

Case Report | DOI: https://doi.org/10.31579/2834-8389/020
A Curious Case of Retained Gallstone
- Aditya Yawalikar *
- Shivani Desai, Neil Sheth
Postgraduate Student, Department of General Surgery, Bombay Hospital, New Marine Lines, Mumbai, Maharashtra, India.
*Corresponding Author: Aditya Yawalikar, Postgraduate Student, Department of General Surgery, Bombay Hospital, New Marine Lines, Mumbai, Maharashtra, India.
Citation: Aditya Yawalikar, Shivani Desai, Neil Sheth (2024), A Curious Case of Retained Gallstone, International Journal of Clinical Case Reports.3(3); DOI:10.31579/2834-8389/020
Copyright: © 2024, Aditya Yawalikar. This is an open-access artic le distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 02 May 2024 | Accepted: 09 May 2024 | Published: 16 May 2024
Keywords: surgeons prefer laparoscopy; microabscesses; retained gallstone
Abstract
Laparoscopy has become the first choice for cholecystectomy these days. Considering all the benefits of this choice like lesser post-op pain and post-op morbidity, shorter hospital stay [1], it also brings some complications to the table like CO2 narcosis, post-op shoulder tip pain, iatrogenic gall bladder perforation in one-third patients [2]. Perforation may cause spillage of gall bladder contents like sludge and stones. The latter ‘dropped’ stones are retrieved in all but two-third cases and complications can arise years later if not retrieved [3]. Though the incidence of these complications is low, effort should be taken to retrieve the spilled stone as they can result in a variety of problems [4]. These include abdominal abscess or a fistula formation. Abdominal abscesses may present with fever, abdominal pain and are most frequently located near the liver [5]. Abscesses are much more common than fistulas in these cases.
We report a case of a 30 year old female who presented with pain in abdomen while passing urine since 3 months. Patient had an operative history of laparoscopic cholecystectomy 2 years ago. She developed similar symptoms to what she has now one year ago which was diagnosed and treated as a UTI at the time. With no relief of symptoms, a USG and a CT were done which were suggestive of a mass thick walled soft tissue lesion with central abscess/necrosis/ haemorrhage abutting the superior wall of bladder. On excision biopsy this mass showed xanthogranulomatous and foreign body reaction to biliary material with small micro-abscesses. Patient was apparently alright after mass excision till 3 months ago when she again developed similar symptoms and with ascites. Two CT scans and an MRI later which were all insignificant, we did a diagnostic laparoscopy to find something interesting hiding from all the radiological investigations.
Introduction
Surgeons prefer laparoscopy as the first choice for cholecystectomy in most cases. In these cases, early return to regular activities, short hospital stays and lesser post-op pain and morbidity are noted as compared to open cholecystectomy. Though laparoscopy doesn’t come without any complications of its own. The incidence of iatrogenic gall bladder perforations have risen since the advent of laparoscopy. The spillage of gall bladder contents, especially stones warrants their removal to prevent future complications. Though these complications are rare, there is always an associated risk of the retained stone acting as a nidus for infection and subsequent intra-abdominal abscess formation. There is also a recognised risk of stone eroding through the abdominal wall forming fistula to the skin, umbilicus and gluteolumbar region. Abscess formation is much more common than fistulas and present with non-specific clinical symptoms like fever and abdominal pain. Stones within abscesses are not always recognised on radiological investigations which is very crucial. Unlike other intra- abdominal abscesses which are treated with drainage and antibiotics, abscesses due to dropped gallstones need removal of the retained stones or else the abscess will recur.
Case Report
A 30 year old female, with no history of any comorbidities, presented to our clinic with complains of pain in abdomen while passing urine since 3 months. The pain was insidious in onset and occurred whenever the patient had an urge to pass urine, while passing urine and for a few minutes after passing urine. Pain was over the infra- umbilical region, sharp, pulling in nature. There were no associated urinary complaints like burning micturition, hematuria and no history of fever. The patient had a previous operative history of laparoscopic cholecystectomy done in view of symptomatic cholelithiasis 2 years ago. She then presented with similar symptoms of abdominal pain while passing urine 1 year ago. On investigations, patient had a thick walled soft tissue lesion with central abscess/necrosis/haemorrhage in the supravesical region abutting the superior wall of bladder. Patient provides another operative history of excision of this mass. a histopathology of this mass suggested extensive xanthogranulomatous and foreign body reaction to (probably) biliary material with small microabscesses. Following this laparotomy the patient was apparently alright till 3 months ago when she developed current complaints and underwent 2 CT scans and an MRI which were all suggestive of loculated ascites and some adhesions of small bowel to anterior abdominal wall. Ascitic tapping was done and fluid sent for investigations which all came back within normal limits.
