

Case report | DOI: https://doi.org/10.31579/2834-8532/029
A Case Report of Turner Syndrome with Hyper Parathyrodism and Osteoporosis in Adult
- Nezar Mohammed Kheir Mohammed Kheir 1
- Nahla Ahmed Mohammed Abderahman 2*
- Sohep Abdalla Osman 3
- Mohammed Ahmed Ibrahim Ahmed 3
1 MD of Obstetrics and Gynecology SMSB, OBGYN Specialist Atabra Teaching hospital and Elfadlab Hospital River Nile State-Sudan.
2 Assistant professor of Biochemistry, Faculty of Medicine, Department of Biochemistry, Nile Valley University- Atbara, Sudan
3 Assistant professor of Internal Medicine, Endocrinologist, Elsheikh Abdallah Elbadri University-Faculty of Medicine, Sudan 4Assistant professor of Microbiology, Faculty of Medicine, Department of Microbiology, MBBS Bachelor of Medicine and Surgery Nile Valley University- Atbara, Sudan
*Corresponding Author: Nahla Ahmed Mohammed Abdurrahman, Assistant professor of Biochemistry, Nile Valley University, Faculty of Medicine- Atbara, Sudan.
Citation: Nezar M. K. Mohammed, Nahla A. M. Abderahman, Sohep Abdalla Osman, Nahla A.M. Abdurrahman, (2023), A Case Report of Turner Syndrome with Hyper Parathyrodism and Osteoporosis in Adult, Clinical Genetic Research, 2(6); Doi:10.31579/2834-8532/029
Copyright: © 2023 Nahla A.M. Abdurrahman, this is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 12 June 2023 | Accepted: 20 June 2023 | Published: 04 December 2023
Keywords: turner syndrome; parathyrodism; osteoporosis; sudan
Abstract
Background: Turner Syndrome TS (or Bonnevie-Ullrich syndrome, also known as congenital ovarian hypoplasia syndrome) has multiple comorbidities but they are treatable conditions e.g diabetes, hypertension, osteoporosis and cardiac anomalies, so early recognition and proper treatments are needed.
Consent: Written informed consent was obtained from the patient's legal guardian for publication of this case report and any supplementary images
Case Report: A18-year-old Sudanese female who was presented with typical TS features has been reported in Elfadlab hospital-River Nile State-Sudan.
Introduction
TS defined as the combination of characteristic physical features and complete or partial absence of the second sex chromosome, with or without cell line mosaicism (Ballabio A, and Andria G, 1992). It is result as a monosomy or structural defect of the X chromosome that is characterized by short stature, webbing of the neck, cubitus valgus, sexual infantilism, ovarian failure, (Turner HH, 1938), congenital lymphedema of the feet and hands, widely spaced nipples, and primary amenorrhea. It is also associated with congenital renal (horseshoe kidney), cardiovascular (coarctation of the aorta or bicuspid aortic valve), thyroid disease (Atton G et al. 2015), immune diseases and disturbances of the lipid glucose and bone metabolism (Davenport ML, 2010). Additionally, the oral cavity exhibited a number of characteristics such as a high-arched palate, a hypoplastic mandible, thin enamel and less dentin, tooth mobility, periodontal pockets, prematurely erupted teeth, and different malocclusions (Kasagani SK, et al. 2011).
Depending on karyotyping, these clinical manifestations might change. While most females with TS suffer from ovarian failure, some individuals with mosaicism simply exhibit small height and primary amenorrhea without other dysmorphic traits (Murdock DR, et al. 2017). Females with TS have hypergonadotropic hypogonadism as a result of ovarian failure. Only around 4% of girls with TS have menarche, despite the fact that over 30% of them naturally enter puberty (Zhong Q and Layman LC. 2012).
