

Research Article | DOI: https://doi.org/10.31579/2835-7957/147
Perception of Stress in Pregnant Women: Case of Women in Consultation at the “Cité Verte” District Hospital in Yaounde (Cameroon)
- Zemo Gamo Franklin 1*
- Fanta Yadang Sabine Adeline 2
- Mefo Nguenang Ange 3
- Tsata Mariette Noel 3
- Phatouma Boubakari 3
1Department of Animal Biology and Physiology, Faculty of Science, University of Yaounde I, P.O. Box 812, Yaounde, Cameroun.
2 Centre for Research on Medicinal Plants and Traditional Medicine, Institute of Medicinal Research and Medicinal Plants Studies, P.O. Box 13033, Yaounde, Cameroun
3 Department of Health, Private Bilingual Higher Institute les Armandins, University of Ngaoundere, P.O. Box 7045, Yaounde, Cameroon
*Corresponding Author: Zemo Gamo Franklin, Department of Animal Biology and Physiology, Faculty of Science, University of Yaounde I, P.O. Box 812, Yaounde, Cameroun.
Citation: Zemo G. Franklin, Sabine Adeline FY, Mefo N. Ange, Tsata M. Noel, Phatouma Boubakari, (2025), Perception of Stress in Pregnant Women: Case of Women in Consultation at the “Cité Verte” District Hospital in Yaounde (Cameroon), Clinical Reviews and Case Reports, 4(5); DOI:10.31579/2835-7957/147
Copyright: © 2025, Zemo Gamo Franklin. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 07 August 2025 | Accepted: 22 August 2025 | Published: 02 September 2025
Keywords: stress; perception of stress; pregnant women
Abstract
Objective: The aim of the present study was to assess the perception of stress among pregnant women’s consulting at the “Cité Verte” District Hospital in Yaoundé (Cameroon).
Methods: A quantitative, comparative study was conducted using a questionnaire adapted from the Antenatal Perceived Stress Inventory (APSI). The two groups in the study consisted of primiparous (first-time) and multiparous (experienced) women. We aimed to compared their perceptions of prenatal stress factor and identify the different stress levels across the three trimesters of pregnancy.
Results: The results obtained show a high level of stress for the items regarding the baby’s health, the obstetric or medical problems that can occur during pregnancy, and the items regarding the events of the delivery (epidural, episiotomy, delivery date). The results also show that the primiparous women are more stressed during pregnancy than the multiparous for most items of the ASPI scale.
Conclusion: Pregnancy leads to a high level of stress, especially for primiparous women. Results are in favour of creating better caring for these women, by installing prenatal preparation for birth, at the very beginning of pregnancy, as well as a personal follow-up during the pregnancy for women who feel the most stressed.
1.Introduction
In the world, mental health is a major health issue and pregnancy is a unique maternal experience with significant psychological, physiological and biochemical effects on women [1]. Every pregnant woman experiences some stress whetherfinancial crisis or just how to assemble the crib correctly [2]. Pregnancy is a period of psycho-emotional vulnerability which may increase the level of stress of pregnant women. Mental health problems affect nearly 20% of pregnant women during the prenatal and postpartum periods [1]. Pregnant women are vulnerable because of different changes that occur during pregnancy and that may affect their mental health and fetus. A pregnant woman experiencing stress during her pregnancy may have long-term consequences for her fetus and child including issue related to metabolic functioning, as well as emotional, cognitive, and behavioural problems [3-4]. The most common psychiatric disorders in the perinatal period are maternal anxiety disorders. Its prevalence rates are around 11 to 17% and are closely linked with alterations in the human stress systems [3]. In Psychological terms, stress can be defined as a state of anxiety produced when events and responsibilities exceed one’s coping abilities. On a physiological basis, stress may be defined as the non-specific response of the body to any demand placed upon it to adapt, whether that demand produces pleasure or pain [5]. In the body, one of the major regulating systems to cope with stress on a hormonal level is the hypothalamic-pituitary-adrenocortical axis (HPA axis). Some study indicates that high maternal cortisol levels in response to stress may affect the offspring’s HPA axis functioning. The increase in cortisol reactivity, in the long run, increases the risk for developmental problems in the offspring [3].
The pregnant woman may face a certain level of stress during pregnancy because of the new role endorsed upon her, her health as well as the child-to-be born becomes her responsibility [4]. During pregnancy, psychological problems emerge and if it’s not solved, the emotional pressures that result may continue to increase, causing stress and depression [6]. Estimation of the prevalence of depression during pregnancy varies depending on the criteria used. In symptomatic women, this prevalence is about 16% or more and 5% for women with major depression [7]. Some studies suggest that a significant portion of women experience prenatal anxiety both in general and during their pregnancy [8]. An analysis of a diverse urban sample found that 78% of pregnant women experienced low-to-moderate antenatal psychosocial stress and 6% experienced high levels [9]. Some of the stressors that commonly affect women in pregnancy around the globe are low material resources, unfavourable employment conditions, heavy family and household responsibilities, strain in intimate relationships, and pregnancy complications [8]. In Africa and Cameroon in particular, little works are interested in the perception of stress by pregnant women and their origin. Based on this, the aim of the present study was to assess stress-promoting-factors in pregnant women’s consulting at the “Cité Verte” District Hospital in Yaounde (Cameroon).
2. Materials and methods
2.1. Study sample and population
The study was carried out during one month in pregnant women’s consulting at the “Cité Verte” District Hospital in Yaoundé (Centre Region of Cameroon). The sample size consisted of 40 pregnant women who attended the outpatient hospital and consented to participate in the study. The participants were selected by the simple random sampling method. All the participants fulfilled the following inclusion criteria: student, worker, unemployed, and no adverse medical events during their pregnancies.
2.2. Data collection
Data were collected from January 6 to February 6, 2022, at the “Cité Verte” District Hospital in Yaoundé, Cameroon. A quantitative and comparative study methodology was used for this work. The minimum sample size for this study was determined using a non-probability convenience sampling method. The scale used for assessing stress was adapted from the Antenatal Perceived Stress Inventory (APSI) adopted by Razurel in 2013[10]. The adapted scale consisted of 13 items, representing 76% of the original ASPI scale (76% of ASPI scale). Participant rated their level of stress perception on a 5-point Likert scale, where: 1 = Not at all stressed, 2 = A little stressed, 3 = Moderately stressed, 4 = Very stressed, and 5 = Extremely stressed.
Data collection was conducted using the medical records of pregnant women, adata collection technical sheet and face-to-face interview methods. APSI: The APSI was developed by Razurel et al. in Sweden to evaluate perceived stress during the prenatal period by determining stress factors among women expecting their first child [10]. To adapt the ASPI in the context in Cameroon, some items were modified. The inventory adapted-ASPI has a 5-point Likert scale and consists of 13 items:
The medical and obstetric risks/foetal health subscale consists of 3 items: 1- Baby's health; 2- Ultrasound; 3- Obstetric and medical problems.
The psychosocial changes during pregnancy subscale consists of 7 items: 4- Current fatigue; 5- Mood changes (hypersensitivity); 6- The relationship with the partner; 7- Gaining weight during pregnancy; 8- The fact of not currently being able to do what she was doing before (smoking, drinking, going out, travelling, sports); 9- The fear of losing her husband*; 10- The fact of not having money for the layette*.
The prospect of childbirth subscale consists of 3 items: 11- The risk of having an episiotomy; 12- The fact of not knowing the date on which the delivery will take place; 13- Pain during childbirth*.
