

Research Article | DOI: https://doi.org/10.31579/2834-8508/016
A Future Investigation on Clinicopathological Approaches of Neck Lymphadenopathy by Fine Needle Aspiration Cytology
1Department of Microbiology, Women University Mardan, Pakistan
2Department of Zoology, Abdul Wali Khan University, Mardan (23200), Pakistan
*Corresponding Author: Laila Aziz, Department of Microbiology, Women University Mardan, Pakistan
Citation: Laila Aziz, Arsalan Rasheed (2023), A Future Investigation on Clinicopathological Approaches of Neck Lymphadenopathy by Fine Needle Aspiration Cytology. Archives of Clinical and Experimental Pathology. 2(4); Doi:10.31579/2834-8508/016
Copyright: © 2023 Laila Aziz, This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 21 June 2023 | Accepted: 10 July 2023 | Published: 24 July 2023
Keywords: fine needle aspiration cytology, neck lymphadenopathy, tuberculous lymphadenitis, reactive lymphadenopathy.
Abstract
Background: Peripheral lymphoid glands located throughout the neck are cervical lymph nodes. Nodes are irregular in scale, quality or numbers and palpable are referred to by the name lymphadenopathy. Neck lymphadenopathy diagnosis can range beyond neoplasm to different types of disease. Exact identification of the origin of lymphadenopathy is capable of also be complicated and can direct to identification complications that origin inadequate care and associated health concerns. Neck lymphadenopathy is a typical clinical appearance in many clinical procedures.
Materials and Methods: In order to illustrate the function of fine needle aspiration cytology in etiological workup in neck lymphadenopathy, this research was done to explain the connexion between clinical presentations of Fine Needle Aspiration Cytology. A prospective observational investigation was carried out over a period of one and half years on 80 patients of cervical lymphadenopathy who presented in the surgical outpatient department of Madras Medical College. Detailed history, physical examination and necessary investigations including Fine Needle Aspiration Cytology were workout in all patients. Most patient’s age was between 35 to 55 Years old.
Results: Results have shown in the present research that tuberculous lymphadenopathy is the most prevalent source of cervical lymphadenopathy with 59%, accompanied by persistent non-specific lymphadenopathy with 26. Of the 29 patients with granulomatous modifications in fine needle aspiration cytology, 49 had subsequent surgery and histological evidence of cytological presentation 25 reported Tuberculous Lymphadenopathy, so the sensitivity of Fine Needle Aspiration Cytology in diagnosing granulomatous lymphadenopathy relevant to tuberculosis was 85%. Non-specificity was documented histologically by one false positive Fine Needle Aspiration Cytology. There was swelling of the cervical lymph node during the latest investigation. Fever (29%), weight loss and appetite loss (18%), cold abscesses (7%), axillary and inguinal swelling (5%), discomfort (7%), sinus discharge, sore throat, old sinus scars, cough, teeth decay (3%) were other typical presenting symptoms. In 69% of cases, only unilateral node involvement was affected in 28 % of cases, while in 39 % of cases, bilateral involvement was affected in 12% of cases. In 11% of the instances, the lymph nodes were correlated with other lymph node classes.
Conclusion: In our investigation, the sensitivity and specificity of tuberculous cervical lymphadenopathy Fine Needle Aspiration Cytology are 81 and 96 respectively. The findings concluded that tuberculosis, accompanied by reactive lymphadenitis and metastatic deposits, was the common prevalent cause of cervical lymphadenopathy in the Indian community. Reactive lymphadenitis in multiple age groups, contagious in 35-55 years, is the most frequent cause of enlargement of the cervical lymph node. The age range involves tuberculosis and suppurative lymphadenitis, neoplastic lesions like metastatic cancer and nonhodgkin's lymphomas among more than 55 age levels. Fine Needle Aspiration Cytology is an essential diagnostic modality in severe cervical lymphadenopathy for the etiological workup and is just as responsive and precise as biopsy of the excision lymph node when expert eyes inspect an acceptable aspirate. The most prominent cause of neck lymphadenopathy is Reactive Lymphadenopathy. However, with non-neoplastic to neoplastic disorders, variable diagnosis can be possible.
