

Research Article | DOI: https://doi.org/10.31579/2834-5177/048
Use of Generative AI for Health Among Urban Youth in Pakistan: A Mixed-Methods Study
- Ahsan Mashhood *
- Aamna Ahmed
- , Inaya Khan
- Maryam Hashim
- Sara Baloch
Department of Medical Laboratory Techniques, Eldivan Vocational School of Health Services, Çankırı Karatekin University, Çankırı, Turkey.
*Corresponding Author: Ahsan Mashhood, Department of Medical Laboratory Techniques, Eldivan Vocational School of Health Services, Çankırı Karatekin University, Çankırı, Turkey.
Citation: Ahsan Mashhood, Aamna Ahmed, Inaya Khan, Maryam Hashim, Sara Baloch, (2025), Use of Generative AI for Health Among Urban Youth in Pakistan: A Mixed-Methods Study, International Journal of Clinical Infectious Diseases, 4(5); DOI:10.31579/2834-5177/048
Copyright: © 2025, Ahsan Mashhood. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 06 October 2025 | Accepted: 16 October 2025 | Published: 28 October 2025
Keywords: chatgpt; generative artificial intelligence; public health; ypar (youth participatory action research)
Abstract
Abstract
GAI tools are increasingly used informally for health, yet evidence from low- and middle-income countries (LMICs) is limited. This study generates early evidence on such health systems from the fifth most populous country: Pakistan.
Methods:
We used a youth-led convergent mixed-methods design among digitally connected urban youth in Pakistan (survey N=1240, 20 interviews). The primary outcome was any GAI use for health. We fitted multivariable logistic regression models and conducted reflexive thematic analysis.
Findings:
Overall, 69.0% of participants reported using GAI for health. Higher odds of use were observed among women (aOR = 1.57, 95% CI [1.17–2.11], p = 0.003) and youth reporting any mental or physical condition (aOR = 1.82, 95% CI [1.34–2.48], p < .001). Greater trust in AI strongly predicted use (per-level aOR = 4.21, 95% CI [2.98–6.01], p < .001). High confidence using AI (aOR = 1.81, 95% CI [1.11–3.07], p = 0.022), awareness of AI risks (aOR = 1.67, 95% CI [1.20–2.31], p = 0.002), and prior use of other (non-generative) digital health tools (aOR = 4.48, 95% CI [2.59–8.23], p < .001) were also associated with higher likelihood of use. Telemedicine use was significant though weaker in magnitude (aOR = 1.58, 95% 1.01–2.54 p = 0.049)
Interviews highlighted three themes: (1) access and affordability driving first-line use; (2) emotional safety and informational support, especially for stigmatized concerns; and (3) perceived empowerment in interpreting tests, organizing symptoms, and preparing for clinical visits.
Conclusion: Given constrained, stigmatizing, and costly services, GAI may function as an adjunct “first step” for youth health information and emotional support in Pakistan’s health ecosystem.
1.Introduction
In recent years, generative artificial intelligence (GAI) tools such as ChatGPT, Gemini (Bard) and Claude have rapidly entered the everyday lives of digitally connected youth (Renjith et al., 2024; Schaaff et al., 2025). These tools offer an unprecedented form of real-time, anonymous, and conversational information delivery, which distinguishes them from earlier digital health technologies such as search engines, static health websites, and scripted rule-based chatbots. While recent debates around GAI have largely centered on misinformation, copyright, and productivity (Simon et al., 2023; Blease et al., 2024), surprisingly little is known about how these tools are being used informally for health-seeking, particularly in the Global South (Siddals et al., 2024; Das & Muschert, 2024), where youth often face stigma, limited access to health services, and structural barriers to care (Khan et al., 2023; Choudhry et al., 2023; Mubeen et al., 2024; Mashhood et al., 2025). Accordingly, this paper contributes: (i) early evidence from a large-sample LMIC estimate of youth GAI health use; (ii) a theory-linked account (socio-ecological) of who uses GAI and why; (iii) policy, practice, and systems implications for integrating GAI in youth health, especially in the LMIC context.
In Pakistan, a country with a median age of 21 (United Nations, 2024) and socio-cultural constraints around health disclosure (Husain et al., 2020; Rashid et al., 2025), these tools may be forming an infrastructure of self-directed care by offering nonjudgmental, always-available alternatives to a relatively dysfunctional healthcare system (Khan et al., 2023; Mubeen et al., 2024). A deluge of local social media content suggests that young people may be turning to GAI for advice related to anxiety, sexual health, acne, fitness, nutrition, and other concerns they may feel uncomfortable discussing with parents or doctors. However, this remains an understudied phenomenon. Little to no research efforts have comprehensively explored how young people in Pakistan (or the Global South) are using and appropriating unregulated GAI tools to meet their health needs, nor how individual, relational or community factors interact to shape this behavior. Existing research, mostly from the Global North, investigates specific regulated Chatbots like Woebot (Fitzpatrick et al., 2017) or Replika (Maples et al., 2024) instead of GAI tools like ChatGPT that young people are already using (e.g., for education) or at least increasingly familiar with (see Supplement 1).
1.1 Theoretical Framework
To examine this emerging phenomenon, we draw on the socio-ecological model as our guiding theoretical framework, particularly its adaptation by Mansfield and colleagues (2022). This model conceptualizes health behaviors as the outcome of dynamic interactions between (1) individual (e.g., demographic), (2) relational (e.g., interpersonal) and, (3) community factors (Figure 1). These are critical to understanding the Pakistani context. Accordingly, extending this framework to the context of GAI health use, we consider how individual demographics (gender, socio-economic class, sexual orientation, pre-existing conditions etc.) intersect with interpersonal dynamics (e.g., perceived social support; friends and family), and community structures (e.g., healthcare access), to shape how and why young people turn to GAI for health information and potentially, decision-making. In doing so, we explore health-seeking via GAI as an emergent response, worth timely exploration in Pakistan’s layered and often exclusionary health ecosystem (Ali & Rais, 2021).
