

Research Article | DOI: https://doi.org/10.31579/2834-8486/019
Spermatocele: A Review and Update
- Anthony Kodzo-Grey Venyo *
North manchester general hospital, department of urology, delaunays road. Manchester, United Kingdom.
*Corresponding Author: North manchester general hospital, department of urology, delaunays road. Manchester, United Kingdom.
Citation: Anthony Kodzo-Grey Venyo., (2022). Spermatocele: A Review and Update., International Journal of Clinical Therapeutics. 3(6); DOI:10.31579/2834-8486/019
Copyright: © 2022, Anthony Kodzo-Grey Venyo. Nguyen, this is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 18 November 2024 | Accepted: 02 December 2024 | Published: 20 December 2024
Keywords: Spermatocele; testis; rete testis; epididymis; dilatation; asymptomatic; pain; scrotal mass; torsion; ultrasound scan; magnetic resonance imaging scan
Abstract
A spermatocele is a benign dilatation of efferent ductules within the testis, rete testis or head of the epididymis. The size of a spermatocele does tend to vary from a few millimeters to 2 cm. A spermatocele is usually an idiopathic lesion; nevertheless, cystic dilatations within the epididymis or rete-testis could emanate from outflow obstruction of the genital drainage system. A spermatocele could be palpable upon manual examination of the scrotum and scrotal contents but the diagnosis of spermatocele tends to be demonstrated by the undertaking of ultrasound scan of scrotum and scrotal contents that would illustrate the cystic dilatation related to the epididymis or testis / rete testis or on rare occasions by the undertaking of magnetic resonance imaging scan of scrotum and scrotal contents which would usually demonstrate the cyst. However, Aspiration of the cyst or cysts for cytopathology examination or frozen section examination of biopsy specimen of the cyst or the completely excised cyst or an orchidectomy specimen based upon a provisional diagnosis of testicular cancer is what confirms presence of spermatozoa within the cystic cavity to establish the diagnosis of a spermatocele. A spermatocele, generally tends to be lined by cuboidal, columnar, ciliated, or flattened epithelium. The cystic contents of a spermatocele contain spermatozoa. Clinically, it is not easy to differentiate a spermatocele from an epididymal cyst. All ages of males have been documented to have a spermatocele from individuals who are young or adults and it has been reported in a 2-month-old baby / child, other children and teenagers as well as older people but the common age groups affected by spermatocele have tended to be aged between 20 years and 50 years. There has tended to be a higher incidence of spermatocele associated with cystic fibrosis as well as with exposure within the uterus to diethyl stilbesterol. Spermatocele may be idiopathic and associated with no symptoms and may be found incidentally or a spermatocele may manifest as a noticeable or palpable intra-scrotal mass that is separate from the testis, an ache or dull / mild pain within the scrotum, and occasionally acute sudden onset of pain tends to simulate the manifestations of torsion of the testis. A spermatocele may manifest as a mass that simulates testicular tumour, a hydrocele or hydrocele of the cord, a cystadenoma of testis or possibly other types of intra-scrotal lesions including other rare types of intra-scrotal malignant lesions. A spermatocele could be unilateral or bilateral, single, or multiple. A spermatocele may be found alone or in association with other intra-scrotal lesions and some of these include: another type of intra-scrotal cyst, hydrocele, or hydrocele of the cord, inguinal-scrotal hernia, or varicocele. A spermatocele sometimes may simulate a testicular cancer. Majority of spermatoceles tend to be managed conservatively or expectantly. However, some spermatoceles had been treated by means of aspiration of the spermatoceles plus / sclerotherapy. Other spermatoceles had been effectively and successfully treated surgically by exploration of the scrotum and excision of the spermatocele completely whilst preserving the epididymis and the testis which enabled the male to impregnate his female partner. Surgical treatment for spermatocele tends to be undertaken due to increasing pain in the scrotum, continued enlargement of the intra-scrotal mass, the spermatocele has been adjudged to simulate a testicular tumour or is provisionally diagnosed as a testicular tumour, torsion of the testis or a provisional diagnosis of an inguinal-scrotal hernia, a hydrocele or hydrocele of the cord and during the operation the spermatocele is diagnosed. Unfortunately, some patients who had spermatoceles that had been misdiagnosed as testicular cancer had undergone radical orchidectomy only to find that they only had spermatoceles. In some reported cases of infertility associated with spermatocele and pain, successful excision of the spermatocele whilst preserving the epididymis had emanated in the successful impregnation of the patients partner subsequently, as well as aspiration of spermatozoa from the spermatocele to be preserved and used for assisted conception has enabled a man with a spermatocele to impregnate his partner. There is a documentation of a man who was born without epididymis who had undergone construction of an artificial spermatocele and ensuing this operation, the partner of the patient subsequently was impregnated by the man with an artificial spermatocele. Considering that some intra-scrotal cystic masses tend to be spermatoceles and testicular cancer, if Urologists and interventional radiologists agree as routine undertake preceding the procedure of radical orchidectomy for all cystic types of “testicular tumours”, aspiration / biopsy of the cystic lesions for pathology examination as part of treatment planning, then the diagnosis of spermatocele would be confirmed and an unnecessary radical orchidectomy would be avoided.
Introduction
{A] OVERVIEW
Definition / general [2]
- The terminology spermatocele is used for benign dilatation of efferent ductules within the rete testis or head of epididymis
- It has been pointed out that the size of a spermatocele does range a few millimetres up to 2 cm
Essential features
The essential features of a spermatocele had been summated as follows: [2]
- A spermatocele represents a benign dilatation of the efferent ductules within the rete testis or head of the epididymis
- A spermatocele is usually idiopathic but cystic dilation from outflow obstruction may play a role in the development of a spermatocele.
- A spermatocele is usually diagnosed by the undertaking of ultrasound scan of scrotum and scrotal contents which does tend to demonstrate a well-defined simple cyst
- A spermatocele is lined by cuboidal, columnar, ciliated or flattened epithelium
- The cystic contents of a spermatocele often contain spermatozoa
Terminology
- With regard to terminology, it has been pointed out that a spermatocele is often indistinguishable from epididymal cyst [2]
Epidemiology
- With regard to the epidemiology of spermatocele, it has been iterated that all ages of males are affected but typically a spermatocele does tend to occur in 20-year-old, to 50-year-old men [2]
Sites
With regard to the sites of spermatoceles, it has been pointed spermatocele could be found within: [2]
- The testis and
- The epididymis
Aetiology [2]
- Aetiology of spermatocele development has been stated to usually of idiopathic origin; nevertheless, cystic dilation from outflow obstruction may play a role [3]
- It has been iterated that there has tended to be a higher incidence of spermatocele in cystic fibrosis and diethyl-stilbestrol exposure in utero. [4]
Clinical features
- It has been pointed out that a spermatocele does tend to manifest with a painless bulging mass within the scrotum that is separate from the testis. [2]
Diagnosis
- It has been pointed out that diagnosis of a spermatocele has tended to be established by the undertaking of radiology imaging, including ultrasound scan of the scrotal contests and testes and less commonly by the undertaking of Magnetic Resonance Imaging (MRI) Scan of the testes and scrotal contents, followed by pathological evaluation of the resection specimen or at times aspiration of the cyst for cytology examination which demonstrates spermatozoa within the aspirate obtained from the cyst in the epididymis or testis.
Radiology image description
- It has been iterated that ultrasound scan of the scrotal contents and testes does tend to demonstrate, simple cysts which generally tend to be well defined and anechoic; nevertheless, low-level echoes demonstrating “falling snow sign” or sedimentation levels can be demonstrated upon radiology imaging of the scrotal contents. [5] [6]
- It has been pointed out that with regard to spermatocele, the cyst may displace the testis if it is large [2]
- It has been explained that a spermatocele is distinct from a hydrocele, which does envelop the testis but does not displace it [2]
Other ways of diagnosing spermatoceles
- A spermatocele on rare occasions may manifest with acute scrotal pain on rare occasions. [7]
- A spermatocele may be diagnosed under the pivot of undertaking fine needle aspiration for cytology pathology examination of the intra-scrotal cystic lesion which may confirm the diagnosis of the spermatocele. [8]
- A spermatocele may simulate a hydrocele therefore a high-index of suspicion is required to diagnose some cases of spermatoceles and there may be difficulty in diagnosing some cases of spermatoceles. [9]
Treatment
- Some spermatoceles may be left alone or they may be managed expectantly and surgical excision undertaken when required. [2]
- Surgical resection of the spermatocele which is referred to as spermatocelectomy is the definite treatment for a spermatocele when it is required. [2]
Gross description
The macroscopy examination features of spermatocele specimens had been summarized as follows:
- The excised spermatocele specimen does arrive in the laboratory as a collapsed, thin -walled membrane [10]
- The spermatocele specimen upon gross examination does look round or ovoid with regard to its size.
- The cysts of spermatocele may be unilocular or multilocular and translucent [10]
- Spermatocele most commonly arises from the head of the epididymis
Microscopy (histologic) description
- It has been explained that microscopy examination of a specimen of a spermatocele does initially tend to be lined by single layer of cuboidal to ciliated columnar epithelium which becomes flattened as fluid accumulates [10]
- A spermatocele does have a thin wall of fibromuscular soft tissue
- The lumen of a spermatocele comprises cyst wall and the adjacent soft tissue does contain spermatozoa and proteinaceous fluid [11]
- Upon microscopy examination, a spermatocele does tend to be found to be associated with foreign body giant cell reaction, cholesterol clefts [11]
- Microscopy examination of a spermatocele does demonstrate that the epithelial lining may form papillary structures with fibromuscular cores that are lined by a single layer of columnar to cuboid epithelium with vacuolated cytoplasm [2]
Cytology description
- It has been iterated that cytology examination of spermatocele specimen does tend to demonstrate cysts which could contain spermiophages, macrophages with abundant distended cytoplasm containing intact spermatozoa [2] [11]
Positive stains
It has been pointed out that specimens of spermatoceles do tend to exhibit positive immunohistochemistry staining for: [2] [11]
- AE1/AE3.
- EMA.
- Vimentin. [12]
Negative stains
It has been pointed out that specimens of spermatoceles do tend to exhibit negative immunohistochemistry staining for: [2]
- Calretinin.
- D2-40.
- WTI. [13]
Differential diagnoses
The differential diagnoses of spermatoceles had been summated to include the following: [2]
- Hydrocele:
- A hydrocele does tend to originates between the parietal and visceral layers of tunica vaginalis
- The lining of a hydrocele is mesothelial and its lumen does not contain spermatozoa
- Mesothelial cyst:
- Mesothelial cyst does usually originate from tunica vaginalis or tunica albuginea
- Cystic dysplasia of rete testis:
- Cystic dysplasia of rete testis is a congenital lesion of newborns which is associated with ipsilateral renal agenesis
- Sertoliform cystadenoma of rete testis:
- Sertoli cystadenoma of rete testis does contains tubules with or without lumen [14]
- Simple cyst of rete testis:
- Simple cyst of rete testis does tend to bulges into the testis proper
- Simple cyst of rete testis tends to be commonly found in men who are undergoing renal dialysis
- Simple cyst of rete testis tends to have columnar epithelium, calcium oxalate crystals, fibrosis and giant cells
- Tubular ectasia of rete testis:
- Tubular ectasia of rete testis does contain numerous dilated canaliculi
- Tubular ectasia of rete testis could coexist with a spermatocele [15]
- Dermoid cyst:
- Dermoid cyst rarely manifests within the spermatic cord or as a para-testicular mass
[B] Miscellaneous Narrations and Discussions Related to Some Case Reports< Cases>
Erikci et al. [4] undertook a retrospective review to evaluate the clinical presentation of children who had epididymal cysts (EC) and outcome of management within their institution. Erikci et al. [4] reported that there were 49 patients who had EC in their series. The diagnosis of EC was made based upon clinical examination and this was confirmed by the undertaking of ultrasound (US) scanning of the scrotum and scrotal contents. Erikci et al. [4] summarized the results as follows:
- The average age at presentation of the patients was 10.7 years and the ages of the patients had ranged between 2 months and 16 years.