Different karyotypes can be seen in women who have TS, all of which lack X-chromosomal material and cause the onset of the clinical illness (Gravholt, CH. et al. 2017). The karyotype 45, X (total loss of one X chromosome) and various mosaics such as 45, X/46, XX and 45, X/47, XXX. According to Gravholt, CH. et al. 2017 and El-Mansoury, M. et al. 2007, the 45, X karyotype is prevalent in about 40–50% of women with TS (Gravholt, CH. et al. 2017; El-Mansoury, M. et al. 2007). 20% of women have isochromosomes, 15 to 25 percent have mosaicism with the 45, X/46, XX chromosomes, and just a few women have ring X chromosomes. Additionally, 10-12% of women have varying quantities of the Y chromosome; of these women, 3% have 45, X/46, XY (Gravholt, CH. et al. 2017; Cameron- Pimblett, A et al. 2017).
There aren't many research from Africa, Asia, or South America regarding TS, however the female phenotype for TS occurs in communities of many ethnicities at around 50 per 100,000 with median age at diagnosis around 15 years (Stochholm, K., et al. 2006; Berglund, A., et al. 2019) indicating that many females with TS are not identified until maturity, and others are never (Tuke, M. A. et al. 2019).
Case presentation
A Sudanese female of 18 years old who visited the obstetrics and gynecology referral clinic at Elfadlab Hospital in River Nile State, Sudan, was found to be underweight, have primary amenorrhea, and the breasts is not developed. Examining the patient's prior medical history, current medicines, dietary supplements, allergies, and social background revealed nothing noteworthy. No one in the family shared her facial characteristics or other dysmorphic traits, and no birth defects, sexual anomalies, or hereditary disorders were noted. However, her parents were consanguineous, which is unusual. The normal history and clinical dysmorphic characteristics were used to make the clinical diagnosis of TS.
On Examination: Upon physical examination, the patient was hemodynamically stable, blood pressure (BP) 100/70 millimeter of mercury (mmHg), Pulse 82, respiratory rate (RR) 16, weight 33-kilogram (kg), height 137 (centimeter) cm, and BMI was 17.58.
Dysmorphic Features: The phenotype of current case was reported and conformed by photographic image which was presented in image1-5.
Image 1 and 2 showed webbing, a low-set posteriorly orientated ear, a short lower jaw (micrognathia) and a short wide neck.

Image 1: Turner Syndrome phenotype

Image 2: Turner Syndrome phenotype

Image 3: Turner Syndrome phenotype
Widely spaced nipples were seen in image 3.

Image 4: Turner Syndrome phenotype
Cubital valgus increased angulation was visible at the elbow in image 4.



Image 5: Turner Syndrome phenotype
Bilateral short fourth fingers and Fingernails and toenails that turn slightly upward (Spoon shaped nails) were represented in image 5.
Biochemical Measurements:
The level of gonadotropin level on 12/9/2022 of the case showed increased of Follicle Stimulating Hormone (FSH level= 171 IU/L) and Luteinizing Hormone (LH level=29. 8 IU/L). On 9/12/2022, the primary laboratory profile comprised the following biochemical measurements: whole blood count, Renal and liver function tests, fasting blood sugar concentration, serum uric acid, and lipid profiles levels. The results showed that all of these tests were within normal ranges with the exception of serum calcium Ca++, which had an increased level (11.1 mg/dl).
| Measurements | On 3-11-2022 and 28-12-2022 | On 24-01-2023 |
| Calcium | 8.9 mg\dl | 8.9 mg\dl |
| Sodium | 134mmol\l | - |
| Potassium | 3.8mmol\l | - |
| Phosphorus | 5.1 mg\dl | 4.6 mg\dl |
| Serum Creatinine | 0.6 mg\dl | - |
| Serum Urea | 16mg\dl | - |
| Uric Acid | 3.5mg\dl | - |
| Random blood glucose | 87mg\dl | - |
| Cholesterol | 146mg\dl | - |
| Triglycerides | 79mg\dl | - |
| Alkaline Phosphatase | 164 IU\L | - |
| Para thyroid hormone | 77.7 Pg | 76 Pg |
| Vitamin D | 14.8 ng\ml | 10.9 ng\ml |
mg\dl= milligram per deciliter; mmol\l= millimol per liter; IU\L= international Unit per liter; pg=pictogram; ng per ml=Nano gram per milliliter.
Table 1: Biochemical measurements of the patient
Speculum Examination: revealed normal external genitilia.
