20 recoveries from our various centres (Meyer, Sandfort & Bender, 2021).
“Total confirmed cases now stand at 1212, with 610 active cases in Edo State. Total discharged patients now stand at 121, with 59 moralities in the third wave. We lost two patients; both males were 61-year-old and 73-year-old and they were unvaccinated.” On his part, Permanent Secretary, Edo State Ministry of Health, Dr. Osamwonyi Irowa noted: “I encourage our people to embrace the vaccines and utilize its availability positively by ensuring that we get it administered to them for their safety. “We also call on all citizens of Edo State to disregard the negative statement about the vaccines on social media as the vaccines are safe and nobody who has taken the vaccine has died as a result of taking the vaccine” (Emary et al., 2021).
A Federal High Court in Port Harcourt, Rivers State, has restrained the Edo State Government and its Governor, Godwin Obaseki, from forcing residents of the state to take COVID-19 vaccine, according to a report by The Nations newspaper (Emary et al., 2021). Mr Obaseki had said recently in Benin that Edo residents would be required to show proof of COVID-19 vaccination before they would be allowed into public places like churches, mosques, and malls (Eyre, Taylor & Purver, 2021). The Nation reported that the court in a suit, dated August 30, 2021, ordered the governor, the Edo State Government, and three other respondents, “to maintain status quo pending the hearing and determination of the motion on notice, for the enforcement of the applicant’s fundamental human rights and for the leave of court to serve the respondents by publishing the court’s processes in a national daily newspaper circulating in Nigeria.” The suit was filed on behalf of the applicant, Charles Osaretin by Echezona Etiaba, a Senior Advocate of Nigeria, according to the report. The case, which has been adjourned to September 10 for hearing of the substantive motion, was heard by a vacation judge, Stephen Pam.
The Edo State Government said on Friday that it recorded four deaths and 28 new cases of COVID-19 within the last 24 hours from the third wave of the pandemic. The Head of COVID-19 response team in the state, Ebomwonyi Osagie, disclosed this during a press briefing on COVID-19 in Benin. Mr Osagie, a medical doctor, said the state has recorded a total of 28 new cases with four deaths and no recoveries within the last 24 hours from unvaccinated persons. “We have 34 persons in admission, 226 persons in home care and 99 persons have been discharged and 9,663 samples have been collected since the current outbreak of the third wave (Hagan, 2021). “As we speak to you today, we now have 18 people dead from the third wave while from the beginning of the outbreak we have over 200 people who died,” he said. Also speaking, the Permanent Secretary in the state ministry of Health, Osamwonyi Irowa, said efforts were being made to vaccinate teachers ahead of school resumption. Mr Irowa further said that there was a need for parents to also get vaccinated so that they don’t get infected with the virus transmitted through their children. Edo is the seventh most infected state in Nigeria, with 5,525 confirmed cases, according to data from the Nigeria Centre for Disease Control. The Edo State Governor, Godwin Obaseki, in order to curb the spread of the Delta Variant of COVID-19 in the state, introduced a controversial policy seeking to bar unvaccinated residents from having access to public places like church, mosque, and malls. The governor said he would go ahead to implement the policy, despite a restraining order from a Federal High Court, Port Harcourt (Teyssou et al., 2021).
COVID-19 Outbreak Preparedness in Nigeria
Prior to the importation of COVID-19 into Nigeria, the government established a “Coronavirus preparedness group” through its nation’s leading public health agency, the Nigeria Centre for Disease Control (NCDC), which commenced point of entry screening for travelers. Based on lessons learnt from the EVD outbreak, the NCDC strengthened the National Reference Laboratory with diagnostic capacity for epidemic-prone pathogens. Through this process, the NCDC supported 22 of the 32 states to establish emergency operation centres (EOC), and trained rapid response teams in all the 36 states (Ihekweazu, 2020). Furthermore, the agency provided relevant public health advisory to the Nigerians; shared the case-definition and preventive information with networks of national and subnational public health workers; built capacity for contact tracing and case management; and strengthened five laboratories for diagnostic capacities (Adepoju, 2020).
Also vital to the COVID-19 outbreak preparedness is the country’s Polio infrastructure - a programme originally aimed at the eradication of poliomyelitis. The structure brings on board its technical expertise, logistical capacity, human resources, community network and disease surveillance experience. The EOCs coordinating the outbreak response in each state are modelled after the Polio EOC operating under six functional units, namely: point of entry, epidemiology and surveillance, risk communication, management and communication, case management, and laboratory services (World Health Organization, 2020 – e). The Polio infrastructure was vital to the success of the 2014 EVD outbreak response (Hagan, 2021). Currently, it provides technical support to government agencies including NCDC (Global Polio Eradication Initiative, 2020) and has an on-ground network of human resources including traditional and religious leaders, community mobilizers and health workers to support the COVID-19 response. In addition, the Polio infrastructure had SMS-based application, auto-visual AFP detection and reporting (AVADAR) that support disease surveillance through networks of community volunteers and healthcare workers. This app has been useful for the current pandemic as COVID-19 surveillance questions have been added to this app (World Health Organization, 2020 – e).
