

Case Report | DOI: https://doi.org/10.31579/2834-5142/104
Unilateral Fibromuscular Dysplasia in a Young Lady Presenting with Renovascular Hypertension: A Rare Clinical Entity
*Corresponding Author: Richmond Ronald Gomes, Professor and Head, Medicine, Ad-din Women’s Medical College Hospital, Dhaka Bangladesh.
Citation: Richmond R. Gomes, (2025), Unilateral Fibromuscular Dysplasia in a Young Lady Presenting with Renovascular Hypertension: A Rare Clinical Entity. Int. Journal of Clinical Nephrology. 4(2); DOI:10.31579/2834-5142/104
Copyright: © 2025, Richmond Ronald Gomes. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 10 April 2025 | Accepted: 17 April 2025 | Published: 28 April 2025
Keywords: renovascular hypertension; secondary hypertension; fibromuscular dysplasia
Abstract
Renovascular hypertension is associated with increased cardiovascular mortality and morbidity and may constitute a treatable cause of secondary hypertension. Renal artery stenosis (RAS) due to fibromuscular dysplasia (FMD) is an uncommon cause of renovascular hypertension. It frequently affects children, but is very rare in adults and is more common in females. We report the case of a 22-year-old asymptomatic female found to have high blood pressure on routine checkup. Doppler ultrasonography and CT angiography of renal arteries revealed fibromuscular dysplasia involving the right renal artery.
Introduction
Renovascular hypertension is one of the most common treatable causes of secondary hypertension. The incidence depends upon the clinical presentation with ranges from <1>
Case report
We present a case of 22-year-old overweight, female student who was found to have high blood pressure during routine checkup. She did not have any symptoms prior to the hospital visit. There was no family history of hypertension or familial dyslipidemia. Her maximal recorded blood pressure was 190/110 mmHg in both the arms. All peripheral pulses were palpable with no radio-radial or radio-femoral delay. The initial clinical exam showed an overweight (BMI- 24.5 kg/m2) female patient with normal cardiovascular, respiratory, and central nervous system examinations and no detectable heart or vascular (including abdominal) bruits. There were no features of hypo- or hyperthyroidism and Cushing’s syndrome. Routine blood investigations including urea, creatinine was normal. Serum electrolyte showed mild hypokalemia (3.1 mmol/L). No changes were found concerning the plasmatic and urinary cortisol and thyroid hormones’ dosages. The urine analysis revealed no signs of proteins, red cells or cellular elements. We evaluated 17 hydroxyprogesterone, testosterone, luteinizing hormone, follicle-stimulating hormone, and prolactin in order to eliminate the possibility of an 11-hydroxylase deficiency (known to associate elevated BP and hypokalemia tendency). Also, the progesterone was measured on the 22nd day, in order to document the ovulation and plasma free metanephrine. The results of the above-mentioned tests were not relevant for any endocrine possible cause of hypertension in this particular case (pheochromocytoma, Cushing disease,11 hydroxylase deficiency). Moreover, the patient was not using oral contraceptives.
Additionally, we attempted to dismiss the possibility of a reno parenchymal hypertension. Therefore, we performed an abdominal ultrasound that did not show any renal or adrenal masses, but there was major size difference between the two kidneys (left kidney 105 mm and tight kidney 85 mm) with normal cortico-medullary differentiation possibly suggesting renal artery stenosis) (Figure 1)
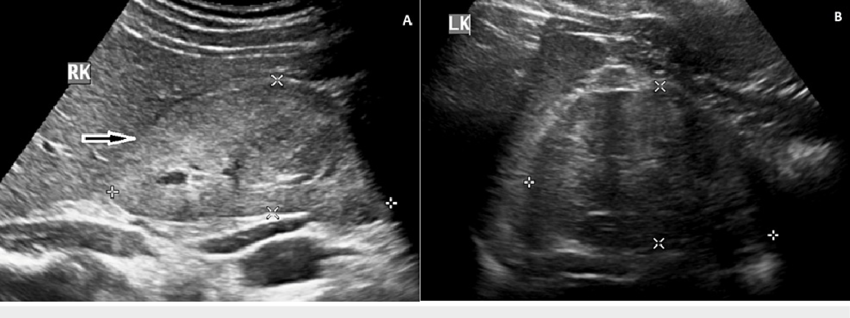
Figure 1: Ultrasonography of abdomen revealed small right kidney
Her chest X-ray and ECG were normal. During the echocardiography investigation, a slight hypertrophy of the ventricular walls was described, without any impact on the overall and segmented heart function and no hemodynamically significant valvulopathy.
