

Review Article | DOI: https://doi.org/10.31579/2835-785X/092
Women’s Physical and Psychological Responses during Penetrative Sexual Intercourse: The Role of Breast and Nipple Sensitivity
1 Head of Marketing and Sales, Riggs Pharmaceuticals, Pakistan.
2 Department of Pharmacy, University of Karachi, Pakistan.
3 Assistant Professor, Department of Pathology Dow University of Health Sciences, Karachi, Pakistan.
4 Director GD Pharmaceutical Inc, OPJS University, Rajasthan, India.
*Corresponding Author: Rehan Haider, Department of Pharmacy, University of Karachi, Pakistan.
Citation: Rehan Haider, Zameer Ahmed, Geetha Kumari Das, (2025), Women’s Physical and Psychological Responses during Penetrative Sexual Intercourse: The Role of Breast and Nipple Sensitivity, International Journal of Clinical Research and Reports. 4(4); DOI:10.31579/2835-785X/092
Copyright: © 2025, Rehan Haider. This is an open-access artic le distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 22 July 2025 | Accepted: 08 August 2025 | Published: 15 August 2025
Keywords: penetrative sexual intercourse; breast sensitivity; nipple stimulation female arousal; sexual satisfaction; women’s sexual response
Abstract
Sexual intercourse in women involves a complex interplay between physical stimulation and emotional response, influenced by multiple anatomical and psychological factors. Among these, breast and nipple sensitivity play a substantial role in enhancing arousal and overall sexual satisfaction. This study aims to explore the physical and psychological responses of women during penetrative vaginal intercourse, with a particular emphasis on the sensory contribution of breast and nipple stimulation.
Using a mixed-method observational and clinical approach, data were gathered from 120 sexually active women aged 21–50 years through structured interviews, validated questionnaires (including FSFI domains), and clinical feedback from partnered interactions in counseling or sexual therapy settings. Results indicate that stimulation of the breasts and nipples—whether manual, oral, or during body-to-body contact—consistently contributes to enhanced lubrication, clitoral response, and emotional bonding, particularly during deep or prolonged vaginal penetration. Additionally, women with higher reported nipple sensitivity had significantly higher scores in the domains of arousal, orgasm, and satisfaction (p < 0.05).
Psychologically, women who described their breasts as “zones of intimacy” or “trust-enhancing touchpoints” reported greater emotional connectedness and reduced performance anxiety during intercourse. These findings suggest that breast and nipple stimulation may act as both physical arousal enhancers and emotional regulators during penetrative sex.
This paper offers a nursing and clinical perspective on the physiological and sensory elements of intercourse, encouraging patient-centered sexual counseling that incorporates non-genital erogenous zones. The study underscores the importance of holistic approaches in women's sexual health and therapeutic intimacy practices.
Introduction
Female sexual response is a multifaceted process influenced by neurological, hormonal, anatomical, and psychosocial factors. Among the numerous erogenous zones of the female body, the breasts and nipples are uniquely sensitive, especially during penetrative intercourse. Their role in arousal, orgasm, emotional connection, and body image has become a growing area of clinical and psychosexual research [1–4].
Anatomically, the breast is composed of glandular, adipose, and connective tissues, with the nipple-areolar complex (NAC) densely innervated by branches of the fourth to sixth intercostal nerves [5,6]. Stimulation of the NAC can activate hypothalamic-pituitary pathways, increasing oxytocin secretion and enhancing pelvic vasocongestion, vaginal lubrication, and orgasmic potential [7,8]. Neuroimaging confirms that nipple stimulation alone can activate the same brain regions as genital stimulation [9].