On the 7th of October 2021, 290 new confirmed cases and 2 deaths were recorded in Nigeria. Till date, 207210 cases have been confirmed, 194796 cases have been discharged and 2742 deaths have been recorded in 36 states and the Federal Capital Territory. The 290 new cases are reported from 15 states- FCT (127), Lagos (45), Kaduna (28), Delta (18), Kwara (17), Plateau (13), Zamfara (10), Rivers (8), Imo (21), Ekiti (5), Nasarawa (4), Edo (3), Ondo (3), Akwa Ibom (2) and Oyo (1). A multi-sectoral national emergency operations centre (EOC), activated at Level 2, continues to coordinate the national response activities (Teyssou et al., 2021).
At the federal level and in most states, evidence-based policies such as social distancing and “test and trace” approaches have been implemented. However, implementation has happened on a base of weak health systems, sluggish emergency response, weak accountability systems, and fragmented data and information monitoring systems. These weaknesses have led to implementation gaps. The federal government and the Central Bank of Nigeria have initiated programs to mitigate economic shocks. But, the financial packages rolled out will mostly provide relief to workers only in the formal sector. Similarly, social welfare schemes—such as food assistance and cash transfers—have been inadequate and inefficient. The combined effects of COVID-19 and low oil prices have put Nigeria in a precarious financial situation. Given the low oil prices, the brakes put on economic activity due to the lockdown, and a weak global macroeconomic situation, the economic condition in the country could worsen and Nigeria will almost certainly require more efficient, equitable, and accountable use of domestic resources. There is also a potential scope for more international support than currently envisioned (Glatman-Freedman et al., 2021).
Challenges and Impact of the COVID-19 Outbreak on the Health Care System
With an Epidemic Preparedness Index of 38.9% (Africa’s Pulse, 2020), Nigeria has been rated better than many African countries to respond to the COVID-19 outbreak (Donnelly, 2020). However, its capacity to adequately respond in the face of local and community transmission has been said to be questionable (Ebenso & Out, 2020). As of 10 April 2020, over 9,000 contacts have been traced (Nigerian Newspapers, 2020), which is an average of 3.5 contacts per confirmed case. About 118,000 house-holds were visited for active case searches within 2 days in Lagos, among which 119 confirmed cases were identified (Sahara Reporters, 2020). The continued increase in the number of cases has overwhelmed the human resources for health involved in the various aspects of response activities, particularly contact tracing (Curran et al., 2021).
Many clinical activities have been reduced or halted in order to control COVID-19 transmission (Salako et al., 2020). More so, there have been numerous complaints about the shortages of personal protective equipment and ventilators needed to combat COVID-19 (World Economic Forum, 2020). This is further compounded with reported COVID-19 infection among healthcare workers as a result of occupational exposures, a figure estimated as 113 (about 6% of confirmed COVID-19 cases) as of 1 May 2020 (Abu-bashal, 2020).
The COVID-19 outbreak is also coming at a time when the country is currently battling with Lassa fever outbreak and preparing for certification exercise to be declared polio-free (Adepoju, 2020). As of the Epidemiological week 16 of the year 2020, the country has recorded 979 confirmed cases and 188 deaths (CFR 19.2%), against 546 confirmed cases and 123 deaths (CFR 22.5%) in the corresponding epidemiological week of 2019 (Nigeria Centre for Disease Control, 2020-c). Having being free of wild polio virus cases for a period of three years, the Independent Africa regional Certification is expected to make a decision in July 2020 to certify Nigeria polio-free (World Health Organization, 2020 – e). Response activities to this outbreak have a tendency to divert the limited resources away from current health issues and gains previously made on other health indices. The fear of being infected by COVID-19 at health facilities and the current lockdown order is also likely to limit access to health services routinely provided by CHWs. These include routine immunization, ante-natal services, maternal, neonatal and child health services, family planning, HIV/TB, management of minor ailments, disease surveillance and health management information system. Disruption of these health services could lead to reduction in immunization coverage, and increases in morbidity and mortality of infectious diseases as well as maternal, neonatal and childhood health issues (McAlister et al., 2021).
WHO Preparedness and Response
•WHO has developed interim guidance for laboratory diagnosis, advice on the use of masks during home care and in health care settings in the context of the novel coronavirus (2019-nCoV) outbreak, clinical management, infection prevention and control in health care settings, home care for patients with suspected novel coronavirus, risk communication and community engagement and Global Surveillance for human infection with novel coronavirus (2019-nCoV).
