

Case Report | DOI: https://doi.org/10.31579/2835-785X/013
A Complication in Gastric Bypass: Gastro-Jejunal Twisting
- Gianfranco Gioia *
- Paolo Calò
Medical Doctor, Bariatric Surgery, Sandro Pertini Hospital, Rome, Italy.
*Corresponding Author: Gianfranco Gioia. Medical Doctor, Bariatric Surgery, Sandro Pertini Hospital, Rome, Italy.
Citation: Gianfranco Gioia, Paolo Calò. (2023). A Complication in Gastric Bypass: Gastro-Jejunal Twisting, International Journal of Clinical Research and Reports 2(1); DOI: 10.31579/2835-785X/013
Copyright: © 2023, Gianfranco Gioia, this is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 03 February 2023 | Accepted: 10 February 2023 | Published: 16 February 2023
Keywords: gastric bypas; gastro-jejunal twisting; surgical approach
Abstract
The gastric bypass operation is an effective procedure to achieve weight loss in overweight patients
Case Study
The gastric bypass operation is an effective procedure to achieve weight loss in overweight patients. But long-term chronic complications after Roux-en-Y gastric bypass (Figure 1) are possible, such as König’s syndrome (i. e. abdominal pain related to meals with diarrhea, constipation, meteorism, and abdominal distension) or candy cane syndrome (i. e. chronic abdominal pain, vomiting, dysphagia, and nausea).

Best long-term follow-up diagnostic exams are barium swallow, oesophago-gastro-duodenoscopy, and, in our case, explorative laparoscopy after computed tomography (CT) with oral contrast showing the presence of a blind and twisted afferent Roux limb at the gastrojejunostomy, i. e. candy cane syndrome (Figure 2).

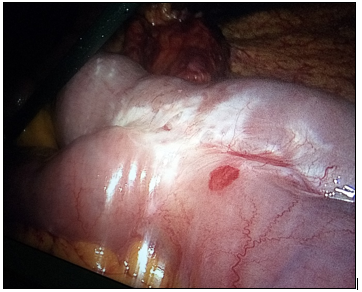
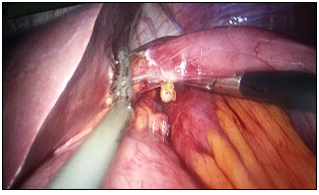
There are little data about the efficacy of surgical revision (1, 2) that seems to be the best treatment with symptomatic relief. In our case study, a 40-year-old female patient with an initial body mass index (BMI) of 36.5 kg/m2 was submitted for a Roux-en-Y gastric bypass. At the 3-year follow-up, BMI was 22.4 kg/m2 with a significant weight loss. In the last 2 months, there was a further weight loss of 6 kg with the presence of chronic abdominal pain, dyspepsia, dysphagia, abdominal distension, and vasomotor problems (hot flushing, sweating, palpitations, and diarrhea). So, consequently to CT, the patient was submitted for: diagnostic laparoscopy showing the integrity of distal anastomosis (Figure 3),
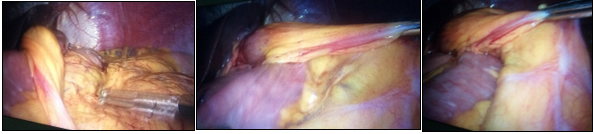
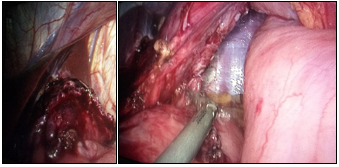
the presence of a twisted candy cane (Figure 4)
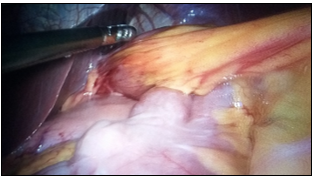
liver (Figure 6) and proximal anastomosis;identification and resection (Figure 7)
of proximal anastomosis with isolation of gastric reservoir (Figure 8)
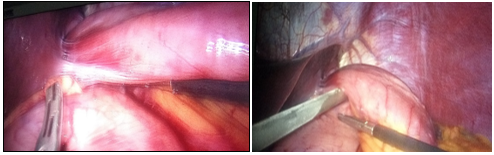
untwisting, right repositioning, lifting and re-anastomosis of proximal bypass with gastric reservoir (Figure 9).

The postoperative stages were uneventful and the patient was discharged on the third postoperative day. Finally, our lifting surgical approach led us to conclude that this complication could be avoided by not making such a long loop in gastric bypass surgery.
References
- Cartillone M, Kassir R, Mis TC, Falsetti E, D'Alessandro A, Chahine E, Chouillard E. König's (2020) Syndrome After Roux-en-Y Gastric Bypass: Candy Cane Twist. Obes Surg 30(8): 3251-3252.
View at Publisher | View at Google Scholar - Owens M, Shukla H, Sczepaniak J, Mahdavi A. (2013) Variations on bowel obstruction after gastric bypass and management of the twisted Roux limb. Surg Obes Relat Dis 9(6): 1020-1021.
View at Publisher | View at Google Scholar