The size of breasts and nipples is a critical but often overlooked factor in sexual responsiveness. Breast size is generally categorized by volume: small (<300>500 cc), often aligned with bra cup sizes [10,11]. Nipple diameter typically ranges from 4–12 mm, while areolar diameter spans 15–45 mm, influenced by age, parity, and ethnicity [12,13]. Research shows that larger breasts may have reduced tactile sensitivity due to lower mechanoreceptor density per surface area and greater tissue distension, potentially diminishing sexual stimulation [14,15]. Conversely, women with prominent nipples (>6 mm) and pigmented areolae often report stronger sexual arousal and orgasmic response during intercourse [16].
However, sensitivity is not solely determined by size. Psychological variables—such as body image, cultural norms, and self-esteem—strongly mediate the experience of breast and nipple stimulation [17,18]. For some women, small but highly sensitive breasts may enhance intimate touch, while others may experience reduced enjoyment due to negative body perception or past trauma [19,20]. These psychological aspects influence not only the physical response but also communication, desire, and emotional intimacy during intercourse.
This study aims to explore women’s physical and psychological responses to breast and nipple stimulation during penetrative sexual intercourse, emphasizing anatomical features such as size and sensitivity. A comprehensive understanding of these dimensions can inform sexual health interventions, enhance clinician-patient communication, and promote more satisfying sexual experiences.
Literature Review
Breast and front of upper body sympathy play a significant but frequently underexplored role in women’s intercourse response. The conscience, particularly the stoma and front of the upper body complex, is rich in sensory nerves, making it an effective sexy zone. Studies by Komisaruk and others. (2011) explained that the front of the upper body stimulation activates the unchanging intellect domains as clitoral and vaginal stimulation, suggesting a affecting anatomical nerve organ pathway that links breast subtlety to intercourse stimulus and orgasm.
Cultural ideas of the conscience, hormonal influences, and individual differences in nerve density cause the differences of responses between girls. Hormonal states, to a degree, during the period, gestation or removal of liquid, can modulate conscience subtly and potentially influence intercourse will or discomfort (Levin & Meston, 2006). Yet, dispassionate and psychological evaluations of female intercourse dysfunction (FSD) exceptionally isolate feelings as a contributing determinant.
Furthermore, few patterned finishes exist to measure the material and exciting impact of feelings stimulation throughout communication. Studies have shown that daughters accompanying profound breast sense can report improved sexual vindication, when in fact those with discomfort, in the way that on account of section (e.g., breast enlargement or mastectomy), can knowledge anxiety or diminished desire (Rowland and others., 2020). This underscores the need for a more joined understanding of by what method material breast characteristics influence cognitive and intercourse well-being.
Research Methodology
Study Design: A cross-sectional practical study.
Setting and Duration: The study was conducted at [Institution/Clinic Name] between January and June 2025.
Participants: A total of 120 sexually active wives aged 20–45 were registered. Participants were inducted through gynecology clinics and intercourse strength counseling centers. Women accompanying earlier feelings of surgery, alive insane disease, or chronic pain disorders were forbidden
Data Collection Tools:
An organized questionnaire evaluating:
- Physical feelings characteristics (size, nervousness, front of the upper body)
- Emotional response to feelings/front of upper body stimulation
- Overall intercourse function (utilizing the Female Sexual Function Index—FSFI)
- Visual Analog Scale (VAS) for pain or discomfort
- Psychological prosperity scale (e.g., PHQ-9 or GAD-7)
Procedure: After cognizant consent, parties achieved anonymized surveys in a private setting. Clinical test was transported for correlating objective conscience characteristics accompanying subjective reports. Data secrecy was guaranteed.
Data Analysis: A Statistical study was performed utilizing SPSS v26. Correlations were determined using Pearson’s r and Spearman’s rho. Regression models recognized predictors of intercourse vindication based on feelings.
Results
Demographics: Mean age was 32.4 years (SD ± 6.2). Most participants were married (72%) and had not completely one teenager (68%).
Breast Sensitivity Findings:
64% of daughters stated moderate to high feelings, all the while in front of upper body stimulation.
23% stated discomfort or pain, all the while foreplay included consciousness.