•WHO is working closely with International Air Transport Association (IATA) and have jointly developed a guidance document to provide advice to cabin crew and airport workers, based on country queries.
•WHO has been in regular and direct contact with Member States where cases have been reported. WHO is also informing other countries about the situation and providing support as requested.
•WHO is working with its networks of researchers and other experts to coordinate global work on surveillance, epidemiology, mathematical modelling, diagnostics and virology, clinical care and treatment, infection prevention and control, and risk communication. WHO has issued interim guidance for countries, which are updated regularly.
•WHO has prepared a disease commodity package that includes an essential list of biomedical equipment, medicines and supplies necessary to care for patients with 2019-nCoV.
•WHO has provided recommendations to reduce risk of transmission from animals to humans.
•WHO has published an updated advice for international traffic in relation to the outbreak of the novel coronavirus 2019-nCoV (Hagan, 2021).
•WHO has activated the R&D blueprint to accelerate diagnostics, vaccines, and therapeutics (Emary et al., 2021).
•OpenWHO is an interactive, web-based, knowledge-transfer platform offering online courses to improve the response to health emergencies. COVID-19 courses can be found here (OpenWHO) and courses in additional national languages. Specifically, WHO has developed online courses on the following topics:
oA general introduction to emerging respiratory viruses, including novel coronaviruses (available in Arabic, Chinese, English, French, Russian, Spanish, Hindi, Indian Sign Language, Persian, Portuguese, Serbian and Turkish);
oClinical care for Severe Acute Respiratory Infections (available in English, French, Russian, Indonesian and Vietnamese) (Hagan, 2021);
oHealth and safety briefing for respiratory diseases - ePROTECT (available in Chinese, English, French, Russian, Spanish, Indonesian and Portuguese);
oInfection Prevention and Control for Novel Coronavirus (COVID-19) (available in Chinese, English, French, Russian, Spanish, Indonesian, Italian, Japanese, Portuguese and Serbian); and oCOVID-19 Operational Planning Guidelines and COVID-19 Partners Platform to support country preparedness and response (available in English and coming soon in additional languages).
•WHO is providing guidance on early investigations, which are critical in an outbreak of a new virus. The data collected from the protocols can be used to refine recommendations for surveillance and case definitions, to characterize the key epidemiological transmission features of COVID-19, help understand spread, severity, spectrum of disease, impact on the community and to inform operational models for implementation of countermeasures such as case isolation, contact tracing and isolation (Pascall et al., 2021). Several protocols are available. One such protocol is for the investigation of early COVID-19 cases and contacts (the “First Few X (FFX) Cases and contact investigation protocol for 2019-novel coronavirus (2019-nCoV) infection”). The protocol is designed to gain an early understanding of the key clinical, epidemiological and virological characteristics of the first cases of COVID-19 infection detected in any individual country, to inform the development and updating of public health guidance to manage cases and reduce the potential spread and impact of infection (Curran et al., 2021).
Vaccines
To combat the widespread and provide immunity against the covid-19 infection, the COVID-19 vaccine was discovered after the phase 3 trial where the vaccine showed an effectiveness of about 95% in preventing covid-19 infection (Shrotri & Swinnen, 2021). According to WHO, five vaccines has been granted for emergency use and they include (Emary et al., 2021);
- Astrazeneca/Oxford originating from the United Kingdom/Sweden of which two does are to be administered with an interval of 4-12 weeks and storage temperature of 2-8 degree Celsius
- Pfizer-Biontech originating from Germany /United state of which 2 doses are to be administered within an interval of 3-4 weeks and storage temperature of –70 +-10 degree Celsius
- Johnson & Johnson originating from United states/Netherlands of which a single dose is administered with a storage temperature of 2-80C.
- Moderna originating from the United states with 2 doses for administration within an interval of 4 weeks and storage temperature of -20±50C.
- Sinopharm (BBIBP-CorV) originating from China with 2 doses for administration within a space of 3-4 weeks and storage temperature of 2-80C (WHO, 2021).
As same with every other vaccine the covid-19 vaccine on administration probes the body to start developing immunity against the virus that result in the infection of covid-19 (Meyer et al., 2021). The body develops full protection against the virus approximately two weeks after complete vaccination (National Centre For Immunization and Respiratory Disease (NCIRD), 2021).
In the WHO strategic response plan for covid19 virus in Africa as earlier stated, two of the responses include;
i.Setting innovative and research priorities by speeding up support through a clear and transparent process to fast track and proportionally increase research, development and availability of vaccines and diagnostics (Emary et al., 2021).
ii.Accelerate the development of therapeutic, diagnostics and vaccines and also fast tracking the extent of transmission and infection (Curran et al., 2021).
