

Research Article | DOI: https://doi.org/10.31579/2834-5118/65
A Patient from Brazil with Severe Cerebral Palsy and Refractory Epilepsy: Expert opinion and the recommended Evidence-Based Multimodal Therapy
Advisor in Pediatrics and Pediatric Psychiatry, The National Training and Development Center and Baghdad Medical City.
*Corresponding Author: Aamir Jalal Al-Mosawi, Advisor in Pediatrics and Pediatric Psychiatry, The National Training and Development Center and Baghdad Medical City.
Citation: Aamir Jalal Al-Mosawi, (2025), A Patient from Brazil with Severe Cerebral Palsy and Refractory Epilepsy: Expert opinion and the recommended Evidence-Based Multimodal Therapy, International Journal of Clinical Surgery, 4(6); DOI:10.31579/2834-5118/65.
Copyright: © 2025, Aamir Jalal Al-Mosawi. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 04 November 2025 | Accepted: 18 November 2025 | Published: 27 November 2025
Keywords: cerebral palsy; refractory epilepsy; citicoline; cerebra lysin; baclofen; evidence-based medicine
Abstract
Background: Severe cerebral palsy with refractory epilepsy and cortical visual impairment is associated with profound disability. Families often pursue unproven interventions, underscoring the need for evidence-based medicine in clinical practice.
Patients and methods: A 3-year-old Brazilian girl with hypoxic-ischemic encephalopathy leading to spastic quadriplegic cerebral palsy, uncontrolled epilepsy, cortical visual impairment, and feeding difficulties requiring gastrostomy is described.
Despite multiple prior therapies including cannabidiol, stem cells, exosomes, ketogenic diet, and integrative interventions, the girl remained severely impaired. Brain MRI revealed encephalomalacia and gliosis in the left parietal and occipital lobes with ipsilateral ventricular dilatation. An evidence-based medicine-guided multimodal protocol (carbamazepine, clonazepam, baclofen, citicoline, Cerebro lysin, nutritional supplementation, and continuation of clobazam) was initiated.
Results: Within weeks, her mother reported improved alertness, smiling, vocalization, participation in physiotherapy, and feeding tolerance. Seizure burden was perceived as significantly reduced.
Conclusion: This case illustrates the value of evidence-based medicine in complex neurodevelopmental disorders, highlighting how rational pharmacological choices and avoidance of polypharmacy can yield meaningful functional gains and improved quality of life.
Introduction
Cerebral palsy is a leading cause of childhood disability worldwide, often complicated by epilepsy, spasticity, and cortical visual impairment. Severe cases pose therapeutic challenges, with families frequently pursuing experimental treatments despite limited or absent scientific support [1-13].
The practice of evidence-based medicine requires integration of [14]:
- Best available research evidence
- Clinical expertise
- Patient and caregiver values
Here, we describe a case of severe spastic quadriplegic Cerebral palsy with refractory epilepsy in a child who previously underwent multiple non-evidence-based interventions. Transition to a rational, evidence-based medicine-guided multimodal protocol resulted in measurable improvements in quality of life.
Patient and methods
A Brazilian, mother consulted us about the possible therapies for the treatment of her daughter. The girl was at about the age of three years. She was born on March 24, 2019 by normal delivery. At birth she experienced birth asphyxia and was considered to have cardiorespiratory (Apgar score = 0). Thereafter, she developed seizures. The girl was diagnosed in Brazil as having severe spastic quadriplegic cerebral palsy associated with uncontrolled epilepsy and cortical visual impairment, and required feeding through gastrostomy tube.
Neurological course:
- 5 months: Developed infantile spasms, which resolved after 3 months of ketogenic diet.
- Following years: Refractory epilepsy with multiple daily seizures despite 10 anti-seizure medications.
- Severe cerebral palsy: Spastic quadriplegia, cortical visual impairment, global developmental delay, and oral-motor dysfunction requiring gastrostomy.