Computed Tomography (Ct) Of Upper Abdomen & Pelvis: Examination was done without using oral and IV contrast on 12/9/2022.
Findings:
- Liver is normal in size with smooth contour. There is no solid or cystic focal mass lesion. Portal and hepatic veins are normal. Intrahepatic and extra hepatic bile ducts are not dilated. Gall bladder is unremarkable.
- Spleen is normal in size with homogenous parenchymal density.
- Head, body and tail of pancreas appeared normal. Per-pancreatic fat tissue is intact.
- Both kidneys are normal in size with smooth contour. Parenchymal density is homogenous. No pelvic-alyceal dilatation is identified. Peripheral areas are normal.
- Adrenal glands are normal in morphology and density.
- Aorta and vena cava inferior appear normal. There is no pathology in para-aortic region
- Urinary bladder is not distended, TS wall and lumen cannot be evaluated.
- Uterus and ovaries are not visualized. No mass -like density in these beds.
- Rectum and perirectal region are normal. No abnormality in ischiorectal fossae.
- No free or loculated intra-abdominal fluid collection is identified.
- Lumbar lordosis is accentuated. Right ward scoliosis is also noticed.
- There is diffuse trabecular density decrease indicating osteoporotic changes.
Findings of ultrasound of genitourinary system:
- Kidneys both RT< kidneys>
- Urinary bladder normal wall thicknesses no stone.
- Small uterus noted 4.5 cms uterine length, 0.6cm thickness.
- Both ovaries not noted (Extremely Small).
- No ascites No mass.
Clinical Photographs of The Patient: Chromosome analysis, which was part of further investigation, revealed a gene karyotype of 45X.

Image 6: Karyotype of the patient
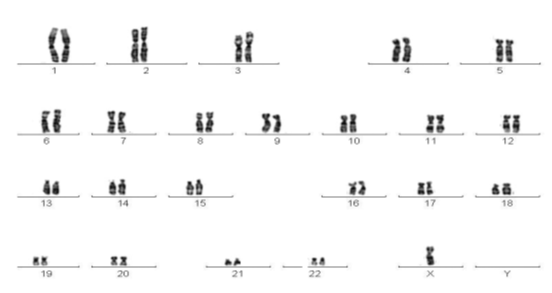
Image 7: Turner syndrome karyotype (45 X), Source: (Gravholt, CH, et al. 2017)
Echocardiography:
Echocardiography report noted no cardiac anomaly.
Final Comments:
Hyperparathyroidism was firstly suggested by the finding of an elevated serum calcium concentration with osteoporosis in addition to high gonadotropin level and luteinizing hormone indicating primary amenorrhea. In view of clinical photographs of the patient, CT of upper abdomen & pelvis and chromosomal analysis confirmed the diagnosis of Turner’s syndrome.
Discussion
The definition of the current case as TS was consistent with the recommendation made by Saenger P. et al in their 2001 research, which advised physicians to evaluate the diagnosis of TS in any female patient who had unexplained growth failure or pubertal delay with primary or secondary amenorrhea as result of increased levels of FSH, or small height with diminishing development velocity (10th percentile for age). Moreover, any pattern of the TS stigmata seen in the newborn period or subsequently any constellation of the following: cubitus valgus, nail hypoplasia, hyperconvex uplifted nails, multiple pigmented nevi, characteristic faces, short fourth metacarpal, and high arched palate, extensive and chronic problems with otitis media in addition to absence of breast development by 13 years of age besides unexplained short stature in adolescence (Saenger P. et al 2001).
The results of recent case were match with those of Elsheikh M, et al. 2001 and Gravholt CH. 2005 who found that the uterus in turner females is small because its full development depends on hormonal stimuli and that the gonads are typically two fibrous streaks in which no germ cells or follicular formations are present but only tissue similar to the stroma of the ovarian cortex is found. (Elsheikh M, et al. 2001; Gravholt CH. 2005).