*: items added according to the Cameroonian context.
2.3. Ethical considerations
This study was carried out with the approval from the “Cité Verte” District Hospital, in Yaoundé Cameroon (Reference No: 8067/L/MINSANTE/DRSC/DSCV/DHCV, dated January 5, 2022) and received ethical clearance from the Regional Ethics Committee for Human Health Research in Yaoundé (Reference No: 059/CRERSHC/2023, dated February 23, 2023). In addition, all participants in the study provided informed consent. This study conformed to the principles outlined in the Declaration of Helsinki.
2.4. Statistical analysis
The data were analyzed using Microsoft Excel 2013 and GraphPad Prism (version 5.03) softwares. The results were expressed as a percentage of the level of perceived stress.
3. Results
3.1. Description of the study population
The total sample of the population studied was n = 40. General information about the description of the study population is presented in Table 1 below. The average age of the study population was 36 years.
Number of deliveries | |||||
Primiparous, n = 18 | Multiparous, n = 22 | ||||
Average age: 26 years | minimum age: 21 years | maximum age: 40 years | Average age: 32 years | minimum age: 22 years | maximum age: 45years |
Trimester of pregnancy | |||||
In trimester 1, n = 6 | In trimester 2, n = 18 | In trimester 3, n = 16 | |||
Activity | |||||
Working, n = 18 | Unemployed, n = 10 | Students, n = 12 | |||
Table 1: Description of the study population
3.2. Perception of stress related to medical and obstetric risks/foetal health
3.2.1. Baby's health
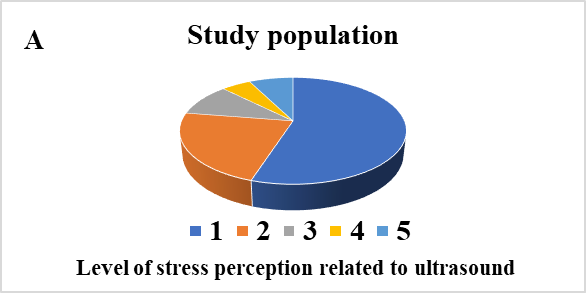
The analysis of the results presented in Figure 1A shows that 40% of pregnant women were not at all stressed by the health of the baby and 30% were little stressed. Among the multiparous women, 54.54% report that they were not at all stressed and 31.81% report they were little stress
regarding the health of their baby. In contrast, 27.77% of primiparous women report experiencing a little stress (Figure 1B). According to the trimester of pregnancy, 50% of these women in the 1st trimester were not at all stressed by the health of the baby and 33.33% were little stressed. In the 2nd trimester, 44.54% of these women were not at all stressed by the health of the baby and 22.22% were little stressed. Finally, in the 3rd trimester, 37.50% of women were not at all stressed by the health of the baby while 37.50% were little stressed (Figure 1C).
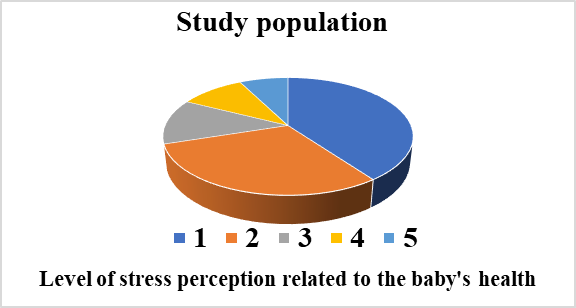
Study population: n = 40. A= In all pregnant women; B= Between multiparous and primiparous; C= Between the three trimesters of pregnancy. 1 = Not at all stressed, 2 = A little stressed, 3 =Moderately stressed, 4 = Very stressed, 5 = Extremely stressed.
3.2.2. Ultrasound
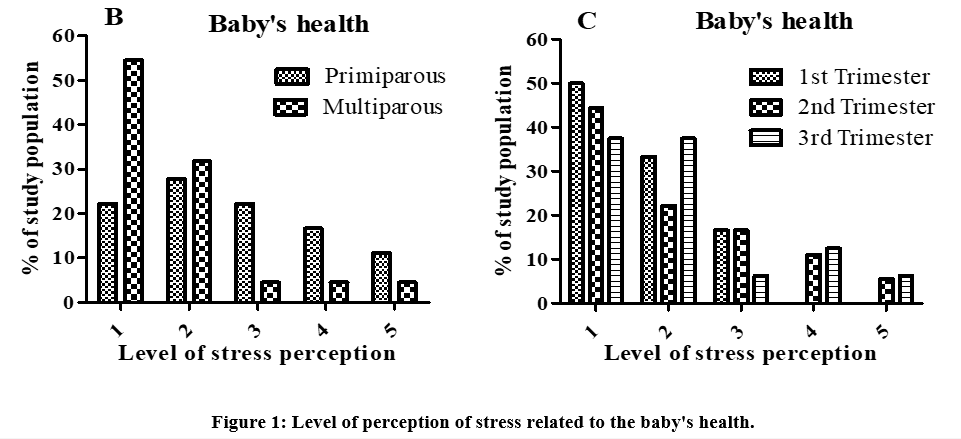
As shown in Figure 2A, approximately 55% of the study population does not experience stress related to ultrasound while 23% report feeling a little stressed. 59.09% of multiparous and 50% of primiparous were not at all stressed by ultrasound, while 18.18% of multiparous and 27.77% of primiparous were little stressed (Figure 2B). Regarding the trimester of
pregnancy, 16.66% of pregnant women in the 1st trimester were not at all stressed by ultrasound and 50% were little stressed. In the 2nd trimester, 55.55% of study population is not at all stressed by ultrasound and 27.77% werelittle stressed. Finally, in the 3rd Trimester, 56.25% were not at all stressed by ultrasound, while 18.75% werelittle stressed (Figure 2C).
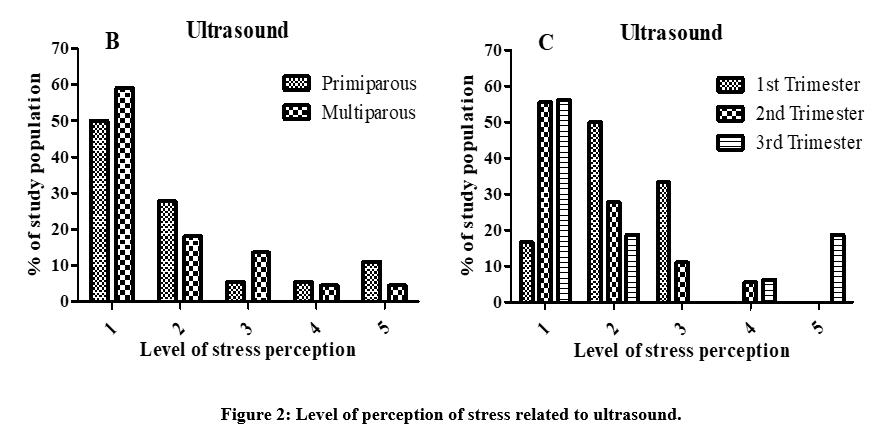
Study population: n = 40. A= In all pregnant women; B= Between multiparous and primiparous; C= Between the three trimesters of pregnancy. 1 = Not at all stressed, 2 = A little stressed, 3 = Moderately stressed, 4 = Very stressed, 5 = Extremely stressed.