Prior interventions: Physiotherapy, speech therapy, acupuncture, cannabidiol, REAC therapy, growth hormone, exosomes, photo bio-modulation, and one dose of mesenchymal stem cells. None yielded sustained benefit.
The girl has been receiving physiotherapy (Figure-1), speech therapy, and acupuncture since she was a baby and has also received cannabidiol, radio electric asymmetric conveyer, and 3 treatments with growth hormone.
Since April 2021, she received 9 ampoules of exosomes, and Tran-cranial Photo biomodulation was performed at home. In addition, she received mesenchymal stem cells taken from the pelvis once.

Figure-1A: The girl has been receiving physiotherapy

Figure-1B: The girl has been receiving physiotherapy
Developmental status (early 2022):
- Unable to sit unsupported, roll, or grasp objects
- Absent visual fixation and face recognition
- Minimal interaction or social response
- Recently initiated smiling and random vocalizations
- Oral feeding tolerated for pasty foods but liquids via gastrostomy
During February, 2022, she was unable to sit without support.
She was not pronouncing vowels just random vocalizations,
She was not recognizing faces, but she started to react to voices with her vocalizations.
She had almost no voluntary movements, when she was put on the floor she pedals like a baby; her head is turned to one side a lot.
Seizure status
The mother has already changed 5 neurologists. They have already tried 10 types of medication, combinations, and none of them controlled the seizures and on the contrary, she was doped up and full of side effects. The mother stopped all medication but continued only clobazam 15mg and the girl continued to experience several types of rapid seizures (2.3 seconds) a day. Her weigh was 16.5 kg (36.37 L) and her height 93 cm tall.
Neuroimaging: MRI (Figure-2) showed encephalomalacia and gliosis in the left parietal and occipital lobes with compensatory dilatation of the ipsilateral lateral ventricle. No cortical malformations or posterior fossa abnormalities.
Family perspective: The mother expressed frustration after years of empiric therapies and explicitly sought an evidence-based medicine-guided approach.
Intervention
An individualized evidence-Based multimodal therapies were recommended based on our extensive published evidence-based experiences with treatment of cerebral palsy and refractory epilepsy [1-13,15], and included:
- Carbamazepine (Tegretol): 100 mg/5 ml, 5 ml orally three times daily (antiepileptic).
- Clonazepam (Rivotril): 0.25 mg, twice daily.
- Clobazam: 15 mg daily, continued (antiepileptic).
- Baclofen (Lioresal): 5 mg, three times daily (antispasticity).
- Cerebrolysin: 2.5 ml intramuscularly, every other day for 15 doses (neurotrophic, cognitive support).
- Citicoline (Somazina): 3 ml orally daily (neuroprotective, cognitive support).
- Royal Plus softgel: twice daily (nutritional support).
- Discontinuation of unproven or experimental therapies.
Outcomes
The mother reported obvious improvements with significant reduction of seizure.