Due to comparable phenotypic and subtle signs, TS is associated with hyperparathyroidism, osteoprosis, decreased Ca++ level and deficiency of vitamin D which were clearly identified in the present case. According to Radetti G et al. (1995), between 10 and 30% of people with TS experience primary hypothyroidism, which is typically accompanied by antithyroid antibodies (Radetti G et al. 1995). Increased in age was proportionate with osteoporosis and a decrease in bone density. According to researches, patients with TS above the age of 45 years had a greater risk of all fractures, which is consistent with many previous data. In order to adjust for this, persons with TS should have measurements of bone mineral density performed at their initial visit and again three to five years later (Gravholt CH, et al. 1998; Landin-Wilhelmsen K, et al. 1999). Additional measurements may be taken at less frequent intervals if there is no change. Modern guidelines for treating osteoporosis should be used if there is a considerable decline in bone mass.
Conclusions
According to the karyotype 45, X chromosome beside phenotype abnormality which was detected, a female with TS was confirmed. Photograph indicated small uterus noted 4.5 cms uterine length, 0.6 cm thickness, both ovaries not noted (Extremely small). Uterus and ovaries are not visualized. No mass like density in these beds. The ultra sound detected diffuse trabecular density decrease indicating osteoporotic changes.
Recommendations
- Early diagnosis of such cases is crucial during the prenatal and neonatal stages.
- Patients who have TS require extensive monitoring and care, ideally from a specialized multidisciplinary clinic, in order to live healthy and somewhat normal lives.
- In order to detect mullerian malformations, transvaginal or abdominal ultrasonography should be used as the primary imaging technique.
- Early specialized care engagement is essential to discuss treatment choices, offer psychiatric support, and check for conditions such congenital heart disease, horseshoe kidney disease, and hypothyroidism that are frequently linked to TS.
- When treating osteoporosis in a patient with TS and normocalcaemia, serum calcium levels and hyperparathyroidism should be closely monitored.
Acknowledgement
I want to thank Professor Imad Fadl-Elmula from the MD Craiova University and the Swedish Board of Urology. Lund University PhD in clinical genetics n-DIP in pediatric urology -Dip- Consultant Urologest and andrologest, Malamo Renal Transplant. Chromosome analysis consultant clinical geneticist and molecular biologist.
References
- Atton G, Gordon K, Brice G, Keeley V, Riches K, Ostergaard P, Mortimer P, Mansour S. (2015). The lymphatic phenotype in Turner syndrome: an evaluation of nineteen patients and literature review. Eur J Hum Genet, 23(12):1634-1639.
View at Publisher | View at Google Scholar - Ballabio A, Andria G. (1992). Deletions and translocations involving the distal short arm of the human X chromosome: review and hypotheses. Hum Mol Genet, 1(4):221-227.
View at Publisher | View at Google Scholar - Berglund A, Viuff MH, Skakkebæk A, Chang S, Stochholm K, Gravholt CH. (2019). Changes in the cohort composition of turner syndrome and severe non-diagnosis of Klinefelter, 47, XXX and 47, XYY syndrome: a nationwide cohort study. Orphanet J Rare Dis, 14:14(1):16.
View at Publisher | View at Google Scholar - Cameron-Pimblett A, La Rosa C, King TFJ, Davies MC, Conway GS. (2017). The Turner syndrome life course project: Karyotype-phenotype analyses across the lifespan. Clin Endocrinol (Oxf), 87(5):532-538.
View at Publisher | View at Google Scholar - Davenport ML. (2010). Approach to the patient with Turner syndrome. J Clin Endocrinol Metab, 95(4):1487-1495.
View at Publisher | View at Google Scholar - El-Mansoury M, Barrenäs ML, Bryman I, Hanson C, Larsson C, Wilhelmsen L, Landin-Wilhelmsen K. (2007). Chromosomal mosaicism mitigates stigmata and cardiovascular risk factors in Turner syndrome. Clin Endocrinol (Oxf), 66(5):744-751.
View at Publisher | View at Google Scholar - Elsheikh M, Wass JA, Conway GS. (2001). Autoimmune thyroid syndrome in women with Turner's syndrome--the association with karyotype. Clin Endocrinol (Oxf), 55(2):223-236.