3.2.3. Obstetric and medical problems
Results present in Figure 3A show that 42.50% of pregnant women in consultation at the “hôpital de district de la cité verte” (HDCV) were little stressed and 20% were moderately stressed by obstetrical or medical problems. 50% of multiparous were little stressed by obstetrical or medical problems and 33% of primiparous were moderately stressed (Figure 3B). Regarding the trimester, 83% of pregnant women in the 1st trimester, 50% in the 2nd trimester and 31.25% in the 3rd trimester were little stressed by obstetrical or medical problems (Figure 3C). 31.25% of pregnant women in the 3rd trimester were also moderately stressed by obstetrical or medical problems.
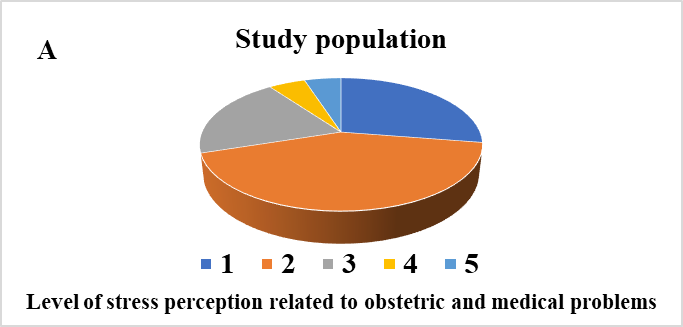
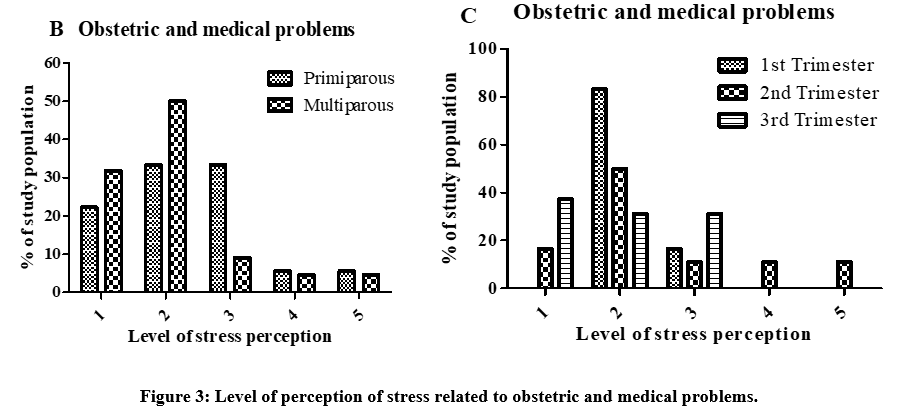
Study population: n = 40. A= In all pregnant women; B= Between multiparous and primiparous; C= Between the three trimesters of pregnancy. 1 = Not at all stressed, 2 = A little stressed, 3 = Moderately stressed, 4 = Very stressed, 5 = Extremely stressed.
3.3. Perception of stress related to psychosocial changes during pregnancy
3.3.1. Current fatigue
Figure 4 present the level of perception of stress related to current fatigue. As shown on figure 4A 52.50% of the study population were not at all stressed and 37.50% were little stressed by current fatigue. 45.45% of multiparous and 61.11% of primiparous were not at all stressed by current fatigue. Whereas 33.33% of multiparous and primiparous were little stressed by current fatigue (Figure 4B). Regarding the period of the pregnancy, in the 1st trimester, 66.66% of study population were not at all stressed by current fatigue and 16.66% were little stressed. In the 2nd trimester, 50% were not at all stressed by current fatigue and 38.89% were little stressed. Finally, in the 3rd trimester, 50% were not at all stressed by current fatigue and 43.75% are little stressed (Figure 4C).
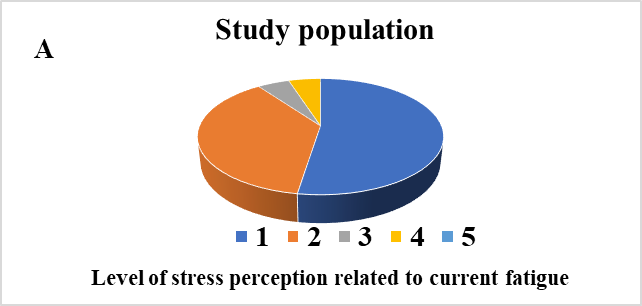
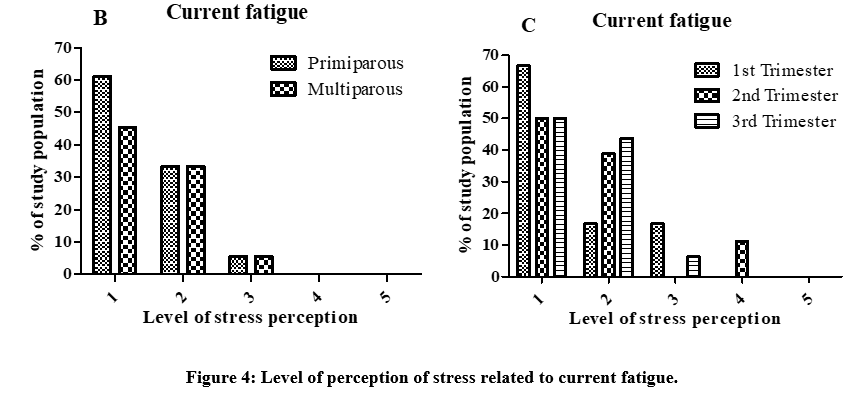
Study population: n = 40. A= In all pregnant women; B= Between multiparous and primiparous; C= Between the three trimesters of pregnancy. 1 = Not at all stressed, 2 = A little stressed, 3 = Moderately stressed, 4 = Very stressed, 5 = Extremely stressed.
3.3.2. Mood changes
The analysis of Figure 5A show that 40% of pregnant women in consultation at the HDCV were little stressed by mood changes (hypersensitivity). 54.55% of multiparous were little stressed by mood changes, while 44.44% and 27.78% of primiparous were not at all stressed and little stressed, respectively (Figure 5B). Regarding the trimester, 50% of pregnant women in the 1st trimester, 55.55% in the 2nd trimester, and 25.00% in the 3rd trimester were little stressed by mood changes (Figure 5C). 31.25% of pregnant women in the 3rd trimester were not at all stressed by mood changes.
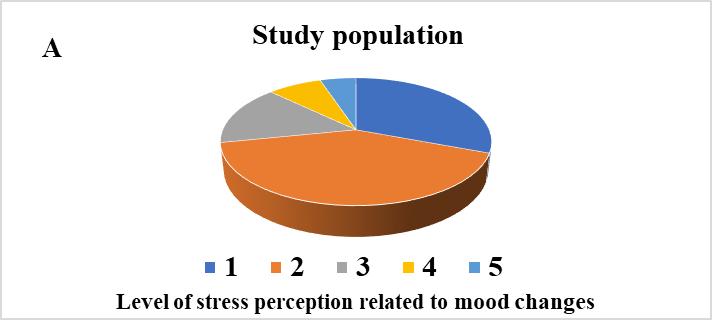
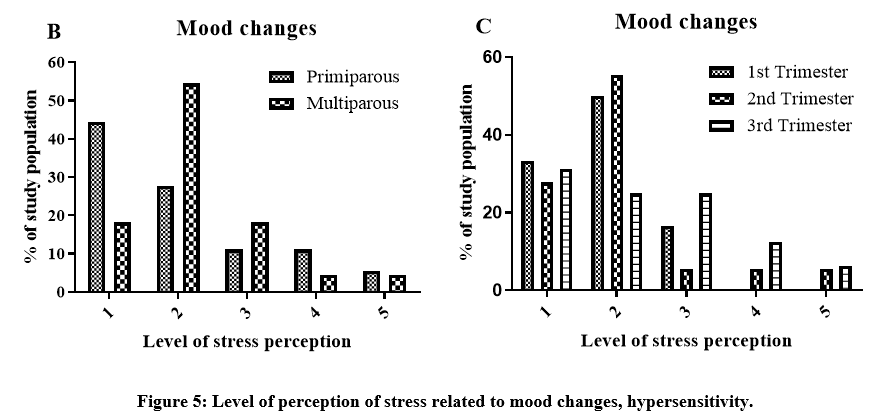
Study population: n = 40. A= In all pregnant women; B= Between multiparous and primiparous; C= Between the three trimesters of pregnancy. 1 = Not at all stressed, 2 = A little stressed, 3 = Moderately stressed, 4 = Very stressed, 5 = Extremely stressed.
