

Research Article | DOI: https://doi.org/10.31579/2834-8087/047
Socio-Psychological Factors in People with HIV and Adherence to Pharmacological treatment. Pinar del Río, 2023
- Elizabeth Hernández Álvarez 1*
- Geydi González Serrano 2
- Lázaro Guillermo Ortega Castillo 3
- Dania Soto Carballo 4
- Marilin González Tielves 5
- Noralydis Rodríguez Washington 6
- Isabel Francisca Márquez García 7
- Provincial Center for Hygiene, Epidemiology and Microbiology, Pinar del Rio, Cuba.
- University Teaching Polyclinic “Ernesto Guevara de la Serna”, Sandino, Cuba.
- General Teaching Hospital “Heroes of Baire”, Nueva Gerona, Cuba.
- Community Teaching Polyclinic “5 de September”, Consolación del Sur, Cuba.
- Provincial Center for Hygiene, Epidemiology and Microbiology, Pinar del Rio, Cuba.
- Department of Social Sciences Teaching. National School of Public Health, Havana, Cuba.
- Department of Social Sciences Teaching. National School of Public Health, Havana, Cuba.
*Corresponding Author: : Elizabeth Hernández Álvarez, Provincial Center for Hygiene, Epidemiology and Microbiology, Pinar del Rio, Cuba.
Citation: Elizabeth H. Álvarez, Geydi G. Serrano, Ortega Castillo LG, Dania S. Carballo, Marilin G. Tielves, et al, (2025), Socio-Psychological Factors in People with HIV and Adherence to Pharmacological treatment. Pinar del Río, 2023, Archives of Clinical Investigation, 4(5); DOI:10.31579/2834-8087/047
Copyright: © 2025, Elizabeth Hernández Álvarez. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 01 October 2025 | Accepted: 16 October 2025 | Published: 24 October 2025
Keywords: Socio-psychological factors; person with HIV/AIDS; non-adherence to treatment
Abstract
Abstract
Introduction: Non-adherence to antiretroviral therapy (ART) in people living with HIV is a global challenge, even in Cuba, where there has been progress in prevention and universal access to healthcare. Pinar del Río has a rising prevalence of HIV, especially among men who have sex with men (MSM). This study aims to analyze the socio-psychological factors associated with non-adherence to ART in people living with HIV in Pinar del Río during 2023.
Method: A descriptive cross-sectional study was conducted with 35 non-adherent individuals (viral load ≥1000 copies). Questionnaires such as the COPE-28, the IDARE-IDERE, and the Lifestyle questionnaire were used, in addition to clinical interviews and a review of medical records. The analysis combined qualitative and quantitative methodologies using SPSS v25.
Results: The sample was predominantly male, homosexual, and reported low levels of perceived social and familial support. Eighty percent used emotion-focused coping strategies, primarily denial. Sixty percent exhibited unhealthy lifestyle habits such as smoking, alcohol consumption, and poor diet. Negative beliefs associated with external control or stigmatization were prevalent, while only 20% displayed proactive beliefs. Fifty-seven-point one percent reported moderate anxiety and depression, associated with a lack of support.
Conclusions: Non-adherence to ART in Pinar del Río is influenced by factors such as dysfunctional coping strategies, risky lifestyles, lack of social and family support, and negative beliefs. It is recommended to implement psychoeducational interventions to improve adherence, addressing emotional and social dimensions, with a focus on vulnerable groups such as men who have sex with men (MSM).
Introduction
The approach taken in Cuba to care for people with the Human Immunodeficiency Virus (HIV) and acquired immunodeficiency syndrome (AIDS) has been internationally recognized for its achievements in treatment and prevention. In this regard, since 2015 Cuba It was recognized as the first country by the World Health Organization (WHO) to eliminate mother-to-child transmission of HIV and syphilis . The prevalence of HIV in the sexually active population has been effectively controlled thanks to the implementation of public health policies that guarantee universal access to medical care and prevention programs .