By collecting primary data on digitally connected urban youth aged 18–30 in Pakistan, this study investigates the prevalence, predictors and perceptions associated with GAI use for health purposes. Simply put, we center youth and use socio-ecological theory to examine who is using GAI for health and why, to discuss implications for social policy, health literacy, and the ethical governance of GAI systems. In doing so, we contribute new empirical evidence to this nascent subfield of digital public health, while also raising critical questions about the big picture i.e., what constitutes care in this new era of algorithmic therapeutic alliance and the ethics of potential ‘task shifting’ via GAI.
2. Methods
Given the fundamentally exploratory nature of this study, we employ a convergent mixed methods design (Creswell & Plano Clark, 2017) to investigate how digitally connected urban youth in Pakistan repurpose GAI tools for health-related queries. This approach integrates a quantitative survey to establish patterns and predictors of GAI use with qualitative interviews to explore the motivations, perceptions, and experiences. We draw particular inspiration from socio-ecological youth health research from Mansfield and colleagues (2022). A pre-analysis plan for the quantitative analysis was registered at AsPredicted, #236264 (Wharton Credibility Lab). We used the GRAMMS Checklist (O’Cathain et al., 2008) to ensure transparency, rigor and replicability (see Supplement 3)
2.1 Quantitative Survey
The cross-sectional survey was developed through a multi-stage, iterative process informed by formative research, cgnitive testing, pilot feedback, and a review of gray literature on digital health-seeking behaviors in LMICs. Care was taken to ensure that the survey was culturally appropriate, youth-centered, and mobile-optimized.
To minimize drop-offs and respondent fatigue, the final survey was limited to a median completion time of three minutes (see Supplement 2 for items). Key variables included demographics (age, gender, education board, sexual orientation), social support, healthcare avoidance, existing physical or mental health conditions, previous use of non-GAI health tools, trust in AI, confidence using AI, and awareness of AI risks. These were entered as predictors in multivariable logistic regression models assessing likelihood of GAI use for health. Bivariate associations (e.g., between gender and specific health-related queries) were tested using chi-square tests; model fit was assessed using McFadden’s R², and multicollinearity was checked via generalized variance inflation factors (GVIF).
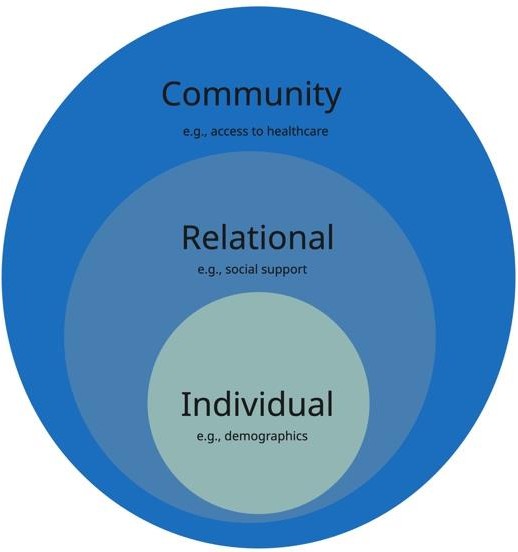
Figure 1: Socio-ecological Model (Mansfield et al., 2022; CDC, 2022)
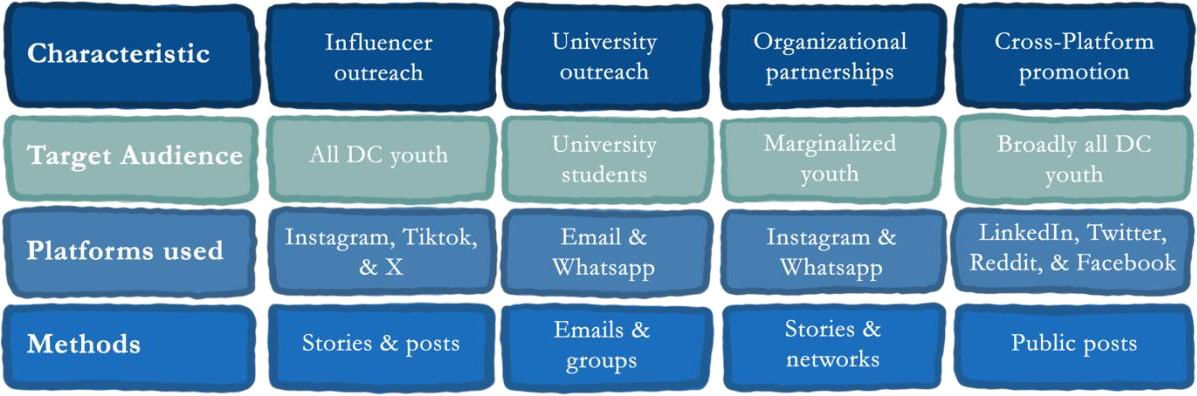
Figure 2: Quantitative Survey Dissemination Strategy
2.2 Qualitative Interviews:
To complement the quantitative insights and gain richer data about youth GAI experiences, we conducted parallel semi-structured in-depth interviews with a diverse subset of participants (n = 20). The interview guide covered user motivations, trust in AI, the perceived role of AI in help-seeking journeys, and comparisons with peer, familial, or professional support systems. This interview guide was also informed by the same steps that helped create the quantitative survey.
Interviewees were selected via social media i.e., individuals that responded to story and post requests and defined themselves as routine users of GAI for health. Interviews were conducted in June and July 2025, virtually, to ensure geographic accessibility and participant comfort. Recordings were transcribed verbatim via Turboscribe and analyzed using reflexive thematic analysis, guided by Braun and Clarke’s six-phase approach (2006). The analytic process was iterative and inductive, with codes developed collaboratively by the research team and continuously refined to capture patterns across participant narratives. Emphasis was placed on preserving participant voice, especially in relation to agency, stigma, and lived experience concerning health and GAI.
.3 Convergent Design
Our convergent mixed-methods design was pre-specified and guided by GRAMMS, with concurrent timing and equal weighting of quantitative and qualitative components. Integration was embedded a priori across stages e.g., formative qualitative work and a targeted literature review informed construct selection and item wording for both the survey and interview guide while cognitive testing and a pilot survey fed back to refine qualitative sampling criteria, interview guides and prompts. Furthermore, throughout data collection, we used joint displays and narrative weaving during weekly team presentations to assess convergence, divergence, and other signals.