- The most frequent presenting symptoms were scrotal mass which was noted in 22 patients and intra-scrotal pain in 21 patients.
- Seven patients were lost to undergo follow-up assessment.
- The cysts were solitary with regard to 32 patients and multiple in 10 patients.
- The mean measurement of the cysts with regard to their size was 6.7 mm but this had ranged between 2 mm and 20 mm.
- The cyst localisations were 22 in the left side, 16 in right side, and bilateral in 4 in the patients.
- They had detected complete involution of cysts in 14 children.
- The average involution time was 11.2 months and this had ranged between 1 month and 37 months. With regard to 20 cases, a decrease in cyst size was found.
- Cyst excision was undertaken in 8 patients who had persistent scrotal pain or no cyst involution observed during follow-up.
Erikci et al. [4] made the ensuing conclusions:
- Conservative management of epididymal cysts is practical.
- Nevertheless, surgical excision is recommended in patients who develop intractable scrotal pain or if the cyst size does not seem to involute.
Hikosaka and Iwase al. [7] reported a case of a patient who had a spermatocele and who had manifested with an acute scrotal pain. This case report is important in that even though most cases of spermatocele tend to be discovered incidentally or the patients who have spermatoceles do present with intra-scrotal mass only. Hence clinicians who encounter patients who present with acute or chronic intra-scrotal pain should have a high index of suspicion in order to regard spermatocele as a differential diagnosis in cases of intra-scrotal pain.
Sakuma et al. [8] reported a patient with an intra-scrotal lesion which was diagnosed a spermatocele based upon the observation of spermatocytes in the fine needle aspirate of spermatocele of the patient’s scrotum. A lesson that needs to be learnt from this case report is the fact that many cases of spermatocele can be diagnosed without the undertaking of more invasive procedure of exploration of scrotum and biopsy or intra-operative aspiration of the cystic intra-scrotal lesion for pathology examination to confirm the diagnosis of spermatocele.
Yeh et al. [9] stated that spermatoceles usually tend to be asymptomatic and they often tend to be found incidentally during physical examination. Yeh et al. [9] reported a case of giant spermatocele that simulated a hydrocele. Yeh et al. [9] reported the case of a 55-year-old man who had suffered from right scrotal enlargement for many years. As the heavy sensation and scrotal soreness worsened over the preceding months, he came to their outpatient clinic for help. Hydrocele was suspected as the provisional diagnosis due to the transilluminating appearance of the scrotal content. Surgical exploration was then arranged and undertaken and during the procedure a giant spermatocele was found. Total excision of the spermatocele was undertaken and the patient recovered well. The specimen was sent for pathology examination and pathology examination of the specimen was reported to have confirmed the diagnosis of a spermatocele with spermatozoa was noted.
Ejeckam et al. [10] reported a case of cyst of seminal vesicle which was associated with ipsilateral renal agenesis in a twenty-three-year-old man who had manifested primarily with rectal symptoms. The usual symptoms of the patient had been urinary bladder irritation and pain on ejaculation. Ejeckam et al. [10] stated the following:
- The spermatocele specimen upon gross examination does look round or ovoid with regard to its size.
- The cysts of spermatocele may be unilocular or multilocular and translucent [10]
- Spermatocele most commonly arises from the head of the epididymis
- Shah et al. [16] stated the following:
- Hydrocelectomy and spermatocelectomy are routine scrotal surgical operations.
- A significant number of the surgical specimens tend to be sent for pathology examination.
- Nevertheless, to their knowledge no study had been undertaken to examine the outcomes and necessity, which results in significant potentially unnecessary costs to the patient and the health care system.
- They had evaluated the outcomes and surgical pathology analysis of hydroceles and spermatoceles.
- With regard to the materials and methods of their study, Shah et al. [16] reported the following:
- They had undertaken a retrospective, single institution chart review of all patients who had undergone initial surgery for hydrocele or spermatocele between January 2000 and August 2013.
- They determined the number of cases in which a surgical specimen was sent for pathology examination.
- They had estimated the cost for each specimen at the department of pathology.
- Shah et al. [16] summarized the results as follows:
- A total of 264 routine scrotal cases were undertaken during the 14-year period.
- Surgical specimens were sent for pathology examination in 102 hydrocelectomy cases that amounted to 51% of the hydrocelectomy cases, and in 57 spermatocelectomy cases that amounted to 90% of spermatocelectomy cases.
- No pathology specimen had shown any indication of malignancy.
- The estimated direct total cost of pathology analysis was noted to be $49,449 in the cohort of cases they had studied.
- Shah et al. [16] made the following conclusions:
- No malignancy was identified in 159 hydrocele and spermatocele specimens during the 14 study years, which in their opinion had indicated that the pathology analysis is of little clinical benefit.
- Forgoing surgical pathology analysis of these specimens would have resulted in significant cost savings to the patient and the health care system.
Even though the conclusions of Shah et al. [16] would appear to be reasonable based upon the results of their study, it would be argued that the sample size of their study was not large enough and that the results emanating from some subsequent case reports and case studies had or would document evidence of a malignant lesion associated with hydroceles as well as spermatoceles and that excised hydrocele sacs and spermatocele lesions should all be sent for pathology examination in order not to miss the diagnosis of malignant mesothelioma of tunica vaginalis as well other tumours associated with spermatoceles even if they are rare.
Ameli et al. [17] stated the following:
- Testicular torsion is a rare disease which mostly involves children.
- The peak incidence for the development of testicular torsion is within infancy and in adolescence.
- Testicular torsion is rarely seen in men who are over 40 years of age and has only once been accompanied with spermatocele.
Ameli et al. [17] reported the case of a 40-year-old man who had developed testicular pain one day prior to visiting their clinic. The patient's visit to the clinic was delayed due to his past history of occasional testicular pain which was related to his bilateral spermatoceles. On his arrival, a colour Doppler ultrasound test was undertaken, which had demonstrated a heterogeneous echo within his right testis with no vascular flow, that was indicative of torsion, as well as two cystic lesions within his right and left scrotums indicating spermatoceles. The patient was immediately transferred to the operating theatre where in underwent exploration of his scrotum and his bilateral spermatoceles were found as well as resected and after detorting, the right testis was saved. After four months, his assessment upon follow-up demonstrated a normal left testis along with partial right testicular atrophy. Ameli et al. [17] made the ensuing iterations:
- It is highly recommended for clinicians to educate patients who have spermatocele who have no indication for surgical treatment to visit their physician in case they experience any new testicular pain.
- In addition, testicular pain regardless of the co-existing pathology may always be treated as an indicator of suspected torsion.
Choyke et al. [18] stated the following:
- Epididymal cystadenomas (ECs) are frequently encountered in association with von Hippel-Lindau disease (VHL); nevertheless, little had been reported about their ultrasound scan appearance.
- They had reviewed the ultrasound scan appearance of ECs, the relationship of ECs to other manifestations of VHL, and the specific genetic mutations that are associated with ECs.
- With regard to the materials and methods of their study, Choyke et al. [18] stated the following:
- They had examined fifty-six male patients who had VHL by the undertaking of scrotal ultrasound scanning and clinical examination as part of a larger screening program for VHL.
- They had measured the head of the epididymis in two planes on sonography and they had compared the ultrasound scan findings with age-matched normal controls.
- All VHL patients who had palpable epididymal abnormalities or enlargement of more than two standard deviations of the head of the epididymis upon ultrasound were considered positive for EC.
- Choyke et al. [18] summarized the results as follows:
- Thirty of 56 male patient that mounted to 54% of the male patients who had VHL had demonstrated a unilateral solid abnormality that totalled 10 patients that amounted to 33% or bilateral solid abnormality that totalled 20 patients that amounted to 67% of patients who had solid abnormality within the head of the epididymis that was suggestive of EC.
- The ultrasound scan appearances had ranged from a solid mass with multiple tiny cysts to an almost completely solid mass.
- The commonest appearance was a 15-mm to 20-mm solid mass with small cystic components.
- Dilated efferent ductules were visualized within the testis in 7 men, evidently a result of chronic obstruction.
- There was no association between the clinical subtype of VHL and the presence of ECs (P > 0.10, chi square).
- Mutations that resulted in a truncated gene product were found to be associated with the development of ECs but the association did not reach statistical significance (P = 0.06).
- Choyke et al. [18] made the following conclusions:
- ECs are a common presentation of VHL in men and they do exhibit a range of appearances upon ultrasound scan.
- Ultrasound scan can be utilized to identify ECs and to ascertain the extent of cystic dilation of the rete testes.
- The benign course of ECs and the usual absence of clinical symptoms do favour a conservative approach to their management.
The lesson that needs to be learnt from this article of Choyke et al. [18] is the fact that epididymal cystadenomas do simulate spermatoceles and their ultrasound scan features need to be well known by clinicians, radiologists, and urologists that manage patients who have spermatoceles also need to be familiar with the ultrasound scan features of all the differential diagnoses of spermatocele and to learn that in the end either a fine needle aspiration for cytology examination or biopsy of the intra-scrotal lesion for pathology examination is what will help clinicians to confirm the diagnosis of spermatocele.
Jahnson et al. [19] stated the following:
- Polidocanol sclerotherapy for the treatment of hydrocele or spermatocele combines high efficiency with low morbidity, however, the optimal dose is not known.
- They had compared the efficacy and morbidity of 2 or 4 ml polidocanol sclerotherapy for hydrocele or spermatocele.
- Jahnson et al. [19] reported that from 1993 to 2005, they had conducted a double-blind randomized clinical trial using 2 or 4 ml polidocanol (30 mg/ml) for sclerotherapy of hydrocele/spermatocele in 224 evaluable patients within 3 university hospitals. They had evacuated fluid and 2 or 4 ml polidocanol was administered by a nurse, with the amount injected concealed from others present. During the process of the 3-month follow-up assessment of the patients’ morbidity was ascertained by utilizing a questionnaire that was completed by the patients. Fluid recurrence was determined clinically and generally re-treated in the scenario of evidence of fluid recurrence in any patient. Jahnson et al. [19] summarized the results as follows:
- Pursuant to the first treatment, cure was observed in 59% and 47% in the 4 ml and the 2 ml group, respectively (p = 0.04).
- More patients within the 4 ml group had complications (31% versus 18%, p = 0.04).
- The identified complications were mostly of low or moderate intensity and seldom required medication.
- Pursuant to 1 treatment to 4 treatments 200 of 224 patients that amounted to 89% of the patients were cured and another 10 patients which amounted to 5% of the patients had small amounts of residual fluid, with no difference between the groups.