1. Introduction
Lymph nodes, such as the spine, axilla, inguinal area and within the belly, are found in different areas of the body. Those lymph nodes have lymph that has a part in infection or the immune response [1]. Lymphadenopathy refers to the irregular scale, integrity or number of lymph nodes [2]. There are about 600 lymph nodes in the body, of which approximately 60-70 nodes are located in the area of the head and neck [18]. Any abnormality in the size, consistency, and number of lymph nodes is characterized as lymphadenopathy, caused by either inflammatory or neoplastic cells being invaded or propagated into the lymph node [19]. There is a broad division of lymphadenopathy into localised, generalised, and dermatopathic. It can be acute (2 weeks), subacute (4-6 weeks) and chronic, depending on the duration (does not resolve by 6 weeks duration). [20] For the development of a diagnosis,separating localised and generalised lymphadenopathy is very important. Lymph nodes are colonies of cells that are thin, circular or bean-shaped. There is a mixture of various kinds of immune system cells within the lymph nodes. As it passes through the bloodstream, these specialised cells filter the lymphatic fluid and protect you by killing invaders. Lymph nodes are clustered in clusters, and a particular region of the body is drained from each group. In such regions, such as the lymph nodes in your throat, under your chin, in your armpits and in your groyne, you might be more likely to experience swelling. The location of the lymph nodes that are swollen can help determine the underlying cause. Lymphadenopathy or adenopathy is a lymph node condition where the scale or consistency of the lymph nodes is irregular. Lymphadenitis, [21] causing enlarged or enlarged lymph nodes, is the inflammatory form of lymphadenopathy (the most common sort). In clinical practise, the difference between lymphadenopathy and lymphadenitis is rarely created, and the concepts are often viewed as synonymous. Lymphatic vessel inflammation is known as lymphangitis. [22] Scrofula is a popular term for bacterial lymphadenitis that attacks the lymph nodes in the neck.
A typical and nonspecific symptom is lymphadenopathy. Infections (from small ones like the common cold to serious ones such as HIV/AIDS), infectious diseases, and cancers are common causes. Mostly, lymphadenopathy is idiopathic and self-limiting as well. The most common cause of swollen lymph nodes is an infection, especially a viral infection, such as the common cold. The area of the head and neck is known as the most prevalent location for lymphadenopathy. The most important cause for lymphadenopathy, which is prevalent in India with locoregional diseases, tuberculosis, and filariasis, is inflammation. Iqbal et al. have found that 70.45% of cervical lymphadenopathy is caused by tuberculosis, 13.63% by reactive lymphadenitis, 11.36% by metastases, 4.54% by lymphoma, and 2.27% by chronic non-specific lymphadenitis. Clinically, if lymph nodes are swollen in just one region or "generalised" if they are swollen in two or more noncontiguous regions, lymphadenopathy may be categorised into "localised." The infected lymph nodes are swollen and tender in acute cases, usually infectious, and there can be a variable level of general constitutional disruption in patients with anorexia, pyrexia as well as malaise [5]. Lymph nodes are painless and not tender in chronic conditions, which may be owing to tuberculosis [3]. Therefore, a comprehensive record of age, period and severity of symptoms, together with an evaluation of the personality as well as position of the lymph nodes, combined with the required pathological diagnosis with a cytology or biopsy of fine needle aspiration, can help to treat the disease. The lymph nodes in the neck are classified into classes such as the anterior, submental, submandibular, supraclavicular, and posterior chain [4]. Neck lymphadenopathy is one of the most serious issues found in the outpatient department of surgery.