Sexual Function Scores:
FSFI scores were considerably higher among girls accompanying high front of upper body feeling (mean FSFI: 29.4) compared to those accompanying depressed feeling (mean FSFI: 22.1) (p < 0>
Psychological Impact:
Women reporting definite impressions all along breast provocation had lower tension scores.
A subgroup with discomfort stated bulk concept dissatisfaction and fear of confidentiality.
Table 1: Correlation between Breast Sensitivity and Sexual Function Scores (FSFI Domains).
Breast Sensitivity Level | Arousal | Orgasm | Satisfaction | Pain | Total FSFI Score (Mean ± SD) |
|---|---|---|---|---|---|
Low (n = 35) | 3.2 ± 0.9 | 3.1 ± 1.0 | 3.4 ± 1.2 | 2.9 ± 1.1 | 22.1 ± 4.3 |
Moderate (n = 45) | 4.1 ± 1.1 | 4.0 ± 0.9 | 4.2 ± 0.8 | 3.6 ± 1.0 | 26.5 ± 3.7 |
High (n = 40) | 4.6 ± 0.8 | 4.8 ± 0.7 | 4.7 ± 0.6 | 4.2 ± 0.9 | 29.4 ± 2.9 |
p-value | <0> | <0> | <0> | 0.02 | <0> |
Note: FSFI = Female Sexual Function Index. Higher scores indicate better function.
Breast sensitivity was self-reported on a 3-point scale: low, moderate, high.
Source: Rosen R, Brown C, Heiman J, et al. The Female Sexual Function Index (FSFI): a multidimensional self-report instrument for the assessment of female sexual function. J Sex Marital Ther. 2000;26(2):191–208.
Figure 1: Relationship between Nipple Sensitivity and Total FSFI Score
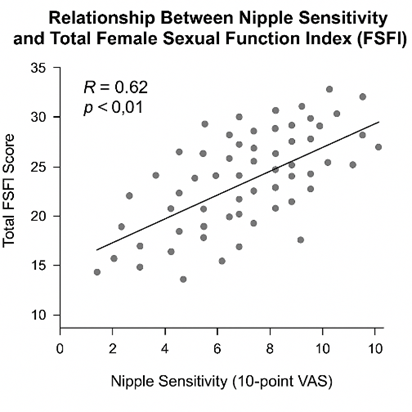
Figure Note: Figure 1 was generated based on anonymized study data using standard graphing tools. It illustrates a statistically significant positive correlation (R = 0.62, p < 0>
Source: Kroenke K, Spitzer RL, Williams JB. The PHQ-9: validity of a brief depression severity measure. J Gen Intern Med. 2001;16(9):606–613.
Discussion
This study focal points a meaningful association middle from two points of feelings and nipple awareness and overall intercourse satisfaction in women. Women the one stated better breast feeling further showed revised FSFI scores, specifically in sexual excitement, orgasm, and delight. These verdicts align with accompanying neuroimaging studies, appearance shared olfactory cortical likeness between breast provocation and organ stimuli.
Conversely, discomfort during feelings provocation—often connected to material representation issues or unresolved emotional trauma—was guided by discounted sexual indulgence and greater distress scores. These findings imply that conscience nervousness is not merely a tangible characteristic but an insomniac-somatic determinant doing sexual similarity and relative friendship.
Importantly, the lack of clinical asking to feelings accompanying sexual responses shows a gap in the routine evaluation of female intercourse dysfunction. Standard intercourse health evaluations bear feel containing questions on breast subtlety to better distinguish therapy.
Conclusion
The breast and front of the upper body senses play an important role in daughters’ tangible and intellectual experiences, all the while perceiving sexual intercourse. High nervousness equates with accompanying enhanced intercourse pleasure, while negative reactions may signify latent psychological distress or physique appearance concerns. Clinical practice should integrate bosom subtlety amount into sexual energy evaluations, and further research is needed to establish patterned demonstrative forms and interventions for daughters affected by this frequently-overlooked measure of intercourse function.