- Out of the patients who had hydroceles/spermatoceles larger than 175 ml, 58% and 34% were cured pursuant to the first treatment in the 4 ml and 2 ml groups, respectively (p = 0.012), with no differences in complications between the groups.
Jahnson et al. [19] made the ensuing conclusions:
- Polidocanol sclerotherapy was effective for the treatment of hydrocele or spermatocele in their patients, with 94% satisfactory results pursuant to 1treatment to 4 treatments.
- A dose of 4 ml was found to be superior to 2 ml, particularly for larger hydroceles/spermatoceles.
Yagi et al. [20] reported a case of a multilocular spermatocele. The patient underwent ultrasound scan of his scrotal contents which demonstrated several cystic spaces within the head of his left epididymis. Based upon the ultrasound scan features of the multiple cystic lesions, Yagi al. [20] could not exclude epididymal tumour, and therefore surgical exploration was undertaken by Johnson et al. Histopathology examination of the excised cystic specimen revealed a multilocular spermatocele which had arisen from his rete testis. Yagi et al. [20] pointed out that most spermatoceles do tend to remain small and rarely manifest marked clinical problems, however, they occasionally tend to be large, and they may simulate a solid tumour.
Walsh et al. [21] stated the following:
- Spermatoceles are benign cystic dilations of the epididymis.
- Despite their relatively common occurrence, it is not clear why or when men want this lesion to be treated.
Walsh et al. [21] reported a single institution series of men who had undergone spermatocelectomy. Walsh et al. [] described the clinical characteristics of men who had these lesions and postulated that men who have spermatoceles seek intervention when the lesion approximates the size of a testis. Walsh et al. [21] reviewed the characteristics of 24 men who sought excision of symptomatic spermatoceles. Walsh et al. [21] reported that the specific characteristics they had assessed included: the subject age, duration of diagnosis, symptom type, and symptom duration. With regard to the study, the spermatoceles were characterized by size, sidedness, and associated findings. Walsh et al. [21] utilized simple descriptive statistics for analysis of their findings. They summarized the results as follows:
- The mean age of men seeking spermatocelectomy was 46 years.
- Most of the men that amounted to 58% of the men, sought surgery due to a combination of pain and sensation of mass within the scrotum.
- The mean duration of symptoms was 48 months.
- At the time of excision of the spermatocele, the average size of the spermatoceles was 4.2 cm in greatest diameter, and most of the spermatoceles that amounted to 71% of the spermatoceles were right sided.
- Men who had experienced pain as an isolated symptom were noted to younger by about 10 years when they were compared to those who experienced mass.
Walsh et al. [21] made the ensuing observational conclusions:
- Men in their reported series appeared to tolerate spermatoceles for a relatively long period of time.
- Once the men seek excision of their spermatoceles, the spermatoceles had notedly grown to roughly the size of a normal testicle and the men were bothered both by pain and mass symptoms.
Weil et al. [22] in 1960 made the ensuing summations related to spermatoceles:
- Spermatozoa from spermatoceles do lack the antigenic material present on seminal spermatozoa, which these latter cells share with the seminal plasma.
- This does provide direct evidence that human spermatozoa acquire antigenic material during their passage through the adnexal glands of the genital tract.
Yeh et al. [9] stated that spermatoceles usually tend to be asymptomatic and spermatoceles are often found incidentally during clinical examination. Yeh et al. [9] reported a case of giant spermatocele that simulated a hydrocele. Yeh et al. [9] reported a 55-year-old man who had suffered from right scrotal enlargement for several years. As the heavy sensation and scrotal soreness worsened over the preceding months to his manifestation, he came to their outpatient clinic for help. Pursuant to his clinical examination, hydrocele was suspected in view of the transilluminating appearance of the scrotal content. He was listed to undergo surgical exploration of his scrotum, and during the procedure, a giant spermatocele was found. Total excision of the spermatocele was undertaken and the patient recovered well. The specimen was sent for pathology examination and spermatocele with spermatozoa was noted upon examination of the excised specimen.
Takimoto et al. [23] stated the following:
- Torsion of a spermatocele upon its pedicle is an extremely rare clinical condition that simulates acute testicular torsion.
- This rare condition had not been well characterized.
- Takimoto et al. [23] reported a case of torsion of a spermatocele. They stated that their reported case in 2002, was the 5th case of torsion of a spermatocele and the first report in a patient with a history of scrotal trauma. A tender cystic mass was found adjacent to the normally appearing testis within the scrotum was highly significant for the differentiation from other types of acute scrotum. Takimoto et al. [23] advised that torsion of a spermatocele should be considered a differential diagnosis of acute scrotum in adolescents and adults.
Basar et al. [24] reported the case of a bilateral, relatively huge, multilocular spermatocele which was diagnosed based upon the undertaking of ultrasound scan of scrotal contents of a man with surgical and pathological correlation. Basar et al. [24] reported a 45-year-old man who had presented with bilateral, large inguinoscrotal masses. He stated that he had had the masses since his adolescence period and their size had gradually increased over the preceding 5 years. He had scrotal ultrasound scan examination of his scrotal contents which showed cystic fluid masses that measured 65 mm × 45 mm × 50 mm in size on the right and 55 mm × 45 mm × 40 mm in size on the left side in multilocular spaces. The cystic masses were excised through a bilateral inguinoscrotal incision staying near the body of the epididymis. The patient had subsequently fathered three children with no fertility problem.
Jimenez Cruz [25] presented a new technique to construct an artificial spermatocele, utilising monofilament knitted polypropylene wrapped with tunica vaginalis and anastomosed end-to-end to the head or the body of the epididymis. The material was tested in 10 dogs. It did not harm the spermatozoa, the function of the reservoir or the tolerance of the encompassing tissues. Therefore, the material was utilised in a patient with bilateral congenital absence of the vasa deferentia, whose wife became pregnant pursuant to her cervical insemination. The spermatòcele was still functional after 15 months.
Low et al. [26] evaluated the efficacy of aspiration and sclerotherapy with 100% alcohol for the primary treatment of benign scrotal cysts. With regard to the methods of their study, Low et al. [26] reported that from March 2014 to March 2018, 114 patients had been identified who had undergone their first aspiration and sclerotherapy procedure which included 80 hydroceles and 34 spermatoceles/epididymal cysts. The procedure was undertaken within the outpatient clinic with local anaesthesia. A 16-gauge intravenous (IV) catheter was used to puncture the sac under aseptic conditions. The volume of alcohol instilled was 10% of the aspirated volume with a maximum volume of 50 mL The patients were then observed within the waiting room and they had completed a questionnaire. The Urology clinic follow up of the patients was scheduled at 6 weeks. Low et al. [26] summarized the results as follows:
- At follow up, 54 patients that amounted to 67.5% of the patients who had hydroceles and 25 patients that amounted to 73.5% of patients who had spermatoceles/epididymal cysts had resolution after a single procedure.
- A second procedure was offered if the fluid collection had persisted, of which 71% of patients who had hydroceles and 100% of patients who had spermatoceles/epididymal cysts had a successful outcome.
- At a median of 31 months pursuant to the initial procedure, the overall success rate, after at most two procedures, was found to be 80% for hydroceles and 85% for spermatoceles/epididymal cysts.
- The complication rate was low which had occurred in 6% of the patients.
- Almost all patients were happy to undergo the procedure again, if required.
- Persistence following aspiration and sclerotherapy were observed to be more likely to occur in younger patients (45.4 versus 61.2 years, P = 0.001).
- Persistence was not related to the volume of fluid aspirated.
Low et al. [26] concluded that aspiration and sclerotherapy with alcohol is a reliable, safe and effective technique for treatment of benign scrotal cysts.
Dollard and Fobia. [27] stated the following:
- Lower quadrant abdominal pain is a common complaint that tends to be evaluated in emergency departments (EDs).
- The number of differential diagnoses is lowered when the pain in a male patient is found to be associated with a palpable tender mass.
- These differential diagnoses include: inguinal hernia, inflamed inguinal lymph node, rectus sheath hematoma, cryptorchidism, mass that is derived from the spermatic cord, and polyorchidism.
Dollard and Fobia. [27] reported report a case of extra scrotal spermatocele which was causing lower quadrant abdominal pain that was misdiagnosed as an inguinal hernia on several of the patient’s emergency department (ED) visits. Dollard and Fobia. [27] stated that: Lower quadrant mass and pain caused by a spermatocele are unusual conditions. Upon the patient's third (ED) visit, the painful mass had remained located within his right lower quadrant of abdomen. The lower quadrant mass was found during the patient’s examination to be movable on palpation and with pressure it could be delivered into the superior aspect of the scrotum. The patient had an abdominal and pelvic computed tomography scan and lower quadrant abdominal ultrasound scan. The radiology imaging studies had demonstrated the mass to be a cystic structure. Surgical excision of the mass was undertaken and pathology examination of the excised specimen confirmed that the mass was a spermatocele.
Albano et al. [28] reported a 46-year-old man who had papillary thyroid cancer post total thyroidectomy and who was referred for post radioiodine (131I) whole-body scan. His Whole-body images revealed intense 131I uptake in the bed thyroid and a focal abnormal uptake within the testicular area. Subsequently he had SPECT/CT which demonstrated that the focal uptake corresponded to his left epididymis, and the pathology report of his excised epididymal lesion revealed a spermatocele with no immunohistochemical features for thyroid tissue. Albano et al. [28] stated that many cases of unexpected radioiodine uptake had been reported in the literature, and spermatocele could be counted for another possibility of incidental 131I uptake despite an unclear mechanism.
Imtiaz Wani. [29] stated the following:
- Giant spermatocele of testis and spermatic cord as content of sac in an indirect hernia is very rare.
- Giant spermatoceles are congenital in nature.
Imtiaz Wani [29] reported a 61-year-old man who was diagnosed as a case of giant spermatocele. He underwent exploration of his scrotum which revealed a documented giant spermatocele and an indirect inguinal hernia of complete type with the testis, spermatic cord and spermatocele as a content of the hernia sac Excision of spermatocele with placement of cord outside sac was undertaken. Imtiaz Wani [29] stated that the reported case was the first kind of case report with new type of hernia reported with spermatic cord as content. Imtiaz Wani [29] made the following concluding iteration recommendations:
- Giant spermatocele should be excised.
- The testis and spermatic cord inside hernia sac have to be made extrasacal in order to prevent recurrence.
Fischer and Grantmyre. [30] evaluated the amount, motility, and viability of sperm within fluid which had been aspirated from naturally occurring spermatoceles and to investigate the effect of cryopreservation of sperm retrieved from spermatoceles. They took into consideration that assisted reproductive technologies had led to successful pregnancies and deliveries using sperm harvested from the epididymis and/or testis of infertile men. With regard to the methods of their study, Fischer and Grantmyre. [30] stated the following:
- Aspiration of spermatocele fluid and analysis of the fluid obtained was undertaken on 20 patients before they underwent elective spermatocelectomy.
- Randomly selected samples that totaled 5 were washed using a 70% Percoll gradient, and repeated semen analysis was undertaken.
- The washed specimens were cryopreserved within liquid nitrogen, and repeated semen analysis was undertaken upon the thawed specimens.
