

Case Report | DOI: https://doi.org/10.31579/2835-2971/006
A Case of Familial Hypokalemic Periodic Paralysis Admitted to the Intensive Care Unit After Traffic Accident
- Ahmet Salih Tüzen *
- Ozan Şanlı
- Atilla Şencan
- Ahmet Arıkanoğlu
- Nagihan Karahan
Department of Anesthesiology and Reanimation, Izmir Katip Celebi University Ataturk Training and Research Hospital, Izmir, Turkey
*Corresponding Author: Department of Anesthesiology and Reanimation, Izmir Katip Celebi University Ataturk Training and Research Hospital, Izmir, Turkey
Citation: Ahmet S. Tüzen, Şanlı O., Şencan A., Arıkanoğlu A., Karahan N. (2022) A Case of Familial Hypokalemic Periodic Paralysis Admitted to the Intensive Care Unit After Traffic Accident. Clinical Pediatrics and Mother Health, 1(2); DOI:10.31579/2835-2971/006
Copyright: © 2022 Ahmet Salih Tüzen, This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 28 September 2022 | Accepted: 27 October 2022 | Published: 14 November 2022
Keywords: hypokalemic periodic paralysis; familial hypokalemic periodic paralysis
Abstract
Hypokalemic periodic paralysis (HPP) is a clinical syndrome characterized by low serum potassium levels and sudden systemic muscle weakness. There are several factors that cause hypokalemia attacks in HPP. In this case, hypokalemia attacks were observed in three different time periods, in the posttraumatic emergency department, in the orthopedic clinic, and in the intensive care unit for pulmonary contusions. To our knowledge, this is the first case to report on the follow-up and treatment process in the ICU. It is very important to be aware of this situation, which can be life-threatening, to avoid hypokalemia attacks and to manage the process well as a multidisciplinary team.
Introduction
Hypokalemic periodic paralysis (HPP) is a clinical syndrome characterized by low serum potassium levels and sudden systemic muscle weakness. Familial hypokalemic periodic paralysis (FHPP) is the most common form of hypokalemic periodic paralysis in the Caucasian population. The disease is inherited in an autosomal dominant manner and its attacks can be fatal [1]. Factors that can trigger HPP attacks include intense exercise, high-carbohydrate diet, cold, psychological stress, anxiety, epinephrine, excessive salt consumption, immobilization, intravenous steroid use, anesthesia, intensive care, and alcohol consumption [1].
In this case, hypokalemia attacks were observed in three different periods during the posttraumatic emergency department, orthopedic clinic, and intensive care unit (ICU) stay for pulmonary contusion. To our knowledge, this is the first case to report the follow-up and treatment process in the ICU. We present a case who was treated in the ICU after a traffic accident and operated on by an orthopedic surgeon. It is very important to be aware of this situation, which can be life-threatening, to avoid hypokalemia attacks and to manage the process well as a multidisciplinary team.
Case Presentation
A 19-year-old male patient was admitted to the emergency department with fractures of the right femur and left tibia after a traffic accident. He was diagnosed with familial hypokalemic periodic paralysis. Laboratory tests revealed a blood potassium level of 1.3 mmol/L. Within 6 hours, he was administered 100 mEq of potassium chloride. After this administration, the potassium level was 2.1 mmol/L at the 3rd hour, and after 6 hours, the potassium level was 4.1 mmol/L. No ECG changes or signs of respiratory failure were noted during follow-up in the emergency department. The patient was admitted to the orthopedic clinic at the 12th hour after arrival in the emergency department.
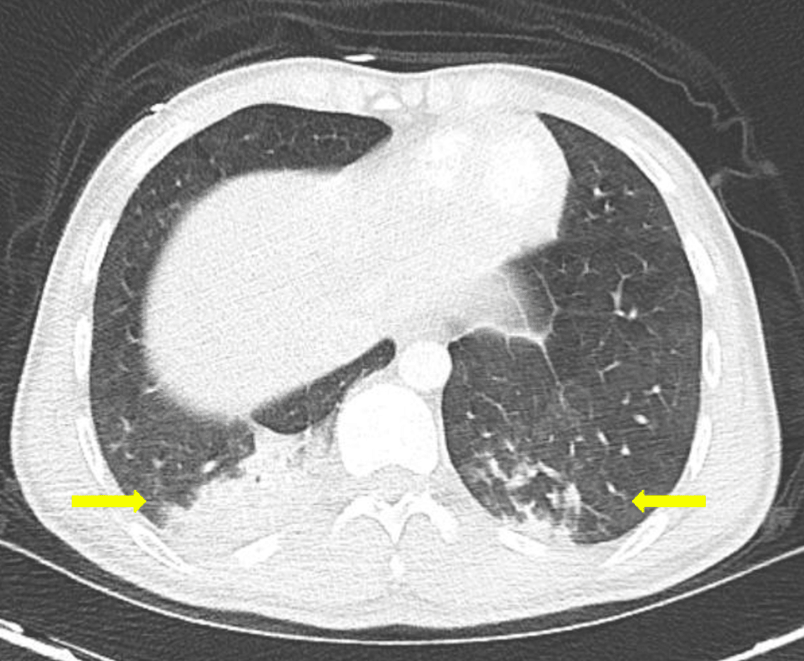
Respiratory failure developed within the 24th hour after admission to the orthopedic clinic. His blood potassium level was 3.1 mmol/L and PaO2 was 31.8 mmHg. He was immediately intubated and transferred to the intensive care unit. On the first day of follow-up in the ICU, no change in blood potassium level was detected. The patient's chest tomography showed atelectasis due to pulmonary contusion in both lungs, mainly in the right lung (Figure 1).