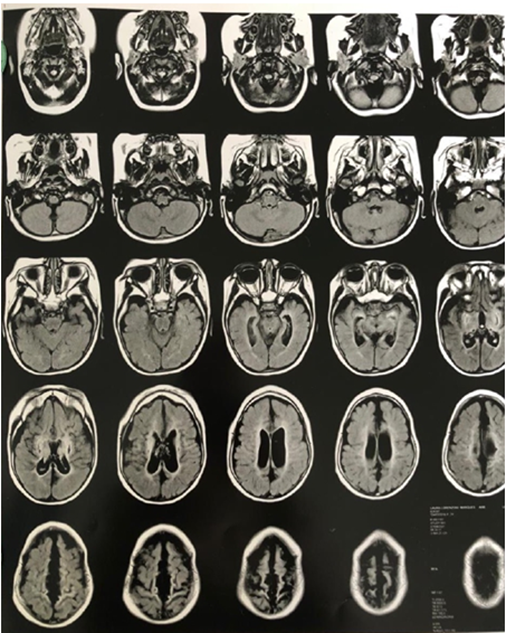
Figure-2A: MRI showed encephalomalacia and gliosis in the left parietal and occipital lobes

Figure-2B: MRI showed encephalomalacia and gliosis in the left parietal and occipital lobes

Figure-2C: MRI showed encephalomalacia and gliosis in the left parietal and occipital lobes
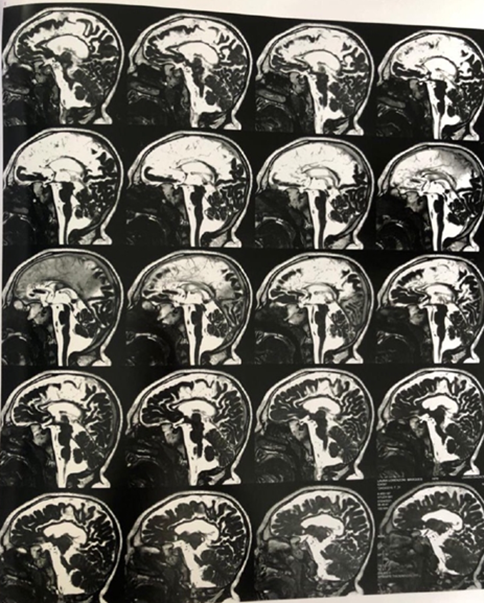
Figure-2D: MRI showed encephalomalacia and gliosis in the left parietal and occipital lobes
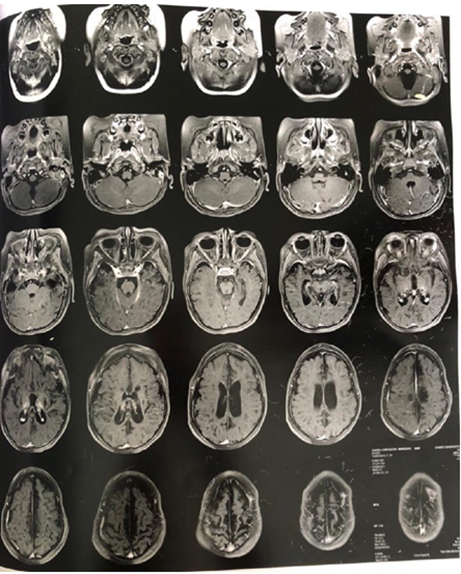
Figure-2E: MRI showed encephalomalacia and gliosis in the left parietal and occipital lobes
Discussion
This case highlights several evidence-based medicine principles:
1. Best available evidence:
- Antiseizure drugs (carbamazepine, clonazepam, clobazam): supported by epilepsy management guidelines for focal seizures and refractory epilepsy.
- Baclofen: established efficacy in spasticity reduction in cerebral palsy.
- Citicoline and cerebrolysin: evidence from clinical and experimental studies suggests neuroprotective and cognitive-enhancing effects in pediatric neurorehabilitation.
2. Avoidance of polypharmacy: Previous regimens involved multiple agents without rational selection. Streamlined evidence-based therapy reduces risks of sedation and drug interactions.
3. Family-centered care: Incorporating caregiver perspectives ensured adherence and satisfaction while discouraging unproven interventions.
4. Outcome focus: Even small functional and behavioral gains represent significant improvements in quality of life for children with severe cerebral palsy.
Cerebrolysin is a mixture of free amino acids (85%) and 15% biologically active low molecular weight amino acid sequences which include low molecular weight neuro-peptides (Brain-derived neurotrophic factor, glial cell line-derived neurotrophic factor, nerve growth factor, ciliary neurotrophic factor.
Cerebrolysin has been used safely with benefit in a variety of neuro-psychiatric disorders including idiopathic mental retardation, cerebral palsy, brain atrophy, myelomeningocele, pediatric juvenile spinal muscular atrophy, pediatric Charcot Marie Tooth disease, kernicterus, and agenesis of corpus callosum with colpocephaly [16-25].
