

Research Article | DOI: https://doi.org/10.31579/2835-9259/002
Research Article: Cyclophosphamıde–Etoposıde + G-csf Compared to G-csf alone in Perıpheral Blood Stem Cell Mobılızatıon for Multıple Myeloma
*Corresponding Author: Aysun Halacoglu, Bahcelievler Medicana Hospital, Hematology Department Istanbul/Turkey.
Citation: Aysun Halacoglu, (2022), Research Article: Cyclophosphamıde–Etoposıde + G-csf Compared to G-csf alone in Perıpheral Blood Stem Cell Mobılızatıon for Multıple Myeloma, Oral Health and Dentistry Case Reports, 1(1); DOI:10.31579/2835-9259/002
Copyright: © 2022 Aysun Halacoglu, This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 15 September 2022 | Accepted: 26 September 2022 | Published: 03 October 2022
Keywords: stem cell; mobilization; multiple myeloma; AHSCT; G-CSF
Abstract
Background: Multiple myeloma (MM) is the leading indication of autologous hematopoietic stem cell transplantation (AHSCT). There are different regimens used for peripheral blood stem cell mobilization in MM. A minimum of 2 × 106 CD34 + cells/kg are needed for engraftment. This study that presents a comparison of the mobilization outcomes Cyclophosphamide-Etoposide (Cy-Et) + granulocyte-colony stimulating factor (G-CSF) group and G-CSF alone group.
Patients and methods: This study has been performed in a retrospective manner. 110 patients with diagnosed MM who underwent stem cell mobilization at Memorial Sisli Hospital between the years of 2013 and 2018 were evaluated. We retrieved data on patient demographics, disease status at mobilization, treatment characteristics, stem cell mobilization, collection and post AHSCT outcomes. For mobilization, 70 patients received cyclophosphamide 1250 mg/m2 for 2 day, etoposide 100 mg/m2 for 3 day and G-CSF 10 mcg/kg/day from day 4 onwards and 40 patients received G-CSF alone.
Results: In 98 of 110 patients (89.1%) first mobilization trial was successful. Four patients in the Cy-Et group (5,7%) and eight patients in the G-CSF alone group (20%) were mobilized three times (p=0.001). The number of CD34 in peripheral blood was significantly higher in Cy-Et group (94±14) than G-CSF alone group (54±7) (p=0.04) on the stem cell mobilization time. Stem cell collection was higher in the Cy-Et group (13.8 × 106 CD34 + cells/kg) compared to the G-CSF alone group (8.8× 106 CD34 + cells/kg) (p =0.001). The median time to neutrophil engraftment was 11 and 13 days in Cy-Et group and G-CSF alone group respectively (p=0.014). The median time to platelet engraftment was 15 and 17 days in Cy-Et group and G-CSF alone group respectively (p=0.006). Median 360 ml stem cells in Cy-Et group and 470 ml stem cells in G-CSF alone group were collected and this difference was statistically significant (P=0.001).
Conclusion: In conclusion, this study was demonstrated that Cy-Et + G-CSF mobilization provides a higher peripheral CD 34 count, less apheresis sessions, less volume, more stem cell mobilization, earlier neutrophils and platelet engraftment for patients with MM and eligible for AHSCT. Today, Cy-Et + G-CSF mobilization is a really useful method than G-CSF alone.
Introduction
Multiple myeloma (MM) is a malignant disease that occurs with an uncontrolled, clonal increase of plasma cells in the bone marrow (1). MM is the leading indication of autologous hematopoietic stem cell transplantation (AHSCT) worldwide (2). High-dose melphalan followed by AHSCT is the standard treatment for MM in eligible patients after induction therapy (3). There are different regimens used for peripheral blood stem cell mobilization in MM, however, there is no consensus as to the optimal mobilization regimen for MM. A minimum of 2 × 106 CD34 + cells/kg are needed for engraftment (4).
This study that presents a comparison of the mobilization outcomes Cyclophosphamide-Etoposide (Cy-Et) + granulocyte-colony stimulating factor (G-CSF) group and G-CSF alone group.