2.4 Ethical Considerations
The study received ethics approval from the Ethics Review Committee at Habib University, Karachi (HU-ERC-2025-AM1, March 2025). Furthermore, a trained and licensed Clinical Psychologist and Public Health Specialist (ScD) reviewed all survey items to ensure low risk and maximum possible construct validity. Informed consent was obtained digitally from all participants. No meaningful identifying information was collected in the survey, and all interview transcripts were anonymized. Participants were informed of their right to withdraw at any time without consequence.
2.5 Reflexivity & Youth-Led Research Approach
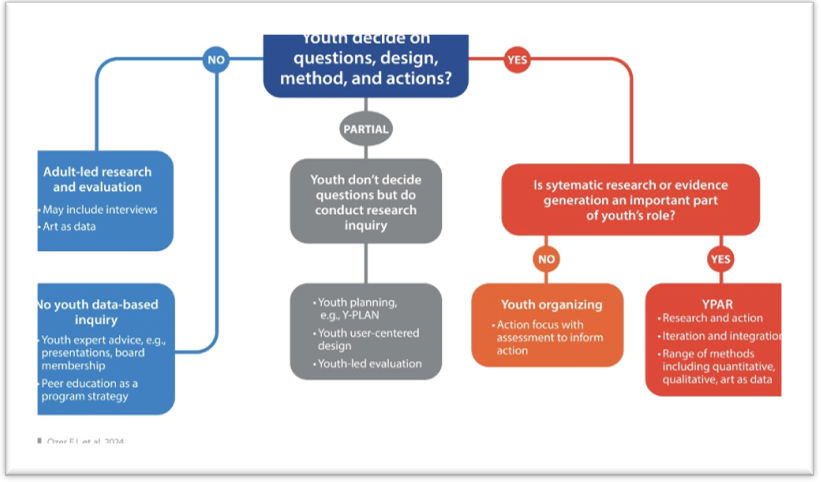
This study was designed and implemented entirely by young Pakistanis aged 20–30 based in Habib University, in line with a youth-led participatory action research (YPAR) framework (Ozer et al., 2024). Such a research approach stands in contrast to traditional YPAR models that involve adult facilitation which are most common in Pakistan. This project was horizontally structured, with no older adult oversight besides receiving funding and IRB approval. Accordingly, youth researchers led all stages of the process, including (1) identifying research questions, (2) designing tools, (3) collecting data, (4) analyzing data, and (5) deciding how to best disseminate findings, as part of our commitment to epistemic justice and power-sharing (Ozer et al., 2024, pp. 402–406).
To support research integrity and reflexivity, the team maintained a shared log documenting decision- making, dilemmas, and shifts in perspective. This reflexive infrastructure was a joint effort and was particularly important given the nature of the topic: youth health in Pakistan. Drawing on calls for stronger youth-centered accountability mechanisms (p. 414), we integrated regular peer check-ins and iterative revisions to our instruments and digital field strategy.
By centering youth as knowledge producers rather than subjects or informants, this study aligns itself with evidence that youth-led inquiry can strengthen research relevance, foster sociopolitical development, and enhance the translational impact of findings (Kim, 2016; Branquinho et al., 2020; Sellars et al., 2021; Igwe et al., 2022). In contexts where extractive research models dominate, especially in LMICs like Pakistan, this fully youth-led design offers an alternative model for ethical, locally grounded, and action-oriented public health scholarship
3. Results
3.1 Quantitative Results
1,305 individuals completed the survey. Out of these, 1,266 met the age criterion (18–30). Of these, 1,240 answered the primary outcome (analysis set). Table 1 shows the demographic breakdown; mostly using the age-eligible set (n=1,266); only the “Used GAI for health” row uses n=1,240. Missing data were minimal, with the highest around ~3% for sexual orientation.
4. Results
4.1 Quantitative Results
1,305 individuals completed the survey. Out of these, 1,266 met the age criterion (18–30). Of these, 1,240 answered the primary outcome (analysis set). Table 1 shows the demographic breakdown; mostly using the age-eligible set (n=1,266); only the “Used GAI for health” row uses n=1,240. Missing data were minimal, with the highest around ~3% for sexual orientation.
6. Results
6.1 Quantitative Results
1,305 individuals completed the survey. Out of these, 1,266 met the age criterion (18–30). Of these, 1,240 answered the primary outcome (analysis set). Table 1 shows the demographic breakdown; mostly using the age-eligible set (n=1,266); only the “Used GAI for health” row uses n=1,240. Missing data were minimal, with the highest around ~3% for sexual orientation.
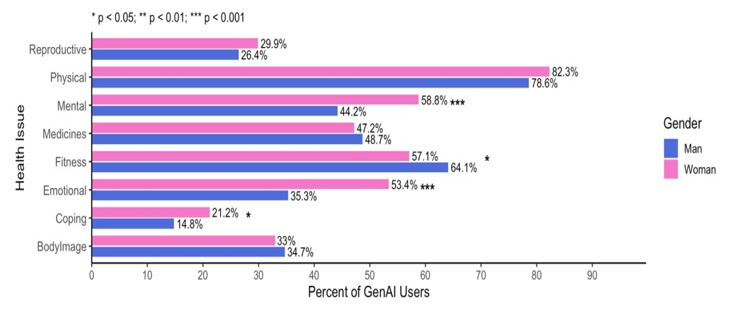
Overall, 69.0% (856/1,240) reported using GAI tools for health-related purposes, with ChatGPT being the most commonly used platform (96.1%, 820/853). The most frequent types of health-related queries were about physical symptoms (80.9%, 692/855), fitness or nutrition (59.9%, 512/855), and mental health (53.2%, 455/855). Key motivations included 24/7 availability (59.3%, 508/856), curiosity (52.8%, 452/856), and affordability (46.3%, 396/856). More than half of GAI users (57.6%, 491/853) reported feeling more comfortable asking sensitive health questions to AI than to a professional or doctor. Awareness of potential risks was also high: 72.0% (886/1,230) of all respondents acknowledged possible dangers associated with AI use in health. Among them, 84.5% (747/884) were concerned about receiving inaccurate or unsafe advice, 55.0% (486/884) about developing over-dependence, and 48.3% (427/884) about privacy issues. Perceived usefulness was also high: 56.5% (481/851) rated AI-generated responses as “somewhat helpful,” 39.2% (334/851) as “very helpful,” and 4.2% (36/851) as “unhelpful.”