Citicoline is a safe form of the choline has been increasingly grouped with the water-soluble B vitamins. It has been increasingly used with noticeable benefits in the treatment of several pediatric and neuro-psychiatric disorders including, cerebral palsy, cognitive impairment, autism disorders, Rett syndrome, and kernicterus [26, 27].
Conclusion
This case demonstrates that Evidence based medicine-guided multimodal therapy can yield meaningful benefits in children with severe cerebral palsy and refractory epilepsy. Rational drug selection, neurotrophic support, and family-centered decision-making contrast sharply with empiric experimental approaches, underscoring the clinical value of evidence-based practice.
Acknowledgement
The author would like to express his gratitude for the mother for kindly accepting publishing the photos of the patient. The author has the copy right of the figures in this paper.
Conflict of interest
None.
References
- Al-Mosawi AJ. (2019). New therapies for the treatment of spastic cerebral palsy. Medical Journal of Clinical Trials & Case Studies (ISSN: 2578-4838) Mar; 3(2): 1-9.
View at Publisher | View at Google Scholar - Al-Mosawi AJ. (2019). The pattern of cerebral palsy in Iraqi children. Med Life Clinics (ISSN: 2689-5943) Aug; 1(1):1-9.
View at Publisher | View at Google Scholar - Al-Mosawi AJ. (2020). New Therapies for the treatment of ataxic cerebral palsy caused by kernicterus. EC Clinical and Medical Case Reports Mar; 3(4): 26-31.
View at Publisher | View at Google Scholar - Al-Mosawi AJ. (2020). The experience with the use of nandrolone decanoate and pyritinol in children with cerebral palsy. Open Access Journal of Bio-generic Science and Research (ISSN: 2692-1081) Jul; 2(3):1-3.
View at Publisher | View at Google Scholar - Al-Mosawi AJ. (2020). Cerebral palsy: A unique illustrated experience. Medico Research Chronicles (ISSN: 2394-3971) Sept; 7 (4): 2017-2239.
View at Publisher | View at Google Scholar - Al-Mosawi AJ. (2021). The early treatment of a boy from Virginia with ataxic cerebral palsy. Journal of Pediatrics and Child Health May; 2 (4): 1-5.
View at Publisher | View at Google Scholar - Al-Mosawi AJ. (2021). Cerebral Palsy, Autistic Features Associated with Periventricular White Matter Hyperintensity on Brain Magnetic Resonance Imaging: A Diagnostic Challenge. Journal of Pediatrics and Child Health Issues, June; 2(5):1-4.
View at Publisher | View at Google Scholar - Al-Mosawi AJ. (2021). A Girl from Canada with Severe Cerebral Palsy Associated with Hydrocephalus and Mutation of Kinase D-Interacting Substrate of 220-KDa (KIDINS220) Gene: A New Syndrome with Unique Brain Imaging Findings and a Therapeutic Challenge. Journal of Clinical Research in Radiology (ISSN: 2639-913X) 2021; 4 (1):22-25.
View at Publisher | View at Google Scholar - Al-Mosawi AJ. (2021). Brain Imaging Abnormalities in Cerebral Palsy. Journal of Clinical Research in Radiology (ISSN: 2639-913X); 4 (1): 11-15.
View at Publisher | View at Google Scholar - Al-Mosawi AJ. (2022). A Girl from Qatar with Post-Infantile Acquired Cerebral Palsy Caused by Submersion Injury: A Rare Etiology and a Therapeutic Challenge. Clinical Research and Clinical Trials (ISSN: 2693-4779) Jan; 5 (1): 1-4.
View at Publisher | View at Google Scholar - Al-Mosawi AJ. (2022). An Indian boy with post-infantile acquired cerebral palsy caused by submersion injury: A rare etiology and a therapeutic challenge. Case Reports & Research Practices in MEDICINE (ISSN: 2771-4845) Mar; 2 (1): 41-44.
View at Publisher | View at Google Scholar - Al-Mosawi AJ. (2022). The initial treatment of a girl from Texas with post-infantile acquired cerebral palsy caused by submersion injury. Journal of Pediatrics and Neonatal Medicine (ISSN: 2694-5983) April (4): 1:1-4.