We started her on standard anti-hypertensive medications with combination of calcium channel blocker and angiotensin receptor blocker and did further investigations. As renal artery stenosis was suspected from clinical examination, renal Doppler was performed, which did not reveal any renal artery stenosis. Because of low sensitivity of the renal Doppler examination, arterial stenosis was not ruled out. Since clinical examination and different kidney sizes were in favor of renal artery stenosis, we decided to go for CT renal angiography which revealed multifocal renal FMD in right renal artery with angiographic appearance of strings of beads. (Figure 2) Left renal artery was normal.
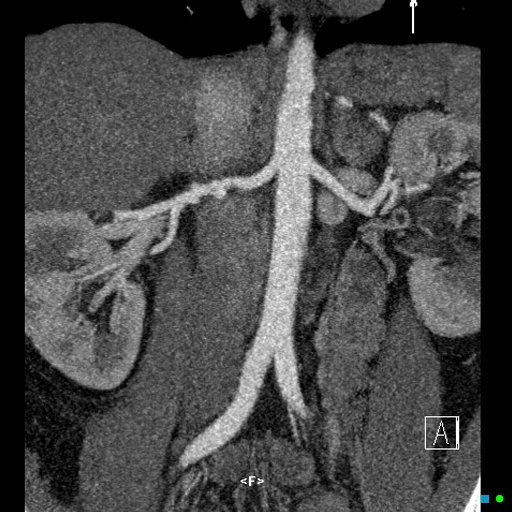
Figure 2: CT renal angiography which revealed multifocal renal FMD in right renal artery with angiographic appearance of strings of beads with normal left renal artery.
She was referred to vascular surgeon for further evaluation and possible need for balloon angioplasty.
Discussion
Fibromuscular dysplasia is an uncommon cause of arterial disease that predominantly affects females.[10] It is a noninflammatory, non-atherosclerotic disease which lead to the narrowing of the small and medium size arteries. It mostly involves the renal and carotid arteries but can involve any arterial bed. Renal artery is involved in around 60–75% of patients.[7] in the distal two thirds or even segmental segments. Despite various hypotheses linking it to genetic, mechanic or hormonal factors that are being suggested, the pathogenesis of this disease remains unknown. Fibromuscular dysplasia (FMD) is one of the two main causes of RAS, accounting for less than 10% of these cases [11].
There is no generally accepted classification. Histologically, FMD is classified based on the dominant arterial wall layer involved, namely intimal, medial, and adventitial (perimedial).[12] The most common is the medial type which accounts for 85% of cases and is characterized by ‘‘string of beads” appearance. The intimal and adventitial types constitute 5% and 10% respectively.[13].
The common age of renal involvement in FMD is between 15 and 50 years of age. Most commonly, the disease is asymptomatic and is discovered during the routine checkup or while investigating for some other disease.[7] The commonest presentation of FMD is renovascular hypertension. The
mechanism depends on whether the stenosis is unilateral (renin-mediated hypertension) or bilateral (volume dependent hypertension).[14] Two-thirds of RAS due to FMD is bilateral.[15]
A recent and sudden onset of severe arterial hypertension in a young female patient with negative pathological personal and family history may raise the possibility of renal artery stenosis. Likewise, refractory hypertension to aggressive antihypertensive treatment is most likely to indicate RAS, and this pathology needs to be investigated (class I, evidence level B) [16]. In the present case report, subsequent to the RAS diagnosis, the fibro-muscular dysplasia was suggested by female gender and age.
During the initial evaluation, FMD is often overlooked, or the diagnostic is established incidentally due to an imagistic exam performed for other reasons. Unlike the atherosclerotic renal artery stenosis, the evolution towards occlusion or ischemic atrophy of the ipsilateral kidney occurs rather seldom. On the other hand, hypokalemia (due to hyperreninemia) can be a helpful predictor for reno-vascular disease. The differential for FMD is set by comparison, to atherosclerotic stenosis, vasculitis, Takayasu arteritis, various rare family conditions (Ehlers–Danlos syndrome, Marfan syndrome, Alport syndrome, alpha1-antitrypsin deficiency). As far as our case was concerned, we considered the patient’s age as well as the negative elements for other causes of RAS the absence of plaque, thickening of the arterial walls and the lack of family history of the disease/syndromes.