However, the global picture is different from the Cuban context. According to data reported on the website of the Joint United Nations Programme on HIV/AIDS (UNAIDS), although new HIV infections fell by 39% globally in 2023 compared to 2010, with sub-Saharan Africa showing the largest reduction at 56%, 1.3 million (ranging from 1.0 to 1.7 million) new infections occurred that year.² This far exceeds the target of 370,000 new infections or fewer by 2025.³
Internationally, regions such as Eastern Europe, Central Asia, Latin America, the Middle East, and North Africa have experienced an increase in new HIV infections. For the first time in the history of the pandemic, more new infections have been recorded outside sub-Saharan Africa than within it. This may reflect progress in HIV prevention across much of the sub-Saharan African region. However, this also contrasts with the lack of similar progress in other parts of the world, where key populations and their partners remain largely underserved in HIV prevention programs. 3
With roughly five years remaining before the evaluation of the 2030 Agenda goals, the world finds itself at a critical juncture, given the potential for governments to fail to meet their commitments to end AIDS as a public health threat. While ending AIDS may be an objective goal, some figures reflect the need to continue working toward it. In this regard, it is important to acknowledge that of the 39.9 million people living with HIV worldwide, 9.3 million—almost a quarter—are not receiving life-saving treatment. As a result, one person dies every minute from AIDS-related causes.
In Cuba, the representation of the Joint United Nations Programme on HIV/AIDS has provided significant support for the control of the epidemic; some data that illustrate this are shown below :
- 86.4% of people living with HIV (28,405) have access to antiretroviral therapy with drugs recommended by the WHO
- 146,458 people from key populations (men who have sex with men, and transgender people) have access to prevention services;
- 26 polyclinics and 5 molecular biology laboratories have strengthened their capacities for the diagnosis and care of HIV, tuberculosis and other diseases;
- 1380 people from key groups have access to pre-exposure therapy, a proven method for HIV prevention;
- 1,776 people from civil society organizations have been trained in HIV prevention, to support community work and reduce human rights and gender-related barriers that limit access to care services for people living with HIV. 4
Specifically in the western province of Pinar del Río, HIV/AIDS has maintained an upward trend since its Begin Ning in 1986. According to a report Fromm the Provincial Center for Hygiene, Epidemiology, and Microbiology, 1,121 people were diagnosed as HIV-positive in 2024, of whom 894 were men (79.7%) and 227 were women (20.3%). Of the total number of men, 777 are men who have sex with men (MSM), representing 86.9% of those infected. These figures support the importance of continuing to develop research focused on this topic.
HIV is considered a chronic disease that, although incurable, has been transformed from a fatal illness into a manageable long-term condition thanks to antiretroviral therapy (ART). These treatments allow people to live long and healthy lives by suppressing viral replication and maintaining undetectable viral loads. This not only improves quality of life but also significantly reduces the risk of transmitting the virus to others.
Due not only to its medical implications but also to its social, economic, and political impact, the fight against HIV/AIDS has been a global chállenle that has mobilized communities, governments, non-governmental organizations, and the scientific community to seek solutions since its emergence in the 1980s. At a social level, HIV/AIDS has exposed and exacerbated many inequalities that were previously virtually imperceptible. It has disproportionately affected communities, increasing their levels of marginalization, including men who have sex with men, sex workers, people who inject drugs, and even people in regions with fragile health systems. The stigma and discrimination associated with HIV have been significant barriers to prevention, diagnosis, and treatment, underscoring the need for a comprehensive approach that addresses both the medical and social aspects of the disease
The loss of life among the economically active population, healthcare costs, and reduced productivity have severely impacted the economies of many countries. The global response to HIV has highlighted the importance of human rights in healthcare and has driven policies against discrimination and to ensure access to health services. The Universal Declaration of Human Rights and the global strategies of organizations such as UNAIDS have been fundamental to this effort. 3
This is undoubtedly a unique disease of the contemporary world, with a profound and multifaceted impact that affects all aspects of society in general and each individual. Therefore, consistent adherence to therapy and regular monitoring are considered essential for maintaining HIV control.
Martín, Grau, and Espinosa define treatment adherence as a dynamic process, which is complex from a behavioral point of view, and whose internal structure also integrates personal and relational components that inevitably involve the health professional. 7
The authors adopt a theoretical and conceptual position that aligns with these ideas. Consequently, they promote the guiding framework, based on the WHO's model of dimensions, which allows for the study of factors affecting individuals' ability to adhere to their treatment. Specifically, they refer to the following groups of factors:
- socioeconomic and demographic factors,
- those in the health system and the health team,
- the characteristics of the disease and its treatment,
- those from the family and social network,
- and those of patient 7.