View at Publisher | View at Google Scholar - Gravholt CH, Juul S, Naeraa RW, Hansen J. (1998). Morbidity in Turner syndrome. J Clin Epidemiol, 51(2):147-158.
View at Publisher | View at Google Scholar - Gravholt CH. (2005). Epidemiological, endocrine and metabolic features in Turner syndrome. Arq Bras Endocrinol Metabol, 49(1):145-156.
View at Publisher | View at Google Scholar - Gravholt CH, Andersen NH, Conway GS, Dekkers OM, Geffner ME, Klein KO, Lin AE, Mauras N, Quigley CA, Rubin K, Sandberg DE, Sas TCJ, Silberbach M, Söderström-Anttila V, Stochholm K, van Alfen-van derVelden JA, Woelfle J, Backeljauw PF. (2017). International Turner Syndrome Consensus Group. Clinical practice guidelines for the care of girls and women with Turner syndrome: proceedings from the 2016 Cincinnati International Turner Syndrome Meeting. Eur J Endocrinol, 177(3): 1-70.
View at Publisher | View at Google Scholar - Kasagani SK, Mutthineni RB, Jampani ND, Nutalapati R. (2011). Report of a case of Turner's syndrome with localized aggressive periodontitis. J Indian Soc Periodontol, 15:173-176.
View at Publisher | View at Google Scholar - Landin-Wilhelmsen K, Bryman I, Windh M, Wilhelmsen L. (1999). Osteoporosis and fractures in Turner syndrome-importance of growth promoting and oestrogen therapy. Clin Endocrinol (Oxf), 51(4):497-502.
View at Publisher | View at Google Scholar - Murdock DR, Donovan FX, Chandrasekharappa SC, Banks N, Bondy C, Muenke M, Kruszka P. (2017). Whole-Exome Sequencing for Diagnosis of Turner Syndrome: Toward Next-Generation Sequencing and Newborn Screening. J Clin Endocrinol Metab, 1;102(5):1529-1537.
View at Publisher | View at Google Scholar - Radetti G, Mazzanti L, Paganini C, Bernasconi S, Russo G, Rigon F, Cacciari E. (1995). Frequency, clinical and laboratory features of thyroiditis in girls with Turner's syndrome. The Italian Study Group for Turner's Syndrome. Acta Paediatr, 84(8):909-912.
View at Publisher | View at Google Scholar - SAENGER, P, K. (2001). ALBERTSSON WIKLAND, G. S. CONWAY, M. DAVENPORT, C. H. GRAVHOLT, R. HINTZ, O. HOVATTA, M. HULTCRANTZ, K. LANDIN-WILHELMSEN, A. LIN, B. LIPPE, A. M. PASQUINO, M. B. RANKE, R. ROSENFELD, AND M. SILBERBACH. Recommendations for the Diagnosis and Management of Turner Syndrome, The Journal of Clinical Endocrinology & Metabolism, 86:7(1):3061-3069.
View at Publisher | View at Google Scholar - Stochholm K, Juul S, Juel K, Naeraa RW, Gravholt CH. (2006). Prevalence, incidence, diagnostic delay, and mortality in Turner syndrome. J Clin Endocrinol Metab, 91(10):3897-3902.
View at Publisher | View at Google Scholar - Tuke MA, Ruth KS, Wood AR, Beaumont RN, Tyrrell J, Jones SE, Yaghootkar H, Turner CLS, Donohoe ME, Brooke AM, Collinson MN, Freathy RM, Weedon MN, Frayling TM, Murray A. (2019). Mosaic Turner syndrome shows reduced penetrance in an adult population study. Genet Med, 21(4):877-886.
View at Publisher | View at Google Scholar - HENRY H. TURNER, A (2012). SYNDROME OF INFANTILISM, CONGENITAL WEBBED NECK, AND CUBITUS VALGUS, Endocrinology, 23(5): 566-574.
View at Publisher | View at Google Scholar - Zhong Q, Layman LC. (2012). Genetic considerations in the patient with Turner syndrome--45, X with or without mosaicism. Fertil Steril, 98(4):775-779.
View at Publisher | View at Google Scholar