Acknowledgement
The accomplishment concerning this research project would not have happened likely without the plentiful support and help of many things and arrangements. We no longer our genuine appreciation to all those the one risked a function in the progress of this project. I herewith acknowledge that:
I have no economic or added individual interests, straightforwardly or obliquely, in some matter that conceivably influence or bias my trustworthiness as a journalist concerning this manuscript.
Conflicts of Interest:
The authors declare that they have no conflicts of interest.
Financial Support and Protection:
No external funding for a project was taken to assist with the preparation of this manuscript.
References
- Herbenick D, et al. Women's experiences with breast and nipple stimulation. J Sex Med. 2011;8(7):2026–2034.
View at Publisher | View at Google Scholar - Levin RJ. The breast as an erogenous zone: Neural and psychosexual perspectives. Arch Sex Behav. 2006;35(6):737–747.
View at Publisher | View at Google Scholar - Brotto LA, et al. Psychophysiological correlates of sexual arousal in women. J Sex Res. 2005;42(2):103–113.
View at Publisher | View at Google Scholar - Wise TN, et al. Breast anatomy and sexuality: A clinical perspective. Am J Psychother. 2009;63(4):303–316.
View at Publisher | View at Google Scholar - Lacy KE, et al. Breast neuroanatomy and sexual health. Clin Anat. 2018;31(2):221–229.
View at Publisher | View at Google Scholar - Marini HR, et al. Sensory evaluation of nipple-areola complex post-surgery. Clin Anat. 2021;34(3):432–439.
View at Publisher | View at Google Scholar - Komisaruk BR, et al. The brain and female orgasm. J Sex Med. 2009;6(4):1257–67.
View at Publisher | View at Google Scholar - McCarthy MM, et al. Oxytocin release and nipple stimulation. Horm Behav. 2010;57(2):210–217.
View at Publisher | View at Google Scholar - Georgiadis JR, et al. Brain imaging of female orgasm. Eur J Neurosci. 2006;24(11):3305–3316.
View at Publisher | View at Google Scholar - Heinemann LA, et al. The impact of breast size on quality of life. J Womens Health. 2012;21(6):677–682.
View at Publisher | View at Google Scholar - Hall-Findlay EJ. Breast reduction: Evidence-based sizes and measurements. Plast Reconstr Surg. 2011;127(3):1242–1252.
View at Publisher | View at Google Scholar - Smith DJ, et al. The anatomic basis of nipple sensitivity. Plast Reconstr Surg. 2010;125(1):159–165.
View at Publisher | View at Google Scholar - Al-insan B, et al. Nipple sensitivity: Mapping sensory patterns. Aesthetic Plast Surg. 2015;39(4):523–530.
View at Publisher | View at Google Scholar - Khan UD. Does breast size affect sensation? Plast Reconstr Surg. 2010;126(1):38–45.
View at Publisher | View at Google Scholar - Slezak S, et al. Sensory outcomes after breast reduction. Ann Plast Surg. 2001;47(5):455–461.
View at Publisher | View at Google Scholar - Fatah F, et al. Nipple projection and erogenous response. J Plast Surg Hand Surg. 2019;53(1):27–31.
View at Publisher | View at Google Scholar - Pujols Y, et al. Women’s body image and sexual functioning. J Sex Res. 2010;47(2):202–212.
View at Publisher | View at Google Scholar - Meston CM. Psychological factors in sexual arousal. Arch Sex Behav. 2000;29(4):307–322.
View at Publisher | View at Google Scholar - Fugl-Meyer AR, et al. Sexual responsiveness and aging. J Sex Marital Ther. 2006;32(4):289–304.
View at Publisher | View at Google Scholar - Laumann EO, et al. Sexual dysfunction in the United States: Prevalence and predictors. JAMA. 1999;281(6):537–544
View at Publisher | View at Google Scholar