In accordance with this, the WHO has been at the core point of covid-19 vaccine roll out in Africa ensuring proper coordination & providing ample guidelines and practical guidance (WHO, 2020a). The Covid-19 vaccine administration has been one of Africa largest vaccination force with a vaccine slow rollout. According to WHO as of May 2021 over 22 million doses has been given on the continent and as of June 3 2021, 48,695,090 million vaccine dose has been received in 50 countries in Africa (WHO, 2021).
Update on SARS-CoV-2 Variants of Interest and Variants of Concern
WHO, in collaboration with national authorities, institutions and researchers, routinely assesses if variants of SARS-CoV-2 alter transmission or disease characteristics, or impact effectiveness of vaccines, therapeutics, diagnostics or public health and social measures (PHSM) applied by national authorities to control disease spread (Curran et al., 2021). “Signals” of potential Variants of Concern (VOCs) or Variants of Interest (VOIs) are detected and assessed based on the risk posed to global public health. National authorities may choose to designate other variants of local interest/concern and are encouraged to investigate and report on impacts of these variants (Kumar, Asghar & Raza, 2021).
Given the continuous need to understand the epidemiological and clinical impacts of VOCs and VOIs, WHO regularly monitors and reviews circulation of variants. The changes in the rise of new variants are being monitored in light of other co-circulating variants, such as Delta. This may mean that Variants of Interest (VOIs) or Variants of Concern (VOCs) may be outcompeted by newly emerging variants, such as VOC Delta. As evidence becomes available, we will revise classifications accordingly. These revisions reflect the continuous evolution of circulating variants and their changing epidemiology (Teyssou et al., 2021).
A recent peer-reviewed study evaluating persons infected with the Delta variant in France measured and compared the relative viral load with three other SARS-CoV-2 variants: Alpha, Beta and the non-VOC (20A.EU2) SARS-CoV-2 variant, collected from four hospital laboratories in the Paris area (Kumar et al., 2021). A total of 738 real time polymerase chain reaction (RT-PCR) SARS-CoV-2 positive nasopharyngeal samples collected from newly diagnosed COVID-19 cases, were screened to determine SARS-CoV-2 viral lineages and measure viral load (Teyssou et al., 2021). The results showed significant differences in the relative viral loads between Delta and other variants: viral loads of 2.5-fold higher were observed compared to Beta (median 7.26 [6.10–8.37]) (p less than 0.05) and to the non-VOC variant; while infections with Alpha and Delta variants had similar viral loads. A cross-sectional study (not yet peer reviewed), focusing on demographic characteristics, including severity of the illness and mortality rate, was conducted in India among COVID-19 cases caused by the non-VOC (B.1) variant and the Delta variant (B.1.617.2) (Pascall et al., 2021). Using viral genomic sequences from 9500 COVID-19 patients, the study found an increased number of infections among younger age groups (0-19 years) and women, a lower mean age for infection and symptomatic illness/hospitalization, higher mortality, and more frequent incidences of post-vaccination infections with Delta variant compared to the non-VOC (B.1) variant (Teyssou et al., 2021).
A retrospective cohort study conducted in the United States of America between 1 December 2020 and 30 July 2021 used sentinel surveillance to estimate the risk of hospitalization following infection with VOC or VOI, adjusting for age, sex, and vaccination status. Of the 27 814 cases identified, 23 170 (83.3%) samples were sequenced through sentinel surveillance, of which 726 (3.1%) were hospitalized due to COVID-19 (Paredes, Lunn & Famulare, 2021). A higher hospitalization risk was found for infections with Gamma (HR 3.17, 95% CI 2.15-4.67), Beta (HR: 2.97, 95% CI 1.65–5.35), Delta (HR: 2.30, 95% CI 1.69-3.15), and Alpha (HR 1.59, 95% CI 1.26–1.99) compared to infections with a non-VOC variant (Kumar et al., 2021). Following infection with a VOC, unvaccinated patients showed a higher hospitalization risk when compared to patients with non-VOC infections. Additionally, vaccinated patients showed an overall lower risk of hospitalization when compared to unvaccinated patients although there was no increased risk in these groups when comparing VOC and non-VOC infections (Teyssou et al., 2021).