| Variable | Category | n | pct |
| Age | Median: 22 [Q1: 20, Q3: 25] | ||
| Gender | Woman | 739 | 58.4 |
| Man | 519 | 41.0 | |
| Other | 8 | 0.6 | |
| Sexual Orientation | Heterosexual | 1,117 | 91.2 |
| LGBTQ+ | 98 | 8.0 | |
| Other | 10 | 0.8 | |
| Education Board | Local | 722 | 57.0 |
| International | 532 | 42.0 | |
| Other | 12 | 0.9 | |
| Close Friends | None | 87 | 6.9 |
| 1-2 | 439 | 34.7 | |
| 3-4 | 490 | 38.7 | |
| Variable | Category | n | pct |
| 5+ | 249 | 19.7 | |
| Comfort Discussing Health with Family | Yes | 442 | 35.0 |
| Sometimes | 470 | 37.2 | |
| No | 350 | 27.7 | |
| Existing Conditions | None | 661 | 52.4 |
| Mental health | 194 | 15.4 | |
| Physical health | 189 | 15.0 | |
|
| ||
| Both | 217 | 17.2 | |
| Non-GAI HealthTools | None | 920 | 72.7 |
| Telemedicine | 126 | 10.0 | |
| WhatsApp/SMS | 89 | 7.0 | |
| Chatbots | 41 | 3.2 | |
| Othercombinations | 90 | 7.1 | |
| Used GAI for health | Yes | 856 | 69.0 |
| No | 384 | 31.0 | |
| General generative AI use (any purpose) | Daily | 687 | 54.3 |
| A few times a week | 385 | 30.4 | |
| A few times a month | 73 | 5.8 | |
|
| ||
| Rarely | 95 | 7.5 | |
Never | 26 |
Table 1: Sample Demographic Characteristics
Note: significance levels are as follows; * p < 0>
6.2 Qualitative Results
We analyzed 20 in‑depth interviews with urban young adults aged 18–30 from across Pakistan. Participant pseudonyms are used to maintain anonymity. Consistent with reflexive thematic analysis, we judged the dataset to have adequate information power (Malterud et al., 2016) for our aims; later interviews added nuance rather than new themes Below, we present the overarching themes explaining why young people turn to GAI tools for health. We draw on the COREQ checklist for reporting. Our reflexive memo and peer debriefings routinely evaluated the 1) methodological limitations, 2) coherence across data, 3) adequacy of data and 4) relevance to the review question.
Participants consistently emphasized how barriers such as increasing costs, long waiting times, and limited availability of quality services pushed them to turn to GAI tools as a first-line resource. GAI (specifically, ChatGPT) was perceived as always accessible and “there for you” when health services were not. This was our most potent and consistent finding, across all interviews. suggested no evidence of multicollinearity, with all GVIF^(1/(2*Df)) ≤ 1.08.
Predictor | aOR CI | p_fmt |
| Woman (vs. Man) | 1.57 [1.17, 2.11] | 0.003 ** |
| LGBTQ+(vs. Heterosexual) | 0.59 [0.34, 1.05] | 0.068 |
| Other(vs. Heterosexual) | 2.61 [0.35, 53.47] | 0.410 |
| International board (vs. Local) | 1.12 [0.83, 1.51] | 0.455 |
| Otherboard (vs. Local) | 0.40 [0.07, 1.80] | 0.245 |
| Social support: High (vs. Low) | 0.91 [0.65, 1.29] | 0.601 |
| Any condition (Yes vs. No) | 1.82 [1.34, 2.48] | <.001 *** |
| Healthcare Delay: Never (vs. Often) | 0.62 [0.35, 1.10] | 0.102 |
| Healthcare Delay: Rarely (vs. Often) | 0.91 [0.62, 1.35] | 0.647 |
| Healthcare Delay: Sometimes (vs. Often) | 0.92 [0.63, 1.34] | 0.678 |
| Trustin AI (per level) | 4.21 [2.98, 6.01] | <.001 *** |
| Confidence: High (vs. Low) | 1.81 [1.11, 3.07] | 0.022 * |
| Aware (vs. Not aware) | 1.67 [1.20, 2.31] | 0.002 ** |
| Telemedicine user (vs. None) | 1.58 [1.01, 2.54] | 0.049 * |
| Other tooluser (vs. None) | 4.48 [2.59, 8.23] | <.001 *** |
Note: Significance: *** p < .001; ** p < .01; * p < .05. McFadden R² = 0.14. All GVIF^(1/(2*Df)) ≤ 1.08.
Table 2: Adjusted Odds Ratios for Regression Results
As Ayesha explained, “[...] therapy is definitely something that's available but at the same time it's not something that's available 24/7 [...] AI has been very helpful in that sense. At 3 AM, no therapist is available, but I have ChatGPT, for example, to kind of keep track of all my emotions.” This constant availability was important for participants who: 1) struggled to secure appointments, 2) could not afford consultations, and 3) had previously had adverse experiences with professionals.
As one key informant noted, “Usually in Pakistan [...] we go to hospitals when we're about to die . Because our health system is not that good [...] People are afraid to go to the doctor, who will bear the expenses?” (Junaid). This quote illustrates what many participants highlighted, i.e., that healthcare- seeking involved significant out-of-pocket expenditure, particularly in private facilities, leading them to either delay or avoid consultations altogether.
Zashe echoed the challenges of long waiting times in addition to cost: “Waiting times at hospitals are so long. ChatGPT provides immediate answers which is reassuring.” This immediacy allowed participants to triage their needs, self-manage minor issues, or decide whether in-person care was necessary. Mujahid summarized this sentiment: “Healthcare is costly and sickness is common [...] AI gives you some answers when going to the doctor isn’t possible.”
A second theme centered on the emotional safety and informational value that participants derived from GAI interactions, overwhelmingly with ChatGPT.
GAI tools were described as judgment-free, non-stigmatizing (“doctors here [in Pakistan] are very fatphobic”), and capable of providing sensitive and holistic explanations about health concerns that professionals in Pakistan were perceived to often lack the time or training (or both) to deliver. Several
participants described AI as a space where they could express sensitive issues such as sexual health, mental health, neurodivergence, or weight concerns,
without fear. One female participant noted, “AI can help with topics [...] like sexual health or weight issues where I have been shamed by doctors” (Samina). This sentiment was echoed by Aliza: “The stakes are obviously much lower. It's just AI. It's not like it's going to tell anyone” and others: “there's always this period, taking sessions, figuring out how secretly homophobic or slut-shamey my therapist is”.