Exploring all these elements in depth exceeds the scope of the research, so the objective proposed for the present work was to characterize people with HIV/AIDS who are not adherent to pharmacological treatment in the province of Pinar del Río, according to socio-psychological factors.
Social support goes beyond the mere presence of people in an individual's life; it manifests in the constant companionship of family and friends, but also in emotional understanding and a willingness to help with daily tasks. It can come from various sources, such as specialized support groups, community networks, or even therapy animals. Each of these forms of support has a unique impact on people's lives, providing not only practical help but also a sense of belonging and connection with others.
In clinical practice, healthcare professionals have observed how social support influences patient recovery: those with a strong support system tend to adhere better to treatment and experience fewer complications 8-12. This evidence supports the importance of considering social support as an integral component of healthcare, going beyond the prescription of medications.
Based on the above and in relation to the presented context, the following question is raised: What socio-psychological factors are related to the non-adherence to pharmacological treatment of people carrying HIV in the province of Pinar del Río during the year 2023?
II. Method
A retrospective, descriptive, cross-sectional study was conducted. The population consisted of 605 people with HIV from the province of Pinar del Río, who underwent viral load testing in 2023. A sample of 35 people was selected from this population using non-probability convenience sampling.
Inclusion criteria:
- Adults over 18 years of age who are willing to participate in the study.
- Time of diagnosis: greater than or equal to 12 months.
- Unsuppressed viral load: greater than or equal to 1000 copies
- People without cognitive or mental disabilities that limit autonomy to spontaneously and consciously access ART; as well as understanding the assessment tools.
To obtain the information, documentary analysis was taken into account through the review of medical records, epidemiological surveys and the Computerized Registry of HIV/AIDS of the Ministry of Public Health.
The following instruments were applied:
- Clinical interview: a technique based on human relations that provides a broad, comprehensive, and in-depth study of the patient. 13 In this study, it was primarily used to assess socio-familial support (as an expression of the Social Support Network) and the beliefs about the illness of the people studied.
- IDARE-IDERE: Self-assessment inventories designed to evaluate two relatively independent forms of anxiety and depression. 13
- COPE-28 Coping Styles Questionnaire: developed by Carver, Scheier, and Weintraub in 1989 following two theoretical models: Lazarus's Model and Bandura's Behavioral Self-Regulation Model. 14
- Lifestyle questionnaire: assesses various aspects of lifestyle, including sexual activity, food consumption, substance use, physical exercise, and recreational activities. It scores different lifestyle stages ranging from unhealthy to healthy.
III. Results
The study group was characterized by a majority of male participants, totaling 27 (77.1%). This translates into greater HIV exposure for men, which, in turn, could be associated with risky behaviors, some of which result from unequal gender roles that reinforce promiscuity and active sexual activity in men. Regarding skin color, white individuals predominated at 51.4%, followed by Black individuals at 40%; this reflects the country's and province's racial composition. Similarly, the majority (68.6%) were employed, while 60% lived in urban areas and 62.9% identified as homosexual; this last point reinforces the classification of men who have sex with men (MSM) as a high-risk group.
As can be seen in Figure 1, of the 28 people in the sample (80.0%) who adopted an Emotion-Focused Coping (EFC) strategy, 20 people (57.1%), 17 men and three women, adopted the Denial style; while eight (22.9%), six men and two women, adopted Behavioral Disengagement. Furthermore, seven people (20.0%), four men and three women, selected the Problem-Focused Coping (PFC) strategy, specifically the Planning style. The distribution of the different coping styles among the women was very similar, while among the men there was a slight predominance of the Denial style.
Chart No. 1. Distribution of people according to sex and coping styles. Pinar del Río, 2023.
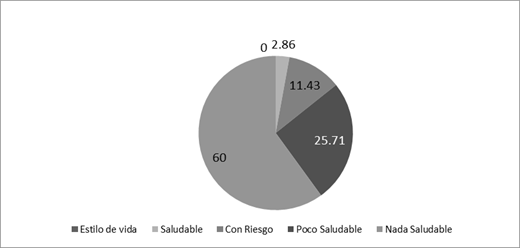
Regarding lifestyles, interpreted through behaviors and attitudes, Figure 2 shows that 60.0% of the individuals studied exhibit behaviors and attitudes that jeopardize their health and disease status. In this respect, the areas with the greatest negative impact were: poor physical condition (95.2%); high consumption of tobacco, alcohol, coffee, and other drugs (85.7%); inadequate eating habits ; and irresponsible sexual behavior (71.4% and 61.9% of participants, respectively). A history of non-adherence to antiretroviral therapy (ART) was also noted among these patients.