Fischer and Grantmyre. [30] summarized the results as follows:
- All spermatoceles that totaled 20 had viable sperm present that was noted to contain a count that ranged between 54 × 104 to 326 × 106 and 16 of them that amounted to 80% out of 20 contained motile sperm.
- The average percentage of motile sperm was 5% within the specimen.
- The average sperm motility and average percent viability of sperm that was recovered after Percoll gradient improved compared with sperm in the initial spermatocele aspirates that had a motility of 5%, and which had ranged from 0% to 25% and viability of 36%, and which had ranged from 2% to 91?fore Percoll versus. motility of 13%, which had ranged from between 2% to 38% and viability of 39%, which had ranged from 10% to 92?ter Percoll).
- Sperm which had been retrieved pursuant to cryopreservation had demonstrated reduced motility and viability; nevertheless, motile and viable sperm were recovered from all washed and cryopreserved samples.
- Fischer and Grantmyre. [30] made the ensuing conclusions:
- Their results had indicated that spermatocele fluid may contain sufficient numbers of sperm for use with assisted reproductive technologies.
- Motile and viable sperm could be recovered pursuant to cryopreservation and storage of sperm obtained from a spermatocele.
- Spermatocele fluid might be an additional source of sperm for the undertaking of assisted reproductive technologies.
- Koçak, et al. [31] undertook a study which was aimed t to determine the cellular contents and concentrations of interleukin 6 (IL-6), interleukin 8 (IL-8) and tumour necrosis factor alpha (TNF-α) within fluids of patients who had spermatocele or epididymal cyst. Koçak, et al. [31] included twenty-five symptomatic patients, 14 who had epididymal cysts and 11 who had spermatoceles in the study. Koçak, t al. [31] obtained fluids during surgical excision of the cysts and they stained cytological smears with May–Gruenwald–Giemsa to establish cell components. Koçak, et al. [31] measured the concentrations of IL-6, IL-8 and TNF-α by chemiluminescent immunometric assay. Koçak, et al. [31] summarized the results as follows:
- Cytological analysis of the fluids had demonstrated various sperm forms ranging from immature germ cells to degenerated spermatozoa without inflammatory cells such as neutrophils and macrophages.
- The concentrations (mean± SEM, pg/mg protein) of IL-6, IL-8 and TNF-α were reported to be 13.52 ± 1.40, 22.20 ± 2.43, 3.51 ± 1.43 in spermatocele fluids and 5.76 ± 0.48, 11.57 ± 1.89, 2.53 ± 0.41 in epididymal cyst fluids.
- Both IL-6 and IL-8 concentrations in the spermatocele group were noted to be higher than in the epididymal cyst group (P < 0.0001).
- No differences were found in TNF-α concentrations between the groups (P > 0.05).
- The findings had indicated that local production of pro-inflammatory cytokines is involved in cyst formation.
- The presence of immunology activation in these fluids does advocate a policy of selective surgical intervention in patients who have spermatocele or epididymal cyst.
Kauffman et al. [32] stated that a microsurgical approach to spermatocelectomy theoretically does minimize the risk of injury to the epididymis and testicular blood supply. Kauffman et al. [32] presented the technique of microsurgical spermatocelectomy and reported their perioperative and recurrence outcomes. With regard to the materials and methods of their study, Kauffman et al. [32] stated the following:
- In a 15-year period, 23 men who had a total of 36 epididymal cystic masses had undergone microsurgical resection with confirmation of spermatocele diagnosis by intraoperative identification of sperm in the cyst fluid.
- They reviewed pathology reports for resected epididymal tissue within the spermatocele specimen.
- The postoperative outcome measures included: complications, sperm count changes, improvement in pain and fertility, and recurrence of the cyst.
Kauffman et al. [32] summarized the results as follows:
• The mean sized of the spermatocele was noted to be 5.0 cm and the size of the spermatocele had ranged from 1cm to 15 cm.
- Common indications for the undertaking of the surgery included pain in 35% of cases, infertility in 30% and the 2 conditions in 13%.
- A total of 13 patients that amounted to 57% of the patients underwent simultaneous procedures for concomitant varicocele and/or hydrocele with a mean overall surgical time of 152 minutes.
- A single scrotal hematoma that was managed conservatively was the only postoperative complication.
- There was no case of infection noted.
- Avoidance of inadvertent epididymal resection was demonstrated by absent epididymal tissue in each of the 36 spermatocele pathology specimens.
- Also, no patient who had pre-operative and post-operative semen analyses available had experienced a decreased sperm count, which had confirmed the avoidance of iatrogenic epididymal tubule obstruction.
- At a mean follow-up of 17.3 months no man had recurrence of his epididymal cyst or testicular atrophy and all of the patients who had pre-operative pain had reported improvement.
- One patient who had pre-operative infertility had achieved pregnancy 12 months pursuant to his surgery.
Kauffman et al. [32] concluded that microsurgical spermatocelectomy is safe and effective and it is associated with a minimal risk of epididymal injury, testicular atrophy and recurrence.
Sista et al. [33] stated that doppler ultrasound scan is not commonly utilized in the evaluation of cystic lesions with internal echoes. Sista et al. [33] reported the use of the mechanical properties of color Doppler sonography to further characterize 3 spermatoceles.
With regard to the methods of their study, Sista et al. [33] reported the following:
- Three patients who had come to the University of California San Francisco Imaging Centre who had painless unilateral scrotal enlargement were evaluated with ultrasound scan and were found to have large spermatoceles.
- Colour Doppler ultrasound scan was applied to these spermatoceles, and digital video clips were obtained as the colour beam was instituted.
With regard to the results of their study, Sista et al. [33] reported that when colour Doppler sonography was applied to each spermatocele, the internal echoes had moved away from the transducer, resulting in an appearance similar to falling snow. Sista et al. [33] concluded that:
The “falling snow” sign can be utilized to enhance the diagnosis of a spermatocele as well as to evaluate a superficial cystic lesion with echogenic fluid and internal micro-debris which is difficult to distinguish from a solid mass.
Brockman et al. [34] described their contemporary experience with aspiration and sclerotherapy (AS) as a non-surgical alternative for patients with symptomatic hydrocele and spermatocele who prefer non-surgical treatment. With regard to the materials and methods of their study, Brockman et al. [34] stated the following:
- They had identified patients by billing diagnosis code for hydrocele or spermatocele from 2015 to 2019.
- The patients had undergone AS with doxycycline (200-400 mg).
- Clinical examination, ultrasound scan and aspirate microscopy were used to differentiate hydrocele from spermatocele.
- They had recorded baseline and follow-up data.
Brockman et al. [34] summarized the results as follows:
- In total, 65 patients had undergone AS, 54 out of 65 patients that amounted to 83% for hydrocele and 11 out of 65 patients that amounted to 17% of the patients for spermatocele with mean aspirate volumes 307 mL and a standard deviation (SD) of 238 mL, and 138 mL and standard deviation (SD) of 112 mL, respectively.
- Follow-up data was available for 38 out of 54 patients that amounted to 70% of the patients who had hydroceles and 8 out of 11 patients that amounted to 73% of the patients who had spermatoceles with median follow-up 28 months (IQR 23-41) and 22 months (IQR 18.5-30.5) months respectively.
- Relief of patient reported bother associated with scrotal size occurred in 29 out of 38 patients that amounted to 77% of the hydroceles and 8 out of 9 that amounted to 89% of the spermatoceles.
- Two out of fifty-four (2/54) patients that amounted to 4% of hydrocele patients developed hematoma that was managed with in-office aspiration.
- Immediate post-procedural pain had occurred in two out of fifty-six (2/56) hydroceles that amounted to 4% of hydroceles and two out of ten (2/10) spermatoceles that amounted to 20% of the spermatoceles.
- Post-procedural pain that required more than 5 tablets of hydrocodone/acetaminophen 5mg/325mg had occurred in two out of fifty-seven (2/57) hydroceles which amounted to 3% of hydroceles and two out of ten (2/10) spermatoceles that amounted to 20% of spermatoceles.
- Surgical repair was ultimately undertaken in 3 out of 38 patients that amounted to 8% of patients and one out of nine (1/9) patients that amounted to eleven percent (11%) of patients who had persistent hydrocele and spermatocele respectively.
- Brockman et al. [34] concluded that AS is a safe and effective alternative treatment option for hydrocele and spermatocele for patients wishing to avoid surgery.
- Gupta et al. [35] stated the following:
- A spermatocele is a cystic cavity that is filled with fluid and spermatozoa probably due to an acquired or congenital partial obstruction of the spermatic ducts.
- Spermatoceles usually tend to be asymptomatic, single and small in size.
- Occasionally, a spermatocele might become large enough to bother the patient; differential diagnoses to be then considered with regard to spermatoceles include: accessory testis, epididymal cyst, encysted hydrocele of cord or tumour.
- Surgical intervention should be considered if symptoms such as persistent disturbing pain or discomfort to patient are the manifestations.
- They were reporting a 35-year-old-man who had giant symptomatic spermatocele with a brief review of literature.
- Gupta et al. [35] reported a 35-year-old adult man who had manifested in the surgical outpatient clinic with complaint of left sided scrotal swelling which was separate from his ipsilateral testis since childhood. He stated that over the preceding 5 years, the swelling had gradually progressively got bigger in size of about 5 cm x 4 cm in his left hemi-scrotum. He had complained of dragging sensation, soreness and even sometimes stretching pain within his left inguinoscrotal region while standing or during his abdominal straining. The discomfort had become more evident within the preceding six months. During his clinical examination, an ovoid, soft cystic swelling was found palpable without tenderness within the upper part of his left hemi-scrotum scrotum (see figure 1). The swelling was located superior and posterior to his left testis separately and it had extended over his spermatic cord. He had transillumination test which was negative. He did not have any history of trauma, infection, or inguinoscrotal operation, including vasectomy. The results of his complete blood count and biochemical examinations were normal. He had an ultrasound scan of the scrotum which revealed a cyst that measured 2.1 cm X 3.6 cm X 4.8 cm along his left spermatic cord which was eccentric to his ipsilateral testis and epididymis that was considered to be likely suggestive of an encysted hydrocele of cord (see figure 2).
- Based upon a clinical diagnosis of encysted hydrocele of cord and/or a testicular mass, surgical exploration was undertaken via a left scrotal approach. A single cystic mass was identified from the spermatic cord to the head of his epididymis that simulated an accessory testis. By undertaking blunt dissection, the cystic mass was separated gently from the spermatic cord and body of the epididymis (see figure 3), and it was then successfully and completely excised. The plane between the mass and epididymis was clear and the epididymis was preserved. The mass did appear to be a Unilateral Giant Spermatocele Mimicking Accessory Testis and to be be unilocular as well as arising from his epididymal body. The size of the mass was 5 cm × 4 cm × 0.5 cm. The aspirated fluid was noted to be barley coloured. The spermatocele was excised and ligated at the junction of his epididymis and testis. The testis and epididymis were replaced within his scrotum and his surgical incision wound was closed in layers. His post-operative period was uneventful. See figure 3 which has illustrated the Intra-Operative Image Showing Left Giant Spermatocele Mimicking Accessory Testis. Microscopy pathology examination of the fluid demonstrated numerous spermatozoa, most of which were noted to be immobile. Histopathology examination of the specimen demonstrated a cyst which was lined by cuboidal to columnar epithelium with few spermatozoa within the lumen and fibro-collagenous wall of cyst features that were indicative of Spermatocele (see figure 4).