Several participants also valued the absence of anxiety and nervousness that otherwise exists with human interaction, even for non sensitive issues e.g., ability to ask multiple questions without embarrassment or time constraints. As Mohib puts it: “With ChatGPT, there’s no fear of judgment like there is when sharing sensitive information with a therapist [...] I can ask the same question five different ways without feeling awkward or weird.”. Other respondents noted similarly: “Even if the responses are biased, sometimes it’s enough to give you closure [...] it gives some peace.”; “Sometimes I don’t want a solution. I ask, are my feelings valid?.”
Beyond emotional safety, GAI was also perceived as a rich source of information that participants struggled to access from healthcare professionals. “Doctors don’t really tell you what’s up [...] they’re busy and won’t engage with you that much. ChatGPT helps me understand my situation better.” Similarly, Saad described using AI to clarify medication information: “In Pakistan, doctors tend to be a bit cruel. They're not going to tell you everything [...] But ChatGPT told me exactly what the medicines were for and how to take them.”
Finally, participants described using GAI tools as a way to gain agency and greater control over their health-seeking journeys. They reported feeling more empowered to interpret medical content (e.g., ulcer reports), organize their concerns, and communicate more effectively with professionals.
Asad described how GAI helped him navigate complex test results: “I used GPT to interpret a tricky [name of scan and details redacted] report for my mother.” Similarly, Marij explained how GAI enabled him to frame health concerns for appointments: “AI even gives me the words to articulate my health issue to the doctor in a structured way, otherwise they just dismiss you for rambling.” Similarly, other key informants noted the following: “I trained my GPT to sympathize first or offer solutions later, depending on what I need”; “I use the same chat so it ‘remembers’ meds and side effects, it’s like a running log for my medications.”
Furthermore, this sense of empowerment extended beyond technical knowledge. Several participants described using GAI to track their symptoms, set health goals, and self-manage conditions. Ghazi explained: “I use ChatGPT to track medications, supplements, and side effects [...] I use it for calorie deficits and screen addiction; it gives me a roadmap.”
GAI tools also offered a more holistic perspective on health than participants perceived from doctors. As Marij observed: “AI takes a more holistic view… doctors in Pakistan mostly just focus on symptoms.” Participants particularly appreciated AI’s ability to link information across previous conversations (e.g., the memory feature that remembers information) and highlight overlooked patterns, which reinforced their sense of control and preparedness.
Overall, across themes, participants framed GAI tools as accessible, non-judgmental, and empowering complements to an overburdened healthcare system. For many, these platforms represented the only viable way to seek health-related information and emotional support without significant cost, stigma, or delay. Furthermore, while participants emphasized that GAI should not replace healthcare professionals, it was often the first point of contact for a variety of health related concerns. This was especially true for sensitive and stigmatized topics.
Discussion
This study provides one of the first large-sample LMIC estimates of youth engagement with GAI for health, showing that nearly 70% of urban Pakistani youth report use. Uptake was patterned by gender, pre-existing health conditions, and trust in AI. Our findings stand in sharp contrast to recent figures from high-income countries (HICs), where uptake remains far lower (e.g., 11% in the United States, Schaaff et al., 2025). While such cross-context comparisons are only illustrative, given differences in sampling and the infancy of this field, they still demonstrate the need and urgency to understand the distinctive structural and cultural drivers shaping adoption in LMICs. In the following discussion we 1) interpret findings through four interrelated themes, before turning to 2) methodological reflections, strengths and limitations, and implications for policy and practice.
4.1 Health Gaps, Stigma, and Compensatory Use
Youth living with pre-existing health conditions were twice as likely to use ChatGPT for health, showing how GAI may serve as a compensatory resource where formal services are absent and/or insufficient. Particularly notable were sociocultural constraints i.e., stigma surrounding sexual and mental health shaped both the content and nature of engagement, echoing prior work on health- seeking in Karachi (Mubeen et al., 2024). Women were especially likely to use GAI, consistent with research on higher baseline help-seeking among women (Liddon et al., 2018; Joshi, 2015), the influence of gender norms (de Visser et al., 2022; Rashid et al., 2025), and the scarcity of confidential, nonjudgmental services in Pakistan (Mashhood et al., 2025). Taken together, our findings highlight how GAI help-seeking may be, in many cases, a necessary workaround for deeply embedded structural and cultural barriers to care, especially in an LMIC context.
4.2 Emotional Safety and Affective Support
Another key theme was the emotional utility of GAI tools. Participants described ChatGPT as a supportive, anonymous presence that helped them
navigate late-night anxiety, relational conflict, and identity dilemmas. This mirrors emerging global research on GAI’s ambient mental health functions (Siddals et al., 2024; Hang et al., 2025), but is particularly notable in Pakistan’s context of stigma, silence, and familial surveillance (Husain et al., 2020; Khan et al., 2023). Some participants likened the tool to a “friend” or “therapist,” validating their concerns in a nonjudgmental tone. Others emphasized its value as a first step, something to consult before making decisions, particularly when human help felt inaccessible. These findings resonate with literature documenting how users treat AI- enabled tools as relational supports during periods of distress (Maples et al., 2024; Luo et al., 2025). Yet participants flagged risks: feelings of over-reliance, the lack of accountability, and concern about engaging too deeply with a non-human interlocutor (Kretzschmar et al, 2019). Such tensions present an important ethical and psychological consideration for public health actors in LMICs, where relational care is both scarce and overburdened (Main & Saleem, 2025).
4.3 Inequalities of Access and AI Literacy
While many participants engaged actively with ChatGPT, iteratively refining prompts to interpret lab results, understand diagnoses, prepare for clinical encounters, etc; such empowerment is unlikely to be evenly shared. Youth with stronger forms of cultural capital, such as English proficiency and prior digital confidence, were more likely to use and benefit from GAI: Interviewees described developing “AI literacy”: the ability to engineer prompts and critically evaluate outputs. Yet in Pakistan, where fewer than 2% of people pursue higher education and private, English-medium schooling remains a major class divide (Rahman et al., 2001), such skills, or the ability to build them quickly, are unequally distributed. This aligns with the concept of cultural health capital (Shim, 2010) and suggests that GAI may widen, rather than narrow, existing inequities.