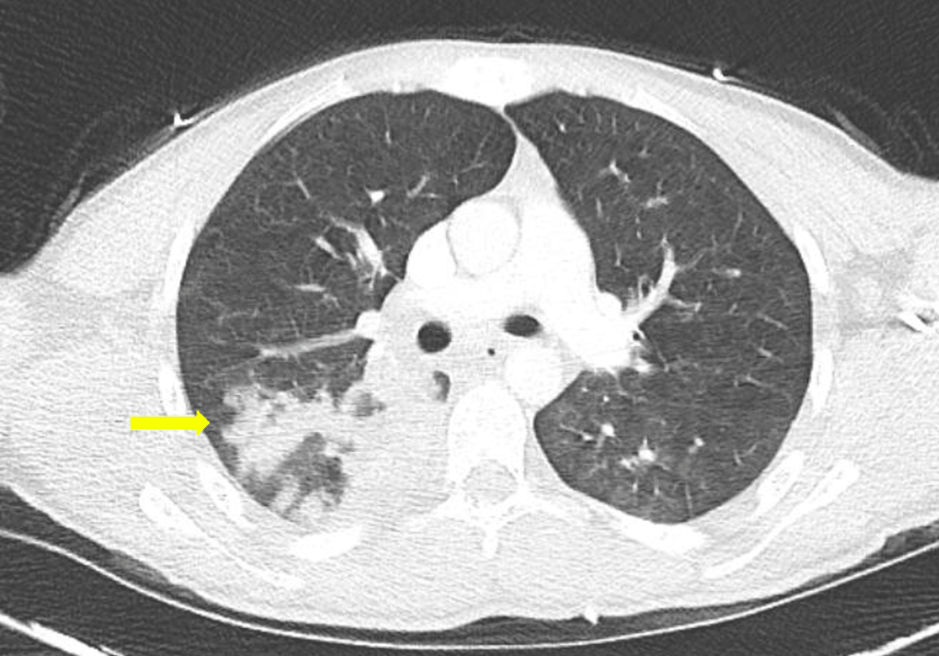
The patient was ventilated with a recruitment maneuver. The patient with control thorax CT showed improvement of atelectasis at the 24th hour after the recruitment maneuver (Figure 2).
Blood gas analysis showed improvement in oxygenation. His thyroid hormone levels were: TSH: 6.63 mIU/L (NR: 0.35 - 5.50), free T3(FT3): 1.87 pg/ml (NR: 2.3 - 4.2), free T4(FT4): 1.19 ng/dl (NR: 0.89 - 1.76). The patient, whose general condition was good and hemodynamically stable, underwent surgery for a femur fracture. In the 24th postoperative hour, the patient was hemodynamically stable and there were no problems with oxygenation. Physical examination revealed muscle weakness in bilateral upper extremities. In pressure support mode, he was breathing with low tidal volumes. A blood test revealed a potassium level of 1.3 mmol/l, after which 100 meq of potassium was administered intravenously over 6 hours. Potassium replacement was also administered twice daily via a nasogastric tube. After 24 hours, the potassium level was 3.9 mmol/L, he was awake, muscle strength was normal, and blood gas levels were within the normal range. The patient was extubated and transferred to the orthopedic clinic after 24 hours of close monitoring.
Discussion
HPP is a syndrome characterised by paralysis of the entire skeletal muscles due to a periodic drop in serum potassium levels. It commonly occurs between the ages of 20-30 years [1, 2]. The disease is caused by various gene mutations in sodium, potassium, and calcium channels in skeletal muscle [3, 4, 5]. It can also occur as a result of medications or adrenal disease. Triggers for hypokalemic attacks should be avoided, especially carbohydrate loads, stress and anxiety, cold temperatures, vigorous exercise, and beta-sympathomimetics [1, 4]. Care should be taken to avoid common triggers, long-term potassium supplementation, and carbonic anhydrase inhibitors such as acetazolamide and dichlorophenamide [4]. Hypokalemia may result from gastrointestinal and renal losses or from the entry of extracellular potassium into the cell. In the second case, hypokalemia is present but the total body potassium level is normal. The shift of extracellular potassium to the intracellular compartment can be observed in familial hypokalemic periodic paralysis, thyrotoxic periodic paralysis, barium toxicity, insulin excess, and alkalosis [1, 2, 6].