- Gupta et al. [35] made the ensuing summating discussion:
- The terminology ‘spermatocele’ was utilized in 1785 by Guerin.
- It has been pointed out that giant spermatocele is an uncommon clinical entity and which usually manifests as a slowly growing painless unilocular swelling. [36]
- Spermatoceles are the sperm-containing cystic dilatations of the efferent ductules within the head of the epididymis.
- Less commonly, spermatoceles are dilatations of the tubules of the rete testis or aberrant ducts. [37]
- In view of the fact that majority of spermatoceles tend to be painless and measure less than 1 cm with regard to diameter, they tend to be overlooked. [38]
- Therefore, the number of reported cases of spermatocele is small and their true incidence had remained unknown. Nevertheless, spermatoceles could sometimes be large enough to so as to cause discomfort when the individuals are walking or when the patients cross their legs.
- Spermatoceles are fairly common in view of the act that they are incidental findings in about 30% of men who have undergone ultrasound scan of the testes for other reasons.
- Spermatoceles usually tend to be encountered within the fourth and fifth decades of life in men. [40].
- The exact aetiology of spermatocele remains unclear
- The aetiology-pathogenesis of spermatocele is considered to be idiopathic; however, a spermatocele might be congenital origin or emanates ensuing epididymitis, trauma, inguinal-scrotal surgery or vasectomy, these leading to scarring, obstruction of proximal efferent ducts and might form a spermatocele. [9]
- It has been pointed out that males whose mothers had undergone treatment with diethyl-stilbestrol (DES) during their pregnancy in order to prevent miscarriage and other pregnancy complications do have an increased risk for the occurrence of spermatocele.
- According to the postulate of Itoh et al, [40] spermatoceles do represent proximal dilation ensuing an obstruction of the efferent ducts, possibly they are caused by the shedding of senile seminiferous epithelium. This shedding does occur normally throughout life; however, the cells might accumulate and cause a blockage in older men, which might explain why the incidence of spermatoceles tends to increase with age.
- Majority of spermatoceles, as in their reported case, have a single simple cyst.
- In view of a high association spermatocele with tubular ectasia of rete testis, multilocular cysts are postulated to be derived from the histological structure of the rete testis, forming irregular anastomosing spaces arising from the tubuli recti [20].
- More commonly, ultrasound scan is undertaken to confirm the diagnosis of spermatocele.
- Ultrasound of scrotal contents usually demonstrates well-defined hypoechoic lesions that generally measure from 1 cm to 2 cm in size with posterior acoustic enhancement. [41]
- It has been pointed out that spermatoceles should be differentiated from hydroceles, varicoceles, epididymal cysts, infection or tumours. [42]
- A spermatocele often tends to lie on the posterolateral border of the testis and does not fluctuate in size upon provocative manoeuvre. [43]
- Urinalysis is indicated in order to exclude genitourinary tract infection.
- Demonstration of sperm within cystic fluid could differentiate it from an epididymal cyst.
- Furthermore, other uncommon conditions may be taken into consideration. Chronic epididymitis is speculated Unilateral Giant Spermatocele Mimicking Accessory Testis to trigger secondary neoplastic epithelial changes within rete testis adenocarcinoma, and might have similar manifestation as a typical spermatocele. [44]
- Torsion of a spermatocele, which is uncommon, often does tend to cause severe scrotal pain and does require the undertaking of surgical intervention. [45]
- Majority of spermatoceles do not require any treatment.
- Spermatocele that become large, spermatoceles that cause bothersome discomfort, or spermatoceles that are difficult to differentiate from neoplasm could be surgically excised.
- Definite diagnosis of a giant spermatocele is difficult to establish based upon the undertaking of history and clinical examination alone.
- In their reported case, surgical exploration was recommended.
- Gupta et al. [35] made the ensuing conclusions:
- They would recommend that such a huge and symptomatic spermatocele should be excised in order to relieve the symptoms of patients.
- Available literature had revealed only individual case reports wherein the spermatoceles had manifested with clinical scenarios simulating malignant/ benign testicular/para-testicular lesions [36] [37] [38] [9] [42] [44]
- Basar et al had reported a case of primary bilateral spermatocele in 2003. [36]
- Multilocular spermatocele had been reported by Matsuoka et al, Yagi et al and Lee et al in individual case reports. [20] [43] [46]
- Jassie et al [45] had reported torsion in giant spermatocele. [45]
Figure 1: Clinical Image with Left Scrotal Swelling Separate from The Ipsilateral Testis. Reproduced from [47] Under the Creative Commons Attribution License. or with permission to re-use provided the original author is cited.

Figure 1: Clinical Image with Left Scrotal Swelling Separate from The Ipsilateral Testis.
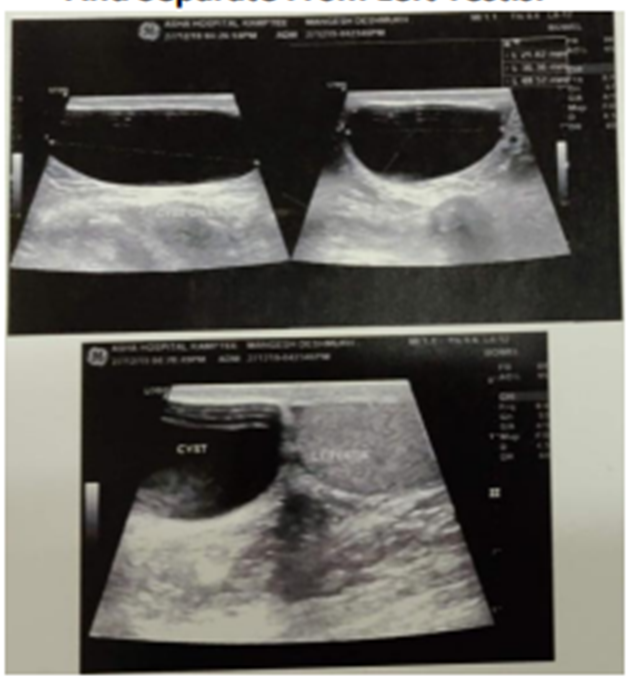
Figure 2: Ultrasound of Left Testis Suggesting Cyst in Association with Left Spermatic Cord and Separate from Left Testis. Reproduced from [47] Under the Creative Commons Attribution License or with permission to re-use provided the original author is cited.

Figure 3: The Intra-Operative Image Showing Left Giant Spermatocele Mimicking Accessory Testis. Reproduced from [47] Under the Creative Commons Attribution License or with permission to re-use provided the original author is cited.
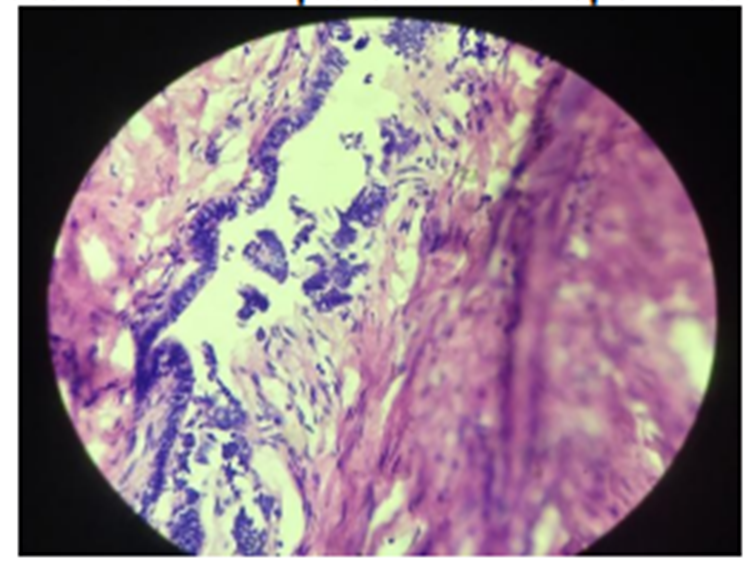
Figure 4: Histopathological Image Showing Ciliated Columnar Epithelium with Spermatozoa Reproduced from [47] Under the Creative Commons Attribution License or with permission to re-use provided the original author is cited.
Reddy Ravindranath [47] reported a 45-year-old man who had presented as part of his infertility evaluation with pain and heaviness within his left hemi-scrotum and this was identified via clinical examination as varicocele with typical “bag of worms” appearance. The diagnosis of varicocele was confirmed pursuant to the undertaking of high-resolution color-flow Doppler ultrasound scan, which had demonstrated dilatation of the vessels of the pampiniform plexus, typically which were greater than 3 mm in diameter (see figure 5). Incidentally, a well-defined ipsilateral intra-testicular cystic lesion was demonstrated that measured 9 mm × 10 mm with irregular walls and fine low-level internal echoes lying adjacent to the mediastinum testis (see figure 6). The laboratory blood test results of the patient demonstrated negativity for tumour markers alpha-fetoprotein, beta-human chorionic gonadotropin, as well as for lactate dehydrogenase. Their positivity could have indicated an underlying germ cell tumour of the testis. Based upon the aforementioned findings, a diagnosis of left-sided varicocele with contemporaneous concomitant intratesticular spermatocele was made. He underwent trans-inguinal exploration of his scrotum and frozen section examination of specimen of his lesion was undertaken, and examination of frozen sections helped in confirming that the cystic lesion was an intratesticular spermatocele with mature spermatozoa as its contents. Reddy Ravindranath [47] stated the following:
- A varicocele is an abnormal dilatation and enlargement of the scrotal venous pampiniform plexus which drains blood from each testicle.
- Varicoceles are far more common on the left side of the scrotum which does account for 80% to 90% of cases of varicoceles.
- If a left varicocele is identified, there is a 30% to 40% probability; it is a bilateral condition.
- The ultrasound scan findings of varicocele include multiple anechoic, serpiginous, and tubular structures of varying sizes.
- Spermatocele is a terminology that refers to an intra-parenchymatous cystic lesion that is adjacent to the mediastinum testis, within the area of rete testis, and it may be septate and communicating with seminiferous tubules.
- Pathogenesis of simple cysts could be elaborated under two main types: an infant type which is caused by congenital anomaly which arises from the remnants of the Mullerian and Wolffian ducts, and an adult type, which is caused by trauma or infection, where it is understood or has been postulated that an infective process might cause occlusion of the draining ducts which emanates into the development of a cystic tumour-like lesion.
- The exact cause of spermatoceles has remained unclear but it has been conjectured to be due to blockage of the epididymal ducts with proximal dilatation. This could be idiopathic or secondary to an infectious or inflammatory process.
- An intra-testicular spermatocele does communicate with the seminiferous tubules, whereas simple ectasia of the rete testis does not do so directly.
- Doppler ultrasound scanning and gray-scale ultrasonography are effective methods that are utilized in the diagnosis of varicocele and intratesticular spermatocele.
- During the ultrasonography examination, spermatoceles tend to be depicted as well-defined epididymal hypoechoic lesions and demonstrating posterior acoustic enhancement with irregular walls, fine low-level internal echoes, and sometimes septations.
- Radiology imaging differential diagnosis considerations of scrotal masses include: testicular tumours, hydatid cyst of morgagni, epidermoid cyst, cysts of tunica albuginea, epididymal cyst, hydrocele, and spermatocele.