Once FMD as a cause of renal artery stenosis is suspected, and there are various methods of imaging for confirmation of the diagnosis. Biochemical tests for the diagnosis of RAS by using renin lack specificity. Renal duplex sonography for the detection of hemodynamically significant renovascular disease has a sensitivity of only approximately 50%. The major limitation of duplex sonography is operator dependency.[17] The advantage is that it is noninvasive and has no apparent side effects.[18] Another advantage is that the measurement of resistive index in the cortical blood vessel can be done. Other methods are magnetic resonance angiogram (MRA) and computed tomographic angiography (CTA) with the use of high-resolution multi-slice detector devices.17 The CT imaging has its limitations; the quality of image depends upon equipment, technique, and reconstruction of the images, patient-related factors, including the presence of calcium, the presence of stents, and the ability to hold one’s breath during imaging.[7] MRA is limited by its frequent association of gadolinium contrast with nephrogenic systemic fibrosis.[19] Despite the invasive nature of investigation the gold standard in diagnosing FMD is intra-arterial angiogram but only as intent to revascularize because of its invasive nature. The characteristic feature is multifocal stenosis with the ‘‘string of beads” appearance, which likely indicates the presence of medial type FMD. Other patterns include tubular or focal lesions.[20] Two retrospective studies conducted on 20 and respectively 25 FMD patients revealed an 87% sensitivity for computer tomography angiography (CTA) by comparison to 97% for magnetic resonance angiography (MRA) in detecting angiographically confirmed lesions [21,22]. Another prospective study proved the excellent specificity of these two methods (99% and 96%). On the other hand, a sensibility of 28% for CTA and respectively 22% for RMA was established concerning the detection of multifocal lesions (medial fibro-dysplasia) [23].
FMD treatment must follow several goals: renal parenchyma protection while preserving renal function, BP control and the prevention of cardiovascular events. It is imperative to manage aggressively the additional risk factors by lowering lipid levels, smoking cessation and glucose levels [24].
Medical treatment is first indicated for the hypertensive patient. Medical management is done in accordance with the guidelines of the Joint National Committee on prevention, detection, evaluation, and treatment of high blood pressure.[24] Almost all the patients require at least one antihypertensive and the initial drug class of choice in FMD is an angiotensin-converting enzyme (ACE) inhibitor or angiotensin receptor blocker (ARB). [25,26,27] ACEI are contraindicated in bilateral severe RAS and single functional kidney. Thiazides, hydralazine, calcium channel blockers and b-blockers are also effective in achieving target blood pressures in individuals with RAS [13]. A recent cohort trial revealed a death rate reduction for patients treated with ACEIs. Since FMD does not affect the vascular endothelium, there are no indications for anti-aggregate treatment.
Revascularization is the treatment of choice in patients in young patients with hypertension refractory to pharmacological therapy, those who are intolerant to antihypertensive and in those who have lost renal volume due to ischemic nephropathy.[7] There are two modalities of revascularization - surgical angioplasty and percutaneous transluminal angioplasty (PTA). Nowadays, PTA has established itself as a revascularization method of choice with success rates of 60–80%.[28,29] The major advantages are that it is less costly, less invasive, can be performed as an outpatient procedure and has a lower morbidity.[7] In FMD, unlike the atherosclerosis, balloon angioplasty is the preferred therapy.[7] Routine use of stents in FMD is not recommended; however, if the dilatation is suboptimal and if renal artery dissection occurs, stenting can be performed.[30,31] Complications of PTA are around 14% and rarely, renal artery perforation, dissection or segmental renal infarctions may occur.[32,33] In 30–50% of cases, complete resolution of hypertension is achieved.[27,28]. There are no controlled studies comparing angioplasty and surgical revascularization. Current guidelines recommend balloon angioplasty for multifocal or troncular fibro-muscular lesions, and surgery for complex lesions (at the junction or reaching the segmental branches, stenosis associated with microaneurysms) or unsuccessful angioplasty (class IIb, evidence level C) [16,34]. Negative prognostic factors after the intervention are related to patient’s age, long period of arterial hypertension, onset of the renal parenchyma disease, type of lesion and associated atherosclerotic lesions.
Conclusion:
In conclusion, renovascular hypertension caused by unilateral renal artery stenosis secondary to fibromuscular dysplasia, a potentially curable and reversible disease when promptly diagnosed and appropriate treatment is implemented. Hyperreninemic hypertension, natriuretic hyponatremia, and unilateral renal hypoplasia are clinical clues that aid in uncovering the diagnosis.