| WHO label | Alpha | Beta | Gamma | Delta |
| Transmissibility | Increased transmissibility | Increased transmissibility | Increased transmissibility | Increased transmissibility and secondary attack rate |
| Disease severity | Increased risk of hospitalization9, possible increased risk of severity and mortality | Not confirmed, possible increased risk of in-hospital mortality | possible increased risk of hospitalization, risk of severity | Increased risk of hospitalization
|
| Risk of reinfection | Neutralizing activity retained, risk of reinfection remains similar | Reduction in neutralizing activity reported; T cell response elicited by D614G virus remains effective | Moderate reduction in neutralizing activity reported | Reduction in neutralizing activity reported |
| Impacts on diagnostics | Limited impact – S gene target failure (SGTF); no impact on overall result from multiple target RT-PCR, No impact on Ag RDTs observed | No impact on RT-PCR or Ag RDTs observed | None reported to date | None reported to date
|
Table 3: Summary of phenotypic impacts* of Variants of Concern
*Generalized findings as compared to previously/co-circulating variants. Based on emerging evidence, including non-peer-reviewed preprint articles and reports, all subject to ongoing investigation and revision. (Kumar et al., 2021; Teyssou et al., 2021)
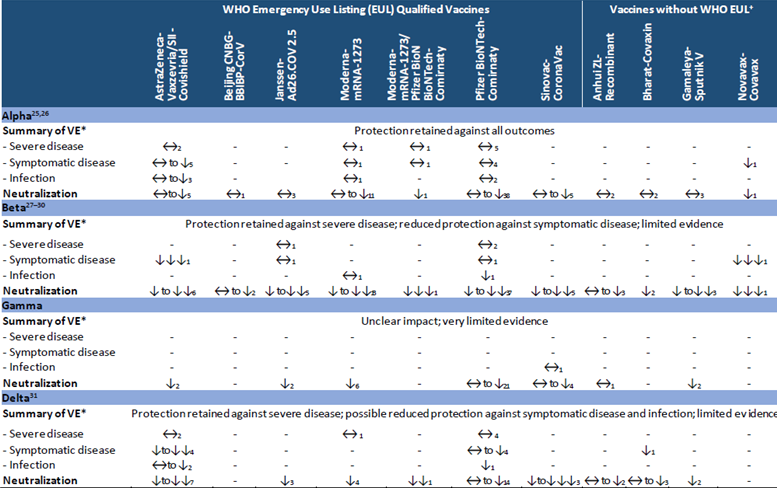
Table 4: Summary of vaccine performance against Variants of Concern
VE refers to vaccine effectiveness and vaccine efficacy
+As of submission of this update
*Summary of VE: indicates the general conclusions but only for the vaccines evaluated against the specific variant. Arrows generalize the magnitude of reduction in VE or neutralization: “↔” <10% reduction in VE, or VE>90% with no comparator, or that there was a <2-fold reduction in neutralization; “↓” 10 to <20% reduction in VE, or 2 to<5-fold reduction in neutralization; “↓↓” 20 to <30% reduction in VE, or 5 to <10-fold reduction in neutralization; “↓↓↓” ⋝30% reduction in VE, or ⋝10-fold reduction in neutralization. When more than one neutralization study is available, the interquartile range (25th and 75th percentiles) of fold-reductions across all studies for specific vaccine/variant was used.
“Moderna-mRNA-1273/Pfizer BioNTech-Comirnaty” indicates that both vaccines were evaluated together in study.
The number of studies is shown as subscripts: vaccine effectiveness and neutralization studies informing this table can be found on the VIEW-hub Resources page (https://view-hub.org/resources). For individual vaccine effectiveness studies, see ‘COVID-19 Vaccine Effectiveness Results Summary’, reference numbers noted with a ‘#’. For a list of all neutralization studies, see ‘COVID-19 Vaccine Neutralization Studies Table’.
(Kumar et al., 2021; Muik, Wallisch & Sänger, 2021)
WHO Regional Overviews
African Region
The African Region reported over 49 000 new cases and just under 1900 new deaths, decreases of 43% and 25% respectively as compared to the previous week. The declining trend in cases reported in the region and observed since early July continued this week. While this trend is true for most countries in the region, in the past week, seven countries reported increases of over 20% in new cases as compared to the previous week.
The highest numbers of new cases were reported from South Africa (9637 new cases; 16.2 new cases per 100 000 population; a 38?crease), Ethiopia (7127 new cases; 6.2 new cases per 100 000; a 19?crease), and Lesotho* (6943 new cases; 324.1 new cases per 100 000). The highest numbers of new deaths were reported from South Africa (752 new deaths; 1.3 new deaths per 100 000 population; a 15?crease), Ethiopia (306 new deaths; <1 new death per 100 000; a 20% increase), and Lesotho* (231 new deaths; 10.8 new deaths per 100 000).
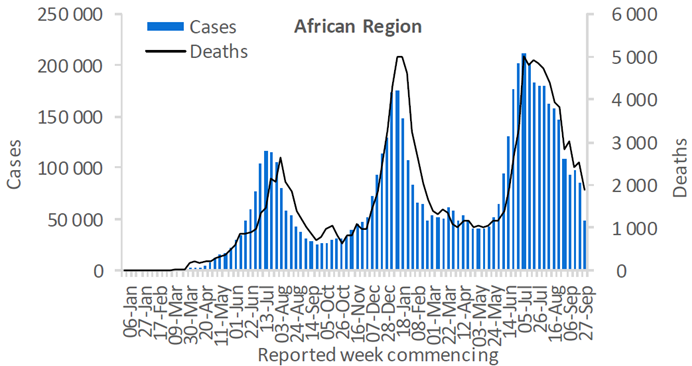
Figure 1: Updates from the African Region
* This marked increase was reported by Lesotho on 30 September 2021 as a batch number for both cases and deaths and will be reviewed as more information becomes available.