3.3.3. Relationship with the partner
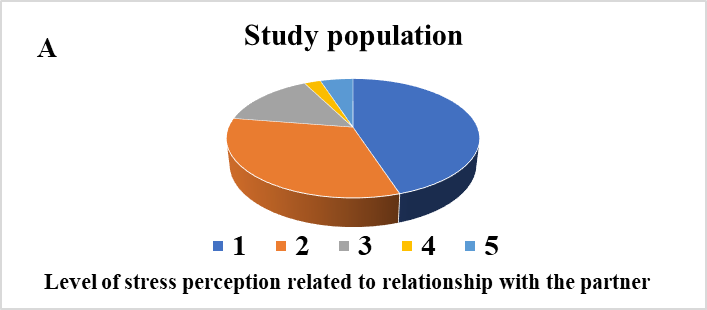
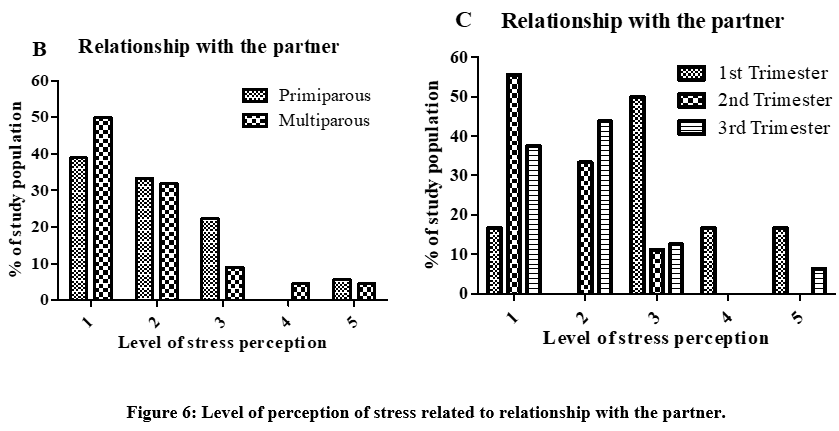
Results present in Figure 6A show that 45% of pregnant women in consultation at the HDCV were not at all stressed and 32.50% were little stressed by their relationship with their partner. Among the multiparous, 50% were not at all stressed and 31.82% were little stressed by their relationship with their partner, while among the primiparous, 38.89%,
33.33% and 22.22% were not at all stressed, little stressed, and moderately stressed respectively (Figure 6B). Regarding the trimester, 50% of pregnant women in the 1st trimester were moderately stressed by their relationship with their partner. In the 2nd trimester, 55.55% were not at all stressed and 33,33% were little stressed, while in the 3rd trimester, 43.75% were little stressed (Figure 6C).
<!-- /* Font Definitions */ @font-face {font-family:"Cambria Math"; panose-1:2 4 5 3 5 4 6 3 2 4; mso-font-charset:0; mso-generic-font-family:roman; mso-font-pitch:variable; mso-font-signature:-536869121 1107305727 33554432 0 415 0;} @font-face {font-family:Calibri; panose-1:2 15 5 2 2 2 4 3 2 4; mso-font-charset:0; mso-generic-font-family:swiss; mso-font-pitch:variable; mso-font-signature:-469750017 -1073732485 9 0 511 0;} /* Style Definitions */ p.MsoNormal, li.MsoNormal, div.MsoNormal {mso-style-unhide:no; mso-style-qformat:yes; mso-style-parent:""; margin-top:0in; margin-right:0in; margin-bottom:8.0pt; margin-left:0in; line-height:107%; mso-pagination:widow-orphan; font-size:11.0pt; font-family:"Calibri",sans-serif; mso-ascii-font-family:Calibri; mso-ascii-theme-font:minor-latin; mso-fareast-font-family:Calibri; mso-fareast-theme-font:minor-latin; mso-hansi-font-family:Calibri; mso-hansi-theme-font:minor-latin; mso-bidi-font-family:"Times New Roman"; mso-bidi-theme-font:minor-bidi; mso-fareast-language:EN-US;} span.q4iawc {mso-style-name:q4iawc; mso-style-unhide:no;} .MsoChpDefault {mso-style-type:export-only; mso-default-props:yes; font-size:11.0pt; mso-ansi-font-size:11.0pt; mso-bidi-font-size:11.0pt; font-family:"Calibri",sans-serif; mso-ascii-font-family:Calibri; mso-ascii-theme-font:minor-latin; mso-fareast-font-family:Calibri; mso-fareast-theme-font:minor-latin; mso-hansi-font-family:Calibri; mso-hansi-theme-font:minor-latin; mso-bidi-font-family:"Times New Roman"; mso-bidi-theme-font:minor-bidi; mso-font-kerning:0pt; mso-ligatures:none; mso-fareast-language:EN-US;} .MsoPapDefault {mso-style-type:export-only; margin-bottom:8.0pt; line-height:107%;} @page WordSection1 {size:8.5in 11.0in; margin:52.0pt 51.0pt 14.0pt .5in; mso-header-margin:5.75pt; mso-footer-margin:0in; mso-paper-source:0;} div.WordSection1 {page:WordSection1;} @page WordSection2 {size:8.5in 11.0in; margin:52.0pt 51.0pt 14.0pt .5in; mso-header-margin:5.75pt; mso-footer-margin:0in; mso-columns:2 even .5in; mso-paper-source:0;} div.WordSection2 {page:WordSection2;} @page WordSection3 {size:8.5in 11.0in; margin:1.0in 1.0in 1.0in 1.0in; mso-header-margin:.5in; mso-footer-margin:.5in; mso-paper-source:0;} div.WordSection3 {page:WordSection3;} -->
Study population: n = 40. A= In all pregnant women; B= Between multiparous and primiparous; C= Between the three trimesters of pregnancy. 1 = Not at all stressed, 2 = A little stressed, 3 = Moderately stressed, 4 = Very stressed, 5 = Extremely stressed.
3.3.4. Weight gain during pregnancy
As shown in Figure 7A, 45% and 37.50% of the study population were not at all stressed and little stressed by the weight gain during pregnancy, respectively. A percentage of 40.91 of multiparous were little stressed by gaining weight during pregnancy, while among the primiparous, 50% were not at all stressed and 33.33% were little stressed (Figure 7B). Regarding the trimester of pregnancy, 50% and 33.33% of pregnant women in the 1st trimester were not at all stressed and little stressed by gaining weight during pregnancy respectively. In the 2nd trimester, 55.55% and 33.33% were not at all stressed and little stressed respectively. Finally, in the 3rd trimester, 43.75% were little stressed about the weight gain during pregnancy (Figure 7C).