View at Publisher | View at Google Scholar - Al-Mosawi AJ. (2022). Cerebral Palsy and Autism Associated with Periventricular White Matter Hyperintensity on Brain Magnetic Resonance Imaging: A New Disorder and Its Treatment. Med Press Psychiatry and Behavioral Sciences Sept; 1(1):1-4 [mppbs–202209007].
View at Publisher | View at Google Scholar - Al-Mosawi AJ. (2006). The Practice of evidence-based medicine. The New Iraqi Journal of Medicine (ISSN: 1817-5562, 1998037X); 2(1):8-10.
View at Publisher | View at Google Scholar - Al-Mosawi AJ. (2022) Childhood Lennox-Gastaut syndrome, low set ears, unilateral cryptorchidism: A new variant. Journal of Clinical Images & Reports Mar; 1(1):1-6.
View at Publisher | View at Google Scholar - Al-Mosawi AJ. (2020) Clinical uses of Cerebrolysin in Pediatric Neuropsychiatry. Science World Journal of Pharmaceutical Sciences; 1(1): 1-4.
View at Publisher | View at Google Scholar - Al-Mosawi AJ. (2019) New medical therapies for the treatment of myelomeningocele. Surgical Medicine Open Access Journal (ISSN: 2578-0379); 2(4): 1-4.
View at Publisher | View at Google Scholar - Al-Mosawi AJ. (2018). A novel therapy for pediatric juvenile spinal muscular atrophy.1st ed., Saarbrücken; LAP Lambert Academic Publishing: (ISBN: 978-613-9-89719-3).
View at Publisher | View at Google Scholar - Al-Mosawi AJ. (2020). The use of cerebrolysin in pediatric Wohlfart Kugelberg Welander syndrome. MOJ Clinical & Medical Case Reports (e-ISSN: 2381-179X); 10(1):20-23.
View at Publisher | View at Google Scholar - Al-Mosawi AJ. (2018). A novel therapy for pediatric Charcot Marie Tooth disease. 1st ed., Saarbrücken; LAP Lambert Academic Publishing: (ISBN: 978-613-8-39043-5).
View at Publisher | View at Google Scholar - Al-Mosawi AJ. (2020). The use of Cerebrolysin in Pediatric Charcot Marie Tooth Disease. Journal Of Neurologi Cal Research and Therapy (ISSN: 2470-5020); 3(2):17-21.
View at Publisher | View at Google Scholar - Al-Mosawi AJ. (2018). A novel therapeutic approach for the neurological complications of kernicterus. 1st ed., Saarbrücken; LAP Lambert Academic Publishing: (ISBN: 978-613-9-98425-1).
View at Publisher | View at Google Scholar - Al-Mosawi AJ. (2019). The novel use of cerebrolysin and citicoline in the treatment of kernicterus. Online Journal of Neurology and Brain Disorders (ISSN: 2637-6628); 3 (1): 208-212.
View at Publisher | View at Google Scholar - Al-Mosawi AJ. (2019). Agenesis of corpus callosum with colpocephaly: A novel therapy. 1st ed., Saarbrücken; LAP Lambert Academic Publishing: (ISBN: 978-613-9-45076-3).
View at Publisher | View at Google Scholar - Al-Mosawi AJ. (2020). The use of piracetam and cerebrolysin in the treatment of agenesis of corpus callosum with colpocephaly. EC clinical and medical case reports; 3(1): 01-05.
View at Publisher | View at Google Scholar - Al-Mosawi AJ. (2019). Citicoline research progress. 1st ed., Saarbrücken; LAP Lambert Academic Publishing: (ISBN: 978-620-0-11372-6).
View at Publisher | View at Google Scholar - Al-Mosawi AJ. (2019). The Use of Citicoline in Pediatric Neurology and Pediatric Psychiatry. Austin Pediatrics; 6(1): 1071-1072.
View at Publisher | View at Google Scholar