Materials and Methods
Patients and methods
This study has been performed in a retrospective manner. 110 patients with diagnosed MM who underwent stem cell mobilization at Memorial Sisli Hospital between the years of 2013 and 2018 were evaluated. All patients gave informed consent for all aspects of AHSCT. We retrieved data on patient demographics, disease status at mobilization, treatment characteristics, stem cell mobilization, collection and post AHSCT outcomes (Tables 1-2). For mobilization, 70 patients received cyclophosphamide 1250 mg/m2 for 2 day, etoposide 100 mg/m2 for 3 day and G-CSF 10 mcg/kg/day from day 4 onwards and 40 patients received G-CSF alone. Prophylactic antibiotic was given from day +5 till absolute neutrophil count was more than 500 x ×106 /L. Stem cell collection began when CD34+ was over 10 cells/µL. All ethical considerations were strictly followed in accordance with the Helsinki Declaration.
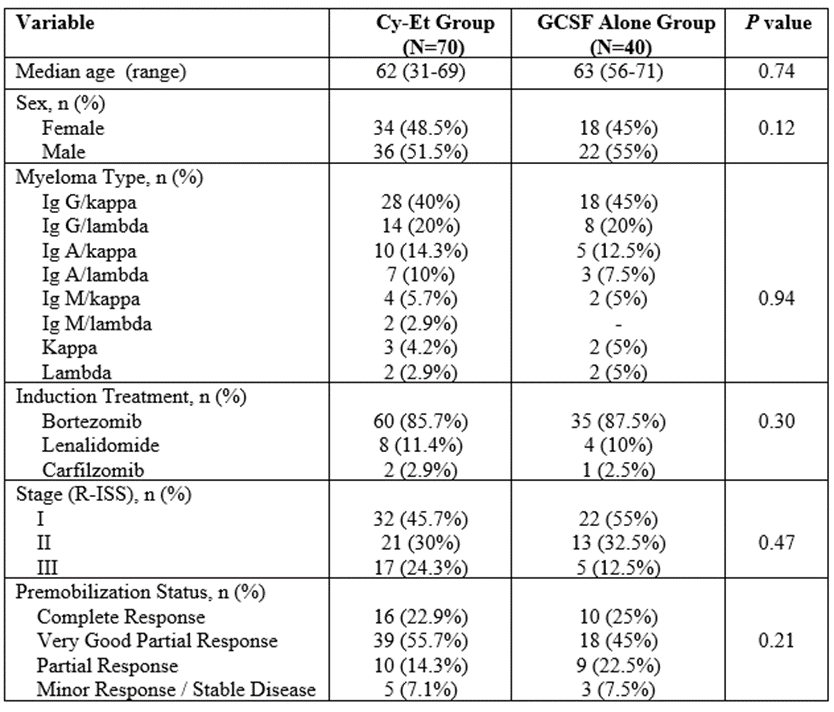
Table 1: Patients Characteristics
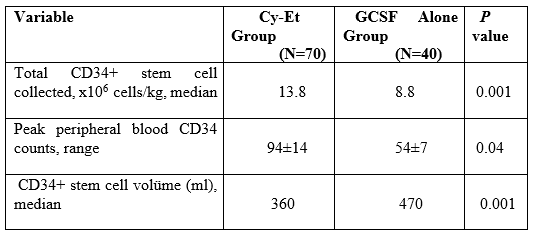
Table 2: Stem cell mobilization outcomes
Definitions
Poor mobilization are a collection of < 2>
Statistical Analysis
SPSS statistics 20 (SPSS Inc., Chicago, IL, USA) was used for statistical analyses. Comparisons of categorical variables in groups were tested by Chi‑square or two‑tailed Fisher’s exact tests. All P values <0>
Results
One hundred and ten patients were included in this study. The median age was 55 (31–71) years at the time of the diagnosis. No significant difference was observed in baseline characteristics between groups, including the disease control and previous therapies.
In 98 of 110 patients (89.1%) first mobilization trial was successful. Four patients in the Cy-Et group (5,7%) and eight patients in the G-CSF alone group (20%) were mobilized three times (p=0.001).
The number of CD34 in peripheral blood was significantly higher in Cy-Et group (94±14) than G-CSF alone group (54±7) (p=0.04) on the stem cell mobilization time.
Stem cell collection was higher in the Cy-Et group (13.8 × 106 CD34 + cells/kg) compared to the G-CSF alone group (8.8× 106 CD34 + cells/kg) (p =0.001).