Exact identification of the origin of lymphadenopathy can also be complicated and can direct to identification complications that origin inadequate care and associated health concerns. There is definitely a variation between the aetiology and clinical diagnosis of cervical lymphadenopathy between various demographic groups. Understanding common symptoms and manifestations in the community of lymphadenopathy would allow the development of a sound clinical procedure in the assessment and diagnosis of this disease to prevent delays in care. This research was conducted to test the Neck lymphadenopathy with demographic factors with the cytopathological diagnosis.
2. Materials & Methods
The comparative retrospective research on 80 patients with cervical lymphadenopathy presenting in the surgical outpatient clinic of Madras Medical College was performed over a course of one and a half years from April 2018 to October 2019. Seventy-eight patients having swollen cervical lymph nodes were included in the analysis.
Provided written informed consent and details on sex, age, health characteristics and history of association with tuberculosis were gathered. Full blood tests, chest X-rays and fine needle aspiration cytology was accompanied by a thorough clinical review of the cervical lymph node. In twenty cases where fine needle aspiration cytology was inconclusive, the excision biopsy was perforated.
Inclusion Criteria:
Cases with other aetiology were not included in these patients, only inflammatory and infective cases were taken Name, Sex, Age, Address, Faith, Profession with patients Cases were stated to have been obtained at choice and only cases consenting for biopsy of the lymph node were selected for research.
Exclusion Criteria:
Except all forms of secondary neck and lymphoma
Exploration:
Investigations were carried out following clinical diagnosis to validate the diagnosis.
Assessment of Blood:
Hemoglobin percentage, differential count, overall white cell count, erythrocyte sedimentation rate, and blood assessment were performed.
Montoux Test:
It was performed by normal procedure and more than 13 mm of erythema is taken as positive after 52 hours.
Chest x-ray:
Photograph demonstrating the smear procedure for plating a sample aspirate. A second slide is used to smear the inhale uniformly over the top of the slide after dropping a slight drop of fluid on a glass slide. For cytologic examination, the slide is then packed. The images of an inhale being put on a glass slide. A few drop of aspirated fluid is taken on a glass slide after the 22-mL disposable syringe with an inserted 24-gauge needle is pointed under the skin surface and the mass is aspirated. A biopsy of the lymph node was performed in both cases. The specimen's macroscopic appearance was noticed and submitted for histopathological examination. The presence of Langhan's giant cell type was taken as the prerequisite for the diagnosis of lymph node tuberculosis [6]. All the specimens were treated by normal processes such as formalin fixation, microtome slicing, and gram and zeihl-Neelson stain staining. All the slides were examined using standard microscopes under 10X, 60X & 100X power. Gram stain and unique stain stained the aspiration substance from the cold abscess. Chest x-ray was workout in the above cases. Procedure of Biopsy The biopsy of the lymph node was conducted by infiltrating 1% lignocaine under local anaesthesia.
There have been biopsies of large lymph nodes where multiple lymph nodes are present. Posterior groups were favoured if anterior and posterior groups were involved. The lymph node and the capsule were taken. Care is taken concerning haemeostasis in the supraclavicular region.
Therapy Directly Observed Care, Short-course Approach of 3 months of acute treatment and 5 months of continuous process therapy with the medications Rifampicin, Pyrazinamide and Ethambutol is used to treat all patients with antituberculous medications. The research involved each patient above the age of 40 who identified with a palpable cervical lymph node.
The research removed patients under the age of 40, or where fine needle aspiration cytology or excisional biopsy could not be done. Only on the report of fine needle aspiration cytology was the diagnosis of the condition made. The Mathematical Kit for Social Science for Windows was used to conduct data processing. Categorical variables were presented with a percentage as the absolute figure.
3. Results
Seventy-eight patients were examined in total. The number of male and female patients, 54 male and 26 female, with a 2:1 ratio, was unequal. The problem of neck lymphadenopathy was most equently seen as seen in Table 1 at the age of 35-55 years.