In this case, who had been diagnosed with familial HPP before the traffic accident, we observed three episodes of hypokalemia. The first episode occurred in the emergency department after trauma, the second episode occurred in the orthopaedic clinic, probably as a result of hypoxia, and the third episode occurred in the intensive care unit after orthopaedic surgery.
Close monitoring is required because malignant hyperthermia may develop under general anaesthesia, possibly in association with hypokalemic periodic paralysis [1, 7]. With regard to the induction of cardiac arrhythmias, caution should be exercised in hypokalemic periodic paralysis, and a basal ECG should be obtained. Agents such as epinephrine used for hypotension are well tolerated by some patients with HPP, whereas they cause hypokalemic attacks in others [1, 8]. In cases where a paralytic episode such as cardiac arrhythmias, respiratory distress, and dysphagia threatens life, IV should be treated urgently for potassium elevation. In the absence of these complications, oral potassium may be considered the first choice to reduce the risk of rebound hyperkalemia [8, 9].
Therefore, the level was first normalised with potassium infusions and then oral potassium treatment was continued to avoid possible complications [1, 8, 10]. An individualised treatment regimen with close monitoring of potassium levels is required.
This case shows that laboratory parameters revealed hypothyroidism when the patient was first admitted to the ICU. Some case reports have reported rhabdomyolysis in concomitant HPP and hypothyroidism [11, 12]. In our case, no rhabdomyolysis was detected.
Conclusions
Familial hypokalemic periodic paralysis is a rare disorder characterized by hypokalemia and muscle weakness. The coexistence of HPP and hypothyroidism is most commonly observed in Asians. No deaths associated with primary HPP have been reported in case reports published to date. If left untreated, it can lead to life-threatening conditions.
We evaluated our case as the first case with hypokalemic attacks, hypothyroidism, and muscle weakness during treatment in the intensive care unit as a result of trauma. We emphasize that this is a patient group that requires attention in the ICU in terms of early diagnosis and treatment of HPP attacks.
References
- Weber, F., & Lehmann-Horn, F. (2002). Hypokalemic Periodic Paralysis. In M. P. Adam (Eds.) et. al., GeneReviews®. University of Washington, Seattle.
View at Publisher | View at Google Scholar - Ahlawat, S. K., & Sachdev, A. (1999). Hypokalaemic paralysis. Postgraduate medical journal, 75(882), 193–197.
View at Publisher | View at Google Scholar - Fontaine, B., Trofatter, J., Rouleau, G. A., Khurana, T. S., Haines, J., Brown, R., & Gusella, J. F. (1991). Different gene loci for hyperkalemic and hypokalemic periodic paralysis. Neuromuscular disorders : NMD, 1(4), 235–238.
View at Publisher | View at Google Scholar - Latorre R, Purroy F. [Hypokalemic periodic paralysis: a systematic review of published case reports]. Revista de Neurologia. 2020 Nov;71(9):317-325.
View at Publisher | View at Google Scholar - Lin, S. H., Lin, Y. F., Chen, D. T., Chu, P., Hsu, C. W., & Halperin, M. L. (2004). Laboratory tests to determine the cause of hypokalemia and paralysis. Archives of internal medicine, 164(14), 1561–1566.
View at Publisher | View at Google Scholar - Gennari F. J. (1998). Hypokalemia. The New England journal of medicine, 339(7), 451–458.
View at Publisher | View at Google Scholar - Venance, S. L., Cannon, S. C., Fialho, D., Fontaine, B., Hanna, M. G., Ptacek, L. J., Tristani-Firouzi, M., Tawil, R., Griggs, R. C., & CINCH investigators (2006). The primary periodic paralyses: diagnosis, pathogenesis and treatment. Brain : a journal of neurology, 129(Pt 1), 8–17.
View at Publisher | View at Google Scholar - Levitt J. O. (2014). “Correction: Practical aspects in the management of hypokalemic periodic paralysis”. Journal of Translational Medicine, 12, 198.
View at Publisher | View at Google Scholar - Asmar, A., Mohandas, R., & Wingo, C. S. (2012). A physiologic-based approach to the treatment of a patient with hypokalemia. American journal of kidney diseases : the official journal of the National Kidney Foundation, 60(3), 492–497.
View at Publisher | View at Google Scholar - Veltri, K. T., & Mason, C. (2015). Medication-induced hypokalemia. P & T : a peer-reviewed journal for formulary management, 40(3), 185–190.
View at Publisher | View at Google Scholar - Meregildo-Rodríguez, E. D., & Failoc-Rojas, V. E. (2018). Case Report: Recurrent hypokalemic periodic paralysis associated with distal renal tubular acidosis (type 1) and hypothyroidism secondary to Hashimoto's thyroiditis. F1000Research, 7, 1154.
View at Publisher | View at Google Scholar - Kadeeja, N., Senthilnathan, N., Viswanathan, S., & Aghoram, R. (2017). Sporadic hypothyroidism-related hypokalemic paralysis: Diagnosis in a resource-poor setting. Journal of family medicine and primary care, 6(4), 862–864.
View at Publisher | View at Google Scholar