The median time to neutrophil engraftment was 11 and 13 days in Cy-Et group and G-CSF alone group respectively (p=0.014). The median time to a platelet count > 20.000 x 109/L for more than 7 days without transfusion was 15 and 17 days in Cy-Et group and G-CSF alone group respectively (p=0.006).
Median 360 ml stem cells in Cy-Et group and 470 ml stem cells in G-CSF alone group were collected and this difference was statistically significant (P=0.001).
Discussion
This single-center, retrospective study involving 110 MM patients who underwent stem cell mobilization, present a comparison of the mobilization outcomes Cy-Et + G-CSF group and G-CSF alone group.
Although different agents are used for stem cell mobilization in MM, there is no consensus on the most appropriate option. Plerixafor can be used in stem cell mobilization by evaluating its side effects, cost-benefit ratio and availability in suitable patients (5, 6). Today, Plerixafor comes to mind in case of failure of first-line mobilization regimens. In this study, adequate mobilization was achieved in all patients without the need for plerixafor use in any of the patients.
In a study (7), two groups that were applied Cy + GCSF and Et + GCSF for stem cell mobilization in MM were compared and more stem cells were obtained in the group mobilized with Et than in the group mobilized with Cy. In our study, more stem cell mobilization was achieved in the Cy-Et group than in the GCSF alone group.
In this study, in the stem cell mobilization process, there was no increase in infection processes in the Cy-Et group, contrary to expectations, compared to the GCSF alone group, and Cy-Et was easily tolerated by all patients. This may be related to the fact that the disease was under control before transplantation in patients who were planned for transplantation.
Some previous studies (8-10) used GCSF alone or Cy + GCSF as a mobilization regimen in MM. However, mobilization insufficiency is around 10-20%. In this study, adequate mobilization was performed in a single session in 89.1% of the patients. Mobilization was required 3 times in 5.7% of the patients in the Cy-Et group and in 20% of the patients in the GCSF alone group.
In a study of 91 MM patients in the literature (11), 42 patients were mobilized with a novel pegylated form of the recombinant G-CSF filgrastim, 49 patients were mobilized with filgrastim, and it was shown that more stem cell mobilization and earlier engraftment were achieved with the pegylated form. The combination of Cy-Et with pegylated form filgrastim is a candidate to be the current cost-effective mobilization option in MM.
In the literature (12), in a multicenter study of 422 MM patients, it was shown that low-dose Cy provides optimal mobilization when Cy is 2 g/m2 and ≥ 3 g/m2 and GCSF alone is used. In this study, when Cy was used with total 2.5 g/m2 and Et, more effective mobilization was achieved than GCSF alone. In addition, in this study, no hemorrhagic cystitis or neutropenic infection was reported due to the use of Cy during stem cell mobilization in MM in previous studies (13-14).
In this study, the fact that more stem cell mobilization was obtained with less apheresis in the Cy-Et group offers an advantage especially for tandem transplantation in MM. Also, earlier neutrophil and platelet engraftment was obtained in the Cy-Et group compared to the GCSF group alone, which may provide a cost advantage due to earlier post-transplant discharge and less hospital stay.
Conclusion
In conclusion, this study was demonstrated that Cy-Et + G-CSF mobilization provides a higher peripheral CD34 count, less apheresis sessions, less volume, more stem cell mobilization, earlier neutrophils and platelet engraftment for patients with multiple myeloma and eligible for ASCT. Today, Cy-Et + G-CSF mobilization is a really useful method than G-CSF alone. Further randomized, prospective studies with larger sample size and clinical, laboratory and histopathological data from such studies are required to support the results of this study.
Compliance with ethical standards
All ethical considerations were strictly followed in accordance with the Helsinki Declaration.
Financial support and sponsorship
Nil
Conflicts of interest
There are no conflicts of interest.
References
- Röllig C, Knop S, Bornhäuser M. Multiple myeloma. Lancet. (2015):385(9983):2197-2208.
View at Publisher | View at Google Scholar - Martino M, Lemoli RM, Girmenia C, Castagna L, Bruno B, (2016): et al. A. Italian consensus conference for the outpatient autologous stem cell transplantation management in multiple myeloma. Bone Marrow Transplant.;51(8):1032-1040.