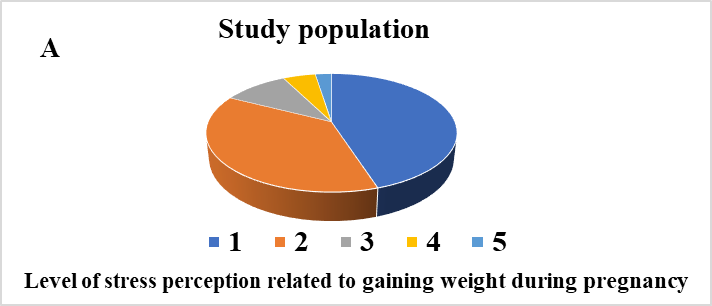
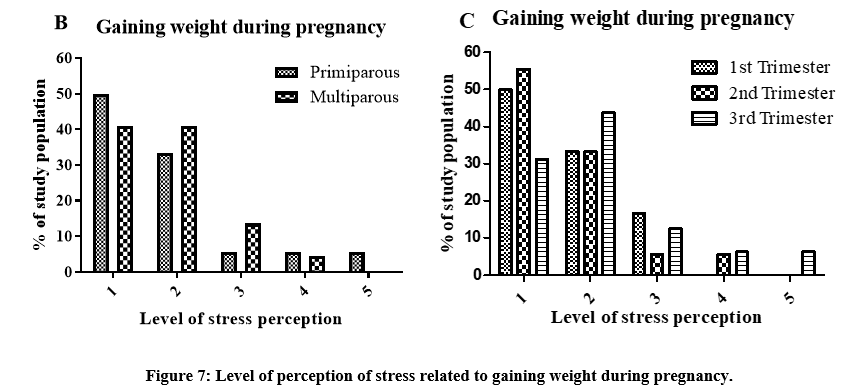
Study population: n = 40. A= In all pregnant women; B= Between multiparous and primiparous; C= Between the three trimesters of pregnancy. 1 = Not at all stressed, 2 = A little stressed, 3 = Moderately stressed, 4 = Very stressed, 5 = Extremely stressed.
3.3.5. The fact of not currently being able to do what she was doing before
The results presented in Figure 8A indicate that 77.5% of pregnant women consultting at the HDCV reported feeling not at all stressed while 10% reported to feel very stressed by the fact of not currently being able to do what they were doing before (smoking, drinking, going out, traveling, sports). Among multiparous women, 63.64% were not at all stressed and 18.18% were very stressed respectively by about these limitations. In contrast, for primiparous women, 94.44% reported no stress at all while 5.56% reported being moderately stressed (Figure 8B). Regarding the trimester, 83.33% of pregnant women in the 1st trimester were not at all stressed and 16.66% were moderately stressed by the fact of not currently being able to do what they were doing before. In the 2nd trimester, 83.33% were feeling not at all stressed and 11,11% were very stressed; while in the 3rd trimester, 68.75% were not at all stressed, 12.50% were moderately, and 12.50% were very stressed (Figure 8C).
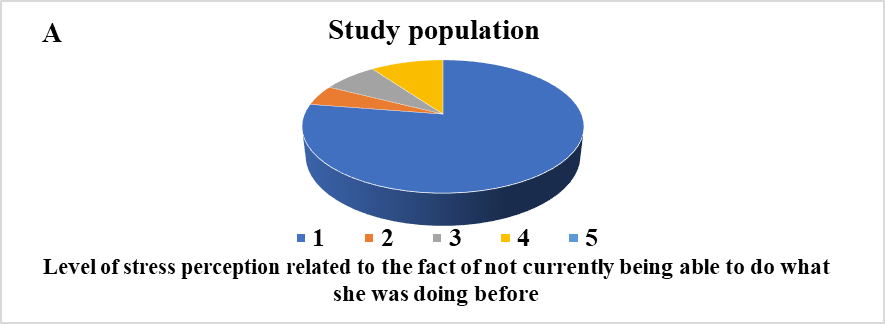
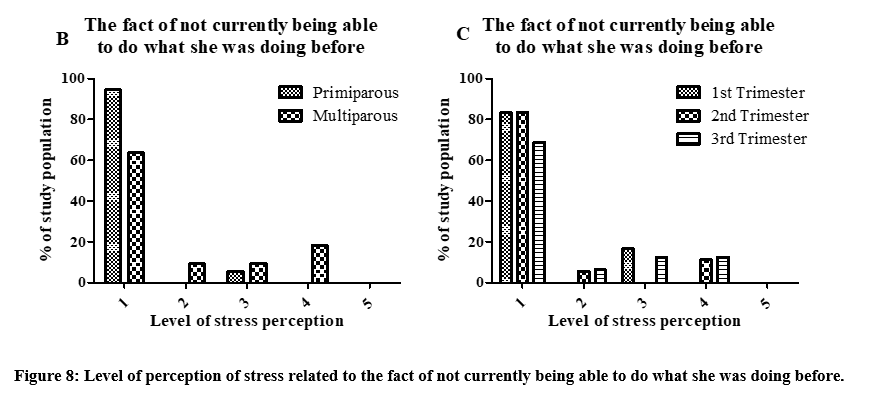
Study population: n = 40. A= In all pregnant women; B= Between multiparous and primiparous; C= Between the three trimesters of pregnancy. 1 = Not at all stressed, 2 = A little stressed, 3 = Moderately stressed, 4 = Very stressed, 5 = Extremely stressed.
3.3.6. The fear of losing her husband*
As shown in Figure 9A, 60% of the study population reported not to be at all stressed by the fear of losing their husband, while 17.50% expressed being very stressed. Among multiparous women, 63.63% were not at all stressed and 18.18% were very stressed regarding this fear. In contrast, 55.55% of primiparous women were not at all stressed and 16.66% were a little and very stressed (Figure 9B). Regarding the trimester of pregnancy,
33.33% of pregnant women in their 1st trimester indicated not being at all stressed about losing their husband, while 16.16% reported feeling little, moderately, very and extremely stressed. In the 2nd trimester, 72.22% of pregnant women were not at all stressed and 11.11% were little and very stressed. In the 3rd trimester, 56.25% of pregnant women were not at all stressed and 25% very stressed (Figure 9C).
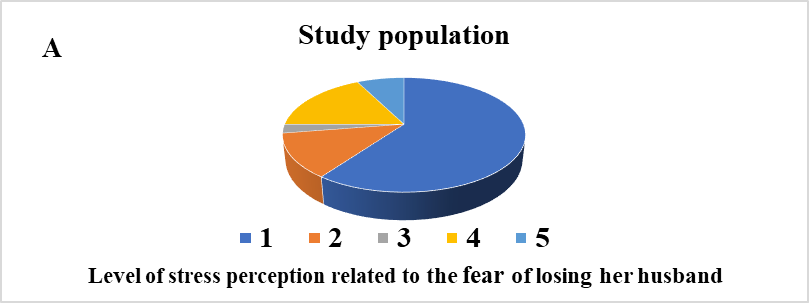
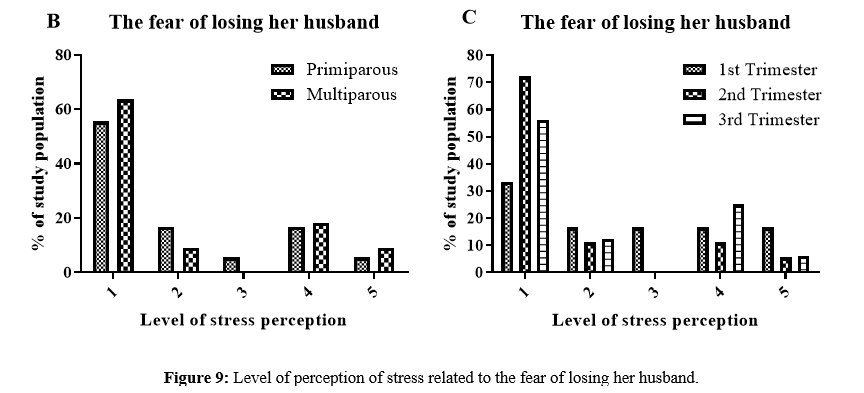
Study population: n = 40. A= In all pregnant women; B= Between multiparous and primiparous; C= Between the three trimesters of pregnancy. 1 = Not at all stressed, 2 = A little stressed, 3 = Moderately stressed, 4 = Very stressed, 5 = Extremely stressed.