Our attempt to capture socioeconomic status (SES) via educational board type (international vs. local) was informed by formative research but has limitations. While the education board reflects some classed dimensions of cultural capital, it may not comprehensively capture precarity linked to household insecurity or intergenerational wealth. Future youth-led work should experiment with and employ more holistic SES measures that better reflect the class divides in Pakistan.
4.4 Convenience, Personalization, and Cost
Participants repeatedly cited GAI’s immediacy, no/low cost, and user-friendly tone as critical factors enabling use. ChatGPT was preferred over Google because it was more conversational, less overwhelming, and available on demand. These findings showcase GAI platforms’ appeal as a responsive, low-barrier tool, especially in a context like Pakistan, where adolescent-friendly services are scarce and healthcare costs are prohibitively high (Khan et al., 2023; Mubeen et al., 2024). Frustrations with local healthcare were in line with expectations and literature (Hussain et al., 2019).
The ability to tailor prompts and receive personalized responses was described as empowering. However, participants also acknowledged the risk of “false confidence” i.e., being misled by GAI’s fluent style and apparent authority. Both the survey and interviews emphasized the importance of verifying GAI responses with human experts. This pragmatic approach, of treating ChatGPT as “a step up from Google” rather than a doctor, echoes recent calls for hybrid care models where informal tools augment formal systems instead of replacing them.
4.5 Ethical Awareness, Misinformation, and Climate Concerns
Despite high levels of engagement, participants demonstrated considerable awareness of GAI’s limitations. Risks cited included misinformation, culturally inappropriate advice, affirmation bias, and limited relevance for specific medical conditions. These concerns resonate with recent research cautioning against over-reliance on GAI tools in health decision-making (Mandal et al., 2025) and many of the risks pointed out were comparable to those of professionals (Blease, et al., 2019).
A surprising and rather unprompted theme was climate anxiety. Although our survey did not include climate concerns, participants used the open-ended “other concerns” field to express concerns about GAI highlighting a form of digital conscientiousness rarely captured in public health literature. Given Pakistan’s history, vulnerability to climate change, and the rise of climate-oriented youth movements, this finding merits further exploration in the LMIC context (Das & Muschert, 2024).
.6 Methodological Strengths & Reflexive Insights
We argue that this study’s methodological design is itself a key contribution in the context of LMIC YPAR research; for instance, the survey instrument was developed through rigorous formative research guided by socio-ecological theory, including cognitive testing to ensure clarity and brevity (≤3 minutes). Design choices were shaped by the constraints of balance: i.e., online youth data collection (ensuring minimal drop-off, higher N) and construct validity of survey-items, with all decisions deliberated up, tested, co-produced, within a resource-scarce setting.
Interestingly, the process also revealed structural barriers to youth participation e.g., the inclusion of a sexual orientation question, essential to public health equity, triggered backlash from some respondents and deterred participation from more conservative male social media influencers. Also, open-text in the survey responses included hostile remarks such as, “this is a muslim country,” illustrating the persistent stigma even within ‘elite’, urban youth spaces. We believe this may be among the first locally led surveys in Pakistan to include sexual orientation in a quantitative public health context, and we call for more ethical yet courageous efforts to ensure sexual and gender minority inclusion in future research (Purdam et al., 2008; Mustanski, 2011; Littlejohn et al., 2019).
4.7 Strengths & Limitations
We claim multiple strengths in this study, which include a pre-specified convergent mixed-methods design with equal weighting, youth-led design, which includes instrument development with cognitive testing/piloting, a relatively large analytic sample (N = 1,240), transparent reporting (pre-analysis plan, model fit, multicollinearity checks), and integration via joint displays that link adjusted odds ratios to interview themes. Perhaps most importantly, this is among the first and few studies that look into this topic (youth GAI use) using this epistemic approach (YPAR).
We also acknowledge several natural limitations, which include non-probability online recruitment (purposive/snowball), introducing potential sampling bias and restricting generalizability to rural Pakistan; an English-literate, digitally connected, largely urban sample that likely overestimates GAI exposure/competence (English/urban skew). While targeting digitally connected youth was intentional, to uncover trends in early adoption, and trickle-down, future research should expand our work and focus on more diverse youth populations. Furthermore, SES was proxied by the education board (imperfect), several constructs used single-item measures, as it had to be balanced with the very real concerns of survey fatigue, drop offs, and ensuring optimization for young people.
Taken together, our results should be read as descriptive evidence among digitally connected urban youth in Pakistan, while the mixed-methods integration and reflexive YPAR approach strengthen credibility and policy relevance. We hope that future researchers can build onto this evidence and also continue incorporating YPAR in the LMIC health context.
4.8 Policy and Practice Implications
Health systems must plan for the emerging reality that GAI is becoming a de facto first point of contact for many young people. To ensure that this use enhances rather than undermines wellbeing, our findings point to five
4.9 Conclusion
Using a theory-driven framework and youth-led design, we identify who uses GAI for health, how, and why. We show that GAI, such as ChatGPT, are functioning as stopgaps, emotional scaffolds, and health literacy aids in the absence of responsive formal care. Youth in Pakistan are turning to them not because they are ideal, but because they are available, affordable, and anonymous, reflecting both the potential and the peril of unregulated GAI in under-resourced settings. Our work hopes to raise critical questions about this new form of therapeutic alliance, augmented by GAI tools, and we call on public health systems and actors to consider this emergent phenomenon more seriously.
Interconnected policy and practice implications:
1. Integrate into digital health plans: Acknowledge youth GAI use in e/mHealth and track risks and opportunities with clear indicators.
2. Treat AI literacy as health literacy: Teach critical appraisal in schools and community programs (e.g., PMYP/Generation Unlimited).
3. Train providers in digital empathy: Equip frontline staff to respond nonjudgmentally to the needs driving GAI use and strengthen therapeutic alliances.
4. Set equity-first guardrails: Require cultural/linguistic inclusion and transparency; co-design with youth to reduce disparities.