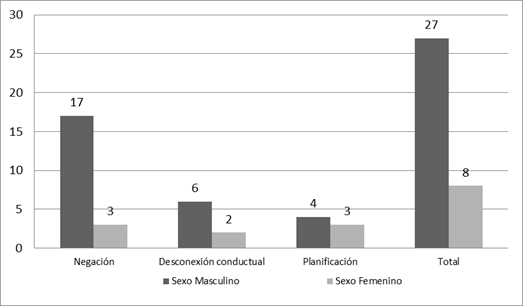
Chart No. 2: Distribution of people according to lifestyle. Pinar del Río, 2023
On the other hand, moderate emotional states are the most prominent, as shown in Figure 3. Of the selected sample, 20 people (57.1%) reported experiencing symptoms of anxiety and depression; of these, 15 do not receive socio-familial support. Following this, 10 (28.6%) reported mild emotional states, six of whom do not perceive this type of support. Another five (14.3%) reported signs of profound intensity in relation to these states, and four also do not experience support. The percentage of those who do not perceive socio-familial support is 71.4%, higher than the percentage who do.
Chart No 3: Distribution of people according to emotional states and perceived socio-family support.
The qualitative approach allowed the beliefs variable to be grouped into two categories. On one hand, there are positive beliefs (CP), which includes the subcategory of analysis Proactive Beliefs (CPA), associated with making decisions quickly to avoid complications based on learning from previous experiences. On the other hand, there are negative beliefs (CN), which includes the subcategory External Control Beliefs (CCE), referring to Carl Rogers ' external locus of control. 16 These beliefs place great importance on external forces or factors beyond a person's control. Similarly, Stigmatization Beliefs (SC) are included in this category, whereby the individual feels or perceives that they are rejected or discredited because of their HIV-positive status. The most frequent beliefs in the studied sample corresponded to External Control Beliefs, representing 44.9% of the total. Phrases such as " God will cure me " and " Everyone has to die of something, and only God knows when that day will come " exemplify this.
Next, beliefs of stigmatization were perceived in 37.1% of the participants, reflected in expressions such as: “ Whatever, to them I'm just a sick person ”; “ I'm disgusted with myself, the best thing would be to die ”; “ What does it matter if nobody cares about me ?” Finally, proactive beliefs were manifested in 20.0% of the people studied, and among the statements that demonstrated this were: “ I felt fine, that's why I stopped taking it, but it won't happen again ”; “ I want to have a future, that's why I'll take the medication ”; “ I take responsibility for my actions and I promise myself and you that it won't happen again .”
IV. Discussion
Health behaviors and their relationship to risk or protective factors, as well as coping strategies, are included among the intermediate determinants of health. Non-adherence to treatment in people with HIV is filtered through individual decision-making based on the meanings, beliefs, and affective-motivational value attributed to health, whether perceived as a risk or threat, or as a source of well-being and protection. A negative attitude or lack of motivation to commit to treatment adherence and good management of their diagnosis represent significant barriers to adherence. 16,17
Tobacco and alcohol addiction, as well as frequent partner changes and unprotected sex, are among the risk behaviors with the greatest impact on HIV transmission; this is especially true considering that the individuals discussed in this study have an unsuppressed viral load. Other behavioral factors, such as dietary patterns and physical activity, influence the achievement of adequate long-term control, the prevention of complications, and the reduction of morbidity and mortality rates. 18,19
People living with HIV, in their social roles, require the support of those around them, especially those with whom they have emotional and cohabiting ties, that is, their family. In this study, most non-adherent individuals reported not feeling supported by their families, indicating the need to implement more interventions to improve this dynamic within the family environment. When these individuals have family and social support, they have a higher level of adherence to ART . 20
Negative beliefs (based on the classification proposed in this study) lead people living with HIV to coping styles that do not promote a healthy relationship with ART. Therefore, for a patient to improve their adherence, they need to take a more active role in managing their illness, increase their autonomy, and enhance their self-care capacity. 16
The factors described above directly and indirectly undermine public health policies and the Cuban government's efforts to provide comprehensive care for people living with HIV. Living with this disease has effects that extend beyond individual health, leading to social rejection and even self-discrimination, significant obstacles to accessing prevention services and reducing the likelihood of viral transmission.