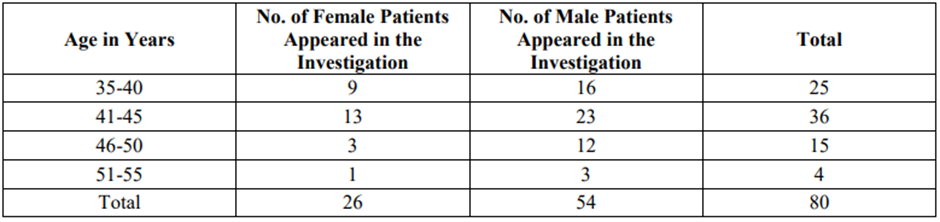
Table 1. Age and Sex Supplement of Neck Lymphadenopathy Patients
It can be seen from Table 2 that tuberculous lymphadenopathy is the very prevalent cause of 76% of neck lymphadenopathy, continued by 32% of recurrent non-specificlymphadenopathy.

Table 2. Aetiology of Neck Lymphadenopathy
Primary Symptoms: Both patients in the present investigation had swelling of the neck lymph node, as seen in Table 3. Fever (29 %), weight loss and appetite loss (18 %), cold abscesses (7 %), axillary and inguinal swelling (5 %), pain (7 %), sinus discharge, sore throat, old sinus scars, cough, rotting of the teeth (3 %) were more typical presenting symptoms.
| Symptoms Appeared in Patients | Number of Appearance | Percentage |
| Pain | 2 | 4% |
| Cold abscess | 5 | 10% |
| Soar throat | 1 | 1% |
| Loss of weight | 9 | 16% |
| Cough | 1 | 1% |
| Fever | 20 | 45% |
| Discharging sinus | 1 | 1% |
| Inguinal swelling | 2 | 4% |
| Old sinus scar | 1 | 1% |
| Axillary swelling | 2 | 4% |
| Carries tooth | 1 | 1% |
| Loss of appetite | 9 | 16% |
| Swelling in the Neck | 80 | 100% |
Table 3. Symptoms Appeared while the Current Investigation
Chest Radiography Results: It is very normal to have generalised tuberculosis which may or may not be associated with a known focus in the body. It is defined by simultaneous enlargement of all the lymph nodes that are palpable. Previous findings found that 18% had a related operative chest x-ray lesion. This analysis is consistent with that of S.D. 28 % of patients had active pulmonary tuberculosis consistent with Purohit tests, as demonstrated by chest x-ray [7]. As seen in the table, the prevalence of co-existing tuberculosis in body parts is minimal. In Faber's studies, the higher frequency was observed (18 %), the lower in Wiimont's studies (4 %). The frequency was 16% in the current report. Effect of Co-Existing Inquiries into Active Tuberculosis Lesions: As explained in Table 4, 5, & 6, the diagnosis of neck lymphadenopathy was made clinically and the tuberculous aetiology was confirmed by the different studies carried out.
Results | Number of Patients Appeared | Percentage |
| Healthy | 58 | 72.50% |
| Appearance of active tuberculosis | 22 | 27.50% |
Table 4. Inquiry of Active Tuberculosis Lesions
| Appearance of Cases Co-Existing Tuberculosis Patients | Number | Percentage |
| Appeared | 22 | 27.50% |
| Not Appeared | 58 | 72.50% |
Table 5. Co-Existing Inquiry of Active Tuberculosis Lesions
Diagnosis | ||
| Appeared Disease in Patients | Not Appeared Disease in Patients | |
| Appeared (Positive) | 39 | 4 |
| Not Appeared (Negative) | 19 | 18 |
| Total | 58 | 22 |
Table 6. Diagnosis of Neck Lymphadenopathy Appeared in the Patients
Blood: Blood sampling has been performed in both cases. 80 % of patients showed poor age %ages of haemoglobin. In the majority of cases, the white blood cell count was regular. There was lymphocytosis in some patients. The sedimentation rate of erythrocytes was increased in 62 % of cases. Although the rate of erythrocyte sedimentation is an unspecific investigation and not a diagnosis, when tracking the patient with antituberculosis chemotherapy, it is useful as a prognostic predictor. The sensitivity and precision of tuberculous cervical lymphadenopathy Fine Needle Aspiration Cytology in our research series is 81 and 96 respectively and has comparable findings in other studies as well. [8].