- Unlike epididymal cysts, spermatoceles often contain low-level echogenic proteinaceous fluid and spermatozoa and could septate.
- Intra-testicular spermatocele does communicate with the seminiferous tubules; nevertheless, ectatic rete testes do not tend to communicate directly.
- Simple cysts are usually smooth walled and anechoic, while spermatoceles exhibit or demonstrate irregular wall with low-level echoes.
- Spermatoceles tend typically to be asymptomatic and they usually do not tend to require treatment.
- Spermatoceles seek intervention when the lesion approximates the size of a testis. Specific characteristics of spermatoceles include the individual's age, duration of diagnosis, symptom type, and symptom duration.
- The location of these benign cysts within the area of the mediastinum and rete testis and the absence of signs of a germ cell tumour might permit testis preservation.
- With regard to spermatoceles, intervention could be considered for uncomfortable, painful, or progressively enlarging spermatoceles.
- The treatment choices for spermatocele could include the following options: radical orchidectomy, enucleation of the cysts with testicular parenchyma preservation, or conservative surveillance by ultrasound scanning.
- Benign testicular cysts which appear to arise from the intratesticular ducts of the mediastinum and rete testis could be identified with confidence with utilization of a high-resolution ultrasound scan.
- A cystic intratesticular lesion that is adjacent to the mediastinum testis and which demonstrates communication with the seminiferous tubules is most likely a spermatocele.
- There were previously reported cases of intratesticular varicocele with extra-testicular varicocele. Nevertheless, contemporaneously concomitant presence of spermatocele with ipsilateral varicocele is a rare entity which had been reported in the current case report.
- Coexistent ipsilateral intratesticular spermatocele with varicocele though it is rare or uncommon it could very well be a possibility.
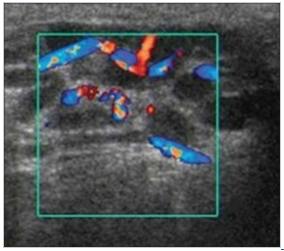
Figure 5: High-resolution color-flow Doppler ultrasound image demonstrating varicocele surrounding the left testis. Reproduced from: [47] under the Creative Commons Agreement Attribution Licence.
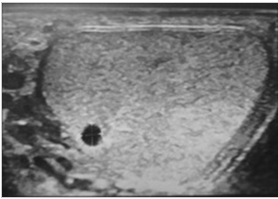
Figure 6: High-resolution ultrasound image demonstrating a well-defined intratesticular cystic lesion with irregular walls and fine low-level internal echoes lying adjacent to the mediastinum testis. Reproduced from: [47] under the Creative Commons Agreement.
Attribution Licence.
MZYIENE et al. [48] stated the following:
- Spermatocele is a fluid-filled cyst which develops at the head of the epididymis.
- The fluid usually tends to be a clear or milky white colour fluid that may contain sperm. [49]
- The clinical presentations of small size spermatocele is sometimes asymptomatic, spermatocele could also grow over time and become troublesome, even painful, requiring surgical management.
- They had reported the case of a spermatocele is a 42-year-old man who had manifested with a scrotal pain of progressive occurrence, having required surgical management with a review of the literature on this pathology. [9]
MZYIENE et al. [48] reported a 42-year-old man who did not have any particular pathological history, and who was married and who was a father of two children who had developed unilateral testicular swelling of progressive evolvement over the preceding 4 years, which had been increasing in size, and becoming painful. During the physical examination of the patient, there was evidence of increased bursary, and volume noted. His right testis was of normal appearance and on the left, and there was an aspect of left hydrocele that was associated with a positive Trans-illumination. The result of his sperm analysis was normal. He had ultrasound scan of his testes and scrotal contents and both of his testes were found to be of normal size that measured 17.1ml for the right testis and 23.2ml for the left testis. His right epididymis looked normal. On the ultrasound scan of his testes, there was evidence of presence of a large left epididymis cyst with thin wall, with an echogenic content, that had measured 69 mm x 36mm in diameter. Bilateral hydrocele of low abundance was also noted. There was no evidence of visible varicocele noted in the ultrasound scan. In front of the functional gene and the patient’s complaints, surgery was regarded as indicated. He underwent his surgical operation under spinal anaesthesia. He had an ipsilateral incision on the left side of scrotum with his testis used as a log, dissection of the different scrotal envelopes was undertaken and upon the scrotal content exploration was noted a fluid cyst located upon the top of the testis, epididymis and extending to the spermatic cord (see figure 7A). No hydrocele blade was found as was mentioned in the ultrasound scan report. His surgical procedure entailed excision of the cyst (see figure 7B) without damaging the spermatic cord and maintaining the integrity of the testis. Plane-by-plane closure of the scrotum was undertaken pursuant to reintroduction of the scrotal contents in place. The excised specimen was for pathology examination and the features of the pathology examination findings were in adjudged to be consistent with a cystic partitioning contained spermatic fluid associated with spermatic cells. The diagnosis was therefore confirmed to be that of a rare giant spermatocele. MZYIENE et al. [48] made the ensuing summating
Discussions:
- The name "spermatocele" has originated from Guerin 1785 who had discovered the spermatocele.
- Spermatocele has been designated as a pathology of insidious onset and slow, painless, and unilateral growth.
- With regard to the aetiologically of spermatocele, many scenarios could explain its occurrence in that it is known that a spermatocele can develop after trauma, infectious damage to the testis, inguinoscrotal surgery, and vasectomy, and it can also be an idiopathic cause.
- According to the known postulate, the occurrence of spermatocele might be due to an obstruction of the efferent ducts emanating in proximal dilatation by seminiferous excretions accumulating throughout life.
- Spermatocele would therefore be a cystic accumulation of semen, which occurs from puberty, and most often is revealed within the fourth and fifth decades in human beings.
- The age range of onset of the cystic lesions is between 65 years and 74 years.
- Spermatocele usually manifests around the age of 65 years according to the epidemiological study by Karl-Johan Lundström. [1]
- In their case reported, the age of the patient was 42 years.
- With regard to the case report of Hsin-Chih Yeh, the patient was 55 years old.
- The development of spermatocele is usually an incipient evolution not entailing any complaint and small size lesion is seen.
- With regard to their reported case, the patient’s lesion had progressed over 4 years, and it had gradually increased in volume until it became uncomfortable for him.
- It is important to distinguish a spermatocele from other testicular diseases including: hydrocele, epididymal cysts, and testicular tumours.
- The evidence of spermatozoids within the cystic fluid makes it possible to differentiate it from an epididymal cyst, in addition, the spermatocele develops upon the posterior side of the testis.
- Usually, the difference between an epididymis cyst and a spermatocele is at the waist level so the epididymis cystic masses that are greater than 2 cm are usually called or referred to as spermatoceles. [27] [49]
- With regard to the management of this condition, there is still no clear codification for this.
- It has been stated that majority of sperm cells do not require treatment if they are not bothersome to the patient. [50]
- Sclerotherapy of spermatocele is more effective, simple to achieve with few complications and good cost-effectiveness and could be undertaken especially in patients with fertility disorders.
- In the case of their reported patient, they had undertaken surgical removal of the spermatocele, their patient did not require paternity and he had already had two children. His sperm analysis before the surgery was normal. [27]
- MZYIENE et al. [48] made the ensuing conclusions:
- Spermatocele is a relatively uncommon cystic disease of the testis.
- Spermatocele is usually small in size, asymptomatic and evolutionary average.
- The localization a spermatocele and the contents of the cyst does make the difference with epididymis cysts.
- The management of spermatocele varies depending upon its impact on the patient. It is important to think of a spermatocele in front of a cystic condition of the testis of more than 2cm in size.
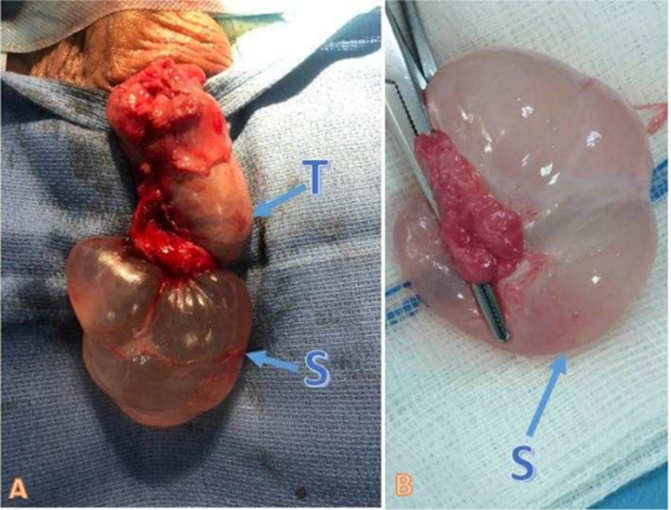
Figure 7: Spermatoccele 7A: Intra-Operative-Image Showing Left Giant Spermatocele (S) On The insertion of the testicular head (T) 7B: an image of spermatocele fluid. Reproduced from: [48] Under the Creative Commons Attribution License.
Chan et al. [51] stated the following:
- Utilization of ketamine is associated with lower urinary tract symptoms (LUTS), functional deficits as well as structural changes.
- These had been first reported in a case series in 2007 by Chu et al. [52] and similar positive associations had also been reported in other studies.
- Ketamine was once the most common recreational drug in Hong Kong.
- Recent data had shown that use of Ketamine is on a decreasing trend and it has been superseded by methamphetamine. [53]
- Nevertheless, the urological complications of ketamine could persist and this group of populations still require ongoing care for their symptoms.
Chan et al. [51] reported a 37 years old man who had a history of ketamine abuse, renal impairment, hypertension and HCV hepatitis, who had manifested to them with insidious onset of painful his scrotal swelling after he had undergone prostate preserving cystectomy. Chan et al. [51] reported that the patient had commenced abuse of ketamine since he was 18 years old. He first manifested with visible haematuria at the age of 24 years, and he was later diagnosed to have ketamine cystitis. He underwent computed tomography (CT) scan as well as intravenous urogram (IVU) examination which had demonstrated bilateral hydronephrosis with bilateral full-length strictures from his uretero-pelvic junction to his vesicoureteric junction. There was also thickening of his anterior urinary bladder wall in his radiology images and a 1.5cm polypoid urinary bladder lesion. He underwent cystoscopy as well as biopsy of the urinary bladder polyp and pathology examination of the biopsy specimen demonstrated granulosa pyogenicum. He had Video-urodynamic study which had demonstrated 140 ml of urinary bladder capacity with detrusor overactivity. When he was aged 33 years, he was admitted due to septic shock related to pyonephrosis with acute on chronic kidney failure. He then underwent insertion of bilateral percutaneous nephrostomy. Following the control of his sepsis, he had antegrade pyelogram which had demonstrated smooth strictures at both of his ureteropelvic junctions. Despite having undergone urinary diversion by the insertion of bilateral per-cutaneous nephrostomy, the patient subsequently had developed progressive kidney failure and had required permanent haemodialysis. Bilateral trans-peritoneal nephrectomy was undertaken when he was 34 years old. Nevertheless, the patient was then admitted repeatedly due to his subsequent development of pyocystitis and for which he underwent insertion of supra-pubic cystostomy for drainage due to him having developed pan-urethral stricture. In view of patient's age and future fertility issue, he underwent prostate and seminal vesicle preserving cystectomy 1 year subsequently. His post-operative erectile function was maintained.