5. Back youth-led research & advocacy: Recognize GAI as a structural determinant of health information-seeking and embed findings in national and WHO-aligned strategies.
Declaration of Interest:
The authors declare no conflicts of interest.
Patient and public involvement:
Youth were involved in all stages (question development, piloting, recruitment materials, interpretation, dissemination) consistent with a YPAR approach.
Role of the funder:
The funder had no role in study design, data collection, analysis, interpretation, or submission.
Generative AI Use
During the preparation of this work, the authors used GPT to improve word choice and debug coding errors. After using this tool and service, the authors reviewed and edited the content as needed and take full responsibility for the content of the publication.
References
- Ali, S. A. M., & Rais, R. B. (2021). Pakistan’s Health-Care System: A Case of Elite Capture. South Asia: Journal of South Asian Studies, 44(6), 1206-1228.
View at Publisher | View at Google Scholar - Blease, C. R., Locher, C., Gaab, J., Hägglund, M., & Mandl, K. D. (2024). Generative artificial intelligence in primary care: An online survey of UK general practitioners. BMJ Health & Care Informatics, 31(1), e101102.
View at Publisher | View at Google Scholar - Blease, C., Kaptchuk, T. J., Bernstein, M. H., Mandl, K. D., Halamka, J. D., & DesRoches, C. M. (2019). Artificial intelligence and the future of primary care: Exploratory qualitative study of UK general practitioners’ views. Journal of Medical Internet Research, 21(3), e12802.
View at Publisher | View at Google Scholar - Branquinho, C., Tomé, G., Grothausen, T., & Gaspar de Matos, M. (2020). Community-based youth participatory action research studies with a focus on youth health and well-being: A systematic review. Journal of Community Psychology, 48(5), 1301–1315.
View at Publisher | View at Google Scholar - Braun, V., & Clarke, V. (2006). Using thematic analysis in psychology. Qualitative research in psychology, 3(2), 77-101.
View at Publisher | View at Google Scholar - Braun, V., & Clarke, V. (2019). Reflecting on reflexive thematic analysis. Qualitative research in sport, exercise and health, 11(4), 589-597.
View at Publisher | View at Google Scholar - Choi, S. (2025). The role of generative AI in fostering digital health literacy among adolescents. Digital Health Education Journal, 12(1), 45–60.
View at Publisher | View at Google Scholar - Choudhry, F. R., Khan, N., & Munawar, K. (2023). Barriers and facilitators to mental health care: A systematic review in Pakistan. International Journal of Mental Health, 52(2), 124–162.
View at Publisher | View at Google Scholar - Tong, A., Sainsbury, P., & Craig, J. (2007). Consolidated criteria for reporting qualitative research (COREQ): a 32-item checklist for interviews and focus groups. International journal for quality in health care, 19(6), 349-357
View at Publisher | View at Google Scholar - Creswell, J. W., & Plano Clark, V. L. (2017). Designing and conducting mixed methods research (3rd ed.). Sage.
View at Publisher | View at Google Scholar - Dave, T., Athaluri, S. A., & Singh, S. (2023). ChatGPT in medicine: An overview of its applications, advantages, limitations, future prospects, and ethical considerations. Frontiers in Artificial Intelligence, 6, 1169595.
View at Publisher | View at Google Scholar - Das, A., & Muschert, G. (2024). A socio-cultural perspective on AI and the Global South: Guest editor’s introduction. Russian Sociological Review, 23(4), 9–15.
View at Publisher | View at Google Scholar - de Visser, R. O., Mushtaq, M., & Naz, F. (2022). Masculinity beliefs and willingness to seek help among young men in the United Kingdom and Pakistan. Psychology, Health & Medicine, 27(5), 1052–1062.
View at Publisher | View at Google Scholar - Fitzpatrick, K. K., Darcy, A., & Vierhile, M. (2017). Delivering cognitive behavior therapy to young adults with symptoms of depression and anxiety using a fully automated conversational agent (Woebot): A randomized controlled trial. JMIR Mental Health, 4(2), e7785.
View at Publisher | View at Google Scholar - Hang, Y., Wu, W., Feng, Y., Yan, K., Liu, Y., Xiao, X., & Qiao, Z. (2025). The effectiveness of CBT-based AI-driven conversational agents for mental health intervention: A systematic review and meta-analysis [Preprint].
View at Publisher | View at Google Scholar - Husain, M. O., Zehra, S. S., Umer, M., Kiran, T., Husain, M., Soomro, M., Dunne, R., Sultan, S., Chaudhry, I. B., Naeem, F., Chaudhry, N., & Husain, N. (2020). Stigma toward mental and physical illness: Attitudes of healthcare professionals, healthcare students and the general public in Pakistan. BJPsych Open, 6(5), e81.
View at Publisher | View at Google Scholar - Hussain, A., Sial, M. S., Usman, S. M., Hwang, J., Jiang, Y., & Shafiq, A. (2019). What factors affect patient satisfaction in public sector hospitals: Evidence from an emerging economy. International Journal of Environmental Research and Public Health, 16(6), 994.
View at Publisher | View at Google Scholar - Igwe, P. A., Madichie, N. O., & Rugara, D. G. (2022). Decolonising research approaches towards non-extractive research. Qualitative Market Research: An International Journal, 25(4), 453–468.
View at Publisher | View at Google Scholar - Joshi, A. (2015). Need for gender sensitive counselling interventions in India. Psychological Studies, 60(3), 346–355.
View at Publisher | View at Google Scholar - Khan, M. D., Daniyal, M., Abid, K., Tawiah, K., Tebha, S. S., & Essar, M. Y. (2023). Analysis of adolescents’ perception and awareness level for sexual and reproductive health rights in Pakistan. Health Science Reports, 6(1), e982.
View at Publisher | View at Google Scholar - Khan, S. J., Asif, M., Aslam, S., Khan, W. J., & Hamza, S. A. (2023). Pakistan’s healthcare system: A review of major challenges and the first comprehensive universal health coverage initiative. Cureus, 15(9), e44641.