Conflict of interest:
None declared
References
- Lewin A, Blaufox MD, Castle H, Entwisle G, Langford H. (1985). Apparent prevalence of curable hypertension in the hypertension detection and follow-up program. Arch Internal Med145 (3):424–427.
View at Publisher | View at Google Scholar - Textor SC, Lerman L. (2010). Renovascular hypertension and ischemic nephropathy. Am J Hypertension 23(11):1159–1169.
View at Publisher | View at Google Scholar - Safian RD, Textor SC. (2001). Renal-artery stenosis. New Engl J Med;344(6):431–442.
View at Publisher | View at Google Scholar - Geavlete O, Ca˘ lin C, Croitoru M, Lupescu I, Ginghina˘ C. (2012). Fibromuscular dysplasia–a rare cause of renovascular hypertension Case study and overview of the literature data. J Med Life 155(3):316 (Sep 15).
View at Publisher | View at Google Scholar - Deal JE, Snell MF, Barratt TM, Dillon MJ. (1992). Renovascular disease in childhood. J Pediat;121(3):378–384.
View at Publisher | View at Google Scholar - Piercy KT, Hundley JC, Stafford JM, et al. (2005). Renovascular disease in children and adolescents. J Vasc Surg 41:973.
View at Publisher | View at Google Scholar - Slovut DP, Olin JW. (2004). Fibromuscular dysplasia. New Engl J Med;350(18):1862–1871.
View at Publisher | View at Google Scholar - Lu¨ scher TF, Keller HM, Imhof HG, et al. (1986). Fibromuscular hyperplasia: extension of the disease and therapeutic outcome. Results of the University Hospital Zurich Cooperative Study on Fibromuscular Hyperplasia. Nephron 44(Suppl 1):109.
View at Publisher | View at Google Scholar - Begelman SM, Olin JW. (2000). Fibromuscular dysplasia. Curr Opin Rheumatol; 12:41–47.
View at Publisher | View at Google Scholar - Chrysochou C, Kalra PA. (2009). Epidemiology and natural history of atherosclerotic renovascular disease. Prog Cardiovasc Dis. Nov-Dec; 52:184-195.
View at Publisher | View at Google Scholar - Harrison Jr EG, McCormack LJ. (1971). Pathologic classification of renal arterial disease in renovascular hypertension. Mayo Clin Proc; 46:161–167.
View at Publisher | View at Google Scholar - Plouin PF, Perdu J, Alanore ALB, Boutouyrie P, Roqueplo APG, Jeunemaitre X. (2007). Fibromuscular dysplasia. Orphanet J Rare Dis; 2:28.
View at Publisher | View at Google Scholar - Olin JW, Novick AC. (1996). Renovascular disease. In: Young JR, Olin JW, Bartholomew JR. Peripheral vascular diseases. 2nd ed. St. Louis. p. 321–342.
View at Publisher | View at Google Scholar - Urban BA, Ratner LE, Fishman EK. (2001). Three-dimensional volume rendered CT angiography of the renal arteries and veins: normal anatomy, variants, and clinical applications. Radiographics 21:373–386.
View at Publisher | View at Google Scholar - Tendera M, Aboyans V, Bartelink ML, Baumgartner I, Clément D, Collet JP, et.al. (2011). Guidelines on the diagnosis and treatment of peripheral artery diseases: Document covering atherosclerotic disease of extracranial carotid and vertebral, mesenteric, renal, upper and lower extremity arteries: the Task Force on the Diagnosis and Treatment of Peripheral Artery Diseases of the European Society of Cardiology (ESC). Eur Heart J. Nov;32(22):2851-2906.
View at Publisher | View at Google Scholar - Mann DL, Zipes DP, Libby P, Bonow RO. (2014). Braunwald’s heart disease: a textbook of cardiovascular medicine. Elsevier Health Sciences, Jul 30.
View at Publisher | View at Google Scholar - Olin JW, Piedmonte MR, Young JR, DeAnna S, Grubb M, Childs MB. (1995). The utility of duplex ultrasound scanning of the renal arteries for diagnosing significant renal artery stenosis. Ann Intern Med 122:833–838.
View at Publisher | View at Google Scholar - Canavese C, Mereu MC, Aime S, et al. (2008). Gadolinium-associated nephrogenic systemic fibrosis: the need for nephrologists’ awareness. J Nephrol 21:324–336.
View at Publisher | View at Google Scholar - Kincaid OW, Davis GD, Hallermann FJ, Hunt JC. (1968). Fibromuscular dysplasia of the renal arteries: arteriographic features, classification, and observation on natural history of the disease. Am J Roentgenol 104:271–282.