(Mwai, 2021; Nyenswah, 2021)
Conclusion
The COVID-19 pandemic hit the world massively, not sparing the Africa continent, Nigeria and Edo State. The paper carefully evaluated the roles of the World Health Organization played in Africa to help combat the COVID-19 pandemic and how effective these roles were.
In conclusion, the World Health Organization in collaboration with other specialized agencies (e.g NCDC) has played and are still playing effective roles in controlling the spread of COVID-19 in Africa from valuable sensitization to assistance of member states. The roles played have gone a long way in reducing the number of daily recorded cases across the continent as well as mortality rates from the pandemic.
An article by Tolbert G. Nyenswah says that although Africa has about 16% of the world population only about 2% of the vaccine has been supplied to the continent. Problems of slow rollout of vaccine leading to the destruction of expired vaccine in some countries, misinformation regarding the vaccine as well as perceived side effects resulting in hesitancy of the masses to take these vaccines are major problems faced in Africa today.
References
- Abu-bashal, Dam (2020). Nigeria: 113 healthcare workers infected with COVID-19 [Internet]. 2020 [cited 2020 May 5].
View at Publisher | View at Google Scholar - Adepoju, P. (2020). Nigeria responds to COVID-19; First Case Detected in sub-Saharan Africa. Nat Med. 26(4):444–448.
View at Publisher | View at Google Scholar - Africa’s Pulse (2020). Assessing the Economic Impact of COVID-19 and Policy Responses in Sub-Saharan Africa [Internet]. Washington, USA: The World Bank, 1818 H Street NW,; 2020 Apr [cited 2020 Apr 25] p. 136. Report No.: Vol 21.
View at Publisher | View at Google Scholar - Bitar, D., Goubar, A. & Desenclos, J.C. (2009). International travels and fever screening during epidemics: a literature review on the effectiveness and potential use of non-contact infrared thermometers. Euro Surveill. 14:1–5.
View at Publisher | View at Google Scholar - Bwire, G.M. & Paulo, L.S. (2020). Coronavirus disease-2019: is fever an adequate screening for the returning travelers? Trop Med Health, 48(3): 14-19.
View at Publisher | View at Google Scholar - Chen, N., Zhou, M., Dong, X., Qu, J., Gong, F. & Han, Y. (2020). Epidemiological and clinical characteristics of 99 cases of 2019 novel coronavirus pneumonia in Wuhan, China: a descriptive study. Lancet. 395(10223):507–513.
View at Publisher | View at Google Scholar - Curran, J., Dol, J. & Boulos, L. (2021). Transmission characteristics of SARS-CoV-2 variants of concern Rapid Scoping Review. medRxiv. Published online January 1, 2021:2021.04.23.21255515.
View at Publisher | View at Google Scholar - Donnelly, E. (2020). Nigeria’s Political Leaders Need to Win Trust to Tackle COVID-19 [Internet]. Chatham House. 2020 [cited 2020 Apr 25].
View at Publisher | View at Google Scholar - Ebenso, B. & Out, A. (2020). Can Nigeria contain the COVID-19 outbreak using lessons from recent epidemics? Lancet Glob Health [Internet]. 2020 Mar 11 [cited 2020 Apr 24];0(0).
View at Publisher | View at Google Scholar - Emary, K.R.W., Golubchik, T. & Aley, P.K. (2021). Efficacy of ChAdOx1 nCoV-19 (AZD1222) vaccine against SARS-CoV-2 variant of concern 202012/01 (B.1.1.7): an exploratory analysis of a randomised controlled trial. The Lancet. 397(10282):1351-1362.
View at Publisher | View at Google Scholar - Eyre, D.W., Taylor, D. & Purver, M. (2021). The Impact of SARS-CoV-2 Vaccination on Alpha & Delta Variant Transmission.; 2021.09.28.21264260.
View at Publisher | View at Google Scholar - Federal Ministry of Health, Nigeria (2019). National Strategic Health Development Plan II 2018 - 2022 [Internet]. [cited 2020 Apr 25].
View at Publisher | View at Google Scholar - Glatman-Freedman, A., Bromberg, M., Dichtiar, R., Hershkovitz, Y. & Keinan-Boker, L. (2021). The BNT162b2 vaccine effectiveness against new COVID-19 cases and complications of breakthrough cases: A nation-wide retrospective longitudinal multiple cohort analysis using individualised data. EBioMedicine. 2021;72.