On follow up approximately 1 year after cystectomy, he complained of insidious onset of painful scrotal swelling, and the pain was noted to be worse following nocturnal tumescence and had persisted for a few days. His clinical examination revealed bilateral gross scrotal swelling of more than 10cm, both of his testes were palpable anterior to his tense scrotal swelling (see figure 8). He underwent ultrasound scan of his scrotal contents which demonstrated grossly distended scrotum which was filled with fluid. He had magnetic resonance imaging (MRI) scan of his scrotum and scrotal contents which demonstrated a 13.5 cm × 16.8 cm × 17.5 cm scrotal sac which had communication with his penile urethra at the root of his penis which was indicative of a urethra-scrotal fistula (see figure 9).

Figure 8: Large firm left scrotal swelling. Reproduced from: [51] under the Creative Commons Attribution Agreement Licences with Elsevier Under a Creative Commons licenseopen access
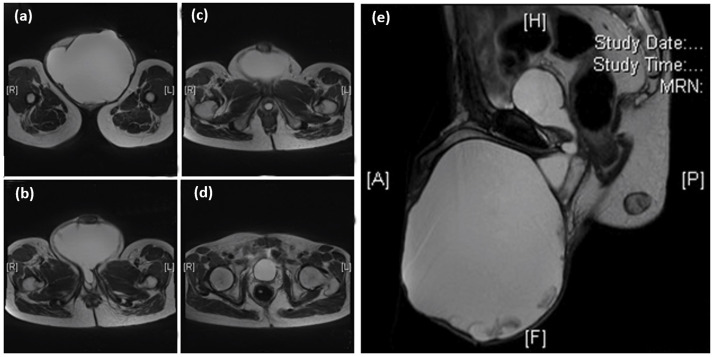
Figure 9: MRI T2 phase of scrotal and pelvis showing 13.5 × 16.8 × 17.5cm scrotal sac filled with fluid showing communication with the penile urethra at the root of penis, the prostate and seminal vesicles were not well seen. Transverse planes at: (a) lower scrotum; (b) & (c) level of the bulbous urethra; (d) base of the remnant bladder; (e) sagittal plane of pelvis and scrotum. Reproduced from [51] under The Creative Commons Attribution License.
He underwent exploration of his scrotum with cystoscopy and a huge scrotum with collection inside was found which had displaced both of his testes laterally (see figure 10), Two and half (2.5) Litres of brownish fluid was drained out. The collection cavity was found to be connected to a well-formed fistula tract leading to the verumontanum and then via his urinary bladder neck to a cavity that was lined by transitional epithelium simulating urinary bladder cavity. The urethral lumen distal to the verumontanum was noted to be blind-ended. Drainage was undertaken.
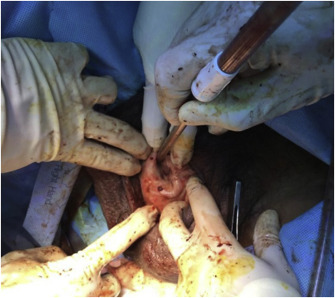
Figure 10: Exploration of scrotum found a huge scrotal collection displacing bilateral, testes laterally. 2.5 L of brownish fluid was drained. Percutaneous drainage was performed. Reproduced from [51] under the Creative Commons Attribution license
Chan et al. [51] made the ensuing summating discussions:
- Their reported case report had demonstrated a urinary tract complication which had previously never been reported in patients who had chronic ketamine utilization.
- Their reported patient had suffered from complications which had involved most of his urinary tract from pyonephrosis, ureteric strictures, pyocystitis, urinary bladder contractures and urethral strictures.
- Despite bilateral nephrectomy, partial cystectomy, he was also found to have a large spermatocele.
- It was postulated that the cause of his spermatocele was likely from urethral stricture with the back flow pressure of ejaculates causing a fistula tract which had led to his scrotum.
- Even though causes of urethral strictures could be iatrogenic, traumatic or infective, the patient did not have any history of such insults and he did not have any complaints of urethral discharge. Therefore, his urethral stricture thought to be likely related to the ketamine irritation.
- The effectiveness of various ketamine uropathy treatment had still remained lacking.
- The mainstream treatment of ketamine cystitis was pain control.
- Instillation of intravesical pentosan polysulphate, which is a heparin like compound, had shown effectiveness in symptoms that relieve the condition and is proposed to protect and assist repairing of the polyglycan layer of the damaged urothelium. [54]
- With regard to cases that are refractory to medication, hydro-distension with or without botulinum toxin injection were undertaken for improvement of urinary bladder capacity as well as for relief of symptoms. [55]
- With regard to surgical intervention, urinary tract strictures had been relieved by drainage with utilization of ureteric stents or insertion of per-cutaneous nephrostomy.
- Selected cases may be treated by the undertaking of augmentation cystoplasty and subtotal cystoplasty, [54] but case series of augmentation cystoplasty in refractory patients had shown deterioration of the symptoms and/or renal function, which was considered could be due to resumption of ketamine use, causing further damage of the urinary tract. [56]
- At the time of publication of their article, there had been no guidelines, and treatment strategy had been based upon individual symptoms, multidisciplinary team involving urologist, physician, psychiatrist and social worker should work together to provide all-rounded services to ensure the best outcome for the patients.
Chan et al. [51] made the ensuing conclusions:
- Ketamine had once been the commonest abused drugs within Hong Kong, despite the efforts of drug cessation regimens and education, a group of patients still suffer from urinary tract complications of Ketamine use.
- Their reported case report had demonstrated multiple complications on the urinary tract in a patient with chronic ketamine use and a rarely seen complication of large spermatocele with urethroscrotal fistula probably due to urinary tract strictures.
- Symptoms based multidisciplinary treatment approach is necessary for the care of this minority group.
Sisodiya et al. [57] reported a 10-year-old male child who had presented with gradually progressive swelling within his right scrotum, on and off pain within it over the preceding 8 months. He did not have any history of trauma to his scrotum/fever/ pyuria/pain in his abdomen. His clinical examination which demonstrated about a 1 cm × 1 cm trans illuminate, non-reducible, cystic mass within his right spermatic cord just above the testis. He had ultrasound scan of his testes and scrotal contents which showed a cystic mass behind and above the testis. He underwent surgical exploration as child due to his being symptomatic, there was evidence of the finding of a 1 cm × 8 mm size cystic mass that was attached with head of his epididymis (see figures 11 and 12). Complete excision of mass was undertaken. Pathology examination of the excised specimen demonstrated a spermatocele. Sisodiya et al. [57] stated the following:
- Spermatocele (epididymal cyst) in children is a rare cause of scrotal swelling. [17]
- The usual treatment of spermatocele has tended to be conservative management with serial follow up. [4] [58] [59]
- Surgical excision of the spermatocele should be considered when the spermatocele is symptomatic, not involuting with time or has developed complication like torsion [4] [58] [59]

Figure 11: Reproduced from: [58] Cystic mass (blue arrow) attached with head of epididymis.

Figure 12: Post of specimen cystic mass. Reproduced from: [57] Under the Creative Commons Attribution Agreement License.
Conclusions
Conflict Of Interest – None
Acknowledgements to:
- National Journal of Integrative Research in Medicine for granting permission for reproduction of figures and contents of their article under the Creative Commons Attribution Agreement License.Statement from the journal website stated the following:
- This is an Open access Journal (which means that all content is freely available without charge to the user or his/her institution. Users are allowed to read, download, copy, distribute, print, search, or link to the full texts of the articles, or use them for any other lawful purpose, without asking prior permission from the publisher or the author. This is in accordance with the BOAI definition of open access) "publication of Association of Health Professionals and Health Educators"
- Journal of Medical Ultrasound and Wolters Kluwer Medknow Publication: for granting permission for reproduction of figures and contents of their article under the Creative Commons Attribution Agreement License.
- Statements from Journal of Medical Ultrasound include:
- Copyright : © 2018 Journal of Medical Ultrasound
- This is an open access journal, and articles are distributed under the terms of the Creative Commons Attribution-Non-Commercial-ShareAlike 4.0 License, which allows others to remix, tweak, and build upon the work non-commercially, as long as appropriate credit is given and the new creations are licensed under the identical terms.
- Urology Case Reports and Elsevier for granting permission for reproduction of figures and contents of their article under the Creative Commons Attribution Agreement License. The Copy right iterations of Urology Case Reports and Elsevier include:
- Creative Commons Attribution (CC BY): lets others distribute and copy the article, to create extracts, abstracts, and other revised versions, adaptations or derivative works of or from an article (such as a translation), to include in a collective work (such as an anthology), to text or data mine the article, even for commercial purposes, as long as they credit the author(s), do not represent the author as endorsing their adaptation of the article, and do not modify the article in such a way as to damage the author's honour or reputation.
- Creative Commons Attribution-Non-Commercial-NoDerivs (CC BY-NC-ND): for non-commercial purposes, lets others distribute and copy the article, and to include in a collective work (such as an anthology), as long as they credit the author(s) and provided they do not alter or modify the article.
- International Journal of Collaborative Research on Internal Medicine & Public Health and I Med Publications, for granting permission for reproduction of figures and contents of their article under Copy Right: Copy Right ©2023; All rights Reserved. iMed Pub Ltd. A Creative Commons Attribution 4.0 International Agreement License.
References
- Lundström KJ, Söderström L, Jernow H, Stattin P, Nordin P. (2019). Epidemiology of hydrocele and spermatocele; incidence, treatment and complications. Scand J Urol.;53(2-3):134-138.
View at Publisher | View at Google Scholar - Patton A, Parwani A. (2003). Spermatocele.
View at Publisher | View at Google Scholar - Herbert V, Fong W, Gulle V, Stopler T. (1990). Low holotranscobalamin II is the earliest serum marker for subnormal vitamin B12 (cobalamin) absorption in patients with AIDS. Am J Hematol.;34(2):132-1139.
View at Publisher | View at Google Scholar - Erikci V, Hoşgör M, Aksoy N, Okur Ö, Yildiz M, et al. (2013). Management of epididymal cysts in childhood. J Pediatr Surg.;48(10):2153-2156.
View at Publisher | View at Google Scholar - Smart JM, Jackson EK, Redman SL, Rutherford EE, Dewbury KC. (2008). Ultrasound findings of masses of the paratesticular space. Clin Radiol.;63(8):929-938.
View at Publisher | View at Google Scholar - Chen F, Cernigliaro J, Desai M, Bhatt S. (2020). The
View at Publisher | View at Google Scholar - Hikosaka A, Iwase Y. (2008). Spermatocele presenting as acute scrotum. Urol J.;5(3):206-208.
View at Publisher | View at Google Scholar - Sakuma T, Mori M, Kokubo C. (2019). Spermatocytes observed in the fine needle aspirate of spermatocele of the scrotum. Case report and review of the literature. Diagn Cytopathol.;47(9):972-974.
View at Publisher | View at Google Scholar - Yeh HC, Wang CJ, Liu CC, Wu WJ, Chou YH, et al. (2007). Giant spermatocele mimicking hydrocele: a case report. Kaohsiung J Med Sci.;23(7):366-369.