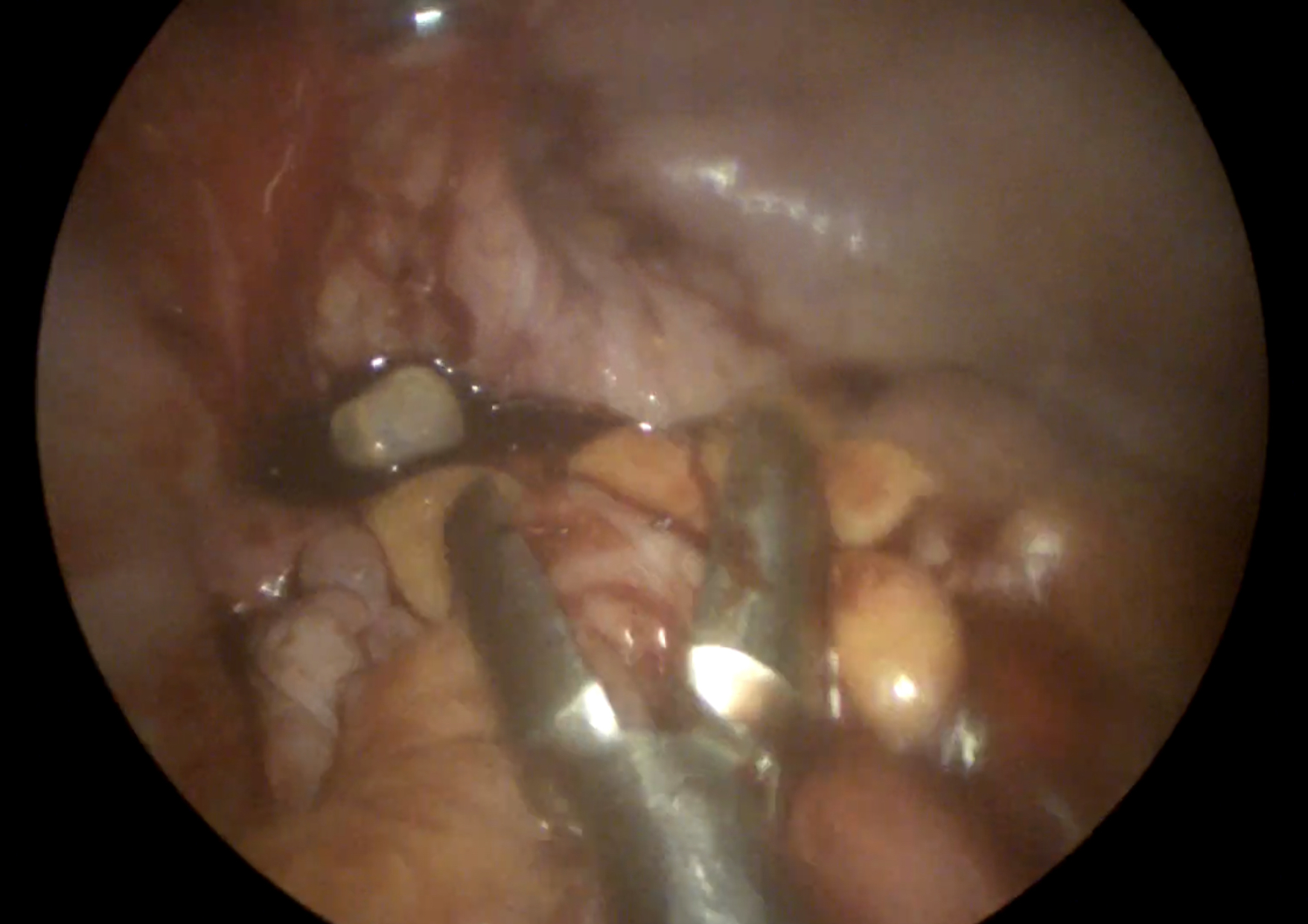
On examination, there were no positive findings. The patient was advised a diagnostic laparoscopy. Intra-operatively, adhesions of small bowel to the lower anterior abdominal wall which were cleared and haemostasis confirmed. On further exploration, a large gallstone was visualised sitting in the uterovesicle recess. This stone was retrieved and no other stones were found on further exploration. The procedure was uneventful. Post-op the patient passed urine and was vitally stable. Oral liquids were started the same day which the patient tolerated. On POD1 the patient was vitally stable with only mild suture site pain, tolerated full diet by the same night. Patient being clinically and vitally stable was discharged on POD2.