View at Publisher | View at Google Scholar - Global Polio Eradication Initiative (2020). Polio eradication staff support COVID-19 response [Internet]. 2020 [cited 2020 May 8].
View at Publisher | View at Google Scholar - Gostic, K.M., Gomez, A.C.R., Mummah, R.O., Kucharski, A.J. & Lloyd-Smith, J.O. (2020). Estimated effectiveness of symptom and risk screening to prevent the spread of COVID-19. Elife. 9:1–18.
View at Publisher | View at Google Scholar - Guan, W., Ni, Z., Hu, Y., Liang, W., Ou, C. et al. (2020). Clinical Characteristics of Coronavirus Disease 2019 in China. N Engl J Med. 20:2-10.
View at Publisher | View at Google Scholar - Hagan, L.M. (2021). Outbreak of SARS-CoV-2 B.1.617.2 (Delta) Variant Infections Among Incarcerated Persons in a Federal Prison — Texas, July–August 2021. MMWR Morb Mortal Wkly Rep.
View at Publisher | View at Google Scholar - Ihekweazu, C. (2020). Steps Nigeria is taking to prepare for cases of coronavirus [Internet]. The Conversation. 2020 [cited 2020 May 8].
View at Publisher | View at Google Scholar - Klompas, M., Morris, C.A., Sinclair, J.P., Aearson, M. & Shenoy, E.S. (2020). Universal masking in hospitals in the Covid-19 era. N Engl J Med. 2:20-34.
View at Publisher | View at Google Scholar - Kumar, A., Asghar, A. & Raza, K. (2021). Demographic characteristics of SARS-CoV-2 B.1.617.2 (Delta) variant infections in Indian population. medRxiv.
View at Publisher | View at Google Scholar - Li, Q., Guan, X., Wu, P., Wang, X., Zhou, L. et al. (2020). Early transmission dynamics in Wuhan, China, of novel Coronavirus infected pneumonia. N Engl J Med. 382(13):1199–1207.
View at Publisher | View at Google Scholar - Mailman School of Public Health (2017). Columbia University, New York, USA., S F, B H, Women4Health Programme, Kano, Nigeria. Cost-Effectiveness of Alternative Models of Community Health Workers for Promotion of Maternal, Newborn and Child Health in Northern Nigeria. Int J Transl Community Med. 12;85–97.
View at Publisher | View at Google Scholar - McAlister, F.A., Nabipoor, M., Chu, A., Lee, D.S., Saxinger, L. et al. (2021). Lessons from the COVID-19 Third Wave in Canada: The Impact of Variants of Concern and Shifting Demographics. Infectious Diseases (except HIV/AIDS); 2021.
View at Publisher | View at Google Scholar - Meyer, E.D., Sandfort, M. & Bender, J. (2021). Two Doses of the MRNA BNT162b2 Vaccine Reduce Severe Outcomes, Viral Load and Secondary Attack Rate: Evidence from a SARS-CoV-2 Alpha Outbreak in a Nursing Home in Germany, January-March 2021.; 2021:2021.09.13.21262519.
View at Publisher | View at Google Scholar - Moeti, Dr Matshidiso. (2020, April 3).
View at Publisher | View at Google Scholar - Muik, A., Wallisch, A.K. & Sänger, B. (2021). Neutralization of SARS-CoV-2 lineage B.1.1.7 pseudovirus by BNT162b2 vaccine–elicited human sera. Science. Published online 2021:eabg6105.
View at Publisher | View at Google Scholar - Mwai, P. (2021). Covid 19 Africa;what is happening with vaccines? Reality Check, 6-10.
View at Publisher | View at Google Scholar - Nahtulya, Kaneza & Mavhinga, Dewa (2020).
View at Publisher | View at Google Scholar - National Centre For Immunization and Respiratory Disease (NCIRD). (2021, May 27).
View at Publisher | View at Google Scholar - Nigeria Centre for Disease Control (2020-a). First Case of Corona virus Disease Confirmed in Nigeria [Internet]. 2020 [cited 2020 Apr 1].
View at Publisher | View at Google Scholar - Nigeria Centre for Disease Control (2020-b). COVID-19 Outbreak In Nigeria Situation Report S/N 54. Abuja; 2020. [Internet]. 2020 [cited 2020 Apr 23]. Available from:
View at Publisher | View at Google Scholar - Nigeria Centre for Disease Control (2020-c). Nigeria Centre for Disease Control Weekly Epidemiological Report, Week 16 [Internet]. 2020
View at Publisher | View at Google Scholar - Nigeria Coronavirus (2020). 198,883 cases and 4,035 deaths– Worldo-meter [Internet]. Delaware: Worldometers.info.