3.3.7. The fact of not having money for the layette*
The analysis of Figure 10A shows that 32.50% of pregnant women in consultation at the HDCV were not at all stressed by the fact of not having money for the layette, while 20% were moderately and very stressed. 31.81% and 22.72% of multiparous were little and very stressed respectively by the fact of not having money for the layette. In comparison, 33.33% and 22.22% of primiparous women were not at all stressed and moderately stressed respectively (Figure 10B). Regarding the trimester of pregnancy, 33.33% of pregnant women in their 1st trimester were not at all and extremely stressed by the fact of not having money for the layette. In their 2nd trimester, 38.88% were little stressed and 31.25% in the 3rd trimester were very stressed (Figure 10C).
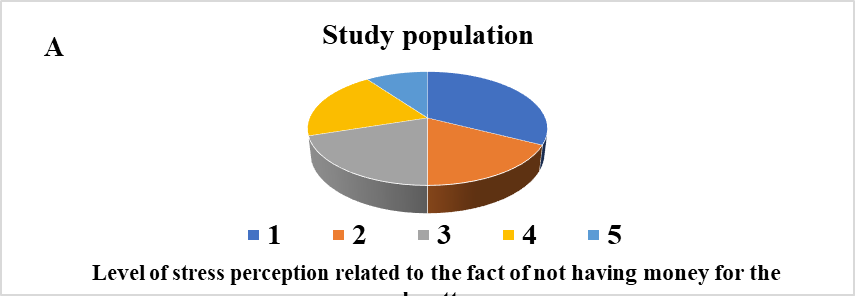
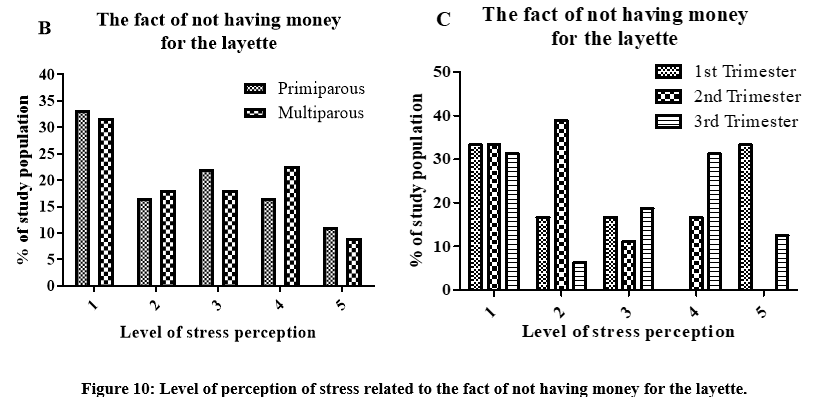
Study population: n = 40. A= In all pregnant women; B= Between multiparous and primiparous; C= Between the three trimesters of pregnancy. 1 = Not at all stressed, 2 = A little stressed, 3 = Moderately stressed, 4 = Very stressed, 5 = Extremely stressed.
3.4. Perception of stress related to prospect of childbirth
3.4.1. The risk of having an episiotomy
As shown in Figure 11A, 30% and 25% of the study population were little stressed and very stressed respectively by the risk of having an episiotomy. 22.73% and 40.91% of multiparous were not at all stressed and little stressed respectively by the risk of having an episiotomy, while 33.33% of primiparous were very stressed and 22.22% were extremely stressed (Figure 11B). Regarding the trimester of pregnancy, 33.33% of pregnant women in the 1st trimester were extremely stressed by the risk of having an episiotomy and 16.16% were not at all, little, moderately and very stressed. In the 2nd trimester, 33.33% of pregnant women were little and very stressed and in the 3rd trimester, 25% of pregnant women were not at all, little and very stressed (Figure 11C).
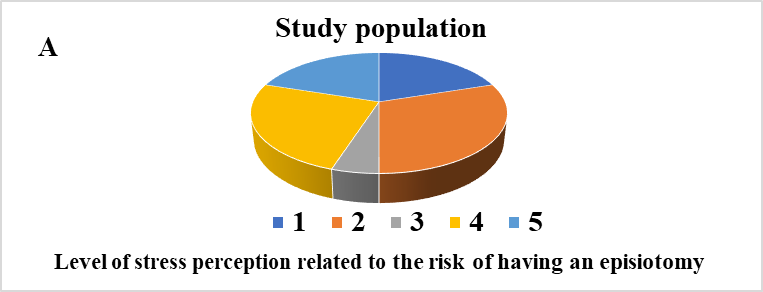
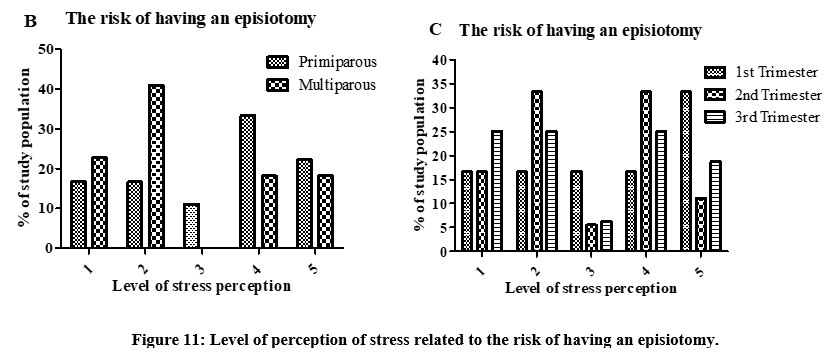
Study population: n = 40. A= In all pregnant women; B= Between multiparous and primiparous; C= Between the three trimesters of pregnancy. 1 = Not at all stressed, 2 = A little stressed, 3 = Moderately stressed, 4 = Very stressed, 5 = Extremely stressed.