View at Publisher | View at Google Scholar - Ebraheem M, Kumar SK, Dispenzieri A, Jevremovic D, Buadi FK,( 2022): et al. Deepening Responses after Upfront Autologous Stem Cell Transplantation in Patients with Newly Diagnosed Multiple Myeloma in the Era of Novel Agent Induction Therapy. Transplant Cell Ther.;28(11):760.e1-760.e5.
View at Publisher | View at Google Scholar - Cottler-Fox MH, Lapidot T, Petit I, Kollet O, DiPersio JF, (2003): et al. Stem cell mobilization. Hematology Am Soc Hematol Educ Program. 2003:419-437.
View at Publisher | View at Google Scholar - Fowler CJ, Dunn A, Hayes-Lattin B, Hansen K, Hansen L, (2009): et al. Rescue from failed growth factor and/or chemotherapy HSC mobilization with G-CSF and plerixafor (AMD3100): an institutional experience. Bone Marrow Transplant; 43(12):909-917.
View at Publisher | View at Google Scholar - Duarte RF, Shaw BE, Marín P, Kottaridis P, Ortiz M, (2011): et al. Plerixafor plus granulocyte CSF can mobilize hematopoietic stem cells from multiple myeloma and lymphoma patients failing previous mobilization attempts: EU compassionate use data. Bone Marrow Transplant.;46(1):52-58.
View at Publisher | View at Google Scholar - Song GY, Jung SH, Ahn SY, Jung SY, Yang DH, (2019): et al. Optimal chemo-mobilization for the collection of peripheral blood stem cells in patients with multiple myeloma. BMC Cancer.;19(1):59.
View at Publisher | View at Google Scholar - Pusic I, Jiang SY, Landua S, Uy GL, Rettig MP, (2008): et al. Impact of Mobilization and Remobilization Strategies on Achieving Sufficient Stem Cell Yields for Autologous Transplantation, Biology of Blood and Marrow Transplantat.;14(9):1045-1056.
View at Publisher | View at Google Scholar - Pavone V, Gaudio F, Console G, Vitolo U, Lacopino P, (2006): et al. Poor mobilization is an independent prognostic factor in patients with malignant lymphomas treated by peripheral blood stem cell transplantation. Bone Marrow Transplant.;(37):719–724.
View at Publisher | View at Google Scholar - Desikan KR, Barlogie B, Jagannath S, Vesole DH, Siegel D, (1998): et al. Comparable engraftment kinetics following peripheral-blood stem-cell infusion mobilized with granulocyte colony-stimulating factor with or without cyclophosphamide in multiple myeloma. J Clin Oncol.;16(4):1547-1553.
View at Publisher | View at Google Scholar - Ding X, Huang W, Peng Y, Fan H, Zhu Y, (2020): et al. Pegfilgrastim improves the outcomes of mobilization and engraftment in autologous hematopoietic stem cell transplantation for the treatment of multiple myeloma. Ann Hematol.;99(6):1331-1339.
View at Publisher | View at Google Scholar - Zannetti BA, Saraceni F, Cellini C, Fabbri E, Monaco F, (2021): et al. Low-Dose Cyclophosphamide versus Intermediate-High-Dose Cyclophosphamide versus Granulocyte Colony-Stimulating Factor Alone for Stem Cell Mobilization in Multiple Myeloma in the Era of Novel Agents: A Multicenter Retrospective Study. Transplant Cell Ther.;27(3):244.e1-244.e8.
View at Publisher | View at Google Scholar - Almalag HM, Alasmari SS, Alrayes MH, Binhameed MA, Alsudairi RA, (2021): et al. Incidence of hemorrhagic cystitis after cyclophosphamide therapy with or without mesna: A cohort study and comprehensive literature review. J Oncol Pharm Pract.;27(2):340-349.
View at Publisher | View at Google Scholar - Corso A, Arcaini L, Caberlon S, Zappasodi P, Mangiacavalli S, (2002): et al. A combination of dexamethasone, cyclophosphamide, etoposide, and cisplatin is less toxic and more effective than high-dose cyclophosphamide for peripheral stem cell mobilization in multiple myeloma. Haematologica.;87(10):1041-1045.
View at Publisher | View at Google Scholar