View at Publisher | View at Google Scholar - Nigerian Newspapers (2020). COVID-19: We have traced 8,932 people of interest – Task Force. Latest Nigeria News, Nigerian Newspapers, Politics [Internet]. 2020 Apr 10 [cited 2020 Apr 25];
View at Publisher | View at Google Scholar - Nyenswah, T. G. (2021, May 14). Africa covid 19 vaccination woes present a pandemic paradox. Vaccine Hesitancy, pp. 17-25.
View at Publisher | View at Google Scholar - OECD. (2020).
View at Publisher | View at Google Scholar - Offiong, Adie Vannessa. (2020).
View at Publisher | View at Google Scholar - Okoli, Obasesan & Bwawa, Tantenda (2020).
View at Publisher | View at Google Scholar - Ozili, P. (2020).
View at Publisher | View at Google Scholar - Paredes, M.I., Lunn, S.M. & Famulare, M. (2021). Associations between SARS-CoV-2 variants and risk of COVID-19 hospitalization among confirmed cases in Washington State: a retrospective cohort study. medRxiv.
View at Publisher | View at Google Scholar - Pascall, D.J., Mollett, G., Blacow, R. & Bulteel, N. (2021). The SARS-CoV-2 Alpha variant causes increased clinical severity of disease.
View at Publisher | View at Google Scholar - Perry, H.B., Dhillon, R.S., Liu, A., Chitnis, K., Panjabi, R., et al. (2016). Community health worker programmes after the 2013–2016 Ebola outbreak. Bull World Health Organ. 94(7):551–553.
View at Publisher | View at Google Scholar - Sahara Reporters, (2020). After Visiting 118,000 Households, We Identified 119 Persons With COVID-19 Symptoms –Lagos Government [Internet]. [cited 2020 Apr 25]. Available from:
View at Publisher | View at Google Scholar - Salako, O., Okunade, K., Allsop, M., Habeebu, M., Toye, M., et al. (2020). Upheaval in cancer care during the COVID-19 outbreak. ecancermedicalscience [Internet]. 2020 Apr 1
View at Publisher | View at Google Scholar - Sherrad-Smith, H.H., Watson, W., Winskill, A., Audu, U., Maikore, O., et al. (2020).
View at Publisher | View at Google Scholar - Shrotri, P. & Swinnen, K. (2021). An interactive website tracking covid 19 vaccine development. Lancet glob health, e590-e592.
View at Publisher | View at Google Scholar - Singhal, T. (2020). A review of Coronavirus disease-2019 (COVID-19). Indian J Pediatr. 87(4):281–286.
View at Publisher | View at Google Scholar - Tay, M.R., Low, Y.L., Zhao, X., Cook, A.R. & Lee, V.J. (2015). Comparison of infrared thermal detection systems for mass fever screening in a tropical healthcare setting. Public Health, 129(11): 1471-1478.
View at Publisher | View at Google Scholar - Teyssou, E., Delagrèverie, H. & Visseaux, B. (2021). The Delta SARS-CoV-2 variant has a higher viral load than the Beta and the historical variants in nasopharyngeal samples from newly diagnosed COVID-19 patients. J Infect. 83(4):e1-e3.
View at Publisher | View at Google Scholar - Watch, Human Right. (2020, June 8).
View at Publisher | View at Google Scholar - World Economic Forum (2020). COVID-19 in Africa: insights from our 23 April WHO media briefing [Internet]. World Economic Forum. 2020 [cited 2020 Apr 25].
View at Publisher | View at Google Scholar - World Health Organization (2020 – e). Nigeria’s polio infrastructure bolster COVID-19 response [Internet]. WHO | Regional Office for Africa. 2020 [cited 2020 May 8].
View at Publisher | View at Google Scholar - World Health Organization (W.H.O). (2020 a).
View at Publisher | View at Google Scholar - World Health Organization (W.H.O). (2020 c).
View at Publisher | View at Google Scholar - World Health Organization Africa (W.H.O). (2021, Semptember).
View at Publisher | View at Google Scholar - World Health Organization. (2020-f). WHO Timeline - COVID-19.
View at Publisher | View at Google Scholar - Worldometer. (2020). Total Coronavirus Cases in the World.
View at Publisher | View at Google Scholar - Wu, C., Chen, X. & Cai, Y. (2020). Risk factors associated with acute respiratory distress syndrome and death in patients with coronavirus disease 2019 pneumonia in Wuhan, China. JAMA Intern Med. 2: 199-207.
View at Publisher | View at Google Scholar - Yadav, Manish Kumar. (2017).
View at Publisher | View at Google Scholar - Zhu, N., Zhang, D., Wang, W., Li, X., Yang, B., et al. (2020). A Novel Coronavirus from Patients with Pneumonia in China, 2019. N. Engl. J. Med. 382 (8), 727−733.
View at Publisher | View at Google Scholar