3.4.2. The fact of not knowing the date on which the delivery will take place
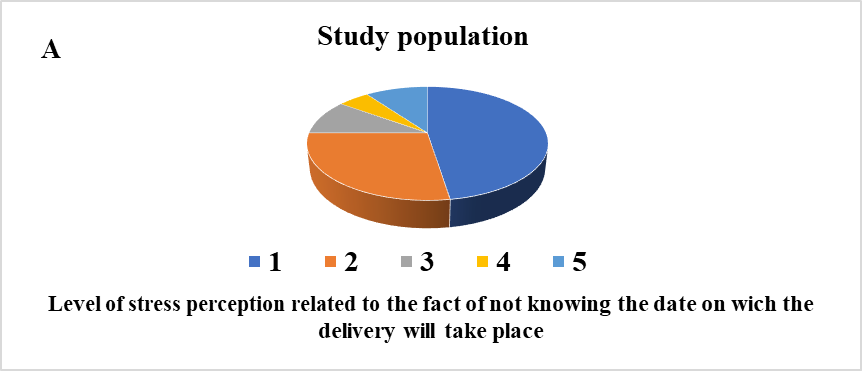
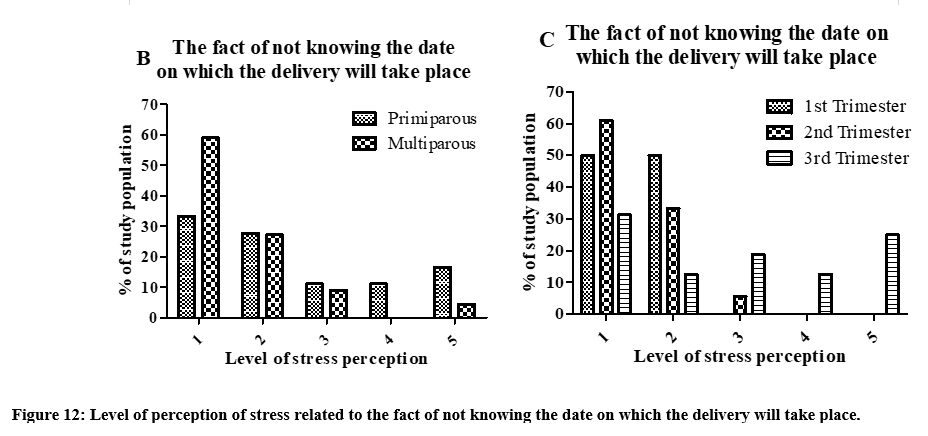
Results presented in 12A indicate that 47.50% of pregnant women in consultation at the HDCV were not at all stressed and 27.50% were little stressed by the fact of not knowing the date of child delivery. 59.09% of multiparous women were not at all stressed and 27.77% were little stressed by the fact of not knowing the date of delivery, while 33,33% and 27.27%
of primiparous were not at all stressed and little stressed respectively (Figure 12B). Regarding the trimester of pregnancy, 50% of pregnant women in the 1st trimester were not at all stressed and 50% were little stressed over not knowing their delivery date. In the 2nd trimester, 61.11% were not at all stressed and 33.33% were little stressed, while in the 3rd trimester, 31.25% were not at all stressed and 25% were extremely stressed (Figure 12C).
Study population: n = 40. A= In all pregnant women; B= Between multiparous and primiparous; C= Between the three trimesters of pregnancy. 1 = Not at all stressed, 2 = A little stressed, 3 = Moderately stressed, 4 = Very stressed, 5 = Extremely stressed.
3.4.3. Pain during childbirth*
The analysis of Figure 13A shows that 27.5% of pregnant women consulting at the HDCV reported feeling very stressed due to pain during childbirth. Among multiparous women, 27.27% reported being moderately stressed, while 38.89% of primiparous were feeling very stressed (Figure
13B). Looking at the data by trimester (Figure 13C), 33.33% of pregnant women in the 1st trimester were very stressed by pain during childbirth. In the 2nd trimester, 38.88% indicated being moderately stressed and 31.25% in the 3rd trimester were feeling a little stressed (Figure 13C).
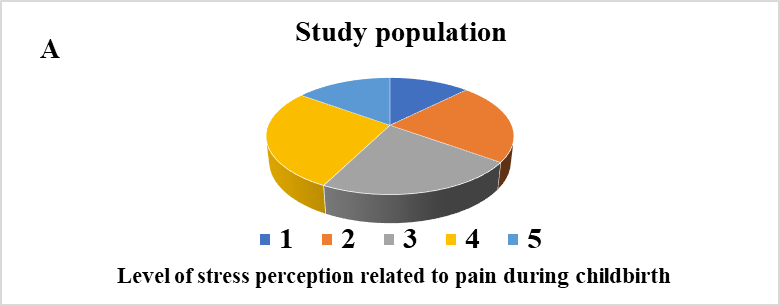
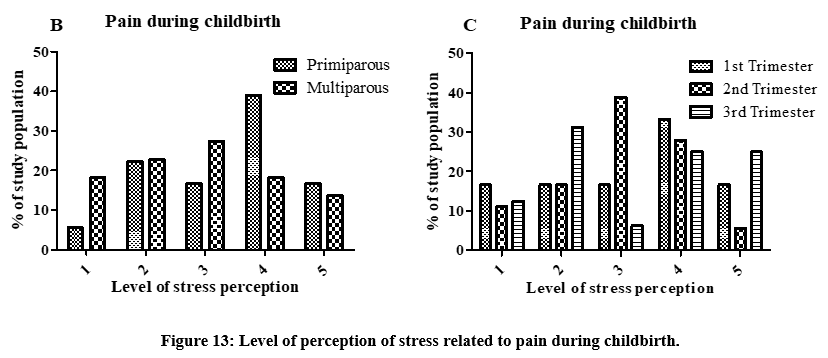
Study population: n = 40. A= In all pregnant women; B= Between multiparous and primiparous; C= Between the three trimesters of pregnancy. 1 = Not at all stressed, 2 = A little stressed, 3 = Moderately stressed, 4 = Very stressed, 5 = Extremely stressed.