Figure 1 & 2 shows that tuberculous neck lymphadenopathy and fine needle aspiration with the aid of a Cameco syringe holder are primarily used for cystic lesions.
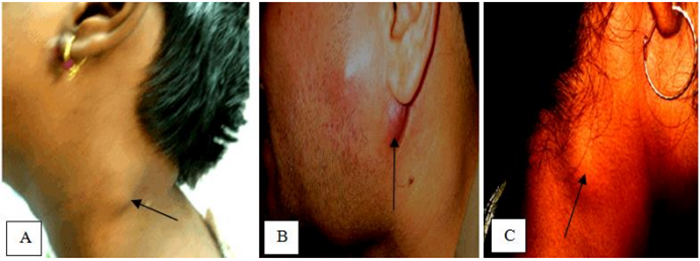
Figure 1. Tuberculous Neck Lymphadenopathy in A. Children, B. Male Adults & C. Female Adults
Figure 1A shows the neck lymphadenopathy appeared in the child. Figure 1B shows the neck lymphadenopathy appeared in the adult of male. Figure 1C shows the neck lymphadenopathy appeared in the adult of female.
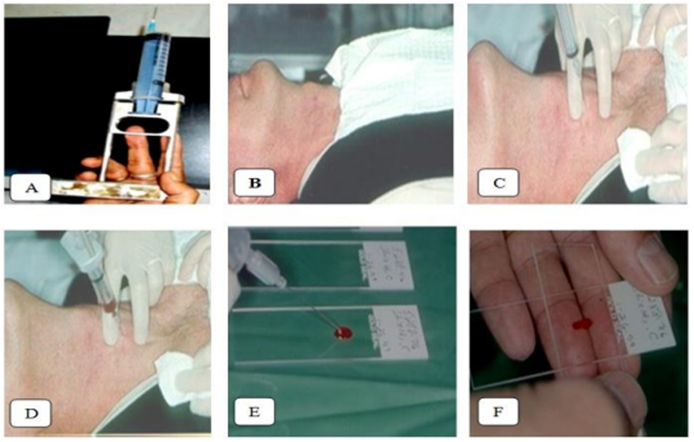
Figure 2. Fine Needle Aspiration with the Aid of a Cameco Syringe Holder Figure 2A, Fine-Needle Aspiration. Figure 2B, Patient location during aspiration of the fine-needle.
Hyperextension of the neck and optimum visibility are enabled by the supine posture and a cushion under that same patient's shoulder. The nodule is marked and stabilised with the non-aspirating hand of the operator in Figure 2C. On the hand of the patient, against that of the ear, the operator sits. From out anxiety over blood borne infections, existing Occupational Safety and Health Administration laws mandate the use of gloves. The needle moves through the skin with a short step in Figure 2D and reaches the nodule. There follows rapid mild suction. The suction is relaxed as soon as the aspirate arrives, and the needle is extracted. Figure 2E, Sample taken from the patients & drop on the cleaned slide. Figure 2F, Blood smear of the blood sample taken from the patients. IV. DISCUSSION Lymph nodes are the organs of lymphoid that are located in different areas of the body that are thought to be involved in immune defense [1]. Of the 800 lymph nodes are present in every human body, 300 are found in the throat [9]. The frequent problems appearing in the Surgery Outpatient Department is cervical lymphadenopathy, identified as nodes in the neck determining more than 1 cm in diameter [10]. The number of male and female patients, 54 male and 26 female, with a 2:1 ratio, was unequal. Women are more affected than men in the investigation completed by Narender NR, which is similar to the findings of the investigation completed by Sharma U. [11, 12]. Prasadarao Desari, however, concluded the investigation, and Pandy revealed marginally male preponderance. [13, 14]. In our research, the issue of neck lymphadenopathy was most frequently seen in the 35-55 age range. These observations are similar to studies performed by Liu B et al. [15]. In all 80 patients, Fine Needle Aspiration Cytology was followed by an easy, secure and cost-effective technique to diagnosis the cause of cervical lymphadenopathy is Fine Needle Aspiration Cytology. [16]. Reactive hyperplasia was seen in the majority of the 48 patients with 64.9 % cytology, followed by tuberculosis in 24 patients with 32.87 %. Our research coincides with the discovery of different experiments where the significant cause was tuberculosis.