Future lines of research should not disregard these aspects, in order to achieve a holistic approach to the phenomenon. Therefore, it is considered that interventions employing psychoeducation will be the most effective and efficient. 21 In this sense, psychoeducation can be considered a part of cognitive-behavioral therapy because it involves both a change in thinking (through the reception of information) and in behavior (applying the information received to adopt healthy habits). Furthermore, its effectiveness is supported by empirical evidence.
Specifically in Pinar del Río, there are experiences like those of Barbosa and González that could be extrapolated to the family context. The aforementioned proposal focused on adolescents, a population highly vulnerable to HIV infection, and considering the type of design employed, it is considered a suitable experience for replication.
Cuba has extensive experience in counseling and advising on HIV-related cases; however, it would be interesting to assess the potential for adaptation to the national context of experiences such as the one developed in Peru by a group of researchers, which shows The guideline is characterized by its usefulness, acceptability, adaptability, and sustainability in its application, and its potential effectiveness in improving adherence among patients who consume alcohol, depending on their consumption levels. 23 The guideline has the potential to be applied in other contexts that share a similar patient profile, namely, Spanish-speaking adults receiving antiretroviral therapy (ART) who are not in the AIDS stage. Furthermore, nurses with similar training and language skills can easily understand and implement the guideline. Likewise, the method used to validate nursing interventions, such as counseling in this case, has been described in a way that allows it to be replicated and adapted for other similar interventions.
V. Conclusions
Among the predominant socio-psychological factors were emotion-focused coping strategies, including denial, which were more evident in men, while women showed relative variability in this regard. Most individuals exhibited risky behaviors, the most frequent being the consumption of tobacco, alcohol, coffee, and other drugs, as well as inadequate eating habits. Similarly, the majority of the sample did not receive socio-familial support, all of which influenced non-adherence to pharmacological treatment among people living with HIV.
Evaluating a group of socio-psychological variables, which may be associated with the social determinants of health and influence therapeutic adherence in people with HIV, can offer a reductionist view of the phenomenon. Logically, the small number of people evaluated makes it impossible to generalize the results to the rest of the population; however, the results highlight the need to increase and broaden the scope of this type of study.
Addressing the socio-psychological factors that influence treatment adherence is essential to mitigating the negative effects of HIV on individuals and society as a whole. This involves designing intervention strategies to modify behaviors, attitudes, and beliefs to improve adherence and, consequently, enhance the quality of life for those living with HIV, particularly those residing in the province of Pinar del Río.
References
- UNAIDS. Cuba ensures that no one is excluded from the AIDS response [Internet]. 2021 [cited 2024 Oct 9
View at Publisher | View at Google Scholar - UNAIDS Fact Sheet – Latest Statistics on the State of the AIDS Epidemic. [Internet] n.d.
View at Publisher | View at Google Scholar - UNAIDS. The urgency of now. Global AIDS Update. [Internet]. 2024 [cited 2024 Oct 9].
View at Publisher | View at Google Scholar - United Nations Cuba. HIV care in Cuba opens doors to possible South-South Cooperation initiatives [Internet]. 2024 [cited 2024 Oct 9].
View at Publisher | View at Google Scholar - Provincial Center for Hygiene, Epidemiology and Microbiology. Section for the Prevention of STIs/HIV/AIDS and Hepatitis. Epidemiological situation of STIs/HIV-AIDS, Pinar del Río. Year 2023 Closing. Pinar del Río: Provincial Center for Hygiene, Epidemiology and Microbiology; January 12, 2024.
View at Publisher | View at Google Scholar - World Health Organization. Global health sector strategies on HIV, viral hepatitis and sexually transmitted infections for the period 2022-2030 [Internet].
View at Publisher | View at Google Scholar - Martín Alfonso L de los Á, Grau Ábalo JA, Espinosa Brito AD. (2014) Conceptual framework for the evaluation and improvement of adherence to medical treatments in chronic diseases. Journal Cuban Journal of Public Health.;40(2):225-238.