View at Publisher | View at Google Scholar - Beregi JP, Louvegny S, Gautier C, Mounier-Vehier C, Moretti A, Desmoucelle F. (1999). Fibromuscular dysplasia of the renal arteries: comparison of helical CT angiography and arteriography.AJR Am J Roentgenol. Jan 172(1):27-34.
View at Publisher | View at Google Scholar - Willoteaux S, Faivre-Pierret M, Moranne O, Lions C, Bruzzi J, Finot M. (2006). Fibromuscular dysplasia of the main renal arteries: comparison of contrast-enhanced MR angiography with digital subtraction angiography. Radiology.2006 Dec;241(3):922-999. Epub Oct 19.
View at Publisher | View at Google Scholar - Vasbinder GB, Nelemans PJ, Kessels AG, Kroon AA, Maki JH, et.al. (2004). Renal Artery Diagnostic Imaging Study in Hypertension (RADISH) Study Group. Accuracy of computed tomographic angiography and magnetic resonance angiography for diagnosing renal artery stenosis. Ann Intern Med. Nov 2;141(9):674- 682; discussion 682.
View at Publisher | View at Google Scholar - Baumgartner I, Lerman LO. (2011). Renovascular hypertension: screening and modern management. Eur Heart J.2011 Jul;32(13):1590-1598. Epub Jan 27.
View at Publisher | View at Google Scholar - Chobanian AV, Bakris GL, Black HR, Cushman WC, Green LA, et.al. (2003). Seventh report of the joint national committee on prevention, detection, evaluation, and treatment of high blood pressure. Hypertension Dec 1;42(6):1206–1252.
View at Publisher | View at Google Scholar - Olin JW, Gornik HL, Bacharach JM, et al. (2014). Fibromuscular dysplasia: state of the science and critical unanswered questions: a scientific statement from the American Heart Association. Circulation 129:1048.
View at Publisher | View at Google Scholar - Tullis MJ, Caps MT, Zierler RE, et al. (1999). Blood pressure, antihypertensive medication, and atherosclerotic renal artery stenosis. Am J Kidney Dis 33:675.
View at Publisher | View at Google Scholar - Dworkin LD, Cooper CJ. (2009). Clinical practice. Renal-artery stenosis. N Engl J Med 361:1972.
View at Publisher | View at Google Scholar - Weinberg I, Gu X, Giri J, Kim SE, Bacharach MJ, Gray BH, et al. (2015). Anti-platelet and anti-hypertension medication use in patients with fibromuscular dysplasia: results from the United States Registry for fibromuscular dysplasia. Vasc Med; 20:447–453.
View at Publisher | View at Google Scholar - Trinquart L, Mounier-Vehier C, Sapoval M, Gagnon N, Plouin PF. (2010). Efficacy of revascularization for renal artery stenosis caused by fibromuscular dysplasia: a systematic review and meta-analysis. Hypertension;56(3):525–532.
View at Publisher | View at Google Scholar - Birrer M, Do DD, Mahler F, Triller J, Baumgartner I. (2002). Treatment of renal artery fibromuscular dysplasia with balloon angioplasty: a prospective follow-up study. Eur J Vasc Endovasc Surg; 23:146–152.
View at Publisher | View at Google Scholar - de Fraissinette B, Garcier JM, Dieu V, Mofid R, Ravel A, Boire L, Boyer L. (2003). Percutaneous transluminal angioplasty of dysplastic stenoses of the renal artery: results on 70 adults. Cardiovas Intervent Radiol Feb 1;26(1):46–51.
View at Publisher | View at Google Scholar - Sos TA, Pickering TG, Sniderman K, et al. Percutaneous transluminal renal angioplasty in renovascular hypertension due to atheroma or fibromuscular dysplasia. N Engl J Med 1983; 309:274–279.
View at Publisher | View at Google Scholar - Tegtmeyer CJ, Selby JB, Hartwell GD, Ayers C, Tegtmeyer V. (1991). Results and complications of angioplasty in fibromuscular disease. Circulation Feb;83(2 Suppl), I155-1161.
View at Publisher | View at Google Scholar - Solinas A, Cadoni R, Usai M, Frongia M. (2010). Fibromuscular dysplasia causing renal artery aneurysm and renovascular hypertension: a case report. Arch Ital Urol Androl. Dec; 82(4):181-183.
View at Publisher | View at Google Scholar