View at Publisher | View at Google Scholar - Ejeckam GC, Govatsos S, Lewis AS. (1984). Cyst of seminal vesicle associated with ipsilateral renal agenesis. Urology.;24(4):372-374.
View at Publisher | View at Google Scholar - Castelino-Prabhu S, Ali SZ. (2010). Spermiophages in a giant spermatocele. Diagn Cytopathol.;38(11):816-817.
View at Publisher | View at Google Scholar - Palacios J, Regadera J, Paniagua R, Gamallo C, Nistal M. (1993). Immunohistochemistry of the human ductus epididymis. Anat Rec.;235(4):560-566.
View at Publisher | View at Google Scholar - Terada T. (2011). Immunohistochemical profile of normal mesothelium and histiocytic/methothelial hyperplasia: a case report. Int J Clin Exp Pathol.;4(6):631-636.
View at Publisher | View at Google Scholar - Paluru S, Ulbright TM, Amin M, Montironi R, Epstein JI. (2018). The Morphologic Spectrum of Sertoliform Cystadenoma of the Rete Testis: A Series of 15 Cases. Am J Surg Pathol.;42(2):141-149.
View at Publisher | View at Google Scholar - Mahlknecht A, Mahlknecht P, Fallaha M, Wieser A. (2015). Tubular ectasia of the rete testis (TERT). Differential diagnosis of cystic testicular disorders. Arch Ital Urol. Androl.;87(1):5-7.
View at Publisher | View at Google Scholar - Shah VS, Nepple KG, Lee DK. (2014). Routine pathology evaluation of hydrocele and spermatocele specimens is associated with significant costs and no identifiable benefit. J Urol;192(4):1179-1182.
View at Publisher | View at Google Scholar - Ameli M, Boroumand-Noughabi S, Gholami-Mahtaj L. (2015). A 14-Year-Old Boy with Torsion of the Epididymal Cyst. Case Rep Urol; 2015:731987.
View at Publisher | View at Google Scholar - Choyke PL, Glenn GM, Wagner JP, Lubensky IA, Thakore K, et al. (1997). Epididymal cystadenomas in von Hippel-Lindau disease. Urology.;49(6):926-931
View at Publisher | View at Google Scholar - Jahnson S, Sandblom D, Holmäng S. (2011). A Randomized Trial Comparing 2 Doses of Polidocanol Sclerotherapy for Hydrocele or Spermatocele. The Journal of Urology.; 186(4): 1319-1323.
View at Publisher | View at Google Scholar - Yagi, H., Igawa, M., Shiina, H. et al. (2001). Multilocular spermatocele: A case report. Int Urol. Nephrol.; 32: 413–416.
View at Publisher | View at Google Scholar - Walsh T J, Seeger K T, Turek P J. (2007). Spermatoceles in adults: when does size matter? Arch Androl. ;53(6):345-348.
View at Publisher | View at Google Scholar - Weil AJ, Rodenburg JM. (1960). Immunological differentiation of human testicular (spermatocele) and seminal spermatozoa. Proceedings of the Society for Experimental Biology and Medicine.;105(1):43-45.
View at Publisher | View at Google Scholar - Takimoto K, Okamoto K, Wakabayashi Y Okada Y. Torsion of Spermatocele: A Rare Manifestation Urol. Int. 2002; 69 (2): 164–165.
View at Publisher | View at Google Scholar - Basar H, Baydar S, Boyunaga H, Batislam E, Basar M M, et al. (2003). Primary bilateral spermatocele. International Journal of Urology.; 10: 59 -61
View at Publisher | View at Google Scholar - Jimenez Cruz J F. (1980). Artificial Spermatocele. The Journal of Urology.; 123(6): 885-886.
View at Publisher | View at Google Scholar - Low LS, Nair SM, Davies AJW, Akapita T, Holmes MA. (2020). Aspiration and sclerotherapy of hydroceles and spermatoceles/epididymal cysts with 100% alcohol. ANZ J Surg.;90(1-2):57-61.
View at Publisher | View at Google Scholar - Dollard DJ, Fobia JB. (2011). Extra scrotal spermatocele causing lower abdominal pain: a first case report. Am J Emerg Med.;29(3): 358.e7-9.
View at Publisher | View at Google Scholar - Albano D, Motta F, Baronchelli C, Lucchini S, Bertagna F. (2017). 131I Whole-Body Scan Incidental Uptake Due to Spermatocele. Clin Nucl Med.;42(11):901-904.
View at Publisher | View at Google Scholar - Imtiaz Wani. (2018). Hernia with spermatocele, cord and testis inside sac: Case report, International Journal of Surgery Case Reports.; 53: 397-399.
View at Publisher | View at Google Scholar - M.A Fischer, J.E Grantmyre, (2003). Retrieval and cryopreservation of sperm from spermatocele fluid, Urology. 61(2): 417-420.
View at Publisher | View at Google Scholar - https://scholar.google.com/scholar?hl=en&as_sdt=0%2C5&q=M.A+Fischer%2C+J.E+Grantmyre%2C+%282003%29.+Retrieval+and+cryopreservation+of+sperm+from+spermatocele+fluid%2C+Urology.+61%282%29%3A+417-420.&btnG=
View at Publisher | View at Google Scholar - Kauffman E C, Kim H H, Tanrikut C, Goldstein M. (2011). Microsurgical Spermatocelectomy: Technique and Outcomes of a Novel Surgical Approach, The Journal of Urology.; 185(1): 238-242.
View at Publisher | View at Google Scholar - Sista A K, Filly R A. Color Doppler Sonography in Evaluation of Spermatoceles The “Falling Snow” Sign Journal of Ultrasound in Medicine.; 27(1): 141-143.
View at Publisher | View at Google Scholar - Brockman S, Roadman D, Bajic P, Levine L A. (2022). Aspiration and Sclerotherapy: A Minimally Invasive Treatment for Hydroceles and Spermatoceles. Urology; 164: 273-277.
View at Publisher | View at Google Scholar - Gupta S, Gupta B,HatwarG, Bansod P. (2020). Unilateral Giant Spermatocele Mimicking Accessory Testis: A Case Report. National Journal of Integrated Research in Mededicine; Vol.11(3): 91-93
View at Publisher | View at Google Scholar - Basar H, Baydar S, Boyunaga H, Batislam E, Basar MM, et al. (2003). Primary bilateral spermatocele. Int J Urol.;10(1):59-61.
View at Publisher | View at Google Scholar - Oliva E, Young RH. (2000). Paratesticular tumor-like lesions. Semin Diagn Pathol.;17(4):340-358. thologic and surgical anatomy. Arch Surg ;86:351-355.
View at Publisher | View at Google Scholar - Rubenstein RA, Dogra VS, Seftel AD, Resnick MI. (2004). Benign intrascrotal lesions. J Urol.;171(5):1765-1772.
View at Publisher | View at Google Scholar - Itoh M, Li XQ, Miyamoto K, Takeuchi Y. (1999). Degeneration of the seminiferous epithelium with ageing is a cause of spermatoceles? Int J Androl.;22(2):91-96.
View at Publisher | View at Google Scholar - Rifkin MD, Kurtz AB, Goldberg BB. (1984). Epididymis examined by ultrasound. Correlation with pathology. Radiology.;151(1):187-190.
View at Publisher | View at Google Scholar - Junnila J, Lassen P. (1998). Testicular masses. Am Fam Physician.;57(4):685-692.
View at Publisher | View at Google Scholar - Lee HH, Fong CJ, Lai CT, Sun GH, Yu DS. et al. (2005). Giant spermatocele with multilocular appearance: a case report and literature review. Journal of Taiwan Urol. Assoc.;16(2):81-84.
View at Publisher | View at Google Scholar - Sánchez-Chapado M, Angulo JC, Haas GP. (1995). Adenocarcinoma of the rete testis. Urology;46(4):468-475.
View at Publisher | View at Google Scholar - Jassie MP, Mahmood P. (1985). Torsion of spermatocele: a newly described entity with 2 case reports. J Urol.;133(4):683-684.
View at Publisher | View at Google Scholar - Matsuoka K. (1989). Multilocular spermatocele: A case report. Nishinihon J. Urol.; 51:1279-1281.
View at Publisher | View at Google Scholar - Ravikanth R. (2018). Varicocele with Concomitant Ipsilateral Intratesticular Spermatocele: A Rarity. J Med Ultrasound;26(4):224-225.
View at Publisher | View at Google Scholar - MZYIENE Mohammed, ZIBA Ouima Justin Dieudonné, MARRAKCHI Jaafar, ENNACIRI Soufiane, ELAMMARI Jalal Eddine, et al. (2021). Spermatocele Mimicking Hydrocele: A Case Report in a Young Patient of 42 Years Old. International Journal of Current Science Research and Review.; 4(5), 422-424
View at Publisher | View at Google Scholar - Spermatocele: Pathologic and Surgical Anatomy | JAMA Surgery | JAMA Network [Internet]. [cited 2021 Apr 25].
View at Publisher | View at Google Scholar - Shakiba B, Heidari K, Jamali A, Afshar K. (2014). Aspiration and sclerotherapy versus hydrocoelectomy for treating hydroceles. Cochrane Kidney and Transplant Group, editor. Cochrane Database Syst Rev [Internet].
View at Publisher | View at Google Scholar - Chan CK, Yeung AM, Lee YK, Chau LH, Man CW, et al. (2020). Urethroscrotal fistula complicating large spermatocele in a male ketamine abuser: A case report. Urol. Case Rep.; 33:101284.
View at Publisher | View at Google Scholar - Chu PS, Kwok SC, Lam KM, Chu TY, Chan SW, et al. (2007). 'Street ketamine'-associated bladder dysfunction: a report of ten cases. Hong Kong Med J.;13(4):311-3. Epub.
View at Publisher | View at Google Scholar - Yek J, Sundaram P, Aydin H, Kuo T, Ng LG. (2015). The clinical presentation and diagnosis of ketamine-associated urinary tract dysfunction in Singapore. Singapore Med J.;56(12):660-664; quiz 665.
View at Publisher | View at Google Scholar - Zeng J, Lai H, Zheng D, Zhong L, Huang Z, et al. (2017). Effective treatment of ketamine-associated cystitis with botulinum toxin type a injection combined with bladder hydrodistention. J Int Med Res.;45(2):792-797.
View at Publisher | View at Google Scholar - Ng CF, Chiu PK, Li ML, Man CW, Hou SS, et al. (2013). Clinical outcomes of augmentation cystoplasty in patients suffering from ketamine-related bladder contractures. Int Urol Nephrol.;45(5):1245-1251.
View at Publisher | View at Google Scholar - Sisodiya RS, Man PK, Panda SS. (2016). Spermatocele Infrequent Cause of Scrotal Swelling in Children. International Journal of Collaborative Research on Internal Medicine & Public Health.;8(8):508-509.
View at Publisher | View at Google Scholar - Niedzielski J, Miodek M, Krakós M. (2012). Epididymal cysts in childhood - conservative or surgical approach? Pol Przegl Chir.;84(8):406-410.
View at Publisher | View at Google Scholar - Chillón Sempere FS, Domínguez Hinarejos C, Serrano Durbá A, Estornell Moragues F, Martínez-Verduch M, et al. (2005). Quistes epididimarios en la infancia [Epididymal cysts in childhood]. Arch Esp Urol.;58(4):325-328.
View at Publisher | View at Google Scholar