View at Publisher | View at Google Scholar - Kretzschmar, K., Tyroll, H., Pavarini, G., Manzini, A., Singh, I., & NeurOx Young People’s Advisory Group. (2019). Can your phone be your therapist? Young people’s ethical perspectives on the use of fully automated conversational agents (chatbots) in mental health support. Biomedical Informatics Insights, 11, 1178222619829083
View at Publisher | View at Google Scholar - Liddon, L., Kingerlee, R., & Barry, J. A. (2018). Gender differences in preferences for psychological treatment, coping strategies, and triggers to help-seeking. British Journal of Clinical Psychology, 57(1), 42–58.
View at Publisher | View at Google Scholar - Littlejohn, T., Poteat, T., Beyrer, C., Mastroianni, A. C., Kahn, J. P., & Kass, N. E. (2019). Sexual and gender minorities, public health, and ethics. In The Oxford Handbook of Public Health Ethics (pp. 1–15). Oxford University Press.
View at Publisher | View at Google Scholar - Luo, X., Wang, Z., Tilley, J. L., Balarajan, S., Bassey, U., & Cheang, C. I. (2025). The global use of generative artificial intelligence for emotional and mental health support [Preprint]
View at Publisher | View at Google Scholar - Main Thompson, A., & Saleem, S. M. (2025). Closing the mental health gap: transforming Pakistan's mental health landscape. Frontiers in Health Services, 4, 1471528.
View at Publisher | View at Google Scholar - Malterud, K., Siersma, V. D., & Guassora, A. D. (2016). Sample size in qualitative interview studies: guided by information power. Qualitative health research, 26(13), 1753-1760
View at Publisher | View at Google Scholar - Mandal, S., & Hawamdeh, M. (2025). Digital well-being and AI. In Digital citizenship and the future of AI engagement, ethics, and privacy (pp. 111–132).
View at Publisher | View at Google Scholar - Mansfield, L. N., Chung, R. J., Silva, S. G., Merwin, E. I., & Gonzalez-Guarda, R. M. (2022). Social determinants of human papillomavirus vaccine series completion among U.S. adolescents: A mixed- methods study. SSM – Population Health, 18, 101082.
View at Publisher | View at Google Scholar - Maples, B., Cerit, M., Vishwanath, A., & Pea, R. (2024). Loneliness and suicide mitigation for students using GPT-3–enabled chatbots. npj Mental Health Research, 3(1), 4.
View at Publisher | View at Google Scholar - Mashhood, A., Saeed, G., & Sami, F. (2025). Sociocultural perceptions of suicide in Pakistan: A systematic review & qualitative evidence synthesis. SSM – Mental Health, 100433.
View at Publisher | View at Google Scholar - Mubeen, Z., Fatmi, Z., Hameed, W., & Asim, M. (2024). Barriers and facilitators to accessing adolescents’ mental health services in Karachi: Users’ and providers’ perspectives. BMC Health Services Research, 24(1), 157
View at Publisher | View at Google Scholar - Mustanski, B. (2011). Ethical and regulatory issues with conducting sexuality research with LGBT adolescents: A call to action for a scientifically informed approach. Archives of Sexual Behavior, 40(4), 673–686.
View at Publisher | View at Google Scholar - O’Cathain, A., Murphy, E., & Nicholl, J. (2008). The quality of mixed methods studies in health services research. Journal of Health Services Research & Policy, 13(2), 92–98.
View at Publisher | View at Google Scholar - Ozer, E. J., Abraczinskas, M., Suleiman, A. B., Kennedy, H., & Nash, A. (2024). Youth-led participatory action research and developmental science: Intersections and innovations. Annual Review of Developmental Psychology, 6(1), 401–423.
View at Publisher | View at Google Scholar - Purdam, K., Wilson, A. R., Afkhami, R., & Olsen, W. (2008). Surveying sexual orientation: Asking difficult questions and providing useful answers. Culture, Health & Sexuality, 10(2), 127–141.
View at Publisher | View at Google Scholar - Rahman, T. (2001). English-teaching institutions in Pakistan. Journal of Multilingual and Multicultural Development, 22(3), 242–261.
View at Publisher | View at Google Scholar - Renjith, G. P., Htoo, K. S. H., Mary, D. P., Samson, R. S., & Rashid, I. A. (2024). ChatGPT for academic purposes: Survey among undergraduate healthcare students in Malaysia. Cureus, 16(1), e51923.
View at Publisher | View at Google Scholar - Rashid, S. F., Desai, S., & Kumar, R. (2025). Situating sex, gender, and health in South Asia. In Handbook on sex, gender and health: Perspectives from South Asia (pp. 3–23). Springer Nature Singapore.
View at Publisher | View at Google Scholar - Schaaff, C., Bains, M., Davis, S., Amalraj, T., Frank, A., Waselewski, M., Chang, T., & Wong, A. (2025). Youth perspectives on generative AI and its use in health care. Journal of Medical Internet Research, 27, e72197.
View at Publisher | View at Google Scholar - Sellars, E., Pavarini, G., Michelson, D., Creswell, C., & Fazel, M. (2021). Young people’s advisory groups in health research: Scoping review and mapping of practices. Archives of Disease in Childhood, 106(7), 698–704.
View at Publisher | View at Google Scholar - Shim, J. K. (2010). Cultural health capital: a theoretical approach to understanding health care interactions and the dynamics of unequal treatment. Journal of health and social behavior, 51(1), 1
View at Publisher | View at Google Scholar - Siddals, S., Torous, J., & Coxon, A. (2024). “It happened to be the perfect thing”: Experiences of generative AI chatbots for mental health. npj Mental Health Research, 3(1), 48.
View at Publisher | View at Google Scholar - Simon, F. M., Altay, S., & Mercier, H. (2023). Misinformation reloaded? Fears about the impact of generative AI on misinformation are overblown. Harvard Kennedy School Misinformation Review,4(5).
View at Publisher | View at Google Scholar - United Department of Economic and Social Affairs, Population (2024). World Population Prospects 2024: Summary of results.
View at Publisher | View at Google Scholar - Wentzell, K., Walker, H. R., Hughes, A. S., & Vessey, J. A. (2021). Engaging social media influencers to recruit hard-to-reach populations. Nursing Research, 70(6), 455–461
View at Publisher | View at Google Scholar - Wright, K. B. (2005). Researching Internet-based populations: Advantages and disadvantages of online survey research, online questionnaire authoring software packages, and web survey services. Journal of Computer-Mediated Communication, 10(3), JCMC1034.
View at Publisher | View at Google Scholar