View at Publisher | View at Google Scholar - Henry JP, Cobb S. (1951) Neurocirculatory Asthenia, Anxiety and Neurosis. New England Journal of Medicine. Nov;245(19):711-719.
View at Publisher | View at Google Scholar - Cacioppo S, Grippo AJ, London S, Goossens L, Cacioppo JT. 2015 Loneliness: Clinical Importance and Interventions. Perspectives on Psychological ScienceMar; 10 (2): 238-249
View at Publisher | View at Google Scholar - Gené -Badia J, Comice P, Belchín A, Erdozain MÁ, Cáliz L, 2020 Torres S, Rodríguez. Resilience. Profiles of loneliness and social isolation in urban populations. Primary Care. Apr ; 52(4): 224-232.
View at Publisher | View at Google Scholar - National Academies of Sciences, Engineering, And Medicine. Social isolation and loneliness in older adults: opportunities for the health care system. Washington, DC: The National Academies Press; 2020. A
View at Publisher | View at Google Scholar - Gerino E, Rollè L, Sechi C, Brustia P. Loneliness, Resilience, Mental Health, and Quality of Life in Old Age: A Structural Equation Model. Frontiers in Psychology. 2017 Nov; 8:2003.
View at Publisher | View at Google Scholar - González Llaneza, FM. 2007. Psychological assessment instruments. Havana City: Ecimed Publishing House ;
View at Publisher | View at Google Scholar - Saavedra Zamora R, Blanco Suárez M, Mariño Pérez Y, Santisteban Cedeño LY, Pérez Estrada LE. Coping styles for chronic non-communicable diseases. 1st Virtual Conference on Family Medicine [Internet]. 2021 [ cited 2024 Oct 9]; Ciego de Ávila, Cuba.
View at Publisher | View at Google Scholar - Rojas Castro Y. Characterization of lifestyles in workers with components of Metabolic Syndrome, Pinar del Río. [Bachelor's thesis]. Pinar del Río: University of Medical Sciences of Pinar del Río; 2012.
View at Publisher | View at Google Scholar - Jimenez Cargua K. Influence of psychosocial factors on adherence to therapeutic treatment in people with HIV/AIDS, treated at a hospital in the city of Guayaquil, from January 2019 to January 2020. [Master's Thesis]. Ecuador: Salesian Polytechnic University; 2021.
View at Publisher | View at Google Scholar - Vásquez Ortega AA. Coping strategies and quality of life in HIV-positive individuals in the city of Guayaquil, 2022. [Master's thesis]. Ecuador: Salesian University; 2022.
View at Publisher | View at Google Scholar - González García WA, Mascon Gómez MN, 2019 Burgos García E. Food consumption, lifestyles and nutritional status of HIV-infected patients treated at a specialty hospital in the city of Guayaquil. Rev Cubana Aliment Nutr .;29(1):47-63.
View at Publisher | View at Google Scholar - Pérez Bastán JE, Viana Castaño LF. Factors associated with non-adherence to antiretroviral therapy in people with HIV/AIDS. Cuban Journal of Tropical Medicine [Internet] 2020 [ cited 2024 Oct 10]; 72(2):e499.
View at Publisher | View at Google Scholar - Tobón B Ángel, García Peña JJ. Emotional profile of people living with HIV. Psychology Iztacala [Internet]. June 28, 2019 [cited October 10, 2024];22(2).
View at Publisher | View at Google Scholar - Neria MR, Sánchez-Sosa JJ, Riveros RA 2020. Psychoeducation for adherence to antiretroviral treatment: the hourglass metaphor. Psychology and Health.;30(2):217-229.
View at Publisher | View at Google Scholar - Barbosa-Ramos RL, González-Rodríguez R. Educational intervention proposal on HIV/AIDS for adolescents in a medical office. Universidad Medical Pin arena. 2020;16(3 ):e 412.
View at Publisher | View at Google Scholar - Musayón -Oblitas FY, Cárcamo CP, Gimbel S, Zarate JIE, Espinoza ABG. Validation of a counseling guide for adherence to antiretroviral therapy using implementation science. Revista Latino-Americana de Enfermagem [Internet]. 2020;28.
View at Publisher | View at Google Scholar -
View at Publisher | View at Google Scholar