Figure 1: Adhesions of small bowel to anterior abdominal wall
Discussion
Laparoscopic cholecystectomy has become one of the commonest surgeries performed in modern times. With the advent of laparoscopy as the method of choice for cholecystectomy, instances of iatrogenic perforation and spillage of stones has also raised. They disseminate throughout the abdominal cavity due to pneumoperitoneum and irrigation [6]. Though rare, these dropped stones have been recognised to cause complications like abscess formation later [7]. Some even rarer complications include migration of stones to pleural cavity due to diaphragmatic defects especially in elderly causing pleural empyema, pleural lithiasis and cholelithoptysis [8]. The need for re- exploration to tackle these complications can be avoided by careful separation of gall bladder from gall bladder fossa during laparoscopy as most perforations occur during this step [9]. Perforation can also occur while delivering the gall bladder out from port and hence extra care should be taken at this step too. Perforation of gall bladder is not considered a major problem by most surgeons and they believe that its harmless [7] even though several studies have established its complications. On CT, dropped gallstones with high calcium content appear as one or more calcified high-attenuation foci. Wide window settings are beneficial in discerning calcified stones. Pure cholesterol gallstones and those with low calcium content may go undetected. On MR, pigmented DGs may appear as hyperintense on T1 weighted images, whereas other stones are hypointense on both T1 and T2 weighted images. Lack of contrast enhancement is useful for making the correct diagnosis [5]. On ultrasound, DGs appear as mobile hyperechoic foci casting marked posterior acoustic shadowing [10].
Conclusion
In conclusion, complications of retained gallstones are rather rare. Even though rare, it is advised to retrieve every dropped gallstone owing to its cumbersome complications. This case has also taught us that radiological investigations are not a 100% sensitive for picking up stones. As in this case Ultrasonography, CT and MRI proved to be of limited use. The lesson learnt here is that proper history taking and clinical examination takes us a long way and radiological investigations need only be tools of support in such cases.
Conflict of Interest
None
References
- Shrestha B, Dunn L. The Declaration of Helsinki on Medical Research involving Human Subjects: A Review of Seventh Revision. J Nepal Health Res Counc. 2020;17(4):548-552.
View at Publisher | View at Google Scholar - Rice DC, Memon MA, Jamison RL, Agnessi T, Ilstrup D, Bannon MB, et al (1997). Long-term consequences of intraoperative spillage of bile and gallstones during laparoscopic cholecystectomy. J Gastrointest Surg1:85–90.
View at Publisher | View at Google Scholar - Helme, S., Samdani, T. & Sinha, P (2009). Complications of spilled gallstones following laparoscopic cholecystectomy: a case report and literature overview. J Med Case Reports 3, 8626.
View at Publisher | View at Google Scholar - Zehetner J, Shamiyeh A, Wayand W (2007). Lost gallstones in laparoscopic cholecystectomy: all possible complications. Am J Surg. 193(1):73-78.
View at Publisher | View at Google Scholar - Nayak L, Menias CO, Gayer G (2013). Dropped gallstones: spectrum of imaging findings, complications and diagnostic pitfalls. Br J Radiol.;86(1028):20120588.
View at Publisher | View at Google Scholar - Out of Sight but Kept in Mind: Complications and Imitations of Dropped Gallstones Nitin K. Ramamurthy, Velauthan Rudralingam, Derrick F. Martin, Simon W. Galloway, and Sathi A. Sukumar American Journal of Roentgenology 2013 200:6, 1244-1253
View at Publisher | View at Google Scholar - Åsa Edergren, Gabriel Sandblom, Thorhallur Agustsson, Gona Jaafar (2022). Intraoperative gallbladder perforation and risk of postoperative abscess with or without antibiotics: national cohort study of more than 108 000 cholecystectomies, British Journal of Surgery, znac351,
View at Publisher | View at Google Scholar - Zehetner J, Shamiyeh A, Wayand W (2007). Lost gallstones in laparoscopic cholecystectomy: all possible complications. Am J Surg 193:73–78
View at Publisher | View at Google Scholar - Yunus Emre Altuntas,1 Mustafa Oncel,2 Mustafa Haksal,2 Metin Kement,1 Ersin Gundogdu,1 Nihat Aksakal,3 and Fazli Cem Gezen2 Gallbladder perforation during elective laparoscopic cholecystectomy: Incidence, risk factors, and outcomes, North Clin Istanb. 2018; 5(1): 47–53.
View at Publisher | View at Google Scholar - Viera FT, Armellini E, Rosa L, Ravetta V, Alessiani M, Dionigi P, et al (2006). Abdominal spilled stones: ultrasound findings. Abdom Imaging 31:564–567
View at Publisher | View at Google Scholar