In a potential clinicopathological investigation of cervical lymphadenopathy, the important aetiology was tuberculosis lymphadenopathy in patients 20 with 64.76 %, followed by non-specific chronic lymphadenopathy in patients 16 with 39.87 %, preceded by various relatively sporadic cases and irregular appearance of Kikuchi disease, Schwannoma, non-Hodgkin's lymphoma, pleomorphic adenoma, and secondary lymphoma [11]. This is close to the 32.89% result of the investigation conducted by Prasadarao et al, 62% of Padmanabh Inamdar, where tuberculosis is the common prevalent cause of neck lymphadenopathy, continued by reactive lymphadenopathy. In their future investigation, Pandy et al observed that most cases have non-neoplastic causes. [14] Reactive lymphadenitis and tuberculosis were widespread in the 35-55 age range in our investigation. This may be linked to areas vulnerable to illness and tuberculosis. Similar to other reports, Vedi et al documented tuberculosis in 48 % of cases. [17].
5. Conclusion
In our research of tuberculosis, the most significant source of cervical lymphadenopathy in our investigation population is reactive lymphadenitis and malignancy. They have remarkably distinct health characteristics in different age ranges. Careful clinical review may allow the diagnosis to be revealed. Fine Needle Aspiration Cytology is particularly responsive and highly precise investigation for early diagnosis.
6. Acknowledgement
The author is thankful to Department of Surgery, Madras Medical College for providing all the facilities to carry out this work.
7. Conflict of Interest
Nil
References
- Vimal S, Dharwadkar A, Chandanwale SS, Vishwanathan V, Kumar H. Cytomorphological study of lymph node lesions: A study of 187 cases. Med J DY Patil Univ.2016; 9(1):43-50.
View at Publisher | View at Google Scholar - King D, Ramachandra J, Yeomanson D. Lymphadenopathy in children: refer or reassure? Archives of disease in childhood. Education and practice. 2014; 99:101-10.
View at Publisher | View at Google Scholar - Reddy, M. Pradeep, Nekhil Moorchung, and Arun Chaudhary.
View at Publisher | View at Google Scholar - Ferlito, A., Robbins, K. T., Medina, J. E., Shaha, A. R., Som, P. M., & Rinaldo, A. Is it time to eliminate confusion regarding cervical lymph node levels according to the scheme originated at the Memorial Sloan-Kettering Cancer Center?. Acta oto-laryngologica, 2002; 122(8), 805-807.
View at Publisher | View at Google Scholar - Brucoli, M., Borello, G., Boffano, P., & Benech, A. Tuberculous neck lymphadenopathy: A diagnostic challenge. Journal of stomatology, oral and maxillofacial surgery, 2019; 120(3), 267-269.
View at Publisher | View at Google Scholar - Ghodke, B., Chaudhari, M., & Sharp, K. Retrospective Analysis of Fine Needle Aspiration Cytology Procedure at Tertiary Care Rural Hospital.