4.2. Analysis and Discussion
The analysis of the results obtained from the adapted ASPI scale shows that pregnant women consulting at the HDCV in Yaoundé, Cameroon were stressed by the medical and obstetric risks/foetal health, the psychosocial changes during pregnancy and the prospect of childbirth subscales. The six most stressed factors observed in the world pregnant population were obstetric and medical problems (42.50%, little stressed), mood changes (40.00%, little stressed), current fatigue (37.50%, little stressed), weight gain during pregnancy (37.50%, little stressed), relationship with the partner (32.50%, little stressed) and risk of having an episiotomy (30.00%, little stressed). According to the results, it appears that pregnant women are all stressed by the medical and obstetric risks/foetal health, the psychosocial changes during pregnancy and the prospect of childbirth. In the population study, the high level of stress, “very stressed”, was obtained with pain during childbirth (27.50%), the risk of having an episiotomy (25%), and the fact of not having money for the layette (20%). We can deduce that, despite all the psychological and physical changes associated with pregnancy, the medical aspects including the health of the baby, ultrasound and medical or obstetrical problems remain the major concern for pregnant women during the entire course of their pregnancy. These results are in disaccord with Razurel et al. study (validation of the APSI scale), which obtained a low level of stress concerning the medical aspects of pregnancy, concerns about the health of the baby and the ultrasound [10]. This difference can be explained by the difference of the studied population (african in our study). Concerning the health of the baby and the medical aspects of pregnancy, these results are consistent with the results obtained by the study by Razurel et al. [10]. On this subject, the author reports that the choice of eliminating pain becomes a central concern. Regarding the items including “the fear of losing her husband” and “not knowing the date of delivery”, the results obtained show that these factors were not very stressful with respectively 60%, 32.50% and 47.50 % of pregnant women in HDCV consultation who do not feel stressed at all. In contrast, Razurel et al. reported significantly higher stress levels associated with these factors [10]. This discrepancy may be attributed to the fact that Razurel et al. focused solely on primigravida women in their validation study of the APSI scale, who may be more sensitive to these events [10]. Additionally, it is important to consider the socio-professional and cultural differences between the two populations being studied. The results from the adapted ASPI scale indicate that pregnant women consulting at the HDCV show that, generally, primiparous women experience more stress than multiparous women. The results obtained from the adapted ASPI scale shows that among pregnant women consulting at the HDCV in Yaoundé, Cameroon, primiparous women are more stressed than multiparous in general. The six most significant stressed factors observed in the primiparous population included the pain of childbirth (38.89% very stressed), the risk of having the episiotomy (33.33%, very stressed), the obstetrical or medical problems (33%, moderately stressed), the current fatigue (33.33%, little stressed), the relationship with the partner (33.33%, little stressed), and the fact of gaining weight (33.33%, little stressed). In the primiparous population, the high level of stress, “very stressed”, was obtained with the pain of childbirth (38.89%, very stressed) and the risk of having the episiotomy (33.33%, very stressed). In the multiparous population, the six most stressed factors observed were the mood change (54.55%, little stressed), the obstetrical or medical problems (50%, little stressed), the fact of gaining weight (40.91%, little stressed), the risk of having the episiotomy (40.91%, little stressed), the current fatigue (33.33%, little stressed), and the relationship with the partner (32% little stressed). Multiparous population were “very stressed” by the fact of not having money for the layette (22.72%), the pain of childbirth (18.18%), the risk of having the episiotomy (18.18%), the fact of not currently being able to do what they were doing before (18.18%), and the fear of losing their husbands (18.18%). These results are consistent with data from the literature. Indeed, Sauvegrain explains that multiparous women typically experience lower stress levels than they did during their first pregnancies [11]. The increased stress levels in primiparas may arise from their inexperience with pregnancy and the new challenges of becoming a parent. Given the results, it seems legitimate to assume that pregnancy, experienced for the first time in primiparous women, represents an unfamiliar and significant life event accompanied by psychological and physical changes, which therefore tends to increase their stress. On the other hand, multiparous women rely on their prior experiences to navigate pregnancy with greater ease. The uncertainty and the unknown around the first pregnancy seems to play a central role in the stress phenomenon. Therefore, it is important to adapt the support and guidance provided to mothers according to their parity, considering the expectations and specific needs of each group. Additionally, educational interventions that bring together both primiparous and multiparous women can help address the stress experienced by first-time mothers while valuing the insights gained from the experiences of those who have previously given birth. This approach aligns with the recommendations from the “Haute Autorité de Santé, France” regarding training for birth and parenthood [12].
Research indicates that, pregnant women experience varying levels of stress throughout the different trimesters of pregnancy. Pregnant women are more stressed in the first trimester than second and third trimesters [11]. During the first trimester, the most stressful factors included relationship with the partner (50%, moderately stressed), the fact of not having money for the layette (33.33%, extremely stressed), the risk of having an episiotomy (33.33%, extremely stressed), and the pain during childbirth (33.33%, very stressed). In the second trimester, the fact of not currently being able to do what she was doing before (11,11%, very stressed), the fear of losing her husband (11.11%, very stressed), the risk of having an episiotomy (33.33%, very stressed), and pain during childbirth (38.88%, moderately stressed) were the most stressful factors. Regarding the third trimester, the most stressful factors were obstetrical or medical problems (31.25%, moderately stressed), the fact of not having money for the layette (31.25%, very stressed), the fact of not knowing the date on which the delivery will take place (25%, extremely stressed), the fear of losing her husband (25%, very stressed), and the risk of having an episiotomy (25%, very stressed). These fluctuations in the stress levels highlights the fact that pregnant women are rather stressed by what they are going through at the time and do not plan much for future events. In the first trimester, the level of stress can be related to the health of the baby and the ultrasound results, while in the third trimester this level is higher with regard to having the episiotomy and the pain of childbirth. Their stress therefore evolves according to the different stages in which they find themselves. These results may lead to increased reflection by health professionals in order to propose new courses of action in order to reduce this perception of stress at the appropriate times.
5. Conclusion and recommendations
The present study aimed to assess the perception of stress in pregnant women’s consulting at the “Cité Verte” District Hospital in Yaoundé (Cameroon). A quantitative, comparative study was conducted through a questionnaire adapted from the Antenatal Perceived Stress Inventory (APSI). This study showed that pregnancy is associated with high levels of stress, especially for first-time mothers (primiparous women). The findings support the the establishment of improved care for these women, including the implementation of prenatal preparation for childbirth at the onset of pregnancy and personal follow-up for those who experience the highest levels of stress.
Consent for publication
Not applicable.
Availability of data and materials
The datasets used and/or analyzed during the current study are available from the corresponding author on reasonable request.
Competing interests
The authors declare that they have no competing interests.
Funding
Not applicable
Acknowledgment
The authors are thankful to all the pregnant women who participate in this study.
References
- Alipour, Z., et al., (2018). The most important risk factors affecting mental health during pregnancy: a systematic review. Eastern Mediterranean Health Journal,. 24(6): p. 549-559.
View at Publisher | View at Google Scholar - Padmavathi, P., (2014). Assess the Effectiveness of Benson’s Relaxation on Stress among antenatal mothers attending outpatient department in selected PHC at Namakkal District. International Journal of Advances in Nursing Management,. 2(2): p. 86-89.
View at Publisher | View at Google Scholar - Anna-Lena, Z., et al., (2019). Emotional Stress During Pregnancy – Associations With Maternal Anxiety Disorders, Infant Cortisol Reactivity, and Mother–Child Interaction at Pre-school Age. Frontiers in Psychology,. https://doi.org/10.3389/fpsyg.2019.02179.
View at Publisher | View at Google Scholar - Pallavi, T. and B. Arunjyoti, (2022). Factors contributing to stress in pregnant women and its Outcome- A Narrative Review. Asian Journal of Nursing Education and Research. 12(3): DOI: 10.52711/2349-2996.2022.00059.
View at Publisher | View at Google Scholar - Seaward, B.L., (2014). Essentials of Managing Stress. 3rd ed. United States of America: Jones and Bartlett Learning.
View at Publisher | View at Google Scholar - Ilknur, A. and S.C. Asli, (2018). The validity and reliability of the Antenatal Perceived Stress Inventory Turkish version: A methodological study. Health Care for Women International,. https://doi.org/10.1080/07399332.2018.1469635.
View at Publisher | View at Google Scholar - Leight, K.L., et al., (2010). Childbirth and mental disorders. International Review of Psychiatry,. 22: p. 453-471.
View at Publisher | View at Google Scholar - Dunkel, S.C. and L. Tanner, (2012). Anxiety, depression and stress in pregnancy: implications for mothers, children, research, and practice. Current opinion in psychiatry,. 25(2): p. 141-148.
View at Publisher | View at Google Scholar - Woods, S.M., et al., (2010). Psychosocial stress during pregnancy. American journal of obstetrics and gynecology,. 202(61): p. e1-61.e7.
View at Publisher | View at Google Scholar - Razurel, C., et al., (2013). Relation Between Perceived Stress, Social Support, and Coping Strategies and Maternal Well-Being: A Review of the Literature. Women & Health,. 53(1): p. 74-99.
View at Publisher | View at Google Scholar - Sauvegrain, P., (2008). « Toutes les femmes ont-elles accès aux séances de préparation à la naissance ? » Spirale,. 47(2008): p. 167-78.
View at Publisher | View at Google Scholar - HAS, Haute Autorité De Santé (2005). Recommandations professionnelles : comment mieux informer les femmes enceintes ? 1ère édition. http://www.hassante.fr/portail/docs/application/pdf/femmes enceintes_recos _ pdf.
View at Publisher | View at Google Scholar