View at Publisher | View at Google Scholar - Alnour, T. M. Smear microscopy as a diagnostic tool of tuberculosis: Review of smear negative cases, frequency, risk factors, and prevention criteria. Indian Journal of Tuberculosis, 2018; 65(3), 190-194.
View at Publisher | View at Google Scholar - Rehman MA, Biswas MMA, Siddika ST, Sikder AM. Histomorphological pattern of Cervical Lymphadenopathy. J Enam Med. 2013; 3(1):13-7.
View at Publisher | View at Google Scholar - Stutchfield CJ, Tyrrell J, Evaluation of lymphadenopathy in children. Paediatr Child Health. 2012; 22(3):98-102.
View at Publisher | View at Google Scholar - Gaddey, H. L., & Riegel, A. M. Unexplained lymphadenopathy: evaluation and differential diagnosis. American family physician, 2016; 94(11), 896-903.
View at Publisher | View at Google Scholar - Narender NR, Rao YJ. A prospective clinicopathological study of cervical lymphadenopathy. Int Surg J. 2017; Dec. 4(12):3967-70. Medicine and Medical Sciences Research Vol 1, Issue 4, December 2021 Copyright © 2021 Mélange Publications 8
View at Publisher | View at Google Scholar - Dasari P, Varanasi S, Pattnayak S, Nagababu, Nandini. Cervical Lymphadenopathy: A Prospective Study in Rajiv Gandhi Institute of Medical Sciences, Andhra Pradesh. International Journal of Scientific Study. 2016; Aug. 4(5):233-8.
View at Publisher | View at Google Scholar - Sharma U, Bajaj A, Bamra NS. Clinicopathological evaluation of lymph node lesions by fine needle aspiration cytology. International Journal of Contemporary Medical Research. 2016; Feb. 3(2):542-5.
View at Publisher | View at Google Scholar - Pandy V, Amalan S, Mohankumar A, Ramesh E, Anandan H. Clinicopathological study of cervical lymph node enlargement: A prospective study. International Journal of Scientific Study. 2017; Apr. 5(1):75-7.
View at Publisher | View at Google Scholar - Liu, B., Gao, S., & Li, S. A comprehensive comparison of CT, MRI, positron emission tomography or positron emission tomography/CT, and diffusion weighted imaging-MRI for detecting the lymph nodes metastases in patients with cervical cancer: a meta-analysis based on 67 studies. Gynecologic and obstetric investigation, 2017; 82(3), 209-222.
View at Publisher | View at Google Scholar - Bhatta S, Singh S, Chalise SR. Diagnostic value of Fine Needle Aspiration Cytology in the Assessment of Cervical Lymphadenopathy. MedPhoenix. 2018; 3(1):36-40.
View at Publisher | View at Google Scholar - Vedi JN, Patel S, Ghormare A. Clinicopathological study in patients of cervical lymphadenopathy. Odisha J Otorhinolaryngol Head Neck Surg 2012; 6:14-7.
View at Publisher | View at Google Scholar - Teymoortash, A., & Werner, J. A. (2012). Current advances in diagnosis and surgical treatment of lymph node metastasis in head and neck cancer. GMS current topics in otorhinolaryngology, head and neck surgery, 11.
View at Publisher | View at Google Scholar - Khan, M. Y., Ali, S., & Umar, M. (2016). Evaluation of clinically Palpable Cervical Lymph Nodes by Fine Needle Aspiration Cytology, A Private Pulmo-Clinic Experience. Pakistan Journal of Chest Medicine, 22(1), 12-18.
View at Publisher | View at Google Scholar - Irwin, R. S., French, C. L., Chang, A. B., Altman, K. W., Adams, T. M., Azoulay, E., ... & Weinberger, M. (2018). Classification of cough as a symptom in adults and management algorithms: CHEST guideline and expert panel report. Chest, 153(1), 196-209.
View at Publisher | View at Google Scholar
View at Publisher | View at Google Scholar
View at Publisher | View at Google Scholar
